
Abstract
Background:
Mistreatment, abuse, or neglect during childbirth is known as obstetric violence (OV), which is increasingly recognized as a human rights issue with significant public health impacts. Research shows that traumatic childbirth can profoundly affect maternal psychological health and undermine positive parenting. This study provides primary evidence on the link between OV and postnatal depression (PND) among rural women in Jharkhand, a region marked by social and infrastructural disadvantage.
Objectives:
(1) Estimate the prevalence and examine the predictors of OV during facility-based childbirth in rural Jharkhand, India, and (2) assess the association between OV and PND.
Design:
A longitudinal community-based study was conducted in two phases (antenatal and postnatal follow-up).
Methods:
Pregnant women in their second or third trimester (n = 246) were enrolled from the rural Chatra district employing a multistage sampling approach. Follow-up assessments were completed with the postpartum (n = 189) women. OV was measured using a typology aligned with World Health Organization and Bowser and Hill’s framework. PND was assessed using a Hindi-translated and reliability-tested Four-Dimensional Symptom Questionnaire. Logistic regression models were used to predict OV and to examine the association between OV and PND, while adjusting for sociodemographic factors.
Results:
Over half of the women (56.1%) experienced at least one form of OV. Physical abuse (47.6%) and non-dignified care (33.9%) were most common. Bribery demands, delivery in government facilities, and deliveries attended by nurses or midwives were the strongest predictors of OV. The prevalence of PND was significantly higher among women exposed to OV (55.7%) than among those who were not exposed (28.9%). The adjusted analysis showed that OV increased the odds of PND by more than threefold (odds ratio = 3.11, p < 0.01). Neglected care, non-dignified care, physical abuse, and privacy violations were significant predictors of PND.
Conclusion:
OV is widespread in rural Jharkhand and strongly associated with PND. Integrating respectful maternity care standards, improving accountability in public facilities, and incorporating routine mental health screening into maternal healthcare are essential to reduce the burden of OV and PND.
Keywords
Introduction
The mistreatment and abuse of women during childbirth, widely conceptualized as obstetric violence (OV), has gained significant attention in global health literature as a pressing public health concern. Recent studies have highlighted a variety of disrespectful and violent behaviors in obstetric care deliveries in many parts of the world.1–4 These include instances in which women are physically abused, humiliated, or sometimes abandoned by healthcare practitioners during pregnancy, childbirth, or the postnatal period. Vacaflor defines OV as “the violence exercised by health personnel on the body and reproductive processes of women (during pregnancy or delivery), as expressed through dehumanizing treatment, medicalization abuse, and the conversion of natural processes of reproduction into pathological ones.” 5 Although a critical public health concern, research on this phenomenon only gained attention in the late 2000s. Bowser and Hill’s landscape study on disrespect and abuse brought attention to the subpar treatment of women during childbirth, highlighting its systemic and widespread nature. 6 In 2014, the World Health Organization (WHO) highlighted the devastating nature of OV on women’s health, stating the mistreatment of women during delivery as a human rights violation. 7 It classified OV to include “physical violence, humiliation and verbal abuse, intimidation, forced medical procedures, neglect, lack of confidentiality, failure to seek consent, refusal to administer pain medications, avoidable complications, refusal of medical admission, and detention of women after delivery based on their inability to pay medical bills.” 8 OV counteracts the WHO’s objective for the quality of care for mothers and infants: communication, emotional and mental support, and dignity and respect. 9
Although the global prevalence of OV is unknown, a comprehensive systematic review of the prevalence of OV worldwide by Hakimi et al. revealed that 59% of women worldwide have experienced at least one form of OV during childbirth, with the most prevalent being non-consented care, making it a widespread phenomenon. 8 According to Martínez-Galiano et al., the prevalence of OV varies by country and ranges from 15% to 91%. 10 Recent studies on women’s experiences during childbirth in India have found evidence of disrespect and abuse experienced by women giving birth in medical facilities.11,12 Between 15% and 83% of women reported receiving any form of disrespect from healthcare providers while giving birth in a hospital.13,14 Women from low socioeconomic backgrounds are more likely to experience OV.15,16 Among women, there is a low level of awareness and a general normalization of OV, with many accepting such mistreatment without questioning. 14 In the Indian context, it is particularly important to understand the impact of caste, class, and religion on women’s experiences of OV. This is especially critical because medical care in India depends on the socioeconomic level, and upper-middle-class Indian women may have very different experiences than their working-class counterparts. 11 Moreover, the social determinants of respectful care delivery remain poorly understood in India.
