
Abstract
Introduction
Digital psychosocial interventions can reduce fear of cancer recurrence and are worth considering for patients whose primary concern is worry about the future. For patients with broader distress or quality-of-life concerns, digital tools may be helpful but often work best alongside human support.
For cancer survivors, completing treatment rarely ends the emotional journey. Fear of cancer recurrence affects up to 70% of patients (Lebel et al., 2016; Simard et al., 2013) yet access to psychosocial support remains limited (Dilworth et al., 2014). Technology-based interventions offer potential solutions to expand access to supportive care.
The systematic review that accompanies this commentary synthesises the available evidence on this topic. In recent editorial on systematic reviews, Thorne (2024) noted that the field increasingly prioritises methodologically tight technical products, over critically reflective thoughtful discussion. Systematic reviews serve an important function in synthesising evidence. However, they can risk narrowing the lens so tightly that the complex, context-dependent nature of nursing phenomena becomes difficult to capture. This commentary aims to provide a reflective engagement that complement the review’s findings, offering a framework for understanding why digital interventions work differently across psychosocial outcomes.
Summary of the paper
The review synthesises 14 randomised controlled trials involving 1509 cancer patients. The authors examined three outcomes: fear of cancer recurrence, psychological distress and quality of life. The main finding is that technology-based interventions significantly reduced fear of cancer recurrence, with minimal heterogeneity across studies. For psychological distress, the pooled effect was not significant, with considerable variation between results. For quality of life, non-significant estimates were observed.
These divergent findings invite a deeper question: Why might digital interventions be more effective for fear of recurrence than for other psychosocial outcomes?
The technology-psychosocial alignment model
The differential findings across outcomes invite us to consider how specific features of technology-based interventions align with different types of psychosocial needs. Drawing on the review’s findings and informed by established theoretical frameworks (Bandura, 1997; Lazarus and Folkman, 1984), we propose the Technology-Psychosocial Alignment Model as a preliminary framework to guide hypothesis generation for future research and to offer clinicians a heuristic for matching interventions to patient needs. This commentary responds to Thorne’s (2024) call for studies that involve the rigorous intellectual work of reading and reflecting on a wide range of writings rather than simply gathering findings from a small number of studies. The model suggests that different psychosocial outcomes have different degrees of ‘fit’ with the core features of digital interventions, determining how consistently technology-based approaches affect each outcome (Figure 1).
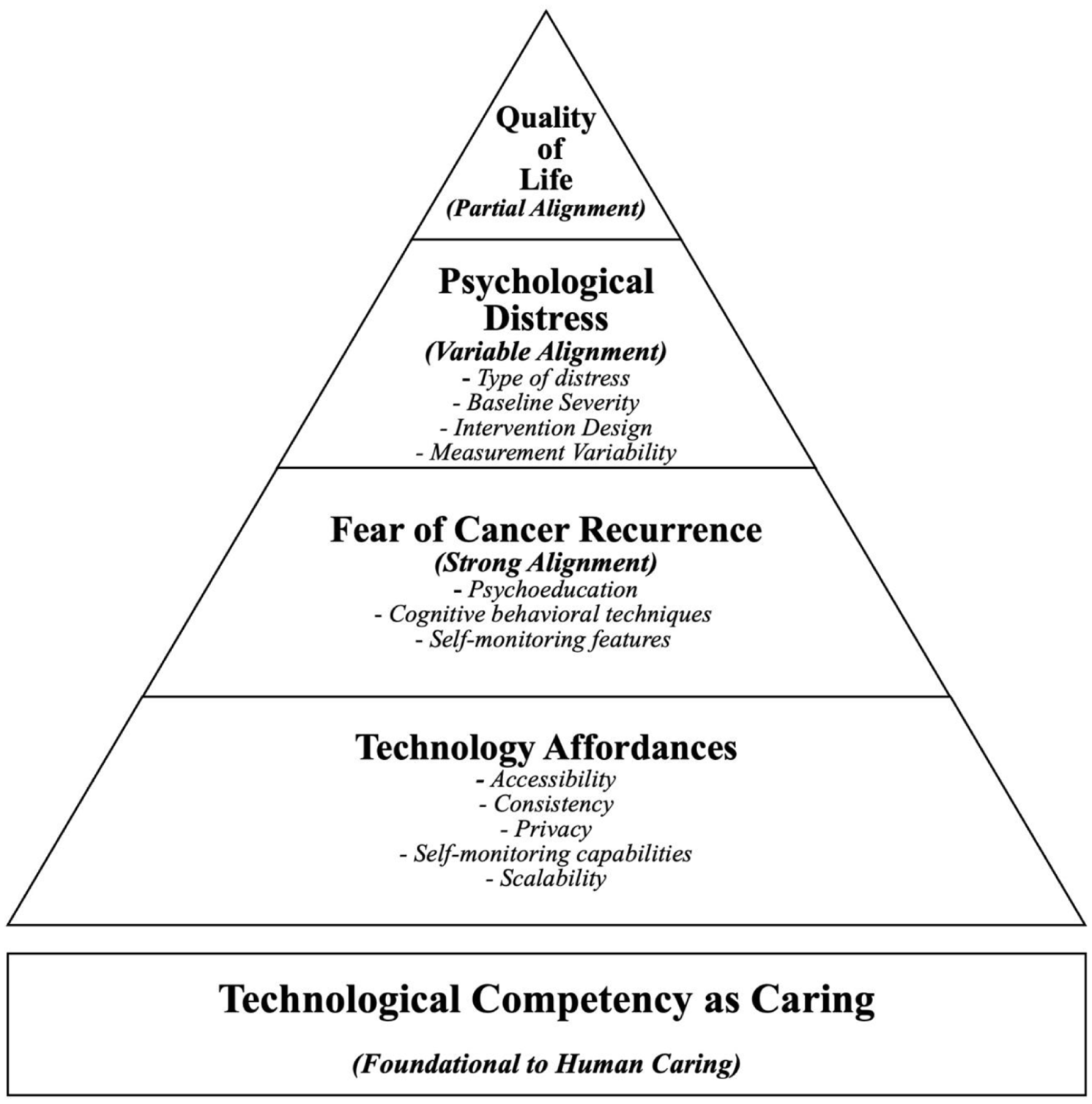
