
Abstract
Background:
Nurses constitute the largest segment of the healthcare workforce, yet they are frequently undervalued within health systems and society. This study explored how nurse managers empower registered nurses and how such empowerment shapes nursing practice, professional identity and care delivery within a resource-constrained Ghanaian hospital.
Methods:
A qualitative descriptive exploratory design was used. Seventeen registered nurses were purposively sampled. Data were collected through semi-structured, face-to-face interviews and analysed using qualitative content analysis, supported by reflexivity, peer debriefing and data saturation. The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist guided the reporting of the study.
Results:
Two themes were identified: (1) Nurse Empowerment in Low-Resource Clinical Settings and (2) Organisational and Leadership Influences on Empowerment. Empowerment enhanced retention, advocacy, autonomy and quality care. Supportive leadership, recognition, training and shared decision-making facilitated empowerment; whereas autocratic leadership, favouritism, limited resources and gender-related challenges hindered empowerment.
Conclusion:
Nurse manager-led empowerment strengthens nurses’ confidence, autonomy and care quality. Culturally responsive leadership, equitable recognition, staff development and inclusive decision-making are essential for sustaining the nursing workforce and improving patient outcomes through advocacy, high-quality care and error reduction in Ghana.
Keywords
Background
Nurses constitute the largest segment of the healthcare workforce, yet they are frequently undervalued within health systems and society. Evidence suggests that nurses often internalise this devaluation, perceiving themselves as inferior to other healthcare professionals, particularly physicians (Guan et al., 2025; Teresa-Morales et al., 2022). In some sub-Saharan African countries, such as Tanzania, nurses have reported experiences of abuse and disrespect (Shimoda et al., 2020). Similarly, in Ghana, nurses report instances of workplace violence, job dissatisfaction and negative attitudes from some patients (Appiah et al., 2023; Boafo, 2018). Such perceptions and experiences can erode professional confidence, limit autonomy and negatively affect job performance and quality of care.
These challenges are further shaped by the historical and socio-cultural positioning of nursing as a profession. Historically, nursing has been socially constructed as a female-dominated profession and is often associated with gendered stereotypes that frame caregiving as weak, subordinate or auxiliary work (Nyholm et al., 2025). Gender norms continue to shape nurses’ professional experiences, influencing interactions in both educational and clinical settings (Olgay et al., 2025). Given that approximately 76.91% of the global nursing workforce is female, these perceptions have profound implications for empowerment, professional identity and leadership engagement within nursing (Kharazmi et al., 2023; Manojlovich, 2007). In sub-Saharan Africa, including Ghana, the perception that nursing is primarily a female profession persists (Appiah et al., 2021). Such gendered expectations may negatively influence motivation, particularly among male nurses, potentially affecting their engagement, retention and opportunities for professional advancement. These challenges highlight the importance of empowerment in strengthening nurses’ autonomy, confidence and overall job satisfaction.
Against this backdrop, understanding empowerment within nursing becomes critical. The concept of empowerment is multifaceted and context-dependent, drawing from social and psychological theories (Chompukum and Vanichbuncha, 2025). In nursing, empowerment is best understood as the process through which nurses gain access to essential organisational structures such as information, resources, support and opportunities while also developing a sense of competence, autonomy and control over their clinical practice (Khrais and Nashwan, 2023; Orłowska and Laguna, 2023). Structural empowerment shapes the conditions that enable nurses to perform effectively, whereas psychological empowerment reflects nurses’ internal perceptions of their ability to influence patient care and organisational outcomes (Orłowska and Laguna, 2023). These dimensions enable nurses to actively participate in decision-making, exercise professional judgement and deliver high-quality care. Both dimensions are strongly associated with improved job satisfaction and reduced burnout (Ibrahim, 2023). However, much of the existing research has focused on high-income settings, with limited exploration of how nurse managers operationalise empowerment in resource-constrained environments.
Within this context, leadership emerges as a key mechanism for fostering empowerment. Leadership plays a pivotal role in addressing the imbalance where nurses are often undervalued, have limited autonomy and are excluded from decision-making processes within healthcare systems. Regardless of individual competence or knowledge, nurses cannot be fully empowered without supportive leadership structures that promote participation, voice and decision-making authority (Mackey, 2014). Contemporary evidence shows that nurse leaders who adopt participatory management approaches can actively empower nurses, reduce burnout and improve workplace engagement (Christensen et al., 2024). In contrast, limited empowerment reinforces perceptions of nurses as lacking autonomy or initiative and perpetuates hierarchical dependence on other healthcare professionals (Godsey et al., 2020).
This challenge extends beyond practicing nurses to nursing students, who may experience marginalisation and devaluation during training, further undermining confidence and professional development (Richter, 2022). This is particularly concerning given that nurses spend more time with patients than any other healthcare professional and are central to patient monitoring, advocacy and continuity of care (Butler et al., 2018). Empowerment is therefore essential not only for workforce well-being but also for patient safety, care quality and health system effectiveness.
Empirical evidence consistently links nurse empowerment to improved organisational commitment, job satisfaction, work motivation and performance, alongside reduced occupational stress and burnout (Rawah and Banakhar 2022; Saleh et al., 2022). Empowerment has also been shown to enhance retention, career advancement and patient outcomes, including reduced mortality and increased patient satisfaction (Dalab, 2024). Importantly, scholars emphasise the need to cultivate empowerment early during nursing education to sustain confidence and professional agency throughout nurses’ careers (Aydogdu, 2024; Chen and Howes, 2024).
