
Abstract
Aim:
To examine the clinical activity and workforce contribution of Advanced Nurse Practitioners (ANPs) working in general practice.
Background:
Primary care systems internationally are experiencing increasing demand due to ageing populations, rising multimorbidity and workforce shortages. Advanced nursing practice has expanded globally as a strategy to strengthen service capacity, improve access and maintain quality outcomes. Although there is substantial evidence regarding patient outcomes associated with advanced practice roles, there is comparatively limited empirical data describing the day-to-day clinical activity of ANPs in primary care settings.
Methods:
This national cross-sectional descriptive study, conducted in Ireland and reported in accordance with the STROBE Statement, involved a 1-week activity capture of General Practice Advanced Nurse Practitioners (GP ANPs) and candidate ANPs (cANPs) working across general practice settings. Data collected included consultation type, prescribing activity, complexity of care and clinical outcomes. Data were analysed using descriptive statistics.
Results:
Twenty GP ANPs/candidate ANPs recorded 1659 consultations, including 757 full episodes of care (45.6%). Practice spanned acute illness (adults and children), chronic disease management, women’s health and preventive services. Medication optimisation activity included 503 medication reviews, 251 prescriptions issued and 59 medications deprescribed. About 15% of consultations were classified as complex and 14.8% involved multiple presenting complaints. Most consultations were independently managed.
Conclusion:
GP ANPs demonstrate broad clinical capability and contribute substantially to general practice capacity. The findings highlight the value of a holistic nursing approach, which is well suited to chronic disease management, health promotion, patient education and the management of multimorbidity, supporting access to care and strengthening primary care workforce capacity.
Keywords
Introduction
Primary care systems internationally are under increasing pressure due to population ageing, rising prevalence of chronic disease and increasing complexity of patient needs. Workforce shortages in general practice; a community-based, multidisciplinary setting that serves as the first point of contact (‘front door’) for healthcare; have been identified across many health systems as a significant threat to service sustainability and accessibility, potentially contributing to unmet healthcare need, delayed care and increased pressure on acute and secondary care services (Collins and Homeniuk, 2021; Freund et al., 2015). These pressures have prompted exploration of new models of care, including expanded multidisciplinary team roles and advanced nursing practice (Casey et al., 2022).
In Ireland, general practice nurses contribute significantly to chronic disease management, preventive care and patient education, providing a strong foundation for the development of advanced practice roles within primary care (Bury et al., 2021).
Within Irish general practice, General Practice Advanced Nurse Practitioners (GP ANPs) are registered nurses who have completed advanced clinical education, to a minimum of master’s level and are authorised to practise autonomously within defined scopes of practice, including assessment, diagnosis and prescribing (Nursing and Midwifery Board of Ireland [NMBI], 2017).
GP ANPs work alongside General Practitioners (GPs) as part of multidisciplinary teams rather than replacing medical roles. Their contribution lies in managing a broad scope of clinical presentations, including acute illness, chronic disease management and preventive care, often independently. This enables redistribution of clinical workload, supports timely access to care and allows GPs to focus on more complex or specialised cases including patients with higher levels of clinical uncertainty, risk or complexity and those requiring coordination across services or specialist input.
In addition to registered ANPs, the workforce includes candidate Advanced Nurse Practitioners (cANPs), who are registered nurses undertaking structured postgraduate education and supervised clinical practice towards ANP registration with the Nursing and Midwifery Board of Ireland (NMBI). During this period, cANPs practise within defined clinical governance frameworks and contribute to service delivery within an agreed scope of practice.
Advanced nursing practice has developed globally over several decades in response to changing health service demands. The role has evolved from early nurse practitioner models in North America to widespread implementation across Europe, Australasia and other regions, supported by regulatory frameworks, postgraduate education and expanded clinical autonomy (Unsworth et al., 2024; Wheeler et al., 2022). ANPs are characterised by expert clinical decision-making, prescribing authority and the ability to practise autonomously within defined scopes of practice (Zhang, 2024; Schober et al., 2020).
Evidence suggests that advanced practice roles have significant potential to contribute to primary care workforce capacity. Cross-national analyses across 39 countries indicate that ANPs can manage substantial proportions of activities traditionally undertaken by physicians, particularly in chronic disease management, preventive care and management of common acute presentations (Maier and Aiken, 2016). Systematic reviews of international evidence, across multiple healthcare systems, demonstrate that nurse practitioner-led care is comparable to physician-led care in terms of safety and clinical outcomes (Htay and Whitehead, 2021; Laurant et al., 2018; Swan et al., 2015).