The health and well-being of the mother and newborn may be adversely affected by mistreatment during childbirth in both direct and indirect ways. 17 Experiences of OV could deter women from utilizing health facilities for childbirth, thereby increasing the risk of birth complications and maternal mortality. 18 It also erodes trust in the healthcare system and can lead to severe psychological trauma.9,19,20 Although research on OV has gained much attention, only a few studies have examined the direct implications of OV on women’s mental health during the postnatal period, particularly postnatal depression (PND). The WHO estimates that 13% of postnatal women and 10% of pregnant women worldwide have mental illnesses. 17 Depression is the most common, with symptoms ranging from depressed mood, sleep disorders, feelings of worthlessness and guilt, excessive worry, difficulty concentrating, and suicidal thoughts. 21 This is even more profound from a community-based and rural area perspective, despite an increase in the amount of research reporting the prevalence and determinants of mistreatment of women in low- and middle-income countries. In India, the prevalence of PND ranges between 4% and 48.5% 22 ; however, its correlation has not been well established, demanding critical inquiry.
In a Spanish study involving 782 women, those who experienced verbal OV were twice as likely to develop PND, and those who experienced emotional (psycho-affective) violence were 2.65 times more likely to have PND. 11 In a French study of 123 women, 10.6% reported disrespect during childbirth, which was significantly linked to higher rates of postpartum depression 2 months after birth. 23 A global review of 21 studies found that women who experienced OV had postpartum depression rates between 17% and 47%, especially when they were young, less educated, or had limited support. 24
Focusing on rural India is particularly important because women in these settings often face multiple structural disadvantages that shape their maternity care experiences. Rural healthcare systems within Jharkhand experience high levels of shortage within their healthcare workforce and inadequate facilities for providing care to women during pregnancy and postpartum depression. Increased levels of staff shortage result in a greater need for accountability within the community, meaning that if the community does not have a way to hold healthcare workers accountable for their actions, they may experience disrespectful or neglectful treatment. Simultaneously, the lack of access to mental health services increases the likelihood for women experiencing postpartum depression not being identified and/or treated for postpartum depression. Social issues, including poverty, early marriage, and the marginalization of Scheduled Caste and Scheduled Tribe populations, only contribute to these vulnerabilities and poor maternal health outcomes. Due to the lack of available research surrounding OV and postpartum depression throughout rural India, primarily in Jharkhand, researchers must conduct more in-depth studies within this particular area in order to obtain a better understanding of the effects of the above social determinants on maternal and child health outcomes.
While general studies on OV in the Indian context abound, studies examining the correlation between OV and mental health are scarce. To date, no empirical, field-based research in India has specifically examined the association between OV and postpartum depression. In this context, the present study examines the prevalence and predictors of OV during facility-based childbirth in rural Jharkhand (secondary objective); and (2) to assess the association between OV and PND in the early postpartum period (primary objective).
Materials and methods
Study setting and participants
This community-based longitudinal study was conducted in two phases among women in rural areas of Chatra district, Jharkhand, India. This manuscript has been prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies, 25 and a completed STROBE checklist is provided as Supplemental Material.
The longitudinal community-based cohort study in the rural Chatra district, Jharkhand, India, was conducted in two phases. Phase I (antenatal assessment) was undertaken for pregnant women in their second or third trimester (⩾28 weeks gestation). Phase II (postnatal follow-up) is conducted around 6–10 weeks following childbirth. The follow-up interval was chosen to detect early PND symptoms while minimizing early postpartum physiological confounding. Ethical Considerations
Ethical approval and informed consent
The ethical approval was obtained by the Institutional Ethics Committee of the International Institute for Population Sciences (IIPS) in Mumbai (Approval Number: IIPS/ACAD/SREC/D/IO-25/2023 before starting the study. All study protocols followed the Helsinki Declaration’s ethical criteria. 26 Verbal informed consent was obtained from all participants prior to data collection and reaffirmed before follow-up interviews. Given the sensitive nature of the study themes (violence and mental health), participants were informed that participation was voluntary and that they could withdraw at any time without any consequences.