Despite its importance, empowerment research has historically received greater attention in disciplines such as social work, community psychology and health promotion, with comparatively limited focus on nursing particularly in low- and middle-income countries (Sharplin et al., 2025). Although global interest in nurse empowerment is growing, evidence from African contexts remains sparse. Studies indicate that in countries such as Ghana, nurses have often been excluded from policy development, decision-making processes and staff development initiatives, further limiting empowerment and motivation (Yeh, 2025).
Although empowerment focuses on enabling conditions and nurses’ perceived ability to act, motivation refers to the internal and external forces that drive nurses’ willingness to perform their roles effectively (Baljoon et al., 2018; Senbetu et al., 2025). Thus, empowerment can be understood as a key antecedent that shapes motivation by creating the conditions and perceptions necessary for nurses to feel capable, valued and engaged in their work.
In Ghana, substantial investments have been made to improve healthcare infrastructure and nurse working conditions. Nevertheless, reports indicate that registered nurses remain largely excluded from decision-making processes, and nurse manager-led empowerment practices remain under-examined (Roji and Jooste, 2020; Shariff, 2015). To date, there is limited empirical evidence examining how nurse managers empower registered nurses in clinical settings, particularly within specialised units.
Study purpose
This study aimed to examine nurse manager-led empowerment of registered nurses. Specifically, the study explores how empowerment is understood, and experienced by nurses; and examines its perceived impact on nursing practice and care delivery within the Ghanaian healthcare context.
Research questions
The following research questions were asked to address the problems identified:
What are the perceptions on empowerment for 21st-century nurses in Ghana?
What are the factors that influence empowerment among nurses in Ghana?
Methods
Design and settings
This study employed a qualitative descriptive exploratory design to examine how registered nurses perceive and experience empowerment by nurse managers in Greater Accra Regional Hospital, Ghana. A qualitative approach was chosen because it provides rich, in-depth insights into participants’ experiences, beliefs and perceptions, generating detailed narrative data rather than numerical measures (Pathak et al., 2013). An exploratory design was appropriate given the limited prior research on nurse empowerment in this context and the need to understand a relatively unexamined phenomenon (Hunter et al., 2019).
The study was conducted at Ridge Hospital, officially known as the Greater Accra Regional Hospital (GARH), located on Castle Road in the Accra Metropolitan District of the Greater Accra Region of Ghana. Historically established in the 1920s and later expanded into a major regional referral and tertiary care facility, it serves as a cornerstone of healthcare delivery in Ghana’s capital, offering a broad range of specialist services including orthopaedics, emergency care, surgery, paediatrics, obstetrics and gynaecology, and diagnostic imaging, among others. The hospital also functions as a teaching and training site for health professionals and supports services across primary, secondary and tertiary care levels. As a busy regional hospital, it provides essential services to diverse populations throughout Ghana, making it an ideal setting to explore nurse empowerment within a complex clinical environment.
Data collection instrument
Data were collected using a semi-structured interview guide, which served as the primary data collection instrument. The interview guide was developed by the first author, a professor of nursing with extensive experience in qualitative research and the use of similar designs in prior studies. The development of the guide was informed by the study objectives and relevant literature on nurse empowerment. To enhance rigour and content validity, the interview guide was peer-reviewed by the other authors. The guide consisted of open-ended questions designed to elicit rich, in-depth responses. Core questions included: ‘Can you describe what empowerment means to you as a registered nurse’, ‘Share examples of how nurse managers have supported or limited your sense of empowerment in your daily work?’, ‘How does feeling empowered or disempowered affect the way you provide care to patients and work with other healthcare professionals’. Probing questions were used as needed to clarify responses and encourage deeper reflection. Interviews were conducted by the first and fifth authors, both of whom are trained in qualitative interviewing techniques.
Reflexivity and bracketing
All but one author are registered nurses with backgrounds in clinical practice, nursing management and education. Many of the authors have held senior leadership or managerial roles, whereas others are nurse educators involved in teaching and mentorship. Acknowledging that these experiences may shape assumptions about nurse empowerment, the research team engaged in regular reflexive discussions to minimise interpretive bias. Interviewers also maintained a neutral, non-directive approach to ensure participants’ perspectives were represented authentically.
Sampling technique and sampling size
A purposive sampling technique was used to recruit participants who could provide rich and relevant insights into the phenomenon under investigation. Registered nurses working at GARH were selected based on their direct experience with nurse manager leadership and empowerment practices within the clinical setting. This sampling approach was appropriate for the exploratory qualitative design, as it enabled the inclusion of participants with firsthand knowledge of the study topic.
The sample size consisted of 17 registered nurses, based on saturation as it was sufficient to achieve depth of understanding the study objectives.
Inclusion criteria were established to select registered nurses who were at least 18 years old, currently employed at the selected facility and had a minimum of 6 months of work experience. The 6-month threshold was chosen to ensure that participants had adequate exposure to nurse manager leadership and mentoring practices and were able to reflect meaningfully on empowerment experiences. Exclusion criteria included nurses who were unavailable during the recruitment period, those who expressed feeling physically unwell or emotionally distressed, and nurses who declined participation.