Patient experience studies have reported high levels of satisfaction with ANP-led care, often associated with longer consultations, continuity and holistic approaches to care (Htay and Whitehead, 2021). These findings have positioned advanced practice roles as a key component of workforce transformation strategies internationally.
Within Europe, implementation of advanced practice roles has accelerated in recent years, although progress has varied between countries due to differences in regulation, workforce planning and health system structure (Unsworth et al., 2024).
The increasing prevalence of multimorbidity presents challenges for primary care services (Savva, 2011; Tadeu et al., 2020). Managing complex patients requires continuity, comprehensive assessment and coordination across services. ANPs are well-positioned to contribute through holistic, patient-centred approaches and continuity of care (Donald et al., 2010; Pelletier et al., 2019).
In Ireland, advanced nursing practice is supported by national regulatory frameworks requiring ANPs to be educated to a minimum of master’s level and registered with the Nursing and Midwifery Board of Ireland (NMBI, 2017).
Although there is substantial international evidence regarding patient outcomes associated with advanced practice roles (McMenamin et al., 2023), there is comparatively limited empirical data describing the volume and scope of clinical activity undertaken by ANPs in routine primary care practice. Much of the existing literature focuses on role implementation or patient outcomes rather than examining day-to-day clinical workload and service contribution.
Understanding how advanced practice roles function in everyday service delivery is important for informing workforce planning and health system development.
This study is among the first to provide empirical, real-world data on the clinical activity of GP ANPs in general practice, offering insight into consultation patterns, prescribing practices and clinical complexity within routine care.
The aim of this study was therefore to examine national activity data relating to GP ANPs, exploring consultation patterns, prescribing activity, clinical complexity and independently managed episodes of care to better understand the potential contribution of advanced practice roles to primary care workforce capacity, in order to provide empirical evidence to inform primary care workforce planning and the development of advanced practice roles
Methods
Study design
This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement (Supplemental File) (von Elm et al., 2007). A national cross-sectional descriptive study was undertaken to examine the clinical activity and workforce contribution of GP ANPs and candidate ANPs (cANPs) working in general practice settings in Ireland.
The study involved a prospective 1-week activity capture designed to provide a snapshot of routine clinical practice, scope of activity and contribution to service delivery within primary care.
Participants and recruitment
Participants included registered GP ANPs and candidate ANPs currently working in general practice settings across Ireland. Recruitment was undertaken through national professional networks and communication channels relevant to GP ANPs, including professional groups and organisational mailing lists. Participation was voluntary, and no incentives were provided. A total of 20 GP ANPs and cANPs participated in the study, representing approximately 40% of the estimated national cohort of 54 practitioners at the time of data collection.
Setting
Participants were employed across a range of general practice settings, including urban, rural and mixed practices. GP ANPs typically work within multidisciplinary teams that include GPs, practice nurses and administrative staff.
Detailed clinic-level characteristics, such as funding model, staffing composition and appointment duration, were not systematically collected as part of this study.
Data collection
Data collected included consultation type (e.g. acute illness, chronic disease management, women’s health and preventive care), prescribing activity (including medication review, prescribing and deprescribing), consultation complexity and clinical outcomes. Consultation activity was recorded prospectively during the study week using a structured electronic data collection tool.
The data collection tool was developed by a group of GP ANPs with experience in primary care practice to reflect key domains of clinical activity relevant to the role, including consultation type, prescribing activity, complexity of care and clinical outcomes. The tool was informed by the scope of practice and role requirements for ANPs, as defined by the NMBI and designed to capture core elements of advanced clinical practice within general practice settings.
The tool was piloted by members of the research team, who are practising GP ANPs, to ensure clarity, usability and relevance to clinical practice, and minor refinements were made based on feedback.
Participants recorded data contemporaneously during routine clinical practice. Data were anonymised and submitted in aggregated format via an electronic Microsoft Excel spreadsheet for analysis.
The data collection tool is available as Supplemental Appendix 1.
Workforce contribution
Workforce contribution was operationalised using three key indicators:
Consultation volume
Number of independently managed episodes of care
Prescribing and medication optimisation activity
Prescribing and medication optimisation were considered as distinct but complementary aspects of medicines management, with prescribing reflecting the initiation of pharmacological treatment and medication optimisation encompassing activities such as medication review, adjustment and deprescribing. These indicators were selected to reflect both the scale and scope of clinical activity undertaken by GP ANPs within general practice.