Participant protection and referral mechanisms
Comprehensive mental health services are still lacking in rural Jharkhand. Given the sensitivity of the discussed topic, many precautions were taken to protect the safety and well-being of participants. To prevent the inappropriate disclosure of information in household settings, all interviews were conducted in private locations. When women reported experiences of obstetric or domestic violence, they were provided with information about their legal rights and the availability of government helplines (181 and 1091), as well as community-level support options. Women who reported moderate to severe depression symptoms on the four-dimensional symptom questionnaire (4DSQ) were directed to contact a psychiatrist at the local hospital or the nearest referral clinic. In case of severe symptoms, participants were encouraged to seek emergency medical assistance from qualified health practitioners. Additionally, participants were informed about the locally available options for understanding various paths to care.
Sample size determination and sampling technique
The sample size was determined using Cochran’s formula for estimating a single proportion:

Assuming a 95% confidence level (Z = 1.96), a prevalence of common mental disorders of 15.3% from a rural Haryana study, 27 and a 5% margin of error, the minimum required sample size was 200. To account for potential non-response and attrition between antenatal and postnatal follow-up, the sample size was increased to 250.
A multistage sampling technique was applied using India’s administrative structure. The district of Chatra has two subdivisions, Chatra and Simaria, which are divided into administrative blocks and panchayats (the lowest administrative units). Using probability proportional to size (PPS), we selected eight panchayats in each block, ensuring proportional representation based on population. Within these panchayats, PPS was again applied to select 50% of villages, aiming for diversity. The sample frame, aided by Health Facility Staff and Female Community Health Volunteers, documented pregnant women’s details, and a random sampling approach was used to select the participants.
We did not conduct an a priori power analysis for multivariable regression models; therefore, the study may be underpowered for detecting associations in smaller subgroups or less prevalent forms of OV. This limitation has been acknowledged in the “Discussion” section.
Sampling representativeness
The sample characteristics closely match the demographic profile of rural Jharkhand, as per NFHS-5 data, despite the study being limited to one district. The State-level rural statistics are consistent with our sample’s distribution of caste groups (SCs/STs), female education levels, maternal age distribution, and the majority of public-sector facility deliveries. This similarity suggests that the study population is reasonably representative of the local context in rural Jharkhand.
Inclusion and exclusion criteria
The study included women in phase I who were pregnant during the recruitment period, in their second or third trimester (defined as ⩾28 weeks of gestation), were permanent residents of the selected rural villages in Chatra district, and were able to provide written informed consent. Only women who intended to deliver within the study area were eligible for enrollment. For phase II, eligibility was restricted to women who had a live birth and delivered in a health facility (public or private), and who were successfully followed up between 6 and 10 weeks postpartum. Women were excluded from the Study if they had a known pre-existing mental illness, cognitive impairment, or severe communication disability. Additionally, widowed or unmarried women were not included in the recruitment. A total of 246 pregnant women were initially enrolled during the antenatal phase of the study. During follow-up, 57 women were excluded from the final analysis due to miscarriage/stillbirth (n = 12), migration or could not be reached (n = 23), Infant death before follow-up (n = 10), or delivery at home (n = 12). The final analytic sample, therefore, consisted of 189 women (Figure 1).