Data collection procedure
Nurses were recruited from GARH during duty hours. Initial recruitment was challenging due to workload and limited interest; however, after repeated visits over 1 month, 30 nurses consented to participate. Recruitment and data collection occurred concurrently, and interviews were scheduled at mutually convenient times. Most interviews were conducted in private rooms at the hospital before or after shifts, whereas a few took place in participants’ homes. Five nurses later withdrew due to personal or work-related circumstances.
Before each interview, researchers established rapport and explained the study purpose, procedures, risks and benefits. Participants provided verbal and written informed consent. Face-to-face, semi-structured interviews were conducted in English, with only the participant and researchers present, in private, quiet settings. Interviews lasted 30–45 minutes.
Data saturation was achieved by the 15th interview, with two additional interviews conducted to confirm saturation, yielding a final sample of 17 participants. Eight additional nurses who had expressed willingness to participate were informed that no further interviews were required due to data saturation; they were thanked for their interest and willingness to contribute to the study. Data collection occurred over 2 months, from September to November 2020.
Ethical consideration
Ethical clearance was sought at GARH before data were collected with ID protocol number: DHIRB/121/09/20. The researchers gave a brief introduction on the purpose of the study and assured the respondents of their privacy, confidentiality and their right to withdraw at any point during data collection. Informed consent was obtained from the respondents.
Data analysis
Data analysis involves moving from participants’ narratives towards an in-depth understanding of their experiences and contexts (Dibekulu, 2020). In this study, data were analysed using qualitative inductive content analysis, as described by Erlingsson and Brysiewicz (2017), which allows for the systematic organisation and interpretation of textual data into categories that reflect manifest and latent content.
All interviews were audio-recorded and transcribed verbatim prior to analysis. The analysis began with repeated reading of the transcripts to achieve immersion and gain a comprehensive understanding of the data. Meaning units relevant to the study objectives were then identified. These meaning units were condensed while preserving their core meaning and subsequently assigned codes that captured key ideas.
Codes were compared and grouped based on similarities and differences to form categories representing the manifest content of the data. These categories were further interpreted to identify underlying meanings (latent content), leading to the development of broader themes that reflect patterns across participants’ experiences.