Data management and analysis
Data were submitted electronically and exported into Microsoft Excel for cleaning and analysis. The data were checked for completeness and consistency prior to analysis. Any incomplete or unclear entries were excluded from analysis where necessary. Descriptive statistics, including frequencies and percentages, were used to summarise consultation activity, prescribing practices, consultation complexity and clinical outcomes.
No inferential statistical analysis was undertaken, as the aim of the study was to provide a descriptive snapshot of clinical activity rather than to test hypotheses or establish causality.
Results
Workforce profile
A total of 20 GP ANPs and candidate ANPs participated in the study (n = 20). Of these, 11 (55%) were registered Advanced Nurse Practitioners (ANPs) and 9 (45%) were candidate ANPs. All respondents were female (n = 20, 100%); however, anecdotal information indicates that there are two male GP ANPs within the wider national cohort. Eighteen participants (n = 18, 90%) reported completing their advanced practice training within general practice settings, whereas two (n = 2, 10%) completed training in secondary care settings. Most participants (n = 18, 90%) reported working more than 35 hours per week, with two participants (n = 2, 10%) working fewer than 20 hours per week. Participants worked across a range of practice settings, including mixed urban and rural practices (n = 10, 50%), urban practices (n = 6, 30%) and rural practices (n = 4, 20%). Participant and practice characteristics are presented in Table 1.
Participant and practice characteristics.
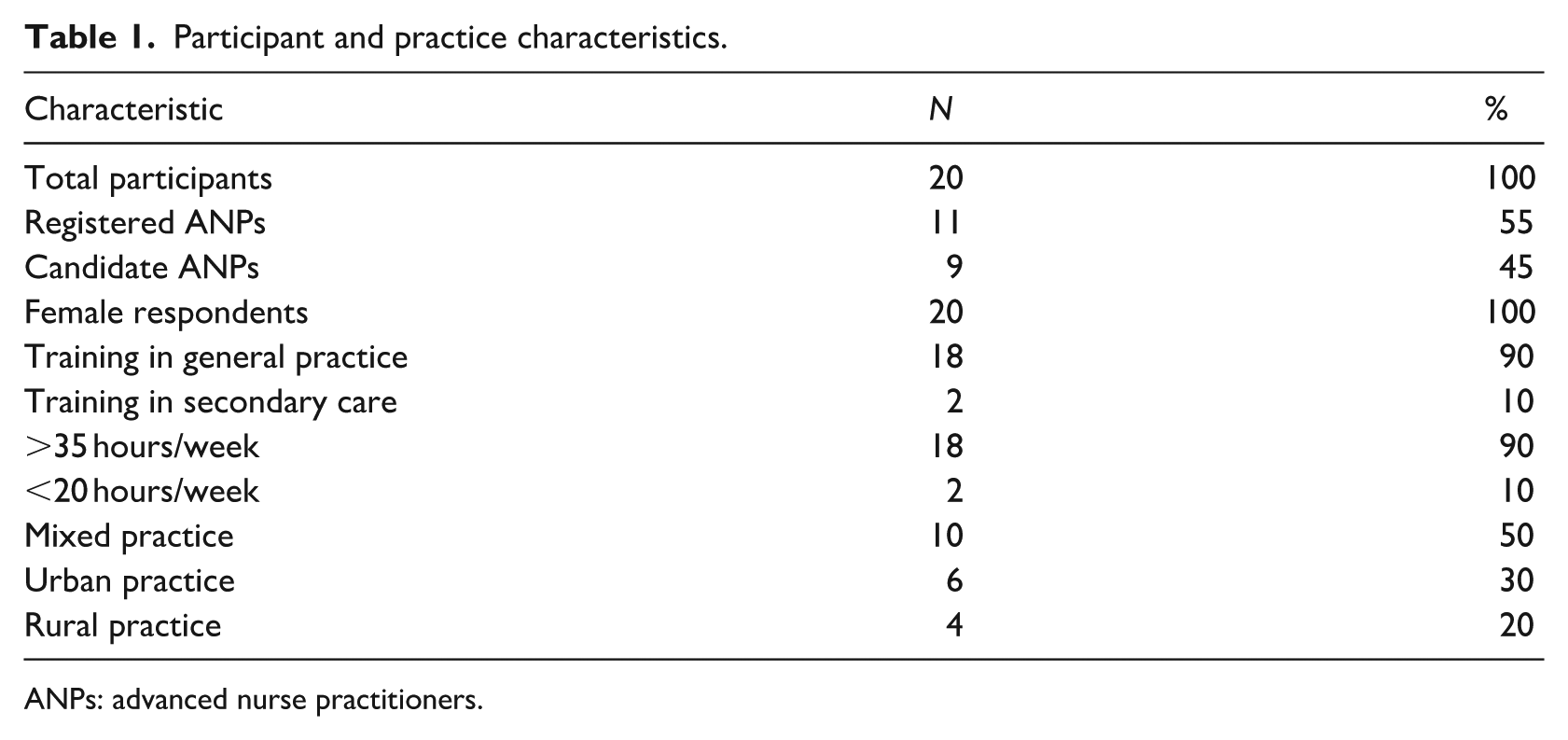
ANPs: advanced nurse practitioners.
