
Abstract
Background and aims:
This randomised controlled experimental study aims to determine the effect of the Emotional Freedom Technique (EFT) applied in the postoperative period on pain and anxiety in patients who have had total knee replacement surgery.
Methods:
The study sample comprised 80 patients (40 experimental, 40 control) selected via block randomisation. A Patient Descriptive Information Form was used to collect socio-demographic data. The Visual Analogue Scale (VAS), State-Trait Anxiety Inventory (STAI-S, STAI-T) and Subjective Unit of Experience Scale (SUE) were employed to assess and compare the effects of the intervention on postoperative pain, anxiety and subjective emotional states across both groups.
Results:
Pre-test STAI-S and VAS scores showed no significant differences between group (p > 0.05). Post-intervention, the experimental group demonstrated statistically significantly lower STAI-S and VAS scores compared to the control group (p < 0.05). This shows that, after the intervention, patients who received EFT experienced lower levels of postoperative state and pain compared with patients who received standard care.
Conclusion:
EFT is a potent, non-pharmacological, nurse-led intervention for reducing postoperative pain and state anxiety. Implementing EFT can enhance recovery quality and promote a holistic, biopsychosocial approach to care while reducing reliance on pharmacological analgesics.
Introduction
Total knee prosthesis is the surgical replacement of the tibial, femoral and patellar joint surfaces with metal and plastic components to treat bone damage caused by osteoarthritis and deformity. The primary goals of this procedure include reducing pain, correcting deformities, ensuring joint stability and mobility and ultimately improving the patient’s functions and quality of life (Altıntaş et al., 2009; Elbaş and Erdil, 2008; Kılıç E et al., 2009). According to the 2025 health statistics report published by the Organisation for Economic Co-operation and Development (OECD), the highest rates of total knee replacement surgeries were recorded in Switzerland (318 per 100,000 inhabitants), Germany (268 per 100,000), Australia (264 per 100,000), Finland (264 per 100,000) and Denmark (263 per 100,000). These high rates indicate that total knee replacement is a widely performed surgical intervention in developed healthcare systems and highlights the growing global burden of knee osteoarthritis, suggesting that the demand for this procedure is likely to increase further in the future. According to this same report in 2025, knee replacement surgeries were performed on 109 individuals per 100,000 people in Turkey (OECD, 2025), reflecting a similar upward trend in regional surgical volumes.
Osteoarthritis (OA) is the primary indication for total knee replacement surgery. Increasing age and obesity are well-established risk factors for the development and progression of knee osteoarthritis, which consequently increases the need for knee replacement surgery (Wallace et al., 2017). Aging promotes OA through biological mechanisms such as oxidative stress and chronic systemic inflammation, which lead to joint tissue destruction. Additionally, age-related declines in muscle strength and subchondral bone density alter joint loading and stability, further driving OA pathogenesis (Felson et al., 2000; Loeser et al., 2016). Concurrently, obesity accelerates joint degeneration not only via increased mechanical load but also through ‘metainflammation’ caused by proinflammatory adipokines (Felson et al., 2000; Wluka et al., 2013). Considering the global increase in the elderly population and the rising prevalence of obesity, these pathophysiological mechanisms suggest that the demand for total knee replacement surgery will continue to escalate significantly in the coming years.
Orthopaedic surgeries are among the most painful operations (Chung et al., 1997; Remérand et al., 2009; Wang et al., 2020) and patients experience moderate-to-severe pain after total knee surgery (Akyol et al., 2009; Dubljanin Raspopović et al., 2021; Parvataneni et al., 2007). Postoperative pain may cause a decrease in patient satisfaction and a delay in mobilisation, as well as increased anxiety (Beattie et al., 2003; Kehlet et al., 2006; Pöpping et al., 2008; Rodgers et al., 2000; Singh et al., 2006). Pain and anxiety are intertwined issues, and one inevitably leads to the other in the postoperative period. Unrelieved anxiety has negative effects on the postoperative recovery of the patient. Pain and anxiety experienced in the postoperative period can prolong hospital stay and wound healing time, reduce patient satisfaction and increase healthcare costs (Caumo et al., 2001; Jamison et al., 1993; Mavros et al., 2011; Korean Knee Society, 2012). For this reason, it is of great importance to ensure postoperative pain control.
Non-pharmacological methods that support pharmacological treatment can be employed to control pain and anxiety (Lim et al., 2022; Tick et al., 2018). The nurse can make a significant contribution to the control of pain and anxiety by using various non-pharmacological methods that can be used together with pharmacological treatment to relieve pain (Frazier et al., 2002; McCaffery, 1990; McCaffery and Beebe, 1994). Stress balls, massage, relaxation exercises (rhythmic breathing, muscle relaxation exercises, etc.), acupressure and acupuncture have been used as non-pharmacological methods to manage anxiety and pain in patients undergoing total knee replacement surgery, and successful results have been reported (Büyükyılmaz and Aştı, 2013; Çınar and Çam, 2018; He et al., 2013; Pellino et al., 2005; Williamson et al., 2007). The Emotional Freedom Technique (EFT) is one non-pharmacological method that can be used for patients after surgery. It is also one of the energy psychology interventions that creates psychological and physical changes in the individual by using cognitive behavioural therapy, exposure therapy and acupuncture points. EFT is also called ‘needle-free acupuncture’ or an emotional form of acupressure (Bougea et al., 2013). When the energy flow in the body is blocked and occlusions occur because of any condition, negative emotions are experienced in the individual. If these negative emotions continue for a long time, they may also cause physical symptoms. EFT aims to eliminate the physical and psychological problems caused by any disorder by correcting the disrupted energy flow in the individual (Church and Brooks, 2010; Craig, 2004).
Previous studies have demonstrated the effectiveness of EFT in reducing pain and anxiety across various clinical and occupational contexts. In a randomised study conducted by Cici and Özkan (2022), EFT applied preoperatively to patients undergoing lumbar disc herniation surgery was found to significantly reduce anxiety levels and stabilise vital signs; moreover, EFT was more effective than music therapy in regulating anxiety and respiratory rate (Cici and Özkan, 2022). In a different context, Dincer and Inangil (2021) reported that EFT significantly reduced stress, anxiety and burnout levels among nurses working during the COVID-19 pandemic (Dincer and Inangil, 2021). With respect to pain-related outcomes, Bougea et al. (2013) evaluated the short-term effects of EFT in patients with tension-type headaches and found significant reductions in perceived stress as well as in the frequency and intensity of headache episodes (Bougea et al., 2013). Similarly, Benor et al. (2017) demonstrated that EFT, when used alongside standard medical care, was a promising intervention for reducing pain, anxiety and depression in patients with chronic pain (Benor et al., 2017). Collectively, these findings suggest that EFT is an effective complementary approach for alleviating pain- and anxiety-related symptoms in diverse populations.