To enhance rigour and credibility, the research team engaged in regular discussions throughout the analytic process to compare coding, resolve discrepancies and ensure consistency in interpretation. This collaborative approach strengthened the trustworthiness of the findings.
Trustworthiness and rigour
The rigour of this qualitative study was ensured using established criteria for trustworthiness: credibility, dependability, confirmability and transferability (Lincoln and Guba, 1985). Credibility was enhanced through prolonged engagement with participants over a period of 3 months, the use of semi-structured interviews to elicit rich and detailed narratives and peer debriefing among the research team during data collection and analysis. Dependability was supported through a transparent and systematic analytic process, including verbatim transcription, stepwise qualitative content analysis and documentation of analytic decisions. An audit trail was maintained to capture methodological decisions and changes throughout the study. Confirmability was strengthened through reflexivity and collaborative analysis, allowing interpretations to be reviewed and challenged within the research team to minimise individual bias and enhance neutrality. Transferability was addressed by providing thick descriptions of the study setting, participant characteristics and contextual factors influencing nurse empowerment within a resource-constrained Ghanaian hospital, enabling readers to assess the applicability of findings to similar contexts. In addition, the study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist to promote transparency and completeness in reporting qualitative methods and findings (Tong et al., 2007). The completed COREQ checklist is provided as Supplemental File 1.
Results
Socio-demographic characteristics
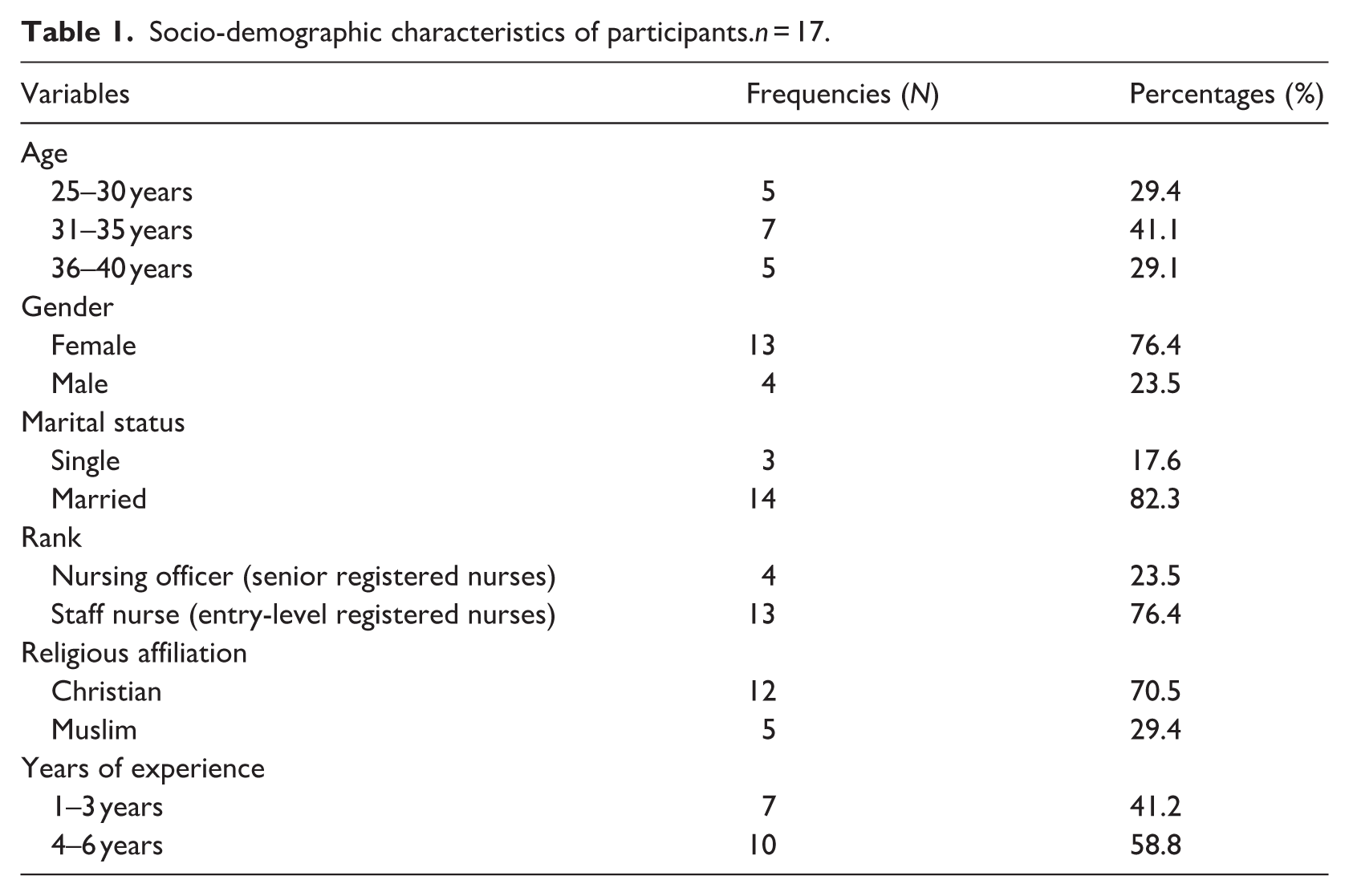
The sample consisted of 17 registered nurses. Most participants were aged 31–35 years (41.1%), followed by those aged 25–30 years (29.4%) and 36–40 years (29.1%). The majority were female (76.4%), whereas 23.5% were male. Most participants were married (82.3%), with 17.6% single. Participants included both staff nurses (entry-level registered nurses) and nursing officers (senior registered nurses). In terms of religious affiliation, 76.4% of participants identified as Christian and 23.5% as Muslim. Regarding years of experience, 58.8% of participants had 4–6 years of experience, whereas 41.2% had 1–3 years. See Table 1 for details.
Socio-demographic characteristics of participants.n = 17.
Organisation of themes
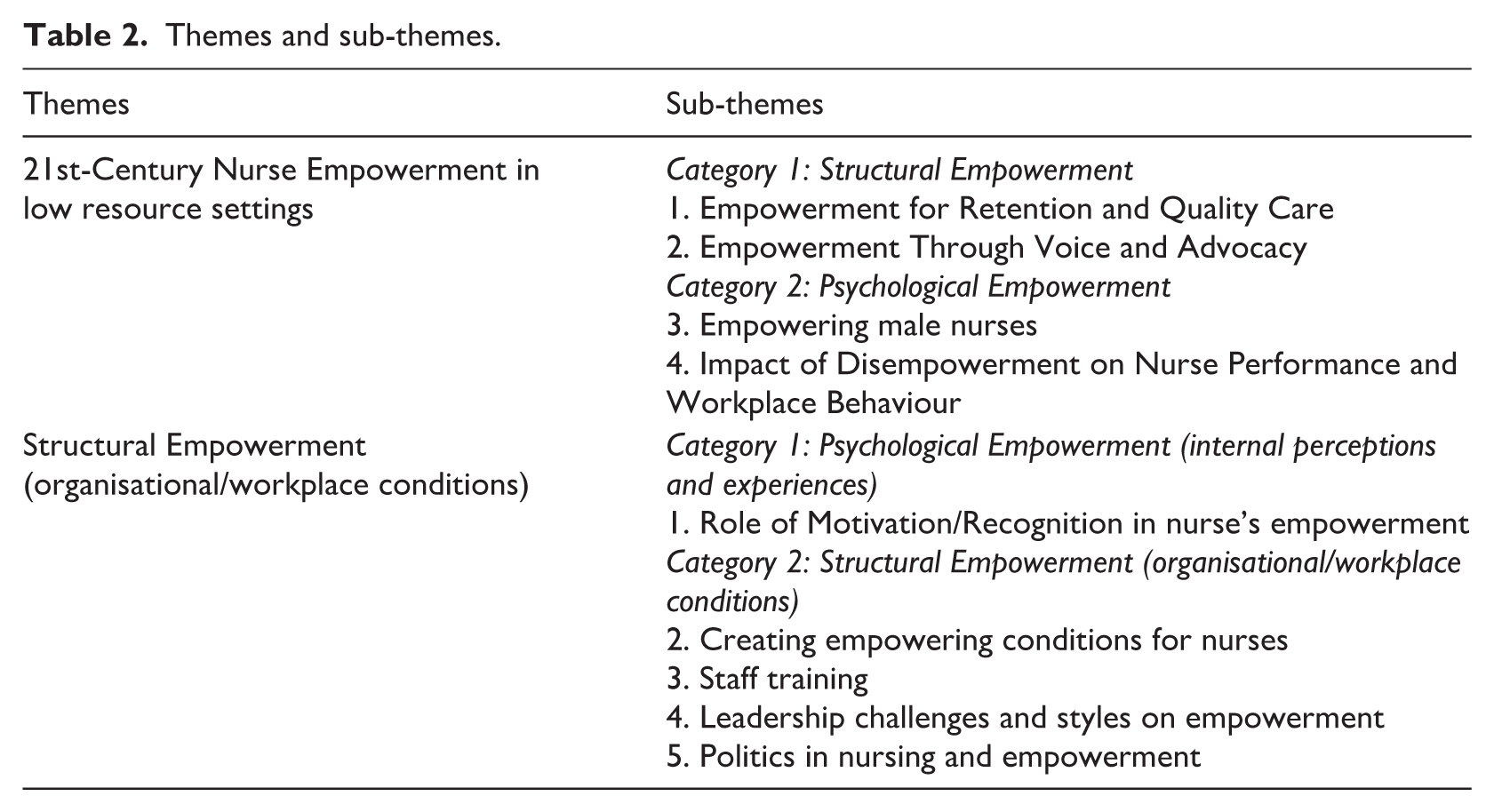
There were two main themes and nine sub-themes identified, as shown in Table 2.
