
Abstract
Background:
Web-based self-care education can improve health outcomes in patients with chronic conditions.
Aims:
This study aimed to examine the impact of a web-based self-care programme based on Orem’s model on the health-promoting behaviours of patients with multiple sclerosis (MS).
Methods:
The study included 91 MS patients, randomly assigned to control (n = 46) and experimental (n = 45) groups using block randomisation. The control group received standard care, whereas the experimental group participated in a web-based self-care education programme. Data were collected using demographic questionnaires, educational needs checks and Walker’s Health-Promoting Lifestyle Profile, then analysed using SPSS-26 with statistical tests (p < 0.05).
Results:
Before the programme, the average health-promoting behaviours score in the two groups did not differ significantly (p > 0.05). After the programme, the experimental group’s health-promoting behaviours score increased from 109.97 ± 13.78 to 119.97 ± 13.44, whereas the control group showed almost no change (110.83 ± 13.25 to 111.72 ± 13.05). Post-programme scores were significantly higher in the experimental group compared with the control group (p = 0.002).
Conclusions:
The web-based self-care education programme positively affects the health-promoting behaviours of patients with MS. It is recommended as an effective approach to improve health-promoting behaviours in patients with chronic conditions.
Keywords
Introduction
Chronic diseases affect people at all stages of their lives (Casariego et al., 2019). Multiple sclerosis (MS) is a chronic and progressive disease of the central nervous system that damages the myelin of the nerves of the brain and spinal cord. MS is the second leading cause of neurological disability among young adults globally (Oh et al., 2018). Iran has the highest rate of MS among Middle Eastern countries (Mousavizadeh et al., 2018; Safian et al., 2020). Despite advances in medical science in recent years, there is no definitive cure for MS. However, pharmacological and non-pharmacological care can help manage the symptoms of the disease and slow its progression (Dahmardeh et al., 2017; Reidy et al., 2025). Among non-pharmacological methods, self-care education plays an important role in helping patients adapt to the complications of the disease (Karimlou et al., 2019). Self-care is one of the basic concepts in nursing care and leads to favourable outcomes in securing, maintaining and encouraging the health of individuals (Nascimento et al., 2021). Self-care programmes are a crucial component of treatment and play an essential role in the management of MS (Demaille-Wlodyka et al., 2011; Wilski et al., 2021). According to evidence, the use of self-care leads to favourable outcomes and better control of the symptoms of the disease (Khodaveisi et al., 2018; Valizadeh et al., 2017). Various methods and approaches have been developed over time to improve the self-care skills of patients. One of the relevant nursing conceptual models in this field is related to the studies and efforts of Dorothea Orem.
The Orem Self-Care Model is one of the most complete nursing models in the field of self-care (Alligood and Hardin, 2025; Hasanpour-Dehkordi, 2016; Rostami et al., 2015). The goal of this model is to help patients take care of themselves. In this model, nurses play a key role in checking self-care needs, finding out patient abilities and identifying self-care deficiencies (Meleis, 2018; Nasiri et al., 2023). In Orem’s theory, education is stressed as a vital part of nursing’s professional responsibilities and one of the basic rights of patients (Acton and Malathum, 2000; Hartweg and Metcalfe, 2022). Self-care education is essential for helping patients adapt to and manage the changes brought on by their disease. To help individuals adopt health-promoting behaviours, they should be encouraged to face the challenges of MS in a constructive manner and remain active members of society (Pourhaji et al., 2024; Prescott et al., 2007).
This study is based on Orem’s Self-Care Deficit Nursing Theory. The theory says that nursing is needed when patients have a self-care deficit – when they cannot meet their own healthcare needs (Smith, 2019). It organises nursing practice around identifying these problems and creating nursing systems to help patients (Alligood and Hardin, 2025). For this trial, the web-based programme was designed and delivered by the research team as a supportive-educative nursing system based on Orem’s theory. It aimed to improve the self-care agency of patients with MS by addressing their specific self-care deficits.
The management and impact of chronic diseases, including MS, can be strongly affected by health-related and health-promoting behaviours (Zhang et al., 2023). Healthy behaviours – such as maintaining a proper diet, doing regular exercise, managing weight and avoiding smoking – play a vital role in promoting overall health and well-being in patients with chronic conditions (Jung et al., 2021). Therefore understanding health-promoting behaviours is important for intervention planning (Van Hijfte et al., 2022; Wood et al., 2015). Technology has been shown to be an opportunity to increase knowledge and learn new skills (Nadri et al., 2020). Current disease management models highlight the importance of combining technology with health interventions to improve the effectiveness of care and enhance quality of life (Chen et al., 2022).
Web-based education is one of the new methods in this field (Ahmadi et al., 2021). This method helps to save time and money by providing attractive content, more learner participation and the possibility of learning anytime and anywhere (Mortazavimoghaddam et al., 2021). In a web-based educational intervention, learners can access and engage with the provided content more easily through various digital formats, including videos, multimedia presentations, text, audio, visual materials, online webinars and other electronic content delivery methods. They also benefit from the flexibility to access and study the materials at their own pace and at convenient times (Green et al., 2022; Matarese et al., 2017).
According to a review of scientific literature, no study has been done to evaluate the impact of a web-based self-care education programme on the health-promoting behaviours of patients with MS. However, the evidence has given important knowledge in this area. For example, research has shown that a self-care programme based on the Orem model, tailored to the educational needs of patients, works as an effective, non-invasive and low-cost nursing intervention that positively affects the levels of fatigue and daily activities of individuals with MS (Dahmardeh et al., 2016; Nasiri et al., 2023). Another study showed that a web-based cognitive behavioural therapy programme in people with MS led to important improvements in depression and fatigue in people with the disease (Siengsukon et al., 2021). Davenport et al. (2024) also showed that health behaviour modification helps mental health outcomes, such as depression and anxiety, in the MS population. A study by Safian et al. (2020) found that the use of mobile-based self-care programmes effectively improves the balance of patients with MS. Finally, Bevens et al. (2022) demonstrated that a web-based educational programme targeting health-related behaviours is a feasible and effective tool for delivering educational content to people with MS via the Internet. These programmes can serve as a useful supportive knowledge base for disease management and the building of self-care skills.