Technology-psychosocial alignment model pyramid.
Technology affordance as pillars
Digital interventions share several common features regardless of the specific format that distinguish them from traditional face-to-face delivery. These pillars include accessibility, consistency, privacy, self-monitoring capabilities, and scalability. Accessibility allows patients to engage 24/7 from any location, benefiting those with mobility limitations, rural residents and patients balancing work or caregiving. Consistency ensures standardised content delivery, maintaining quality control. Privacy reduces stigma associated with seeking mental healthcare. Self-monitoring capabilities track symptoms and behaviours, generating data for clinicians and feedback for patients. Scalability allows deployment to large populations at relatively low marginal cost.
These affordances are not equally relevant for all outcomes. The degree of alignment between what technology offers and what a given outcome requires determines intervention effectiveness.
Fear of cancer recurrence: strong alignment
Fear of recurrence shows the strongest alignment with digital delivery. This outcome is characterised by cognitive components (intrusive thoughts), behavioural components (hypervigilance and avoidance) and information needs (uncertainty about risk). Digital interventions map directly onto these characteristics: psychoeducation addresses information needs on demand; cognitive behavioural techniques target intrusive thoughts systematically, and self-monitoring helps identify triggers and track progress.
The low statistical heterogeneity (I2 = 4.7%) supports this alignment argument. Despite variation in intervention types, populations, cancer types and countries, the effect on fear of recurrence was consistently positive.
Psychological distress: variable alignment
Psychological distress encompasses a range of experiences including anxiety, depression and stress responses. The high heterogeneity observed (I2 = 76.1%) suggests that alignment varies depending on several factors:
Type of distress: Different forms of distress may respond differently. Some symptoms may require human interaction and personalised encouragement to be addressed effectively.
Baseline severity: Patients with mild-to-moderate distress may benefit from digital interventions that provide coping skills and support self-management. Those with more severe symptoms or complex presentations may require the therapeutic alliance and individualised attention that comes with human guidance.
Intervention design: Some digital interventions include human support via video or messaging; others are fully automated (Mohr et al., 2013). This variation likely influences outcomes, particularly for distress.
Measurement variability: Studies used different tools to measure distress, which may capture different aspects of the construct and contribute to heterogeneity.
The variable alignment does not mean digital interventions are ineffective for distress. Rather, it suggests that effects depend on context – patient characteristics, intervention design and distress type all matter.