Themes and sub-themes.
Theme 1: 21st-Century nurse empowerment in low resource settings
Category 1: Structural empowerment
Structural empowerment reflects organisational conditions that provide nurses with access to support, resources and opportunities, influencing retention, quality care and their ability to express voice and engage in advocacy.
Empowerment for retention and quality care
Participants consistently described empowerment as a protective resource that helps nurses cope with the psychological, emotional and physical demands of contemporary nursing practice. Empowerment was viewed not only as essential for sustaining individual resilience but also as a key strategy for workforce retention and safe, high-quality care delivery. Specifically, participants emphasised the role of empowerment in mitigating work-related strain and preventing burnout.
Nurses of today need to be empowered to help them to stay in the profession especially now that a lot of nurses are leaving the nursing profession, it could help to retain nurses. They go through psychological, emotional and physical strain due to the increasing workload and without empowerment, they will break down and lose interest in the profession hence nurses need to be empowered. (P9)
Participants highlighted that empowerment enhances motivation, reduces workplace pressure and promotes safe, high-quality care.
When you are empowered, you want to give your best. You feel free to work without pressure, and that makes you more productive with fewer errors. There have been many times when I felt down, but nurse managers encouraged me and boosted my morale. That support helped me work harder, bring out my best, and deliver quality care while ensuring patient safety by following the right procedures. (P1)
Participants described empowerment as enabling professional autonomy and critical thinking in nursing practice. When nurses felt supported by their managers, they reported greater confidence to think independently, make informed decisions and actively advocate for patients.
When nurse managers empower nurses, we become more analytical and creative, and we are able to make bold decisions regarding patient care. In the 21st century, nurses need to be assertive and confident advocates for their patients. (P5)
Empowerment through voice and advocacy
Several participants described how early messages from nursing leadership shaped their confidence to speak up and advocate for patients. Being explicitly encouraged to prioritise patients’ well-being and to use their professional voice helped some nurses feel justified in questioning decisions and taking action on behalf of those in their care. One participant recalled how this initial orientation message influenced her approach to practice: I remember our first day at work here the managers met us in the conference room and told us that our patients are our priority and hence we should not be afraid to speak up for them especially those who are seriously ill and since then I have always act according to the message by advocating for my patients even when it conflicts with other health professionals’ decisions. (P11)
Participants described how support from educators, in-charges and unit managers fostered independent practice, teamwork and confidence in interprofessional collaboration, reinforcing nurses’ responsibility to act in patients’ best interests without constant supervision. They first highlighted how empowerment supports independent practice and appropriate consultation: As nurses, we have been empowered in school, by our in-charges and managers to always carry out actions independently except when it is beyond our control and because of that I am able to provide care independently, work in a team where necessary and only consult my in-charge when there is a need. (P17)
Participants also emphasised that empowerment strengthens interprofessional collaboration and reduces hierarchical barriers: Also, we have come to understand that doctors are our colleagues and we should work with them as a team rather than been their subordinates, some nurses have some fear when working with doctors but we are colleagues and we have responsibilities for each other and therefore we should respect and support each other. When we are empowered the timidity and inferiority will stop. (P4). Finally, they noted that empowerment enables proactive, patient-centered care without constant supervision: In this unit, every nurse here is being empowered to give their best to the patients because patients here need constant care. Most of them are bedridden and need constant turning and pain relief so we know what to do daily we do not wait for someone to tell us before we do it. (P8)
Category 2: Psychological empowerment
Psychological empowerment reflects nurses’ internal perceptions of confidence, autonomy and self-worth, as seen in experiences of empowerment among male nurses and the reluctance or timidity that arises from a lack of empowerment.
Empowering male nurses
Gender-based challenges within nursing were highlighted, particularly the stigma and exclusion experienced by male nurses. Empowerment through recognition and inclusion was viewed as critical for retention and professional belonging. The need for targeted empowerment to address stigma and enhance inclusion was expressed as follows: Male nurses need to be empowered due to the stigma experienced by them since there is this perception that nursing is a female thing. To retain them in the job they need to be empowered by involving them in decision making, this will make them feel they belong too. (P5)
Experiences of marginalisation and the importance of acknowledging male nurses’ contributions were also emphasised: We the male nurses are always suppressed because the females think the profession is theirs, but we are focused and equally dedicated to our work and are always seeking further knowledge and skills which we impact in our work. Hence, our contributions and efforts should be acknowledged as the females since the number of male nurses is now rising which could help solve the nursing shortage. (P6)
Other participants highlighted perceived gender inequities in career advancement within the nursing profession, noting that male nurses are often overlooked for promotions and professional development opportunities.