Considering the above, it can be concluded that MS is one of the most challenging chronic diseases to manage. Carrying out a comprehensive self-care programme tailored to patients’ needs appears to improve their health. This study aimed to evaluate the impact of a web-based self-care programme created based on Orem’s model on the health-promoting behaviours of MS patients.
Methods
Design and setting
This study was a randomised clinical trial with a before-and-after design including a control group. The study was conducted from 28 September to 20 December 2024, at a large teaching hospital known as the main centre for providing care to patients with MS. This study was reported in accordance with the consolidated standards of reporting trials (CONSORT) guidelines (Schulz et al., 2010). The completed CONSORT checklist is provided as Supplemental Material. The trial was registered at the Iranian Registry of Clinical Trials (IRCT20240811062717N1). The study protocol is available in the registry; the statistical analysis plan is available from the corresponding author upon request. No changes were made to the protocol after commencement. The trial ended as planned after reaching the target sample size and follow-up.
Participants
The participants in this study were patients with MS who were referred to a specialised neurology clinic. A convenience sampling approach was used for recruiting participants; all eligible and available patients from the clinic during the study period were invited to take part. This method was used to easily access the target population.
Sample size calculation, based on Rakhshani et al. (2022), with μ1 = 31.72, μ2 = 35.06, SD1 = 15.01, SD2 = 14.51, α = 0.05, and 80% power, showed that 48 participants per group were needed, including 20% for possible dropouts.
Inclusion criteria for the study were: a diagnosis of MS by a neurologist based on clinical and laboratory criteria, the patient’s clear understanding of their diagnosis, the ability to read and write, being over 18 years of age, at least 6 months since diagnosis, the ability to perform self-care activities, and access to a smartphone or personal computer.
Exclusion criteria were: participation in other educational interventions at the same time as this study, missing or not actively taking part in at least two educational sessions, transfer of participants to medical centres outside of the study area, and having a background in medical education or being a student in health care related fields.
Neither patients nor the public were involved in the design of this study. The intervention was delivered by the principal investigator (S.A.), a registered nurse with a Master’s degree. A total of 96 patients were checked for meeting the inclusion criteria, of which 5 were excluded from the study due to illiteracy.
Randomisation
Participants were assigned via computer-generated block randomisation (block size: 6). An independent statistician prepared sequentially numbered, opaque, sealed envelopes to ensure allocation concealment. After baseline assessment, a research assistant (not involved in recruitment) opened the next envelope in sequence to assign the participant to either the experimental (n = 45) or control (n = 46) group. A detailed diagram of participant flow through the trial is presented in Figure 1.
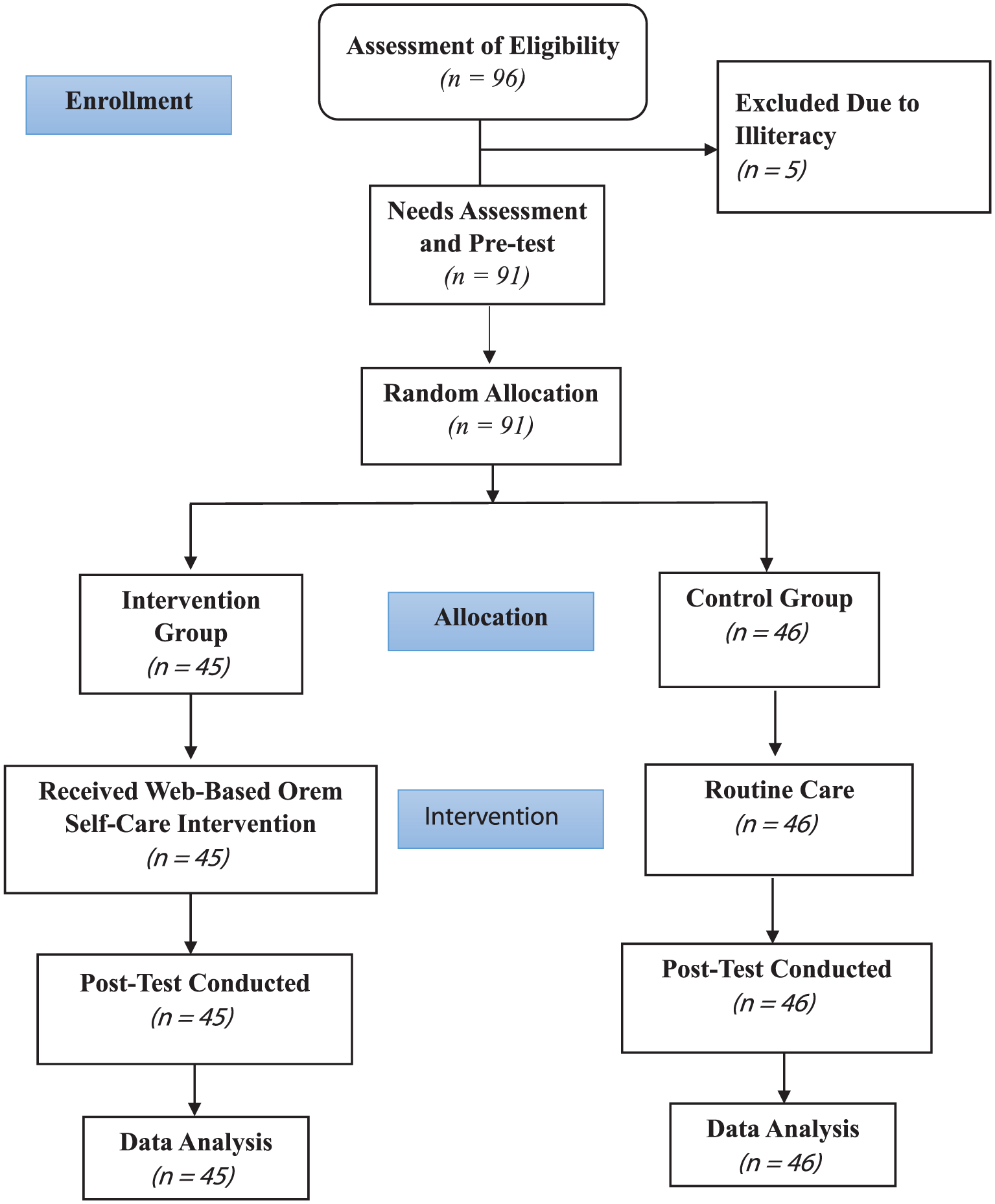
CONSORT flowchart of the study.