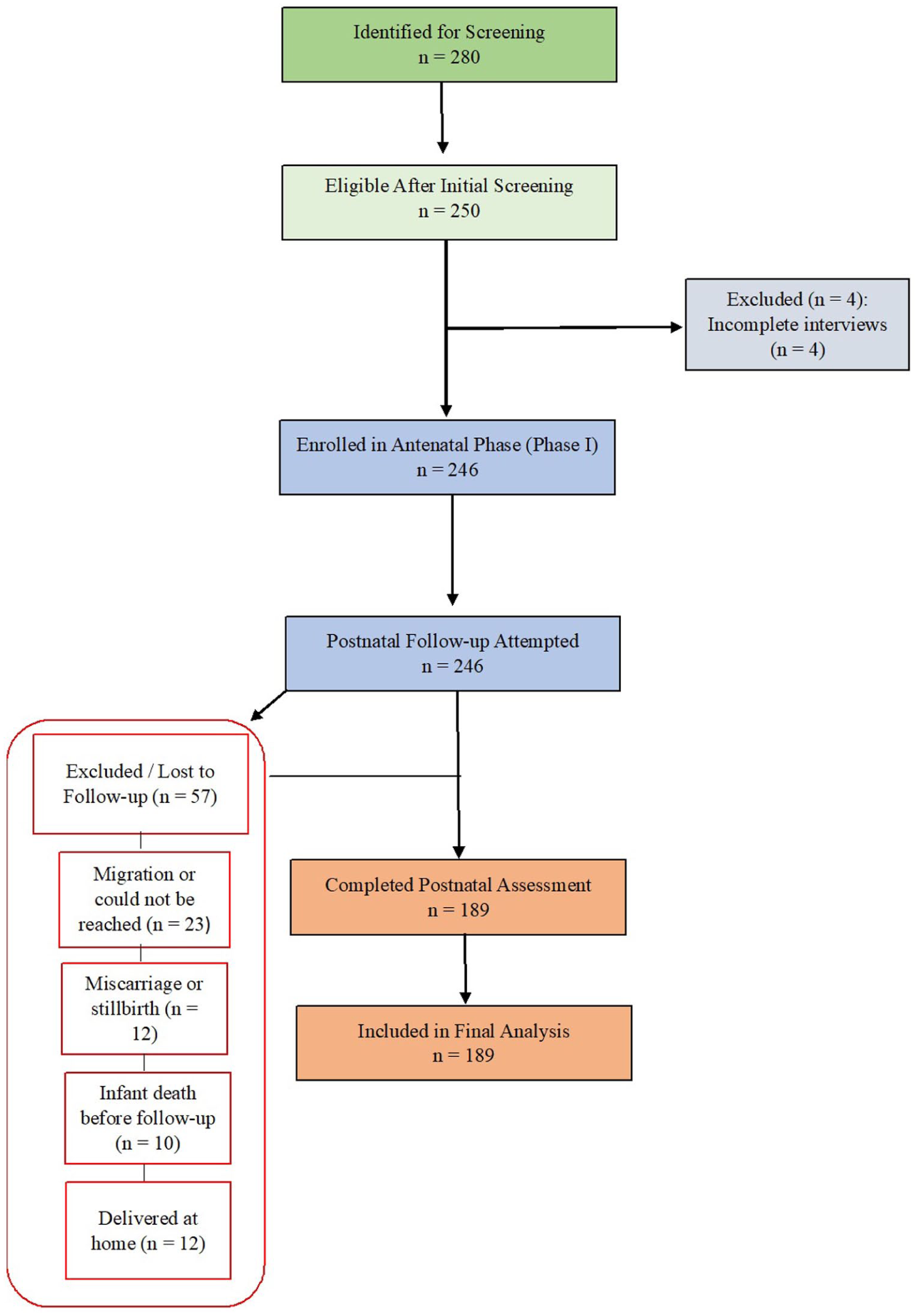
Participant flow diagram.
Data collection procedure and assessment tools
This study employed a longitudinal, community-based observational design consisting of two phases, through face-to-face interviews with the participants. The data collection periods for both stages were April 2024 to May 2024 and March 2025 to May 2025. The temporal evaluation of the impact of birthing experiences, including OV, on postpartum depression symptoms was made possible by this design.
In Phase I, pregnant women in their second or third trimester were recruited from government health sub-centers, Anganwadi centers, and outreach by Accredited Social Health Activists (ASHAs) across selected rural villages in Chatra district. After confirming eligibility, participants were approached at their homes or community health sites to obtain verbal informed consent and to be interviewed thereafter. During this phase, socio-demographic information and baseline data on maternal mental health were collected.
In phase II, postnatal follow-up interviews took place between 6 and 10 weeks after childbirth. This timeframe was chosen in accordance with WHO and international standards, which identify the first 6–12 weeks postpartum as a clinically relevant interval for screening for PND. Conducting the follow-up within this window ensured that symptoms reflected early postnatal mental health changes rather than transient, immediate postpartum emotional fluctuations.