The physiological mechanism of EFT involves the stimulation of acupuncture points, which decreases pain severity by increasing the release of endogenous opioids-such as endorphins, enkephalins and dynorphins-and serotonin while simultaneously modulating brain activity associated with pain perception (Dhond et al., 2007; Ulett, 1992). There are also studies reporting that the signals produced as a result of touching acupuncture points are sent to certain parts of the body faster and more directly than the transmission in the nervous system (Langevin and Yandow, 2002; Oschman, 2003). Although a previous study has documented the effectiveness of EFT in managing postoperative pain (Padmapriya and Jenifer, 2020), its combined impact on both pain and anxiety levels remains unexplored, particularly within the total knee arthroplasty population. In this context, the purpose of the present study was to examine the effects of EFT on pain and anxiety in the postoperative period of patients who underwent total knee arthroplasty.
Research hypotheses
Materials and methods
Study design
This single-centre, randomised controlled experimental study was conducted in Aksaray University Education and Research Hospital, Türkiye between March and September 2022. The study was registered at ClinicalTrials.gov (NCT05541666).
Study population
The study population consisted of patients who underwent total knee replacement surgery at the Orthopaedics and Traumatology Clinic of a Training and Research Hospital from March to September 2022. G*Power 3.1 software (Heinrich Heine University, Düsseldorf, Germany) was utilised to ascertain the sample size for the study, and a statistical power analysis was conducted. The analysis determined the margin of error (α) at 0.05, test power (1–β) at 90% and effect size (f) at 0.74, which is classified as a large effect according to Cohen’s criteria (Cohen, 2013). The study determined this effect size based on the findings of prior analogous investigations (Çınar and Çam, 2018). According to these guidelines, it was determined that 64 patients in total (32 patients in each of the experimental and control groups) would be sufficient. Nevertheless, comparable research has indicated that patient loss rates are approximately 20% (Schulz and Grimes, 2002). However, because of problems, such as voluntary withdrawal and withdrawal during the application process, a higher loss rate was anticipated in this study (Detry and Lewis, 2014). According to these forecasts, 56 patients were initially included in each group, starting the study with a total of 112 patients (56 experimental and 56 control) to account for potential losses and guarantee that the study was finished with adequate statistical power in both groups (Lachin, 2000). This randomised controlled trial was reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) statement (Schulz et al., 2010). Participant recruitment, allocation, follow-up and analysis are presented in the CONSORT flow diagram (Figure 1).
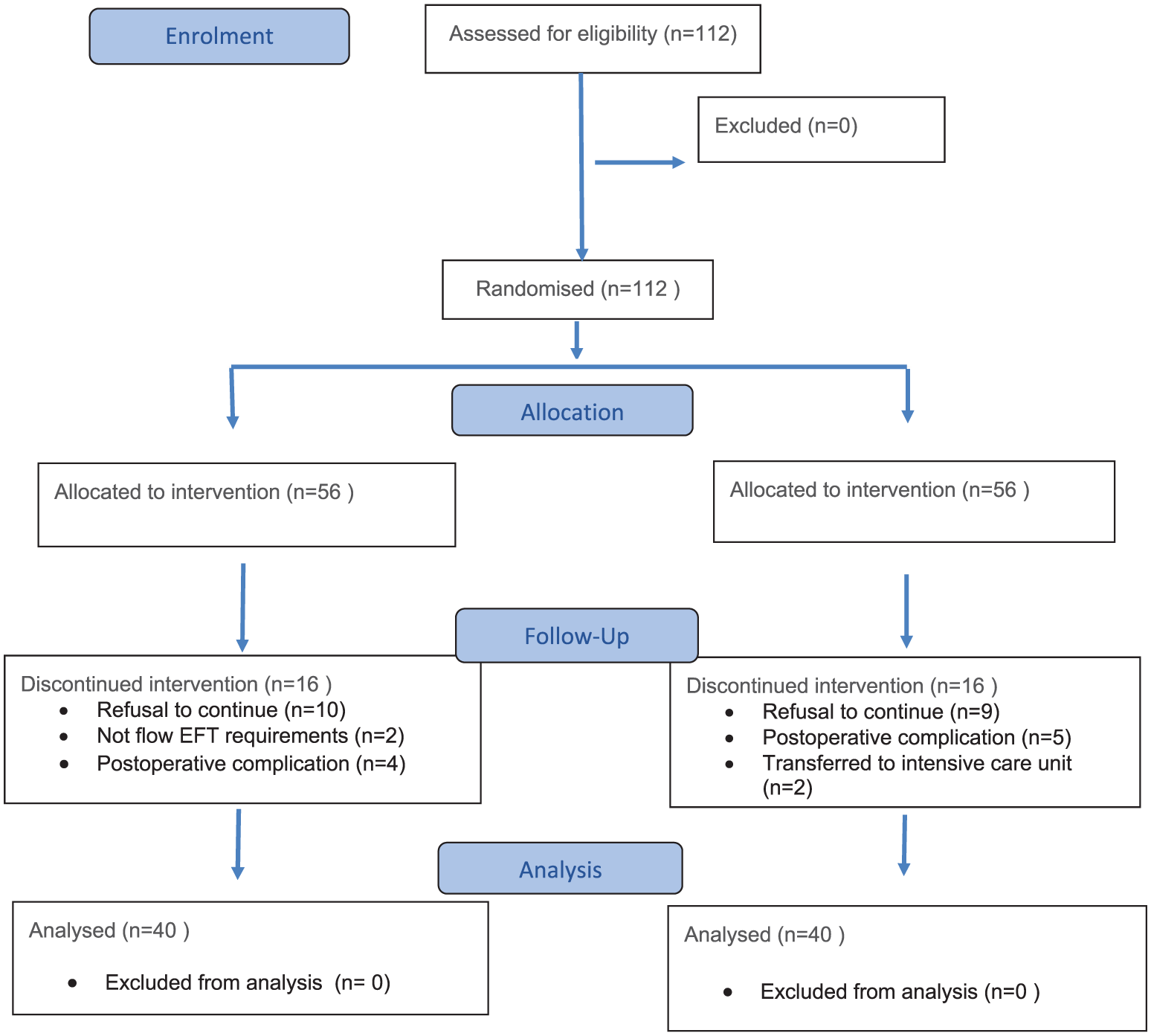
The process of the study based on the CONSORT flow diagram.