Intervention
At the beginning of the study, the self-care needs related to lifestyle and the self-care status of patients in both the experimental and control groups were evaluated using the self-care needs assessment questionnaire based on the Orem model (Seyednazari et al., 2025). Additionally, participants completed the Walker lifestyle questionnaire (HPLP-II) (Mohammadi Zeidi et al., 2012) and a personal characteristics form. The results of this needs assessment served as the basis for designing the educational content.
The intervention took place over a 4-week period, with three web-based sessions each week. The educational content was delivered asynchronously through pre-designed, structured multimedia materials (text, infographics, videos) hosted on the website. There were no live digital meetings; participants could access and study the materials at their own pace within each weekly module. To deliver the intervention, a dedicated website was developed under the direction of the research team at https://fightwithms.ir. The research team designed all educational content and structure, and a professional web developer was contracted for technical implementation. Participants in the experimental group were instructed on how to use the website, and each accessed the tailored educational content by creating a unique username and password.
Our research team designed the educational content and programme structure based directly on Orem’s theory. The initial needs assessment identified specific self-care problems across Orem’s three categories of self-care needs. The complete theoretical framework and mapping of all educational content to Orem’s self-care needs are visually summarised in Figure 2.
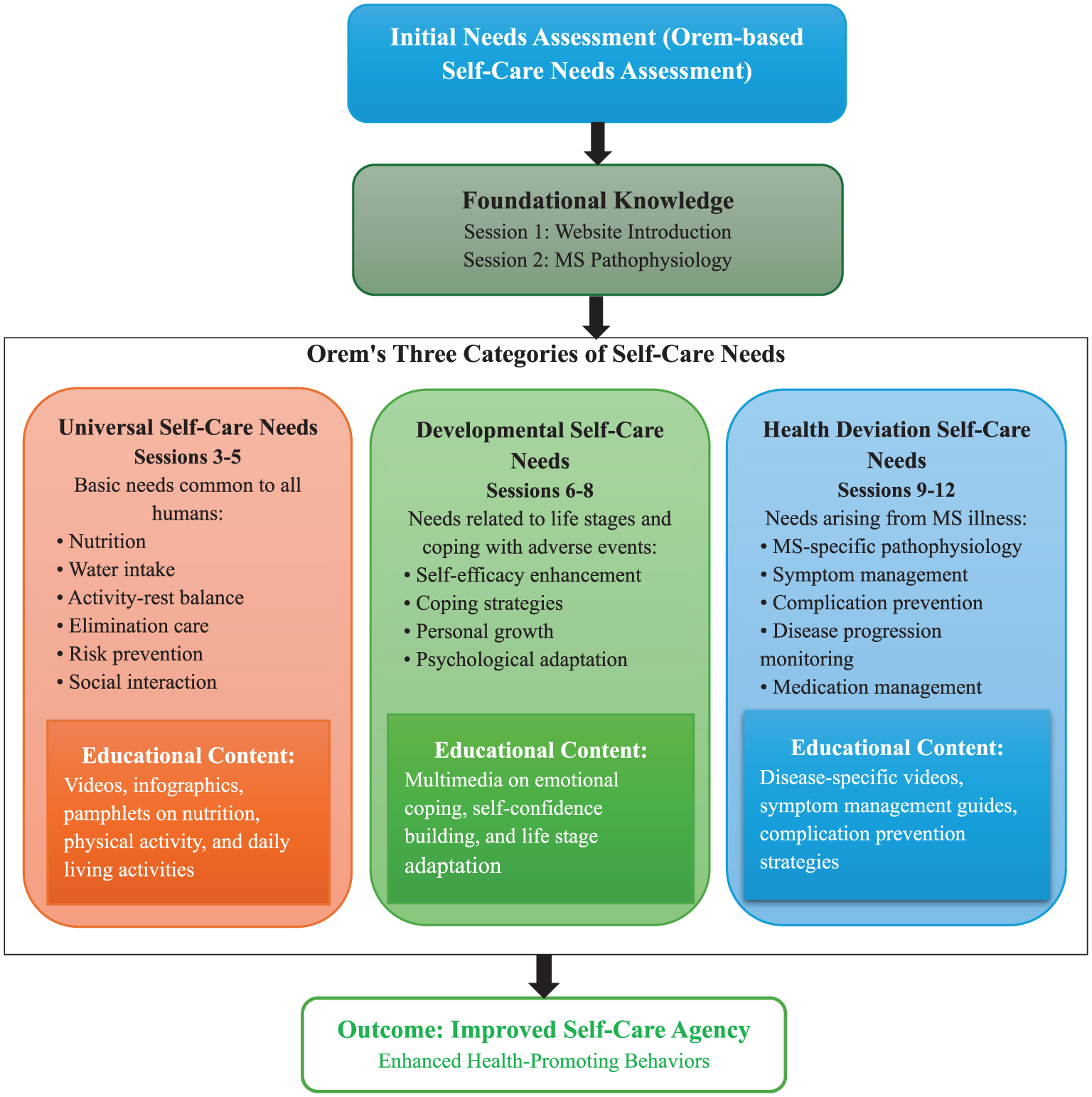
Structure and content of the web-based self-care education programme based on Orem’s model.