Informed verbal consent was obtained from all participants prior to the interviews. According to Institutional Ethics Committee policies, written consent was not required due to the participant’s comfort level and understanding. Instead, verbal consent was documented by the interviewer on a standardized consent verification sheet, in accordance with the procedure approved by the Institutional Ethics Committee, ensuring privacy and confidentiality throughout the data collection process.
The structured questionnaire used in this study included items on sociodemographic characteristics, obstetric history, childbirth experiences, and mental health. The mental health component (4DSQ) is a validated instrument that has been widely used in community and primary care settings. The rest of the sections of the questionnaire were adapted from earlier research, WHO typologies of mistreatment, and previous Indian studies on maternity care experiences. The complete questionnaire was pilot-tested among 25 women (approximately 10% of the target sample) who were not included in the final study. The purpose of the pilot test was to assess clarity, cultural relevance, logical sequencing, and the feasibility of administering the survey through interviews. Based on feedback received during the pilot phase, minor modifications were made to the wording and arrangement of the questionnaire. A copy of the final version of the survey is provided in Supplemental Material 1.
The face-to-face interview assessed women’s disrespect and abuse during childbirth by healthcare providers. Self-reported information on OV was collected in seven types based on Bowser and Hill’ typologies of OV: “physical abuse, non-dignified care, neglected care or abandoned care, discriminated care, lack of privacy, detention in the health facility, and non-consented care.”
These questions were based on the questionnaire used in a large population survey of more than 2000 women conducted in Ghana, which aimed to determine the prevalence and associated factors of OV. 3 For all forms of OV, the questionnaires considered the entire time spent in the hospital, from arrival to discharge. Each question was coded as “yes” and “no,” and binary variables were created to indicate the occurrence of any form of OV. A positive response to each question was used to derive a score indicating OV. We have also conducted a reliability analysis, an independent check of Cronbach’s alpha, and obtained a score of 0.91 for the OV questionnaire in this study, which shows the high reliability of the questionnaire in research.
Although the Edinburgh Postnatal Depression Scale (EPDS) is widely used to assess PND, the 4DSQ was selected for this study for several reasons. First, the 4DSQ evaluates a wider range of psychological symptoms, such as somatization, anxiety, depression, and distress. This is especially important in rural Indian settings where somatic manifestations of psychological distress are prevalent. Second, the 4DSQ performed well throughout translation and pilot testing in this study and has demonstrated high psychometric qualities on a global scale. Third, the 4DSQ can be used to assess both antenatal and postnatal phases, while the EPDS is used only for postnatal screening. Thus, it enables us to maintain consistency of mental health measurements pre- and post-birth.
Although the Patient Health Questionnaire-9 (PHQ-9) is widely used to screen for depressive symptoms, it was not selected for this study. The 4DSQ is preferred over the PHQ-9 due to its exceptional scope and accuracy concerning the mental health status of perinatal women. Specifically, while the PHQ-9 assesses only depressive symptoms and contains physical symptom items that could be confused with changes associated with normal pregnancy, the 4DSQ effectively separates the dimensions of depression, anxiety, distress, and somatization. As such, the 4DSQ’s emphasis on cognitive and emotional symptoms diminishes the potential for misclassification and represents a much more specific instrument when used in community settings. In addition, the 4DSQ is considerably better suited to assess the multifaceted mental health effects of OV and prenatal stress.28–30
Since no Hindi version of 4DSQ was available, we translated the instrument and checked for accuracy by back-translation to English. 31 The data collection instrument was pretested in the pilot phase to enhance its validity and reliability. The internal consistency of the 4DSQ tool was evaluated using Cronbach’s alpha, which resulted in a value of 0.96. Additionally, we conducted an independent check of Cronbach’s alpha, which yielded a score of 0.94 for the depression scale.