Consultation activity
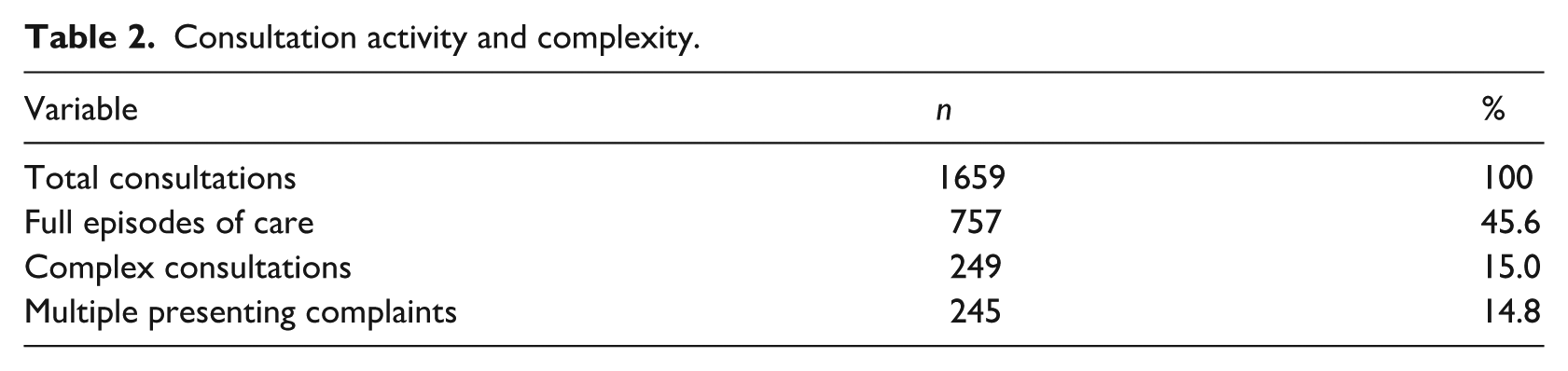
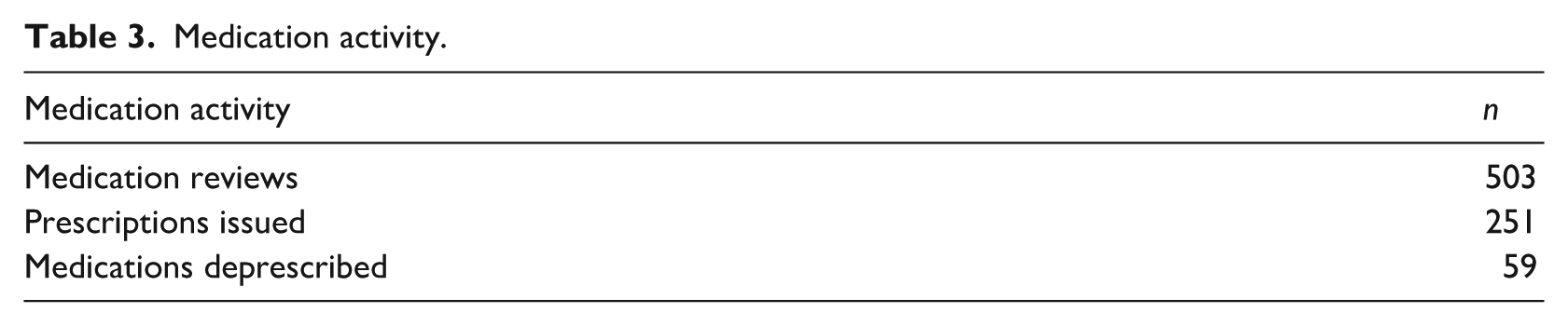
A total of 1659 consultations (n = 1659) were recorded during the 1-week study period, equating to an average of approximately 83 consultations per GP ANP/cANP per week (approximately 16 per day based on a 5-day working week). Of these 757 consultations (45.6%) were classified as full episodes of care, defined as consultations involving comprehensive assessment, clinical examination, diagnosis, treatment planning and follow-up or safety-netting where required. Consultations included chronic disease management, acute illness in adults and children, women’s health and preventive care. A total of 249 consultations (n = 249, 15.0%) were classified as complex, defined by the clinician as consultations involving multiple comorbidities, diagnostic uncertainty or increased clinical decision-making requirements. Additionally, 245 consultations (n = 245, 14.8%) involved patients presenting with more than one complaint during a single consultation (Table 2). Medication-related activity comprised 503 medication reviews, 251 prescriptions issued and 59 medications deprescribed (Table 3).