Content validity was checked (CVI = 0.92) by five experts (neurologists and MS-specialised nurses), and usability was pilot-tested (score: 4.3/5). Based on the pilot feedback, minor technical adjustments were made to improve user interface navigation, whereas the validated educational content remained unchanged. The post-test assessment was done immediately after the end of the 4-week intervention. So, the total time from baseline measurement to post-intervention follow-up was 4 weeks.
No specific adverse events were anticipated from the educational intervention; therefore, systematic harm monitoring was not implemented.
To make effective communication easier, the study nurse’s contact number was provided at the bottom of each page, allowing patients to contact directly with any questions. The intervention was delivered and monitored by the principal investigator S.A., who is a registered nurse with a Master’s degree in Nursing and a member of the research team. To prevent information contamination, participants were told not to share the educational content with others.
The content and structure of the intervention are presented in Table 1.
Structure and content of the web-based educational intervention.
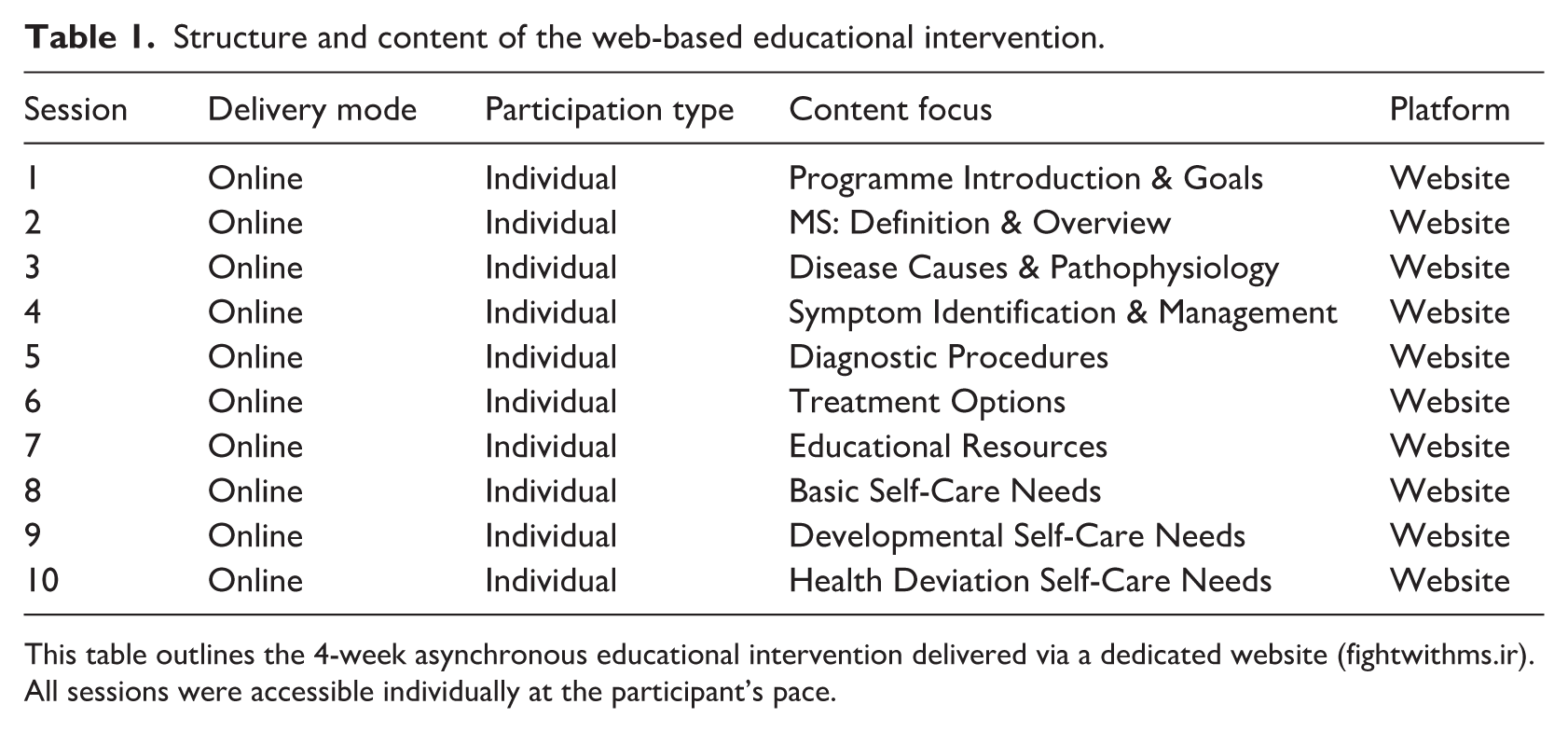
This table outlines the 4-week asynchronous educational intervention delivered via a dedicated website (fightwithms.ir). All sessions were accessible individually at the participant’s pace.
Control group intervention
The control group did not receive any intervention from the research team. They only received routine care from the centre (including outpatient visits to the clinic for drug injections, receiving pamphlets, periodic visits and guidance from a neurologist). At the end of the study period, similar to the experimental group, the lifestyle questionnaires were completed again by the control group. Following completion of the post-test assessment, and in adherence to ethical principles, participants in the control group were granted full access to the web-based self-care education programme at the end of the study period.