In the experimental group, a total of 16 patients were excluded during the follow-up period: four patients due to postoperative complications, five patients who declined to continue participation on postoperative day 2, five patients who requested to discontinue the intervention during the application on postoperative day 1 and two patients who did not comply with the EFT procedure steps. In the control group, 16 patients were also excluded: two patients who were transferred to the intensive care unit, five patients due to postoperative complications and nine patients who declined to answer the questionnaires. Consequently, the study was completed with 80 patients who met the inclusion criteria and consented to participate, with 40 patients in the experimental group and 40 patients in the control group.
Inclusion criteria
Patients who had undergone total knee replacement surgery for the first time, were 18 years of age and over, had not used EFT before, had no vision, hearing or speech problems that would hinder communication, volunteered to participate in the study, had cognitive levels suitable for the procedure and those who did not have another disease that would cause pain and anxiety were included in the study.
Exclusion criteria
Patients who had used EFT before, who developed any complications within 3 days before, during and after the surgery, and who had health problems that prevented the application of the EFT were not included in the study.
Randomisation
Using a block size of four and a ratio of 1:1, the permutation block randomisation approach was used to randomly assign study-eligible patients to either the experimental or control group. To guarantee a numerical balance between the groups, and that each group had an equal number of participants, the block randomisation method was chosen. Two individuals were assigned to experimental and control groups in each block. This procedure involved randomly generating potential permutations that would determine the order in which participants were assigned to the experimental (E) and control (C) groups for each block. For instance, a block of four may have the following permutations: E, E, C, C; E, C, E, C; C, E, C, E, etc. For each block, one of these permutations was chosen at random, and the participants were thereafter allocated to either the experimental or control groups based on the chosen permutation. To maintain the impartiality of data analysis, the data analyst was blinded and unaware of the participants’ group assignments.
Intervention
The researcher received internationally recognised Basic EFT Training and Expert EFT Practitioner Training from The Guild of Energists. One day before the surgery, the patients in both groups were interviewed, and the Patient Descriptive Data Form, Visual Analogue Scale (VAS) Pain (Tulunay and Tulunay, 2000) and State-Trait Anxiety Inventory (STAI) (Oner and Le Compte, 1998; Spielberger et al., 1971) were applied. Then, information was given to the experimental group about EFT and the patients’ questions were answered. On the first postoperative day between 18.00 and 20.00, the patients in both groups were interviewed to collect the pretest data and VAS Pain, State Anxiety Inventory (STAI-S) and Subjective Units of Experience (SUE) (Hartmann, 2021b) were applied. Then, the EFT steps were explained and demonstrated to the experimental group, and a session of EFT was applied. After the EFT, the SUE scale was re-evaluated without any break. On the second postoperative day between 18.00 and 20.00, the patients in both groups were interviewed again, and the SUE Scale was evaluated. Then, a session of the EFT was applied to the experimental group. After the EFT, VAS Pain, STAI-S and SUE were re-applied without any break for post-test data. In the control group VAS Pain, STAI-S and SUE were re-applied for post-test data on the second postoperative day between 18.00 and 20.00.
Each EFT session lasted approximately 25–40 minutes. After the patients to be included in the study were determined, an hour was determined outside the nurses’ treatment and follow-up hours to ensure that the patients could make independent decisions regarding their pain and anxiety assessments and the session was not interrupted, and the nurses were notified before entering the patient room. Also, care was taken to ensure that the patient’s relatives were not in the same room and that the patient did not have any urgent biological need, and that the room was quiet and calm.
Measurements
The following instruments were used in this study: Patient Descriptive Data Form, Visual Analogue Scale (VAS) Pain, State-Trait Anxiety Inventory (STAI) and SUE.
Patient descriptive data form
The Patient Descriptive Data form, which was prepared by the researchers in line with the literature (Büyükyılmaz and Aştı, 2013; Çınar and Çam, 2018), consisted of questions about the patient’s sociodemographic characteristics and general health status.
Visual Analogue Scale pain
The scale consists of a 10-mm horizontal line. One end indicates ‘No pain’ on this line, whereas the other end indicates ‘The worst possible pain’. The patient is asked to mark the appropriate interval on this 10-mm line (Tulunay and Tulunay, 2000).
State-Trait Anxiety Inventory
The State-Trait Anxiety Scale was developed by Spielberg et al. in 1970 (Spielberger et al., 1971). The validity and reliability study of the Turkish form was conducted by (Öner and Le Compte, 1998). The State-Trait Anxiety Scale consists of two separate subscales. The State Anxiety Inventory (STAI-S) measures how the individual feels ‘at a specific moment’ and assesses subjective feelings of tension and apprehension. In contrast, the Trait Anxiety Inventory (STAI-T) assesses ‘anxiety as a stable personality trait’, reflecting the individual’s general tendency to perceive situations as threatening. There are a total of 40 statements; the first 20 items measure the state anxiety (STAI-S) level, and the next 20 items measure the trait anxiety (STAI-T) level. The scores obtained from the scales theoretically range between 20 and 80 (0–19 no anxiety, 20–39 mild anxiety, 40–59 moderate anxiety, 60–79 high anxiety and 80 panic anxiety). The Cronbach’s alpha value found in the reliability analysis was between 0.94–0.96 in STAI-S and 0.83–0.87 in STAI-T (Öner and Le Compte, 1998; Öztaş et al., 2022). Cronbach’s alpha values found in the reliability analysis that was conducted in the present study were between 0.85–0.91 in STAI-S and 0.83–0.91 in STAI-T.
Subjective units of experience
This was developed by SUE Hartman to evaluate the energy flow in the energy body in the simplified version of the energy body stress chart (Hartmann, 2021a). Emotions provide information about the state of the energy body. SUE was used to determine the intensity (degree) of the individual’s emotion at the beginning and end of the EFT session (Hartmann, 2021b).
The evaluation of this scale is between ‘−10’ and ‘+10’.