Maternal mental health was assessed using the depression scale of the 4DSQ. Respondents provided answers to six questions on a 5-point Likert scale (0 = no, 1 = sometimes, 2 = regularly, 3 = often, 4 = very often or constantly), and the answers to each question were categorized into low (0), moderate (1), and high (2–4). By summing these values for all six questions, a depression scale (0–12) was generated, and those with a score of 6 or higher were categorized as depressed.28,30
Additionally, we utilized the National Family Health Survey-5 (2019–2021) questionnaire to learn about the participants’ socio-demographic profiles, other relevant characteristics, such as their experiences of intimate partner violence, and their spouses’ past or present consumption of alcohol and tobacco products.
Statistical analysis
The collected data were coded following a comprehensive review for accuracy and completeness. To validate the data accuracy, 10% of the samples underwent manual rechecking. Statistical analysis was conducted using STATA software version 17. Fisher’s exact tests were used to examine the association between the explanatory variables and the two outcome variables, OV and PND. We conducted a descriptive analysis of the prevalence of OV and then performed a multivariate analysis of the potential associated factors and OV. We assessed using logistic regression analysis, computing unadjusted and adjusted odds ratios (AOR), and examined whether the associations differed according to women’s antenatal depression status.
All logistic regression assumptions were examined prior to model estimation. Variance inflation factors (VIF) were used to assess multicollinearity between independent variables. The mean VIF for the OV base model was 2.22, indicating acceptable collinearity. The mean VIF for the PND base model was 1.98, indicating no evidence of multicollinearity. The Hosmer–Lemeshow goodness-of-fit test was used to assess model fit, 32 and both the OV (p = 0.59) and PND models (p = 0.68) were found to be well-fitted. A complete-case analysis was used to address the small percentage of missing data (<2%), as the pattern of missingness did not indicate systematic bias. Sensitivity analysis comparing models with and without specified covariates produced consistent results, showing the robustness of the findings. However, the sampling strategy involved a multistage selection process; adjustment for clustering was not implemented because the number of clusters at the village level was small and unequal, which may have produced unstable variance estimates. This limitation has been acknowledged in the “Discussion” section.
Results
Table 1 provides some of the background characteristics of the respondents, highlighting critical socioeconomic and health disparities in rural Jharkhand. The sociodemographic characteristics of participants broadly reflected the rural population structure of Jharkhand, supporting the contextual relevance of the sample. Most women (55.56%) were aged 20–24 years, and 28.57% were married before 18 years. Educational attainment is low, with 18.27% having no education and most (82.74%) being housewives. Notably, 41.27% of the respondents belong to the Scheduled Castes, and 72.49% live in extended families. Pregnancy-related data showed that 38.62% were primigravida and 26.46% had a history of pregnancy loss. Alarmingly, 68.78% of the women reported experiencing intimate partner violence during pregnancy, and 84.13% were asked for bribes to access healthcare. Most deliveries (81.48%) were vaginal births, and community health workers assisted in 78.31% of the cases, indicating limited access to medical professionals. Of the respondents, 42.33% reported birth problems, while 83.07% had no exposure to media, indicating a lack of access to health-related information.
Background characteristics of the study participants (n = 246).