Study instruments
Three instruments were used to collect data:
Demographic questionnaire: included information about age, gender, place of residence, duration of MS, education level, employment status, marital status, positive family history of MS and presence of medication side effects.
Self-Care Needs Assessment Form: To check patients’ self-care needs based on the Orem model, a needs assessment form developed and validated by Seyednazari et al. (2025) was used. This form included three dimensions of basic, developmental and health-related needs and contained questions about vital signs (e.g., blood pressure and heart rate), fluid intake, dietary habits, oral and dental care, sleep, activity level, defecation status, self-awareness, self-confidence, body image, social interactions and occupational and residential status. It is a 23-item Orem-based Self-Care Needs Assessment with established validity (content validity index/CVI = 0.89) and reliability (ICC = 0.86 via test–retest; Seyednazari et al., 2025).
Walker’s Health-Promoting Lifestyle Profile II (HPLP-II): This questionnaire has 52 questions in 6 dimensions (nutrition, physical activity, health responsibility, stress management, interpersonal relations and spiritual growth). The response range used a 4-point Likert scale (1 = never to 4 = routinely). The total score ranges from 52 to 208, with higher scores indicating better engagement in health-promoting behaviours. The reliability of the Persian version questionnaire in the study by Mohammadi Zeidi et al. (2012) using Cronbach’s alpha for different dimensions was reported to be between 0.79 and 0.91.
The primary outcome was the total HPLP-II score. Secondary outcomes included its six subscale scores (nutrition, physical activity, health responsibility, stress management, interpersonal relations, and spiritual growth).
Data analysis
Outcome assessors were blinded to group allocation, and data were analysed by a statistician using coded identifiers (Group A/B). Data analysis in SPSS version 26 (IBM Corp., Armonk, NY, USA) was used for data analysis. included descriptive statistics, Shapiro–Wilk normality tests, independent/paired t-tests, chi-square tests and Cohen’s d for effect size (α = 0.05).
To check the homogeneity of the groups, the chi-square test was used for qualitative variables (such as gender, marital status, education, occupation, and presence of drug complications), whereas the independent t-test was applied to quantitative variables (including age and duration of illness). To assess the effect of the web-based self-care intervention on lifestyle: a paired t-test was used to compare the means before and after the intervention in each group, and an independent t-test was used to compare the means between the two groups. A significant level of 0.05 was applied to all tests.
All analyses followed the intention-to-treat principle, including all randomised participants. No interim analyses were performed. Due to the nature of the intervention, participants were not blinded to group assignment. Exploratory analyses of the six HPLP-II subscales were conducted. De-identified data are available from the corresponding author upon reasonable request.
Ethical approval
Ethical approval for this study was obtained from the Ethics Committee of Zanjan University of Medical Sciences (approval code: IR.ZUMS.REC.1403.151), and the trial was registered at the Iranian Clinical Trial Centre (IRCT20240811062717N1). We confirm that all experiments involving human participants were carried out in accordance with the relevant ethical guidelines and regulations. In this study, after explaining the objectives, subject matter, training and how the study would be done, the researcher assured participants that their information would remain confidential, fully following the principle of anonymity throughout the course of the study. Written informed consent was obtained from all participants. Participation in the study was voluntary.
Results
The findings showed no significant differences between the experimental and control groups before the intervention with respect to gender, marital status, duration of illness and other demographic variables (p > 0.05), indicating baseline comparability between the two groups (Table 2).
Demographic and clinical characteristics of participants at baseline.
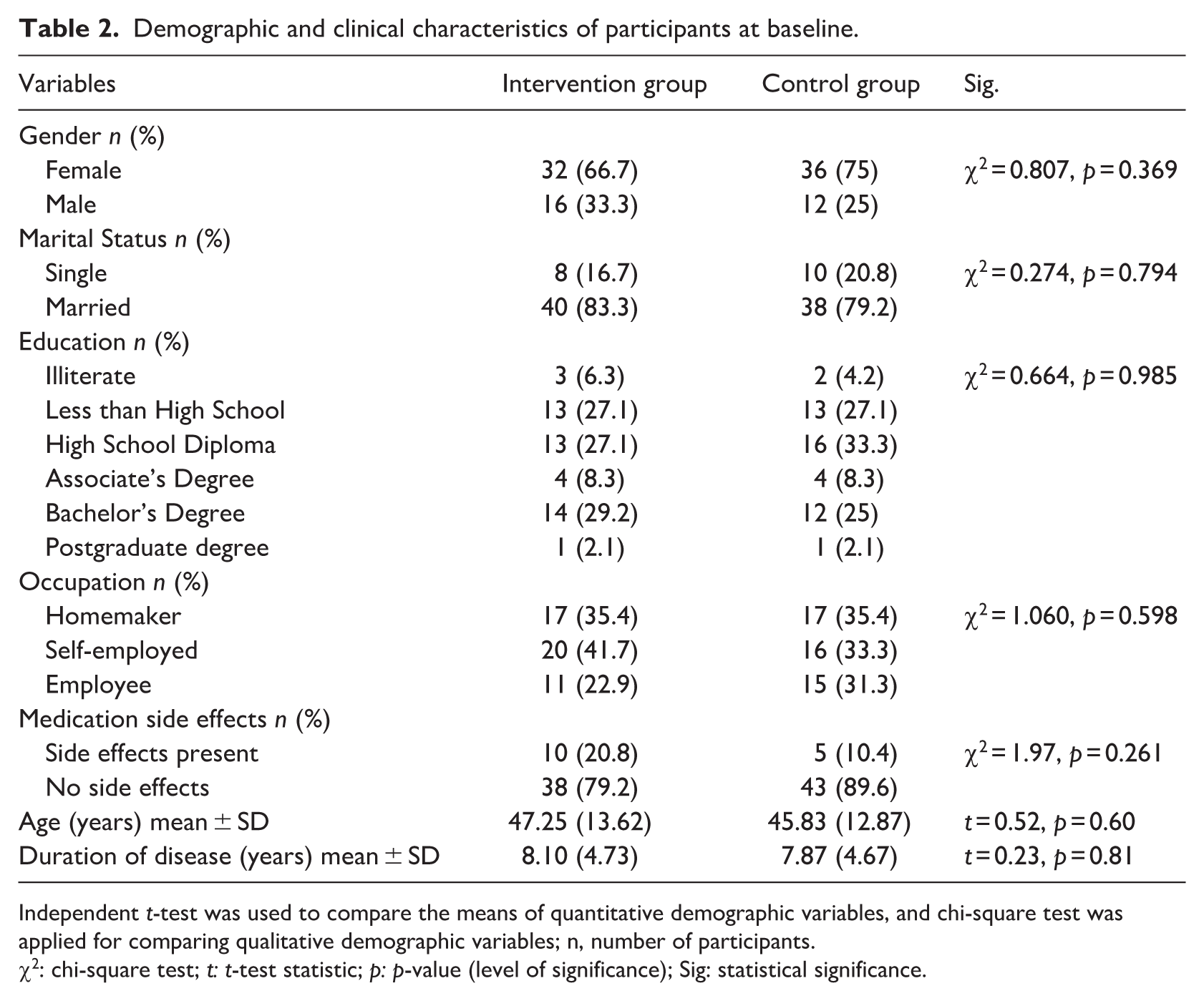
Independent t-test was used to compare the means of quantitative demographic variables, and chi-square test was applied for comparing qualitative demographic variables; n, number of participants.