−10 refers to the greatest pain, disappointment, fear, anxiety, stress, pain, sadness or discomfort imaginable.
‘0’ refers to the state where there is no emotion.
‘+10’ refers to the highest level of joy, happiness or feeling great.
Data analysis
Analyses of the data collected in the study were made with the SPSS for Windows 22.00 statistical package program (IBM Corp., Armonk, NY, USA). Numbers, percentages, standard deviation and mean values were used to evaluate the data. The Kurtosis-Skewness value was checked to determine normal distribution. The reliability of the measurement tools was determined by the Cronbach-α number, and categorical variables were determined by the chi-square test to determine the homogeneity between the groups. The independent groups t-test was used to compare the VAS, STAI-S, STAI-T and SUE score means of the experimental and control groups. The results were interpreted with a 95% confidence interval and at a significance level of p < 0.05.
Ethical statement
Before starting the study, approval was obtained from the Atatürk University Faculty of Medicine Clinical Research Ethics Committee (decision number 67) and written permission was obtained from the centre where the study would be conducted. Only patients who voluntarily agreed to participate in the study were included. All participants were informed about the purpose of the study. Verbal and written informed consent was obtained from all participants after providing the necessary explanations. Participants were clearly informed that they could withdraw from the study at any stage without any consequences. All collected data and the identities of the participants were treated as confidential and used solely for research purposes. To ensure the protection of individual rights, the ethical principles outlined in the Declaration of Helsinki were strictly adhered to throughout the study.
Results
Patient characteristics and surgical details
The study was completed with 80 patients (40 in the experimental and 40 in the control group) who met the inclusion criteria and agreed to participate in the study. The mean age of the participants was 63.10 ± 8.08 years in the experimental group and 65.55 ± 7.07 years in the control group. A significant majority of the participants in both groups were female (82.5%) and married (experimental: 87.5%, control: 95.0%). Regarding their educational background, the largest subgroup comprised those with an elementary education (experimental: 57.5%, control: 50.0%), whereas most participants were housewives (experimental: 80.0%, control: 85.0%). Chronic diseases were highly prevalent across the cohort (experimental: 90.0%, control: 77.5%), and most individuals had prior surgical experience (experimental: 85.0%, control: 72.5%). Most patients underwent unilateral surgery (experimental: 72.5%, control: 77.5%) and reported using analgesics as their primary method for coping with pain. No statistically significant differences were detected between the groups in terms of demographic characteristics (p > 0.05, Table 1).
Demographic data and surgical characteristics.
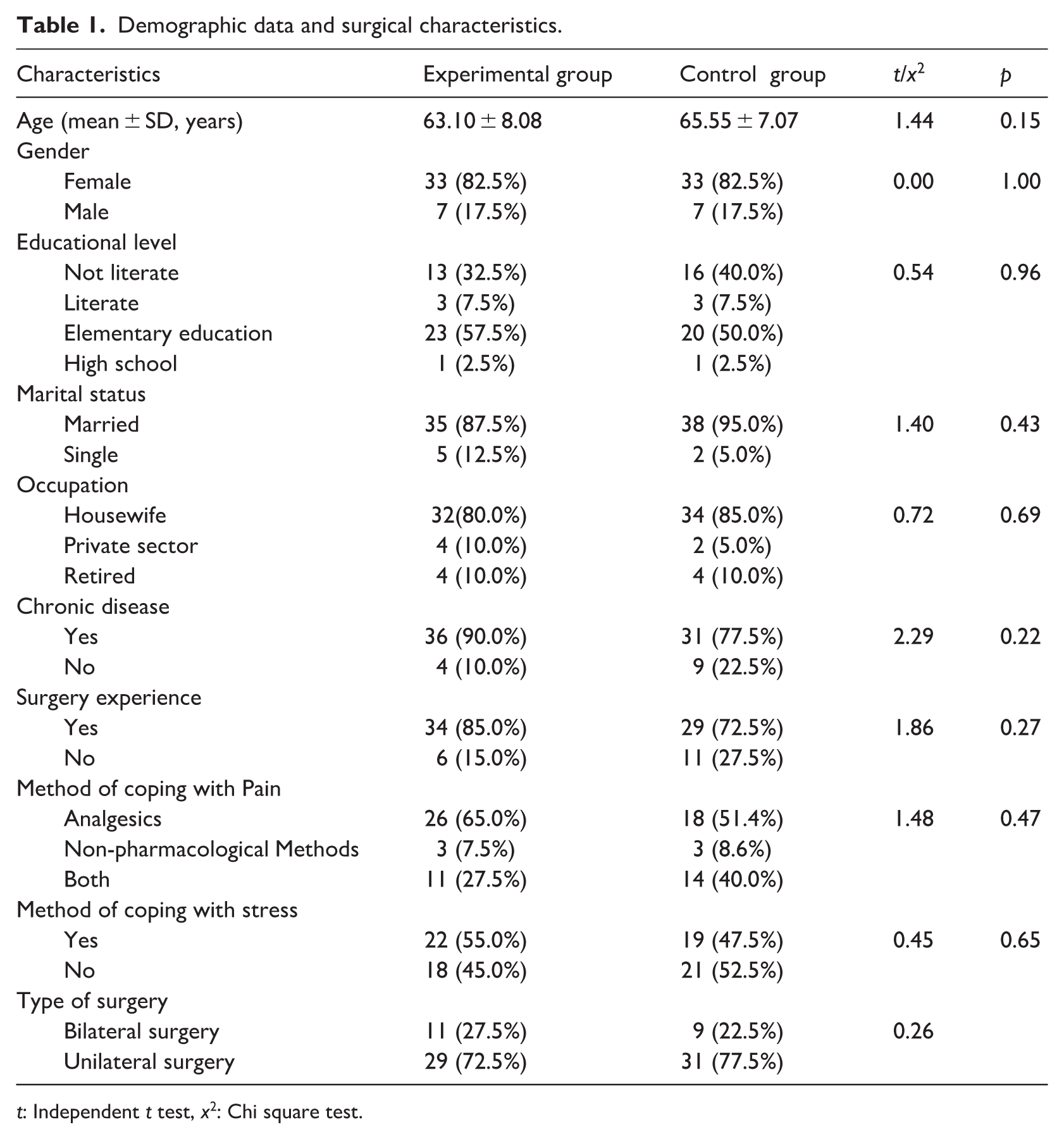
t: Independent t test, x2: Chi square test.