In this facility when it comes to upgrading and promoting most of the time females are considered but it is time for males to be given equal opportunities since they are also needed in the nursing profession. This is one of the reasons male nurses do not stay in the profession for long. (P8)
Impact of disempowerment on nurse performance and workplace behaviour
This theme captures how lack of empowerment negatively influences nurses’ performance and workplace behaviours. Disempowerment was associated with reduced attentiveness, poor punctuality and diminished engagement.
Lack of empowerment impact attentiveness and punctuality as the nurse loses interest in his or her work and cannot concentrate so this can affect punctuality. (P2) It will let individuals go contrary to rules and regulations or not make nurses active at the workplace hence little effort will be given at work. It will also bring about reluctance at work because I feel I am not being given the necessary resources to work with. (P3)
Disempowerment also contributed to non-adherence to professional standards and reduced effort at work: If one is not empowered the person decides to do the work anyhow, and this will lead to malpractice and negligence which will endanger the life of the patients. (P5)
Disempowerment was perceived to negatively affect nurses’ performance, motivation and adherence to professional standards, with implications for patient safety and quality of care.
Theme 2: Organisational and leadership influences on nurse empowerment
Category 1: Psychological Empowerment (internal perceptions and experiences)
Category 1 reflects the psychological dimension of empowerment, capturing nurses’ internal perceptions and experiences within their work environment. Participants emphasised how feelings of motivation, recognition and support from leadership shaped their sense of value, confidence and willingness to perform effectively.
Role of motivation/recognition in nurse’s empowerment
Motivation and recognition, both verbal and material, were identified as key factors influencing empowerment. Expressions of appreciation, feedback and promotion were described as important sources of encouragement that enhance performance even under stressful conditions: Ok, I think the motivation of staff and then promotion of staff. That sweet feedback encourages us to do our best even when we are stressed unfortunately we are rarely motivated that is the sad part working in Ghana. (P2)
Support and reassurance from supervisors were also highlighted as powerful motivators, sometimes outweighing financial incentives: Nothing encourages us more than being supported and assured by our in charges, sometimes that alone motivates us more than the salary. (P4)
Motivation was described as a key driver of increased effort and engagement in nursing practice.
For me when I am motivated in what I do, it gives morale to do more. So, to empower staff nurses, managers should consider the motivation of the staff. (P10)
Category 2: Structural empowerment (organisational/workplace conditions)
This section focusses on organisational and workplace conditions that enable or hinder nurses’ ability to perform effectively. Participants highlighted the importance of supportive work environments, access to training, leadership practices and broader institutional and policy influences in shaping empowerment.
Creating empowerment conditions for nurses
A supportive work environment was identified as essential for fostering nurse empowerment, particularly where staff feel able to express themselves and experience reduced workplace stress.
I know that nurses are empowered to do their best when the work environment is very conducive, in that staff can express themselves in various ways. When shifts are made flexible also, they feel empowered because the stress on nurses will be reduced. (P2)
Effective communication and democratic leadership practices were also highlighted as key elements that enhance empowerment: Another way to increase empowerment is good communication, when there is good communication between staff and managers of the organization it fosters empowerment, especially leaders who are democratic really empower junior nurses unlike autocratic nurse leaders. (P6)
Respectful and empathetic relationships with leadership were identified as essential for fostering nurse empowerment.
There will be an empowerment when there is respect, empathy and understanding between staff nurses and higher authority at the work. (P18)
Staff training
Training was identified as a key factor in promoting nurse empowerment by enhancing knowledge, skills and confidence in practice.
Training of staff to build on their skills and knowledge makes them empowered, nurses are empowered when they are well versed with nursing knowledge and skills hence they carry their duties confidently unlike nurses who do not know their left from their right. (P7)
Ongoing training in current knowledge and skills was also emphasised as essential for sustaining empowerment: So, for me I guess staff nurses should be trained in current knowledge and skills for them to be empowered. (P10)
Gaps in leadership capacity were identified, with some nurse managers lacking the skills to effectively empower junior and novice nurses. Training in leadership and empowerment was therefore viewed as necessary.
Well, training nurse manager on how to empower other nurses is very essential since you cannot give what you do not have. Some of the workshops should address some of these leadership skills because it is a skill that has to be learned. (P16)
The need for targeted training across leadership roles, including preceptors and unit managers, was further emphasised: Most nurse managers are observed discouraging and sabotaging junior nurses simply because they lack knowledge in empowerment so I suggest more attention is channelled towards training nurses in charge, preceptors, and managers on empowerment. (P17)
Leadership challenges and barriers to empowerment
Participants deliberated on barriers to empowerment, and they listed several barriers to empowerment, particularly leadership-related factors such as favouritism, discrimination and negative perceptions of junior nurses.