χ2: chi-square test; t: t-test statistic; p: p-value (level of significance); Sig: statistical significance.
As shown in Table 3 and Figure 3, no significant difference was observed in mean health-promoting behaviours scores between the experimental and control groups before the intervention (p = 0.620). Following the intervention, a significant improvement in overall health-promoting behaviours was observed in the experimental group compared with the control group (p = 0.002), whereas no significant change was found in the control group (p = 0.490). The between-group effect size for the intervention was moderate (Cohen’s d = 0.62).
Comparison of patients’ health-promoting behaviours scores before and after the intervention in the intervention and control groups.
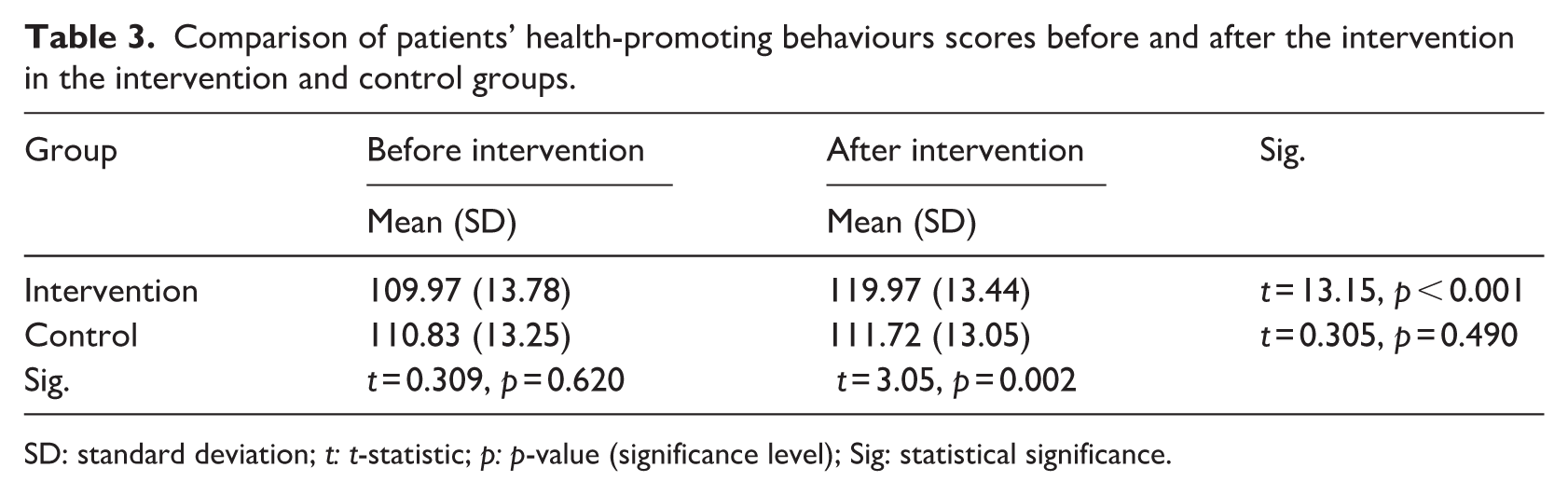
SD: standard deviation; t: t-statistic; p: p-value (significance level); Sig: statistical significance.