Comparison of preoperative pain and state-trait anxiety scores between two groups
The comparison of the mean pain, STAI-S and STAI-T scores of the patients in the groups before the surgery is given in Table 2. It was found that the mean pain, STAI-S and STAI-T scores of the patients in the experimental and control groups before the surgery were similar, and there were no statistically significant differences between the groups (p > 0.05, Table 2).
Comparison of preoperative pain and state-trait anxiety scores between two groups.
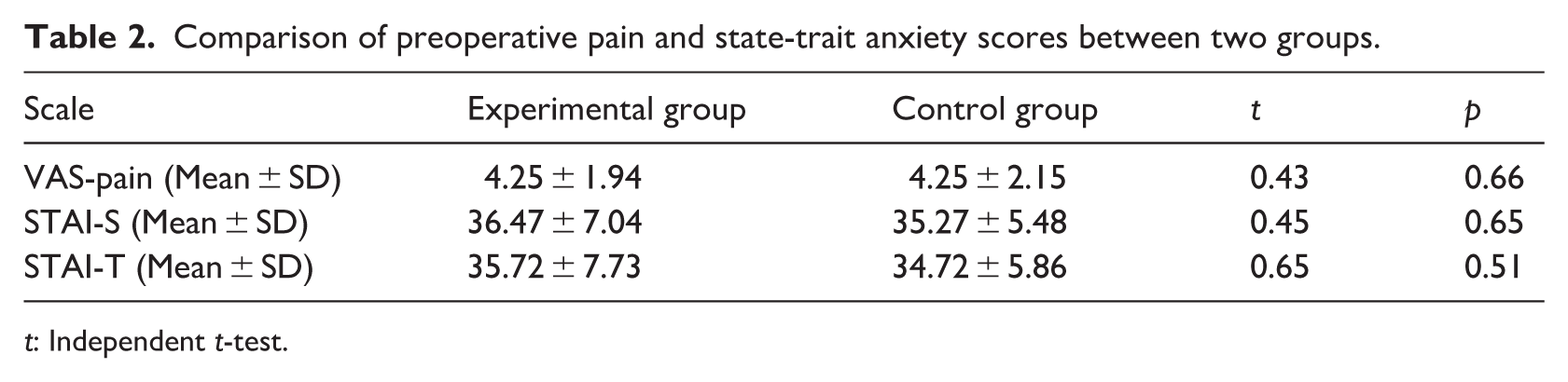
t: Independent t-test.
Comparison of postoperative pain scores between two groups
No statistically significant differences was found between the pain scores of the groups before EFT on the first postoperative day (p = 0.55, Table 3). However, the pain score of the patients in the experimental group (1.72 ± 1.43) was found to be statistically and significantly lower than the pain score of the patients in the control group (4.15 ± 1.52) after EFT on the second postoperative day (p = 0.001, Table 3).
Comparison of postoperative pain scores between two groups.
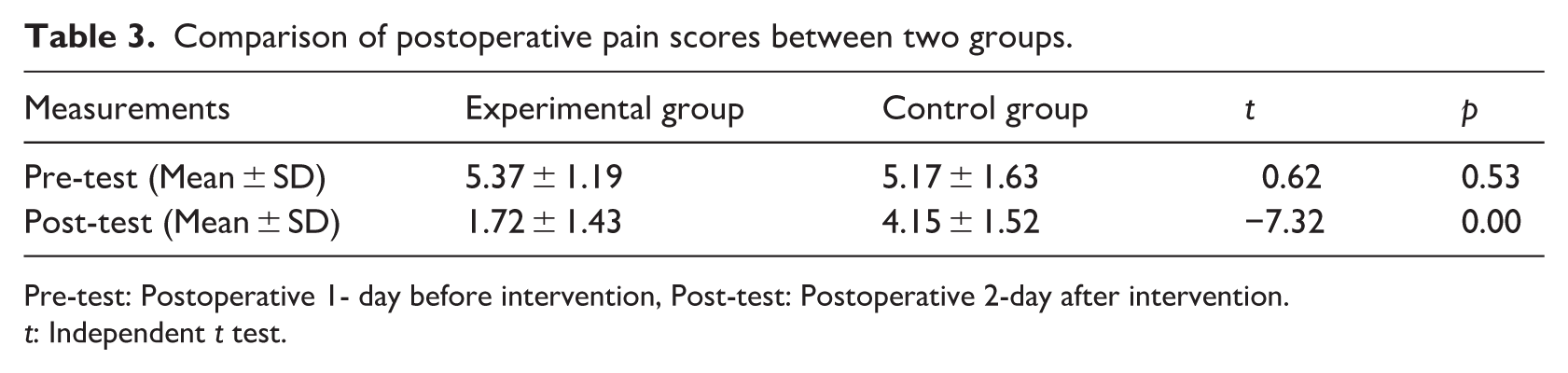
Pre-test: Postoperative 1- day before intervention, Post-test: Postoperative 2-day after intervention.
t: Independent t test.
Comparison of postoperative state anxiety scores between two groups
No statistically significant difference was found between the mean state anxiety scores of the patients in the experimental group and control group before EFT on the first postoperative day. However, the mean state anxiety score of the patients in the experimental group (27.35 ± 4.69) was found to be statistically and significantly lower than the mean state anxiety score of the patients in the control group (36.42 ± 5.83) after EFT on the second postoperative day (p = 0.000, Table 4).
Comparison of postoperative state anxiety scores between two groups.