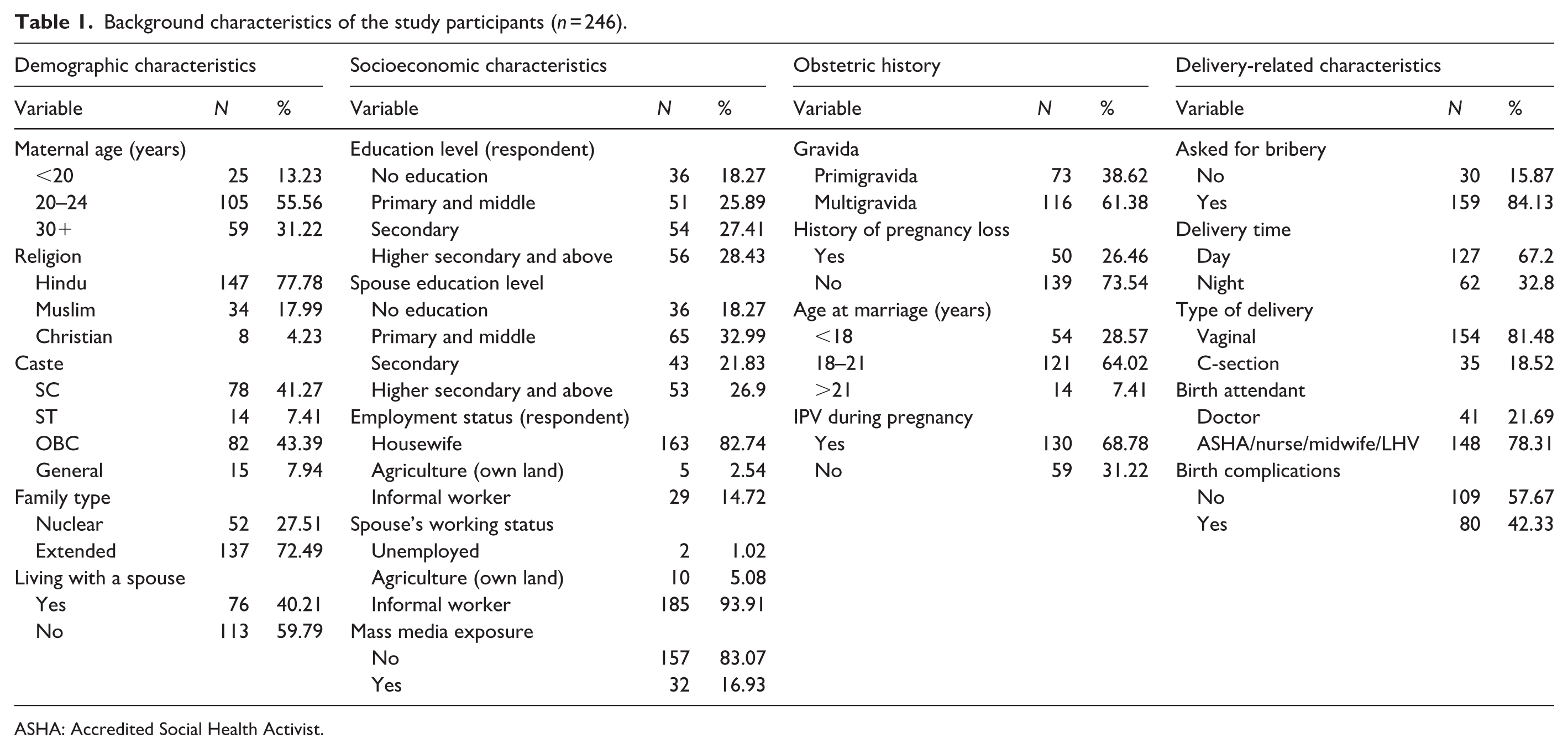
ASHA: Accredited Social Health Activist.
Table 2 reports the prevalence of OV in the study population. Overall, 56.08% of the women reported experiencing some form of OV during childbirth. Physical abuse was the most prevalent form of abuse, with 47.62% of the participants experiencing it. Specifically, 41.8% reported being held on their legs during delivery, 17.99% faced slapping, and 12.18% were beaten or pinched by the staff. Non-dignified care was the second most prevalent, with 33.86% of women reporting it, including shouting (30.16%), scolding (29.63%), and humiliation (17.99%). Restriction from reacting to pain was reported by 26.98% of the respondents, and 18.52% faced neglect or abandonment during care.
Prevalence and types of obstetric violence.