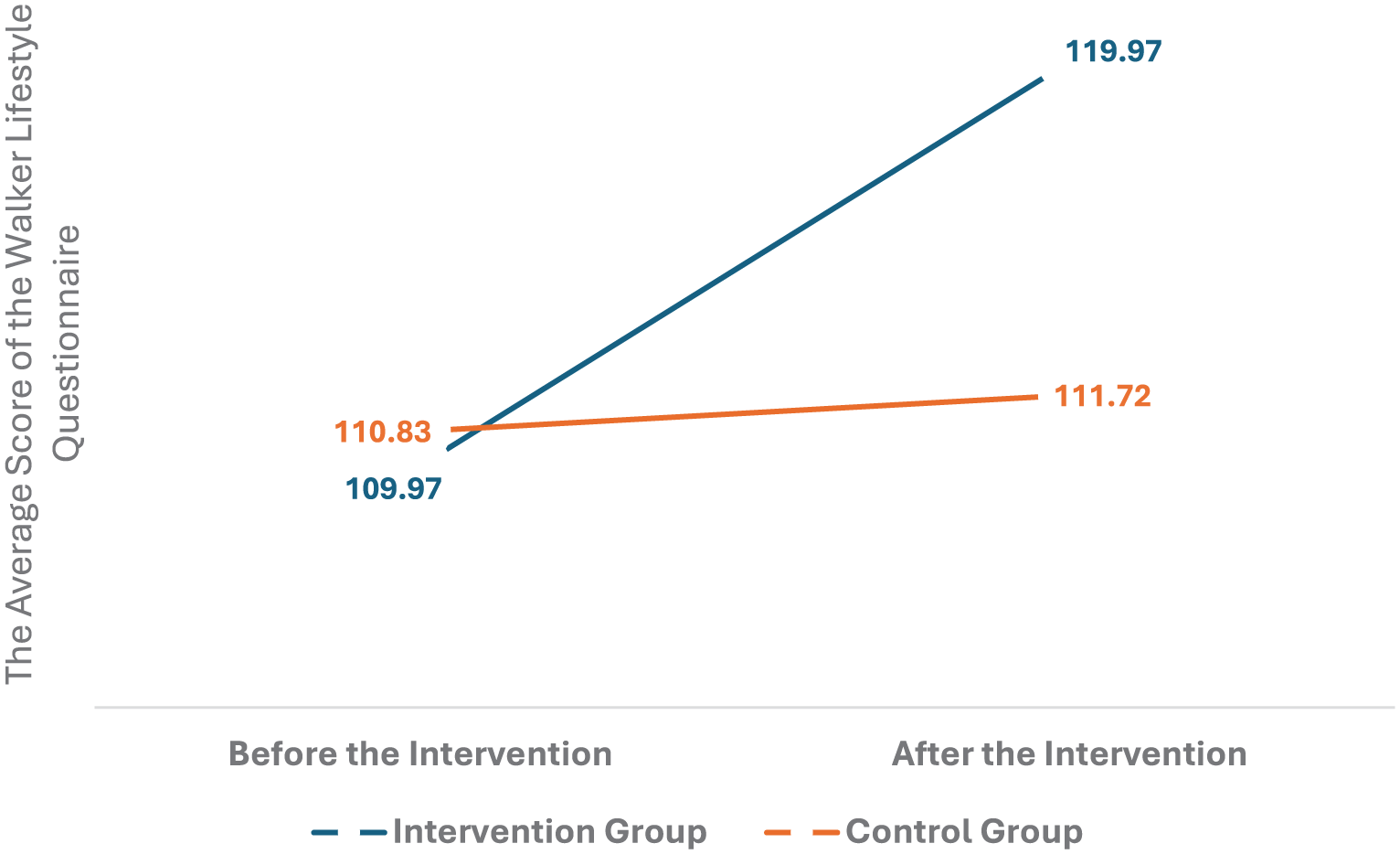
Changes in overall lifestyle scores in the two groups before and after the intervention.
Regarding programme engagement and accessibility, all participants in the intervention group successfully accessed and completed the web-based modules, with no attrition. The integrated chat facility was actively used, with an average of 2.3 (±1.1) contacts per participant over the 4-week period. Most queries were related to exercise safety and planning, stress and fatigue management, medication adherence and daily self-care strategies, whereas fewer questions addressed nutrition and interpersonal relationships. No technical barriers preventing access were reported. No adverse events were reported during the trial.
Further analysis of post-intervention outcomes revealed differential effects across specific health-promoting behaviours. Significant between-group differences were observed in health responsibility (p = 0.017), stress management (p = 0.012) and physical activity (p = 0.023). In contrast, no statistically significant differences were found between the intervention and control groups for spiritual growth, interpersonal relations or nutrition following the intervention (p > 0.05).
All participants allocated to the intervention group completed the web-based education programme, and no attrition was observed during the study period.
Discussion
The present study shows that web-based self-care education grounded in Orem’s self-care theory does not uniformly affect all health-promoting behaviours among people with MS. Rather, the intervention produced selective improvements, with significant gains observed in health responsibility, stress management and physical activity. These behaviours are closely linked to daily self-regulation and may be more amenable to short-term, skill-based educational interventions delivered via digital platforms.
In contrast, domains such as spiritual growth, interpersonal relations and nutrition did not show significant changes following the intervention. These behaviours may be affected by deeply rooted personal values, social contexts or long-standing habits that need longer intervention durations or more intensive, personalised support to achieve meaningful change.
The pattern of participant engagement through the chat facility further supports these findings, as most queries were related to physical activity, stress management and symptom-related self-care, with relatively few questions addressing nutrition or interpersonal relationships.
Orem’s theoretical framework emphasises patient autonomy in healthcare management. The theory encourages self-care behaviours that support independence and empowerment (Libster, 2008). Previous research has shown that self-care interventions can significantly improve quality of life and functional outcomes for individuals with MS (Davenport et al., 2024; Safian et al., 2020).
The current findings align with existing literature on self-care interventions for MS patients, both traditional and web-based approaches. Dahmardeh et al. (2016) Effect of a programme based on the Orem self-care model on sleep quality of patients with multiple sclerosis. Similarly, Safian et al.’s (2020) research highlighted the benefits of mobile phone-based self-care programmes in improving balance among individuals with MS – a key factor for maintaining functional independence.