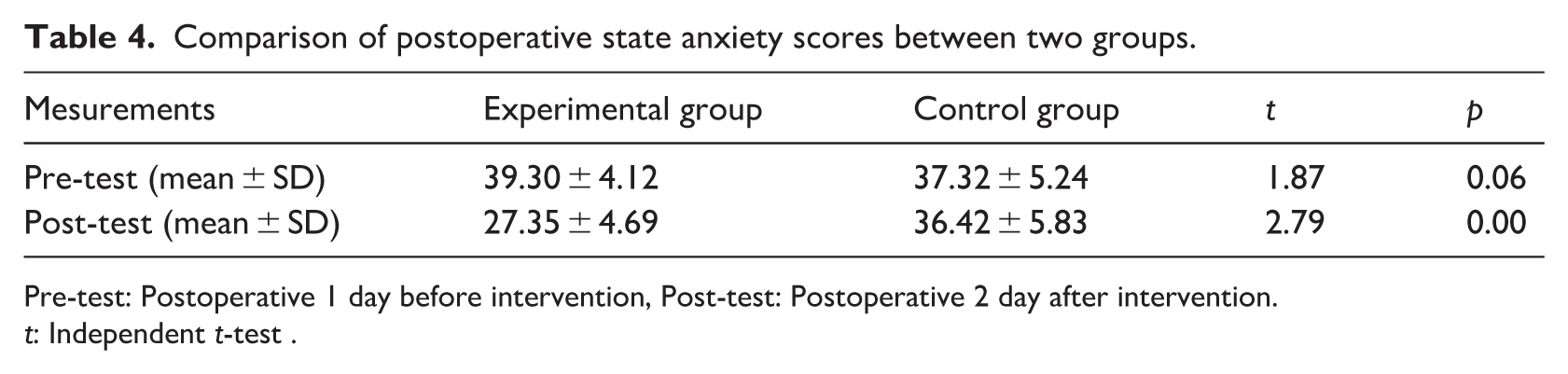
Pre-test: Postoperative 1 day before intervention, Post-test: Postoperative 2 day after intervention.
t: Independent t-test .
Comparison of the SUE Inventory scores within groups according to measurement times
The intragroup comparison of the postoperative SUE scale mean scores of the patients in the experimental and control groups is given in Table 5. The mean SUE score of the patients was −6.47 ± 1.30 in the experimental group before the EFT on the first postoperative day, the mean SUE score after the EFT on the first postoperative day was 7.47 ± 1.24, the mean SUE score before the EFT on the second postoperative day was −5.47 ± 1.69 and the mean SUE score after the EFT on the second postoperative day was 8.02 ± 1.16 and the differences between the groups were statistically significant (p < 0.05, Table 5). In addition, the mean SUE score of the patients in the control group on the first postoperative day was −6.02 ± 1.71 and the mean SUE score on the second postoperative day was −5.15 ± 1.94, and the difference in the mean scores was found to be statistically significant (p < 0.05, Table 5). This statistically significant change in the control group represents a minor clinical improvement that did not alleviate the patients’ negative emotional distress. Consequently, these individuals remained in a state of high stress and anxiety throughout the study period. According to Hartmann, individuals who are at −5 and −6 levels are in a state of high stress, anxiety and fear and cannot control their thoughts, cannot direct their attention and their reasoning abilities may be impaired. However, individuals who are at a +7 energy level have high self-esteem and good relationships, are successful, do energising work that can further increase their energy and are natural leaders for other people (Hartmann, 2021b).
Comparison of the SUE inventory scores within groups according to measurement times.
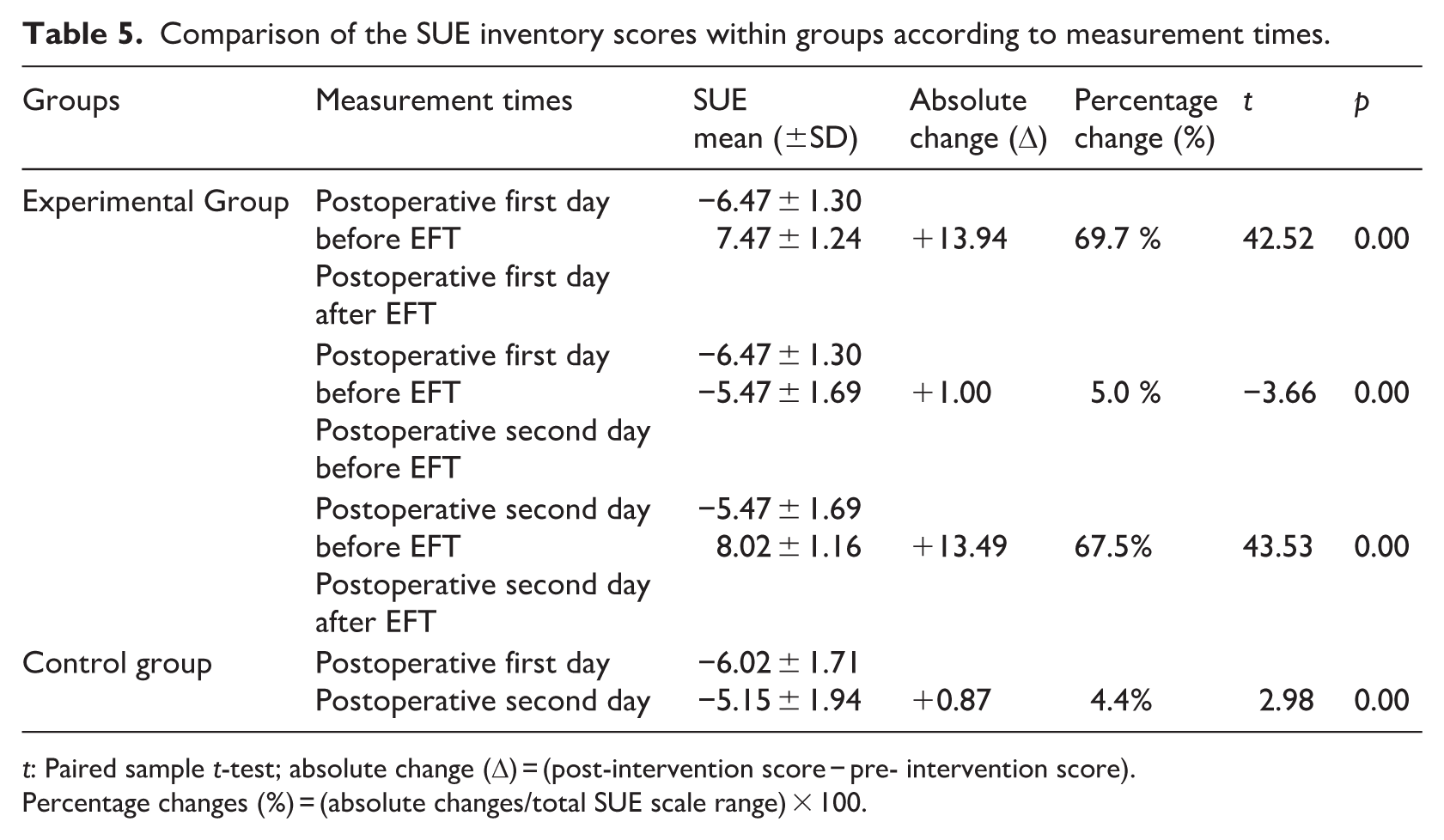
t: Paired sample t-test; absolute change (Δ) = (post-intervention score − pre- intervention score).