Quality of life: partial alignment
Quality of life is a multidimensional construct that includes physical functioning, psychological well-being, social relationships and environmental factors (WHOQoL Group, 1998). The non-significant pooled estimate but consistent trend across studies suggests partial alignment where digital interventions may contribute to quality of life, but the effect may be modest.
Several factors may explain this partial alignment:
Physical dimensions: Symptoms such as pain, fatigue and treatment side effects often require medical management alongside psychological support. Digital interventions focused on psychosocial education may not directly address these physical components.
Social dimensions: Meaningful relationships and social connections typically involve real-time interaction and shared experience. Although technology can facilitate connection through forums or videoconferencing, it may not fully replicate the quality of in-person social support.
Existential dimensions: Concerns about mortality, meaning and purpose may require deep, personalised dialogue that is difficult to standardise or automate. These aspects of quality of life may be more responsive to human interaction.
As Thorne (2024) reminds us, much of what matters in nursing is complex, dynamic and context-dependent, which is not at all amenable to condensation and aggregation. Quality of life may resist simple digital solutions because it is shaped by these multidimensional, relational factors. It is also confirmed that technology can support but not fully substitute for human interaction in these domains. We need multiple patterns of knowing the person as a whole and with a theoretical appreciation of technological competency as caring in nursing.
Technological competency as caring in nursing: foundational to human caring
The Technology-Psychosocial Alignment Model provides a framework for understanding the differential effectiveness of digital tools. However, its application must be guided by an ethico-philosophical foundation to ensure that technology serves, rather than supplants, human connection. Locsin’s Technological Competency as Caring in Nursing (TCCN) theory offers this foundation (Locsin, 2017).
Central to TCCN is the view that the ultimate purpose of using technology in nursing is to ‘know persons as caring’, who are whole and complete in the moment, in order to appreciate their uniqueness, their hopes, dreams and aspirations beyond their diagnosis or symptoms (Locsin and Schoenhofer, 2025). This is achieved through ‘technological competency as expression of caring’, a way of knowing in nursing that engages the competent use of technologies to foster, not replace, ways of appreciating the wholeness of persons. Locsin (2017) emphasised that technologies of care should ‘bring the patient closer to the nurse’ by enhancing the nurse’s ability to know the person more fully, while cautioning that technology can also increase the relational gap if the patient becomes an object of care rather than a participant in their care (Locsin, 2017).
Implications for practice
For clinicians, this framework offers practical guidance. Nurses should assess whether fear of recurrence is the dominant issue or whether broader distress and quality-of-life concerns are more prominent. Patients with multiple interacting symptoms may require blended approaches. Structured self-guided programmes suit fear of recurrence; for psychological distress, interventions with human guidance may be more effective. Following TCCN, nurses must ensure that technology is used to deepen understanding of the person, not merely to track outcomes. Engagement should be monitored, and patients who do not improve should be offered escalation of care.
Implications for research
Following Thorne’s (2024) critique of ‘empty, redundant, or pointless’ systematic reviews, future research should move beyond simply updating existing reviews with additional trials. Mediation studies should examine whether psychoeducation, Cognitive Behavioural Therapy skills and self-monitoring mediate effects on fear of recurrence. Individual patient data meta-analyses could examine moderators of distress outcomes. Hybrid effectiveness-implementation trials with longer follow-up (12–24 months) are needed for quality of life. Research might also examine how TCCN’s concept of ‘technological knowing’ can be operationalised in digital intervention design to ensure caring presence is maintained.
Conclusion
This systematic review by Saragih et al. (2026) provides evidence that technology-based psychosocial education can reduce fear of cancer recurrence among adults with cancer. The Technology-Psychosocial Alignment Model offers a framework for understanding why some outcomes may be more responsive to digital delivery than others. The fear of recurrence aligns well with digital tools’ strengths, while broader distress and quality of life may require more comprehensive approaches. TCCN theory adds an essential ethical dimension where the purpose of technology is not replacement but ‘co-existence’ of using digital tools to know persons more fully while preserving the caring relationship. As Thorne (2024) reminded us, the most meaningful scholarship engages critically with complexity rather than reducing it to simple aggregations. Understanding what works, for whom and under what circumstances remains an important direction for both research and practice.
Footnotes
AI disclaimer
The authors used the assistance of Microsoft Copilot in editing the text to enhance language clarity. The authors reviewed and revised the content and take full responsibility for the final version.