For me, I think favoritism and discrimination hinder empowerment, especially nurses who are not favoured always feel suppressed and do not see the need to do things on their own and be optimistic and this is common in Ghana, sometimes how they addressed and recognize doctors are far better than nurses but we are all doing the same work for one goal. (P1)
Negative perceptions of junior nurses were also described as limiting their involvement in care and undermining confidence: Some nurse managers have the perception that their junior nurses have nothing good to offer and hence prevent them from engaging in patient care. This could lead to lack of confidence which hinders empowerment. (P2)
Certain leadership skills and lack of resources were indicated by some participants as a hindrance to empowerment.
Nurse leaders who are autocratic, they tend not to involve us in decision making and this makes us feel disempowered and if you feel like we have nothing (to offer) we also stay back and let you do it alone you don’t usually see this among doctors they are always doing things together and supporting one another. Also how can you be empowered when you do not even have resources to work with? How is this even possible. (P6)
Politics in nursing and empowerment
Involvement in politics was identified as a pathway for influencing policies, laws and regulations that affect nursing practice. Engagement in political processes was seen as a means to advance nurses’ interests and strengthen empowerment.
Nurse managers should get involved in politics so that they can do something about our salary and that will empower us. (P3)
The importance of representation in decision-making spaces was also emphasised: I think if a nurse gets involved in politics it will go a long way to help the nursing profession since most decisions are taken by those in politics and if we do not have nurses there, we will only carry out others ’ (directives) and not be part of formulating policies. (P6)
Participants further highlighted the limited visibility of nurses in political leadership; and the need for greater participation were further highlighted: For me, it’s okay for a nurse to be involved in politics because I think they can influence a change that will go a long way to empower the nurses in the job, but for now I do not even know any nurse who is at the core of politics and making change. If doctors are there a lot, what stops us from been there? (P7)
Political engagement was seen as a key mechanism for advancing nurse empowerment through representation, advocacy and influence on policies related to working conditions, remuneration and professional recognition, ensuring nurses’ voices are included in decision-making.
Discussion
This study examined how nurse manager-led empowerment influences nurses’ practice and care delivery in resource-constrained healthcare settings. Findings demonstrate that empowerment is shaped by the interaction between structural (organisational) and psychological (personal) factors, both of which are necessary to achieve meaningful empowerment. Structural empowerment was reflected in access to resources, participation in decision-making, supportive leadership and training opportunities, whereas psychological empowerment was evident in nurses’ motivation, confidence, sense of value and ability to act effectively. Consistent with literature, these dimensions are interdependent, as structural conditions influence nurses’ internal perceptions and engagement, ultimately affecting performance and quality of care (Khrais and Nashwan, 2023; Orłowska and Laguna, 2023; Messman et al., 2022).
Importantly, structural empowerment emerged as a critical foundation for psychological empowerment. Limited involvement in decision-making, inadequate resources and autocratic leadership practices constrained nurses’ access to power and participation. These structural gaps translated into psychological consequences, including reduced confidence, diminished sense of control, and disengagement. Although previous studies have described these outcomes (Cai et al., 2011; Trus et al., 2018), in this study they are interpreted as consequences of structural deficiencies, rather than introduced as new conceptual definitions. This distinction strengthens alignment between findings and theoretical framing.
To address these challenges in Ghana and similar low-resource settings, findings suggest context-specific and actionable strategies. At the facility level, nurse managers can adopt inclusive leadership practices, such as involving staff nurses in ward-level decision-making (e.g. shift planning, patient care protocols), creating regular forums for staff feedback and implementing transparent communication systems. Addressing discrimination and favouritism requires establishing clear institutional policies, equitable task allocation and accountability mechanisms within units (Hosseinabadi-Farahani et al., 2023). Recognition can be operationalised through low-cost strategies, such as verbal acknowledgement, performance feedback, peer recognition systems and opportunities for professional development (Jo and Shin, 2025). Additionally, strengthening mentorship structures and preceptorship programmes can support junior nurses and enhance confidence and skill development.
Although broader issues such as remuneration and staffing may be beyond the direct control of nurse managers, they can play an important advocacy role by highlighting resource gaps, communicating needs to hospital leadership and contributing to policy discussions (Zhu et al., 2024). In this study, improving practice environments refers to modifiable workplace conditions within the influence of nurse managers, including respectful leadership, supportive supervision, effective communication, access to essential resources and opportunities for training, even within low-resource settings.
Training was identified as a key mechanism linking structural and psychological empowerment. Providing continuous professional development enhances nurses’ knowledge and skills (structural), while simultaneously increasing confidence and competence (psychological). Equally important is training nurse managers in leadership and empowerment practices, as ineffective leadership was identified as a barrier to empowerment. This aligns with evidence that leadership development is essential for fostering empowering work environments (Christensen et al., 2024; Mackey, 2014).
Although gender-related experiences were reported by participants, these are interpreted within the broader context of empowerment. Specifically, accounts of male nurses highlight how inclusion, recognition and equitable opportunities shape psychological empowerment and professional belonging. Although nursing is a predominantly female profession that has historically faced societal undervaluation, male nurses may experience distinct forms of marginalisation and differential expectations within the profession (Appiah et al., 2021 Olgay et al., 2025). These findings underscore the importance of gender-sensitive but inclusive empowerment strategies that ensure equal access to leadership opportunities, participation in decision-making and professional development for all nurses. Although gender is not the primary focus of this study, it illustrates how empowerment processes are shaped by socio-cultural dynamics within the workforce.