Percentage changes (%) = (absolute changes/total SUE scale range) × 100.
Furthermore, to clarify the immediate impact of EFT, both absolute change and percentage change were calculated. The magnitude of change in SUE scores was calculated as the difference between post-intervention and pre-intervention mean values (Δ = post–pre). Percentage change was calculated based on the total scale range of the SUE (−10 to +10; total range = 20 points) using the following formula: (absolute change/20) × 100. Since no pre-session/post-session measurements were obtained in the control group, the change in SUE scores for the control group was calculated as the difference between first- and second-day measurements. In the experimental group, an absolute change of 13.94 points, corresponding to 69.7% of the total SUE scale range, was observed immediately after EFT on the first postoperative day. A similar immediate effect was noted on the second postoperative day, with an absolute change of 13.49 points (67.5% of the total scale range). In contrast, the control group exhibited a minimal change of 0.87 points (4.4% of the total scale range) between the first and second postoperative days (p < 0.05, Table 5). These findings indicate that patients who received EFT experienced a large and immediate improvement in their emotional state following each session, shifting from high distress to a more positive and regulated emotional level. In contrast, patients in the control group showed only minimal change over time. Overall, this suggests that EFT may provide greater emotional relief during the postoperative period compared with standard care alone.
Discussion
The study was conducted to examine the effects of EFT on pain and anxiety in patients with total knee prostheses. EFT is a novel method used in the management of postoperative pain and anxiety, and there are a limited number of studies examining its effects on postoperative pain and anxiety (Ma’rifah et al., 2018; Padmapriya and Jenifer, 2020). It was determined in the present study that EFT application reduced postoperative pain and anxiety.
After total knee replacement, pain may make it difficult for patients to comply with the treatment and exercise programme. Patients may not want to move for fear of experiencing pain, and as a result, undesirable conditions such as complications and delayed recovery may develop. Furthermore, acute pain in the postoperative period can turn into chronic pain if it is not managed well (Kehlet et al., 2006; Macrae, 2001; Poobalan et al., 2003; Wang et al., 2016; Wylde et al., 2018). In the present study, the mean pain score of the patients in the experimental group was found to be statistically and significantly lower than in the patients in the control group. Although there are various studies in the literature investigating the effects of EFT on pain (Benor et al., 2017; Brattberg, 2008; Bougea et al., 2013; Church and Nelms, 2016; Stapleton et al., 2022), there are a limited number of studies examining its effects on postoperative pain (Padmapriya and Jenifer, 2020). In a previous study examining the effects of EFT on pain after major surgery, EFT was applied to patients 3 hours after the surgery, on the first and second postoperative days, and 93.3% of the patients in the experimental group and 86.7% in the control group reported severe pain before the postoperative EFT. After the EFT on the second postoperative day, 80% of the patients in the experimental group reported that they had no pain, but 83.3% of the patients in the control group reported that they had severe pain and 16.7% had moderate pain (Padmapriya and Jenifer, 2020). In a study comparing EFT and the finger relaxation technique to manage pain after caesarean section, it was reported that the greatest decrease in pain intensity was in the group in which the EFT was applied (Ma’rifah et al., 2018).
Anxiety, which is among the factors increasing postoperative pain levels, has negative effects on the patient’s postoperative recovery. For this reason, reducing the patient’s anxiety level after the surgery must be one of the nursing interventions. The non-significant difference in baseline Trait Anxiety Inventory (STAI-T) scores and State Anxiety Inventory (STAI-S) scores between the experimental and control groups (Table 2) confirms the groups’ homogeneity concerning baseline anxiety predisposition. The mean preoperative STAI-T and STAI-S scores indicate that the patients exhibited a ‘mild anxiety’ level according to the established scale criteria (Öner and Le Compte, 1998). This equivalence provides crucial contextual support for interpreting the observed post-intervention reduction in STAI-S as a result of the EFT application (Table 4). The mean postoperative STAI-S score was found to be statistically and significantly lower in patients in the experimental group than in patients in the control group in the present study. Previous studies similarly reported that EFT reduced anxiety. In a previous study that investigated the effects of EFT and music therapy applied before surgery on anxiety and vital signs, it was reported that EFT was more effective on anxiety compared to music (Cici and Özkan, 2022). In another study examining the effects of Hypno-EFT applied during venous blood collection on anxiety, it was found that EFT was effective in reducing anxiety (Navianti et al., 2018).
The rapid improvement in subjective emotional intensity observed following EFT may be explained by neurophysiological and cognitive mechanisms proposed in previous research. Stimulation of acupuncture points during EFT has been suggested to modulate neurochemical pathways by increasing serotonin levels and reducing cortisol and pain perception, thereby attenuating anxiety-related responses (Lane, 2009; Ulett, 1992). Elevated serotonin activity may influence amygdala functioning and enhance gamma-aminobutyric acid (GABA) transmission, contributing to anxiolytic effects and autonomic nervous system regulation. These neurochemical changes are thought to suppress the fight–flight–freeze response and may help explain the pronounced improvements in subjective emotional states observed following the intervention.
Furthermore, the psychological transition from negative to positive SUE levels can be explained by the ‘positive energy’ component of the intervention (Hartmann, 2021a). The clinical impact of this strategy is shown by the profound shifts observed in recent literature. Özşahin et al. (2025) demonstrated that EFT application for premenstrual syndrome (PMS) led to a significant change in SUE scores from a negative baseline (−5 ± 3.1) to a positive state (7.8 ± 1.7) and resulted in significant reductions in PMS symptoms such as anxiety and pain compared to control groups (Özşahin et al., 2025). Similarly, Okyay and Uçar (2023) found that EFT sessions significantly increased SUE scores from −5.85 ± 1.72 to 1.91 ± 3.23, which was associated with decreased salivary cortisol levels and enhanced psychological well-being (Okyay and Uçar, 2023). These findings mirror our results, where a positive shift in SUE scores directly corresponded to improved mental states and reduced pain intensity. Such a cognitive shift encourages the mind to move away from the perception of physical distress, thereby relieving both anxiety and discomfort. In the high-stress context of total knee replacement surgery, this combination of somatic calming and cognitive reframing provides a more comprehensive level of relief than standard care alone, further supporting the synergy between psychological interventions and surgical recovery (Cici and Özkan, 2022).