Consultation activity and complexity.
Medication activity.
Summary of findings overall, GP ANPs managed a high volume of consultations across a broad clinical scope, with a substantial proportion completed as independent episodes of care.
Discussion
This study provides empirical evidence describing the scope, complexity and workforce contribution of GP ANPs working in general practice. The findings demonstrate that GP ANPs are engaged in a wide range of clinical activities, including chronic disease management, acute care, medication optimisation and management of complex presentations.
GP ANPs function within multidisciplinary general practice teams, complementing rather than replacing GP roles. Their contribution supports appropriate allocation of clinical workload based on professional expertise, enhances overall service capacity and may improve timely access to care within primary care settings, delivering comprehensive, generalist care across the lifespan while drawing on nursing strengths in health promotion, patient education and multimorbidity management. The findings indicate that GP ANPs are managing substantial volumes of clinical activity, including a high proportion of independently completed episodes of care.
These findings are consistent with international evidence demonstrating that nurse practitioners can manage substantial proportions of primary care consultations, particularly in chronic disease management and acute presentations (Laurant et al., 2018; Maier and Aiken, 2016). However, direct comparison across studies remains challenging due to variation in role definitions, regulatory frameworks and healthcare system structures internationally.
The involvement of GP ANPs in managing patients with multimorbidity is particularly relevant within contemporary primary care. International and national evidence indicates that general practice consultations increasingly involve patients presenting with multiple chronic conditions, polypharmacy and overlapping health concerns requiring coordinated management (Savva, 2011; Tandan et al., 2022). This aligns with the strengths of advanced nursing practice, including a holistic approach to care, health promotion, patient education and the coordination and management of complex, long-term conditions (Pelletier et al., 2019; Wheeler et al., 2022).
Taken together, these findings suggest that GP ANPs are functioning as autonomous clinicians within primary care, contributing to both service delivery and workforce sustainability. The ability to manage complex patients and multiple presenting complaints within a single consultation reflects key characteristics of advanced practice, including clinical judgement, comprehensive assessment and continuity of care. Importantly, this also reflects the distinct contribution of nursing practice, characterised by a holistic, person-centred approach that integrates health promotion, patient education and the coordination of care for patients with complex and multimorbid needs.
The finding that most participants completed their advanced practice training within general practice settings may reflect the development of role-specific expertise aligned to the primary care context.
However, the inclusion of ANPs trained in secondary care suggests that advanced clinical competencies may be transferable across healthcare settings, provided appropriate induction and support structures are in place.
The workforce modelling presented in this study provides an illustrative estimate of potential service capacity. For example, if similar activity levels were replicated across a larger cohort, 100 GP ANPs could potentially deliver approximately 3785 independently managed episodes of care per week, equating to approximately 15,140 episodes over a 4-week period.
These estimates should be interpreted cautiously, as they are based on cross-sectional data and do not account for variation in workload, service configuration or seasonal demand. However, they provide a useful illustration of the potential contribution of advanced practice roles to primary care workforce capacity.
The findings also highlight the evolving role of advanced practice within primary care teams. GP ANPs contribute not only through direct patient care but also through service coordination, clinical leadership and support for multidisciplinary team functioning, demonstrating both high clinical capacity and the delivery of high-quality care within general practice settings. This study addresses a notable gap in the literature by providing empirical, real-world data on the day-to-day clinical activity of ANPs in general practice, an area where evidence remains limited internationally.