Finally, participants emphasised the role of political engagement as an extension of structural empowerment. Involvement in policy and leadership spaces allows nurses to influence decisions related to working conditions, resource allocation and professional recognition positioning them as key drivers of meaningful healthcare reform (Gottlieb et al., 2021). In Ghana and similar contexts, strengthening nurses’ representation in policy processes may enhance both structural conditions and psychological empowerment by increasing nurses’ sense of agency and professional voice.
These findings highlight that improving nurse empowerment in low-resource settings requires multi-level interventions, including leadership development, supportive workplace practices, equitable policies and broader advocacy efforts. In contexts such as Ghana, increased participation in political and policy processes offers a critical pathway to strengthening both structural conditions and nurses’ perceived influence, ultimately advancing professional practice and health system outcomes. Addressing both structural and psychological dimensions is essential for strengthening the nursing workforce and improving quality of care.
Strengths and limitations of the study
This study provides novel insights into nurse empowerment within a low-resource healthcare setting in Ghana, addressing a significant gap in the literature where empirical evidence from African contexts remains limited. By adopting a qualitative descriptive approach, the study offers rich, in-depth accounts of nurses’ lived experiences, capturing both structural and psychological dimensions of empowerment. The inclusion of nurses across different ranks enhances the breadth of perspectives and strengthens the credibility of the findings. Additionally, the study highlights the role of political engagement as an emerging dimension of empowerment, extending current understanding beyond traditional organisational and psychological frameworks. This study has several limitations. It was conducted in a single regional hospital in Ghana, which may limit the transferability of findings to other settings with different organisational cultures, leadership structures or resource levels. Although purposive sampling ensured relevant perspectives, the small sample size (n = 17) may not capture the full range of nurses’ empowerment experiences. Data were based on self-reported accounts and may be influenced by recall or social desirability bias, particularly within hierarchical work environments. Finally, the study focused solely on nurses’ perspectives; inclusion of nurse administrators and other healthcare professionals could provide a more comprehensive understanding of empowerment dynamics.
Implications
Future research should examine nurse empowerment across multiple healthcare settings and regions to improve generalisability. Comparative studies of public and private hospitals may reveal structural influences on empowerment, whereas inclusion of nurse managers, physicians and administrators would offer a more comprehensive organisational perspective. Longitudinal studies are also needed to assess how empowerment changes over time and its impact on retention, burnout and patient outcomes in resource-constrained settings. Findings underscore the importance of supportive and participatory leadership that promotes autonomy, confidence and professional growth. Psychologically safe work environments where nurses feel valued and respected can enhance teamwork, reduce errors and improve care quality. Regular recognition, constructive feedback and equitable professional development opportunities are critical to strengthening empowerment and retention.
Nursing education should incorporate empowerment-focused curricula that build confidence, advocacy and leadership skills early in training. Mentorship, simulation and interprofessional learning can support assertiveness and collaboration, whereas addressing gender stereotypes can foster inclusivity and professional identity. At the policy level, frameworks are needed to formally recognise nurses’ contributions and ensure their participation in decision-making. Policies supporting equitable advancement, continuous development, fair resource allocation and nursing representation in health governance can significantly enhance empowerment and health system performance.
Conclusion
This study is among the first to explore how nurse empowerment facilitates action across multiple levels, including patient care, interdisciplinary collaboration, professional advocacy and policy engagement, demonstrating how empowerment fostered through leadership at the interpersonal level can drive both local and systemic change. This study shows that nurse empowerment in Ghana is shaped by both structural factors (e.g. leadership, resources and decision-making opportunities) and psychological factors (e.g. motivation, confidence and sense of value). Supportive and inclusive leadership, along with access to training and resources, enhance empowerment, whereas hierarchical practices and limited resources constrain it. Addressing gender stereotypes requires promoting equitable leadership opportunities and recognising the contributions of all nurses. Future research, including longitudinal studies, is needed to further examine how empowerment evolves over time and to evaluate interventions aimed at improving empowerment in low-resource settings.
Key points for policy, practice and research
Nurse manager-led empowerment enhances retention, autonomy and care quality in resource-constrained settings, reinforcing the need for supportive leadership structures in nursing practice.
Participatory leadership, recognition and inclusive decision-making are critical for fostering professional confidence and advocacy among nurses, with direct implications for workforce sustainability and patient outcomes.
Gender-sensitive empowerment strategies are essential to address stigma and inequities faced by male nurses, promoting inclusivity and retention across the nursing workforce.
Training in empowerment and leadership skills for nurse managers is vital to ensure consistent, equitable support for junior and novice nurses, especially in low-resource environments.
Supplemental Material
sj-pdf-1-jrn-10.1177_17449871261452951 – Supplemental material for Empowerment experiences of registered nurses and the role of nurse managers in Ghana: a qualitative descriptive study
Supplemental material, sj-pdf-1-jrn-10.1177_17449871261452951 for Empowerment experiences of registered nurses and the role of nurse managers in Ghana: a qualitative descriptive study by Stellah Appiah, Deborah Akua Badu, Joyce Ewurabena Mintah, Evans Appiah Osei, Hawah Amadu Toure, Edward Obeng Amoah and Lillian Agyemang in Journal of Research in Nursing
Footnotes
Acknowledgements
The authors wish to acknowledge the authors of all sources used, as well as the nurses and the administrators of the facility utilised for the study.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All relevant data supporting the findings of this study are available within the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.