Strengths and limitations
The strengths of the present study include being the first randomised controlled trial to examine the effects of EFT on pain and anxiety levels of patients undergoing total knee arthroplasty. To ensure sufficient statistical power, the sample size was determined using an a priori power analysis indicating a power of 90%. Additionally, a post hoc power analysis confirmed that the achieved statistical power was 94%.
However, the study also had some limitations. One of the limitations of the study was that it was conducted in one single centre with patients who had total knee replacement surgery in the orthopaedics clinic of a state hospital. For this reason, the study results can only be generalised to the patients in the sample group who have the specified characteristics. A limitation of the study was the procedural complexity and the requirement for active participant engagement in the structured steps of EFT. The intervention requires patients to focus their attention, close their eyes and repeat specific statements, which created a certain level of participant burden. This led to some attrition among patients who were unwilling to adhere to the multi-step procedure. It is important to note that this challenge reflects issues related to participant adherence and engagement rather than intervention fidelity.
A significant limitation regarding the generalisability of the findings is the small number of male participants included in the study. Epidemiological studies indicate a higher prevalence of knee osteoarthritis and, consequently, a higher rate of total knee arthroplasty among women compared to men (Bakılan and Özgen, 2021; Segal et al., 2024). Due to the low number of male patients in our sample, the results may not be generalisable to the male population. Therefore, further research with a larger and more balanced male cohort is needed to validate the effectiveness of EFT in men.
One of the limitations of the study was that potential confounders such as the type of anaesthesia administered during surgery and the type and frequency of postoperative analgesia were not controlled for. We acknowledge that disregarding these factors may have influenced anxiety and pain outcomes independently of EFT. One of the major methodological limitations of this study is that the researcher who delivered the intervention also conducted the outcome assessments, which may limit the independence and objectivity of the evaluation. Due to the nature of the EFT intervention – which requires active somatic and verbal engagement – neither the practitioner nor the participants could be blinded. This lack of blinding may have introduced observer expectancy bias and social desirability bias, and participants’ awareness of group allocation may have contributed to expectancy and placebo effects on the self-reported outcomes.
Consequently, the observed reductions in pain and anxiety may not be solely attributable to the intervention itself. Future studies should preferably adopt double-blind designs when feasible, including blinded outcome assessors and, if possible, placebo control conditions, to minimise treatment effect bias and other these sources of bias. Furthermore, the inclusion of objective physiological measures such as cortisol levels and heart rate variability, in addition to subjective instruments, would help to balance this limitation and strengthen the validity of future findings.
A significant limitation of this study is the reliance on the SUE scale. Although the SUE scale functions similarly to a single-item, self-report magnitude scale, such as the widely accepted Numerical Rating Scale, independent, peer-reviewed literature reporting its comprehensive construct validity and reliability is scarce. Furthermore, the SUE measure’s association with The Guild of Energists introduces potential transparency issues and raises concerns regarding the measure’s objectivity. Consequently, the results based on the SUE scale should be interpreted with significant caution and considered secondary to the outcomes derived from validated measures (VAS, STAI-S).
Future research should prioritise the use of established, fully validated anxiety measures or conduct a formal concurrent validation study for SUE against known psychometric standards.
Implications
Nevertheless, these findings offer valuable implications for the future of orthopaedic nursing and holistic patient care. Regarding nursing education, the integration of energy psychology techniques like EFT into the curriculum could provide future nurses with evidence-based, non-pharmacological tools to manage acute surgical distress. In nursing practice, EFT can be utilised as a cost-effective, bedside intervention to provide immediate emotional relief, particularly during the high-stress early postoperative period. To enhance healthcare delivery, establishing standardised nursing protocols that incorporate EFT alongside conventional pain management could promote a more comprehensive, biopsychosocial approach to recovery. Finally, further research should prioritise multi-centre designs with larger, more balanced cohorts and objective physiological measures to strengthen the validity of energy-based interventions.
Conclusion
In conclusion, this study provides novel evidence as the first randomised controlled trial to demonstrate that EFT is effective in reducing postoperative pain and anxiety in patients undergoing TKA. By demonstrating meaningful improvements in both physical and emotional outcomes during the early postoperative period, the findings highlight the potential value of EFT as a scalable, non-invasive and cost-effective nursing intervention. The nurse-led nature of the intervention aligns with holistic and patient-centred nursing care models, reinforcing the role of nurses in addressing both physiological and psychological dimensions of postoperative recovery.
In addition, this research supports a shift towards more holistic, autonomous nurse-led care models that recognise patients’ psychological and physiological responses as interrelated dimensions of the recovery process. By addressing the emotional impact of surgery through a biopsychosocial lens, EFT may enable nurses to deliver timely, independent interventions that enhance the quality of recovery. The integration of such energy-based techniques into formal nursing protocols represents a promising opportunity for healthcare policies to promote cost-effective, patient-centred and comprehensive postoperative management strategies in orthopaedic settings.
Key points for policy, practice and research
EFT is a non-invasive and cost-effective intervention that reduces pharmacological reliance, facilitates earlier mobility and supports faster hospital discharge, serving as a valuable postoperative option.
This research encourages policymakers to consider the broader integration of EFT in healthcare settings to improve the quality of patient care.
This approach encourages nurses to incorporate EFT as a distraction technique in their clinical practice to enhance the overall experience of orthopaedic patients.
This study highlights the need for further research on the application of EFT as a distraction method in patients undergoing other types of surgical procedures.
Footnotes
Acknowledgements
The authors would like to thank Atatürk University Coordination Unit of Scientific Research Projects for supporting the study with project number TYL-2022-10264.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Atatürk University the Coordination Unit of Scientific Research Projects with project number TYL-2022-10264.
Ethics approval
Before starting the study, the ethical board (25.11.2021 with decision number 67) has been taken from Atatürk University, the Clinical Research Ethics Committee of Faculty of Medicine. The patients voluntarily accepting to participate in the study have been included. Verbal and written permission of the patients have been taken after giving necessary explanations. Participants have been told that they could leave the study process whenever they want. The attained data and the identity of the answerer have been specified to be kept confidential. Because it is necessary to protect the individual rights, Human Rights Helsinki Declaration has been respected during the study.
Trial registration
Data availability statement
The data underlying this article cannot be shared publicly due to ethical/legal reasons.