From a workforce perspective, the findings support the continued development and integration of advanced practice roles within general practice settings. As healthcare systems respond to increasing demand, workforce models that optimise the contribution of skilled clinicians will be essential. This may include the development of nurse-led models of care and specialised general practice services, particularly in areas such as chronic disease management and care of older populations, with emerging examples such as nurse-led menopause services demonstrating the potential of advanced practice roles in targeted areas of care (Keye, 2025).
Strengths and limitations
A key strength of this study is that it captures real-world clinical activity across a substantial proportion of the national GP ANP workforce, providing insight into the breadth, complexity and autonomy of the role within routine practice. A further strength is the inclusion of approximately 40% of the national GP ANP workforce, offering a meaningful and representative snapshot of current clinical practice.
This study should be interpreted in the context of several limitations. The dataset represents a 1-week activity capture and therefore reflects a cross-sectional snapshot rather than longitudinal activity. Participation was based on a convenience sample. Although the cohort represents approximately 40% of the national workforce, the overall number of GP ANPs remains relatively small. Data were self-reported and may be subject to reporting bias. The data collection tool was developed for this study and was not formally validated. Detailed categorisation of presenting complaints was not captured, limiting analysis of the most common reasons for consultation. Finally, data relating to length of time practising as an ANP were not collected, which may limit interpretation of findings in relation to experience and clinical activity.
Implications
The findings from this study have important implications for workforce planning and service delivery within primary care.
The breadth of consultations, prescribing activity and independent episode management observed within this dataset suggest that GP ANPs are contributing meaningfully to clinical workload within general practice settings.
The involvement of GP ANPs in chronic disease management, acute care and multimorbidity reflects the evolving nature of primary care demand in terms of both the quantity and quality of care required and signals a potential shift in workforce considerations towards models that optimise the contribution of advanced practice roles.
Integration of advanced practice roles within multidisciplinary teams may support improved access to care, continuity of care and service responsiveness.
From a systems perspective, the findings suggest that advanced nursing practice may represent an important component of future primary care workforce models, particularly in the context of increasing demand and workforce constraints.
Conclusion
This national cross-sectional study demonstrates the breadth, complexity and autonomy of GP ANP practice within Irish general practice. GP ANPs manage acute illness, chronic disease, women’s health and complex presentations, contributing to service accessibility and continuity of care. GP ANPs appear to contribute substantially to general practice capacity. Expansion of advanced practice roles may represent an important workforce strategy for strengthening access to care and supporting sustainable primary care services. These findings provide important evidence to inform workforce planning and policy development relating to advanced practice roles in primary care.
Key points for policy, practice and research
GP ANPs manage a broad range of clinical presentations across primary care.
A substantial proportion of consultations are completed as independent episodes of care.
GP ANPs contribute to management of complex and multimorbid patients.
Advanced practice roles support primary care workforce capacity.
Further research is needed to examine long-term outcomes and service impact.
Supplemental Material
sj-docx-1-jrn-10.1177_17449871261452880 – Supplemental material for Clinical scope and workforce contribution of advanced nurse practitioners in general practice: a cross-sectional study
Supplemental material, sj-docx-1-jrn-10.1177_17449871261452880 for Clinical scope and workforce contribution of advanced nurse practitioners in general practice: a cross-sectional study by Catriona Keye, Pamela McCann, Orla Loftus Moran, Melissa Hammond, Jane Deehan, Louise Nolan Ryan, Katy Lynch and Carol Kelly in Journal of Research in Nursing
Footnotes
Acknowledgements
The authors would like to thank the GP ANPs who contributed activity data to this project. This study did not include patient or public involvement in its design, conduct or reporting.
Author contributions
Availability of data and materials
Data supporting the findings of this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted as a service evaluation using anonymised, non-identifiable data. Participation was voluntary, and completion of the data collection tool was taken as implied consent. Formal ethical approval was not required in line with institutional guidance. Ethical approval was not sought as the project was classified as a service evaluation in accordance with Health Research Authority guidance. The Health Research Authority, which oversees ethical approval for research involving human participants, specifies that activities such as clinical audit, service evaluation and public health surveillance do not require formal ethical review. This activity capture study was considered to fall within these categories.
Consent to participate
Informed consent was obtained from participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.