Web-based self-care education offers several distinct advantages over traditional methods, including improved accessibility, convenience, patient engagement and self-paced learning (Ahmadi et al., 2021; Hooshmandja et al., 2019). In our study, these advantages were reflected in the high completion rate, active use of chat support and absence of access barriers, as detailed in the results. This approach allows patients to overcome common barriers such as scheduling constraints and geographic limitations, whereas multimedia content and virtual support networks can enhance the learning experience and encourage adherence (Mortazavimoghaddam et al., 2021). In addition, web-based interventions show particular suitability for scalability. Unlike traditional face-to-face programmes that need significant resources and complex logistical coordination, online programmes can reach broader audiences with reduced costs and time investments. This potential for scalable, cost-effective delivery aligns with global health strategies that advocate for digital tools to strengthen chronic disease management and improve health equity (World Health Organization, 2025). By empowering patients with self-management skills and providing continuous support, such interventions have the potential to reduce the economic burden of MS by preventing complications and decreasing unplanned healthcare use. Moreover, they can directly address health disparities by delivering specialised education and support to patients in remote or underserved areas who may have limited access to traditional in-person services. This approach becomes particularly important for chronic conditions like MS, which need ongoing education, support and timely intervention to prevent complications and improve long-term outcomes (Prescott et al., 2007; Safian et al., 2020). However, this digital approach also presents a critical challenge: technological accessibility and the digital divide (as noted in the limitations). Although our programme was designed for flexibility, its digital nature may exclude populations with limited internet access, device availability or digital literacy – an issue noted in web-based health intervention research (Hooshmandja et al., 2019). In addition, the successful integration of such web-based models into routine care needs healthcare professionals, particularly nurses, to be equipped with corresponding digital competencies to guide patients and manage these platforms effectively. The integration of Orem’s self-care theory with modern technology provides a coherent framework that addresses both theoretical foundations and practical implementation considerations.
Strengths and limitations
This study has several strengths, including its randomised controlled design, theory-driven intervention based on Orem’s model, use of validated outcome measures and excellent participant retention with no attrition. However, some limitations should be considered. The convenience sampling from a single centre may limit generalisability. Self-reported measures (HPLP-II, Orem-based assessments) are susceptible to recall and social desirability bias. The short 4-week follow-up period precludes assessment of long-term effect maintenance. The digital delivery format may have excluded populations with limited technological access or literacy (the digital divide). In addition, we did not stratify by MS clinical subtypes – relapsing-remitting MS (RRMS), primary progressive MS (PPMS) and secondary progressive MS (SPMS) – or disability levels using measures like the Expanded Disability Status Scale (EDSS), limiting insights into differential effects across disease stages. Finally, potential contamination between groups cannot be entirely ruled out.
Implications
The findings of this study carry important implications for both clinical practice and health policy. For nursing practice, this web-based, theory-driven programme provides a scalable model for combining structured self-care education into standard care for patients with MS and other chronic conditions. It empowers nurses to move from traditional, episodic patient education to a continuous, supportive-educative role, using technology to extend their reach beyond clinical settings. For health policy, our results support the inclusion of digitally delivered, evidence-based self-care programmes in national chronic disease management frameworks and reimbursement models. Investing in such interventions can reduce healthcare costs related to disease complications and hospital readmissions, while also dealing with health disparities by making access to specialised care better for patients in remote or underserved areas. In addition, policymakers and healthcare institutions should support the development of digital competencies among nurses to make the effective use of such innovative care models easier.
Conclusions
This randomised controlled trial shows that a web-based self-care education programme, based on Orem’s theory, is an effective intervention for improving health-promoting behaviours of patients with MS. The significant improvement in health-promoting behaviours scores highlights the value of combining theory-driven, digital tools into nursing care within chronic disease management.
Based on our findings, we recommend the adoption of this web-based programme as a scalable and accessible part of standard nursing care for MS patients. For future research, investigations with longer follow-up periods are needed to check the long-term sustainability of these benefits. Extending this model to other chronic conditions and doing cost-effectiveness analyses are also recommended.
Key points for policy, practice and further research
Web-based self-care education programmes based on Orem’s model significantly improve health-promoting behaviours in patients with MS.
This approach offers advantages of accessibility, convenience and patient engagement over traditional educational methods.
Healthcare providers should consider combining web-based platforms into routine care for chronic disease management.
Future research should look into long-term sustainability and effectiveness across different populations and healthcare settings.
Supplemental Material
sj-docx-1-jrn-10.1177_17449871261445355 – Supplemental material for The effect of a web-based self-care education programme on the health-promoting behaviours of patients with multiple sclerosis: a randomised controlled trial
Supplemental material, sj-docx-1-jrn-10.1177_17449871261445355 for The effect of a web-based self-care education programme on the health-promoting behaviours of patients with multiple sclerosis: a randomised controlled trial by Sara Akbari, Kourosh Amini, Seyede Fatemeh Gheiasi and Nasrin Hanifi in Journal of Research in Nursing
Footnotes
Acknowledgements
This paper is derived from a Master’s thesis in Medical-Surgical Nursing at Zanjan University of Medical Sciences, and the study was conducted as part of the requirements for completing this MSc degree. The researchers express their sincere gratitude and appreciation to the esteemed Vice Chancellor for Research of Zanjan University of Medical Sciences, the officials and staff of Vali Asr Hospital, particularly the personnel of the Neurology Clinic and the MS patients who cooperated with the research team.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Ethics Committee of Zanjan University of Medical Sciences (approval code: IR.ZUMS.REC.1403.151), and the study was registered with the Iranian Clinical Trial Centre (IRCT20240811062717N1). We confirm that all experiments involving human participants were conducted in accordance with the relevant ethical guidelines and regulations. In this study, after explaining the objectives, subject matter, training and implementation methods, the researcher assured participants that their information would remain confidential, fully observing the principle of anonymity throughout the course of the study. Written informed consent was obtained from all participants in the study. Participation in the study was voluntary.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received financial support from Zanjan University of Medical Sciences in conducting this research (Grant No: A-11-86-31).
Guarantor
K.A. (Kourosh Amini) accepts full responsibility for the integrity of the work as a whole, from inception to published article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.