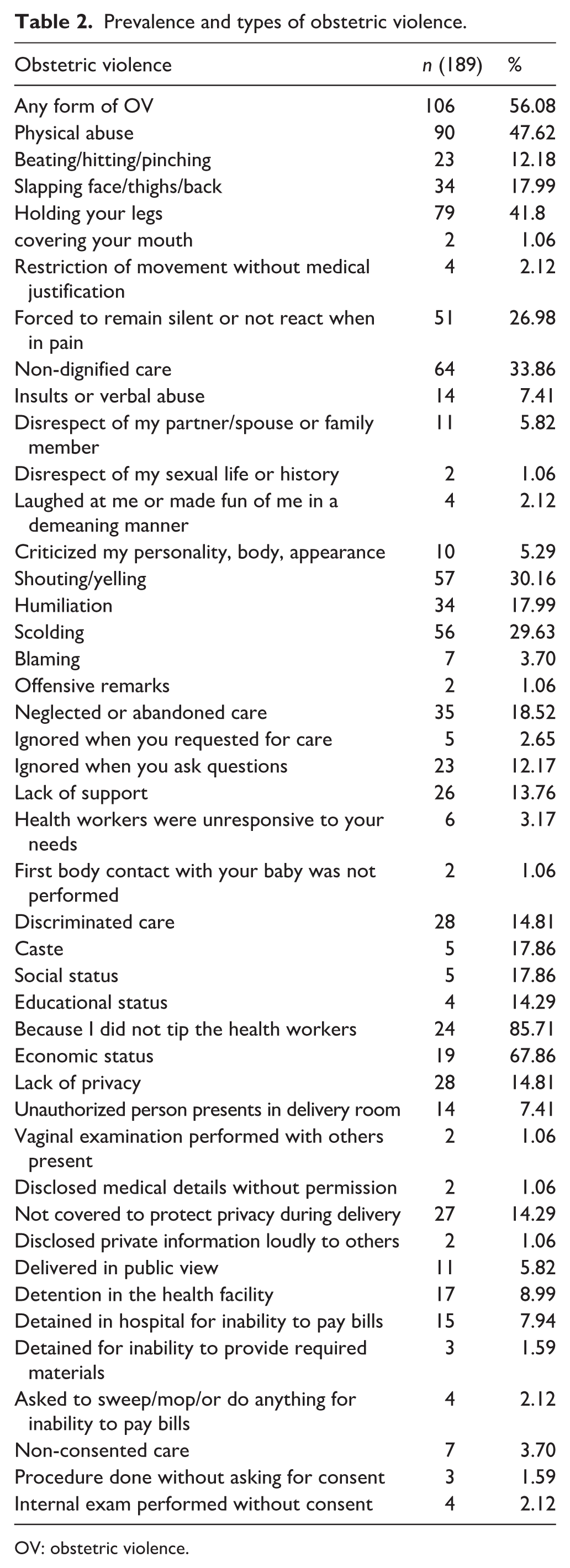
OV: obstetric violence.
Discriminated care affected 14.81% of respondents, primarily due to economic status (67.86%) and refusal to tip health workers (85.71%). Lack of privacy during childbirth was reported by 14.29% of the respondents, including being uncovered (14.29%), being delivered in public view (5.82%), and having others present in the delivery room without consent (7.41%). Non-consented care was also reported by 3.7% of the respondents, with some women subjected to internal examinations without their approval (2.12%). Detention in health facilities was reported by 8.99%, with 7.94% being detained for inability to pay bills on time.
The Fisher exact test was used to assess the association between OV and sociodemographic variables. Significant associations were found for asking for bribery (p = 0.000), religion (p = 0.008), caste category (p = 0.001), type of delivery (p = 0.000), birth attendant (p = 0.000), place of delivery (p = 0.000), and birth complications (p = 0.003).
Women who asked for bribes were more likely to experience OV (62.89%), and OV was higher among Hindus (61.22%) and SC/ST women (69.57%). Vaginal births had a higher OV incidence (64.94%) than C-section deliveries. Deliveries attended by ASHA/nurses observed 66.22% reporting OV, compared to only 19.51% for doctor-assisted deliveries. OV were more common in government hospitals (67.86%) than in private hospitals. Women with birth complications were significantly more likely to report OV (68.75%). Other variables, such as maternal age, family type, education, and work status, were not significantly correlated with OV (Supplemental Table 1).
Table 3 presents the results of the multivariable logistic regression analysis examining the relationship between specific sociodemographic characteristics and OV. The included sociodemographic factors are maternal age, education, caste, exposure to mass media, and family structure. All of the sociodemographic variables were examined for their predictive relationship with OV. However, of all the sociodemographic variables studied, the caste variable was found to be the only one to have a statistically significant association with OV, with women belonging to SC/ST caste groups reporting significantly greater odds of experiencing OV than women of the general caste category (AOR = 2.97; p < 0.10). There was no statistically significant relationship between age, educational attainment, type of family structure, or mass media exposure and OV.
Predictors of obstetric violence: base multivariable logistic regression model.
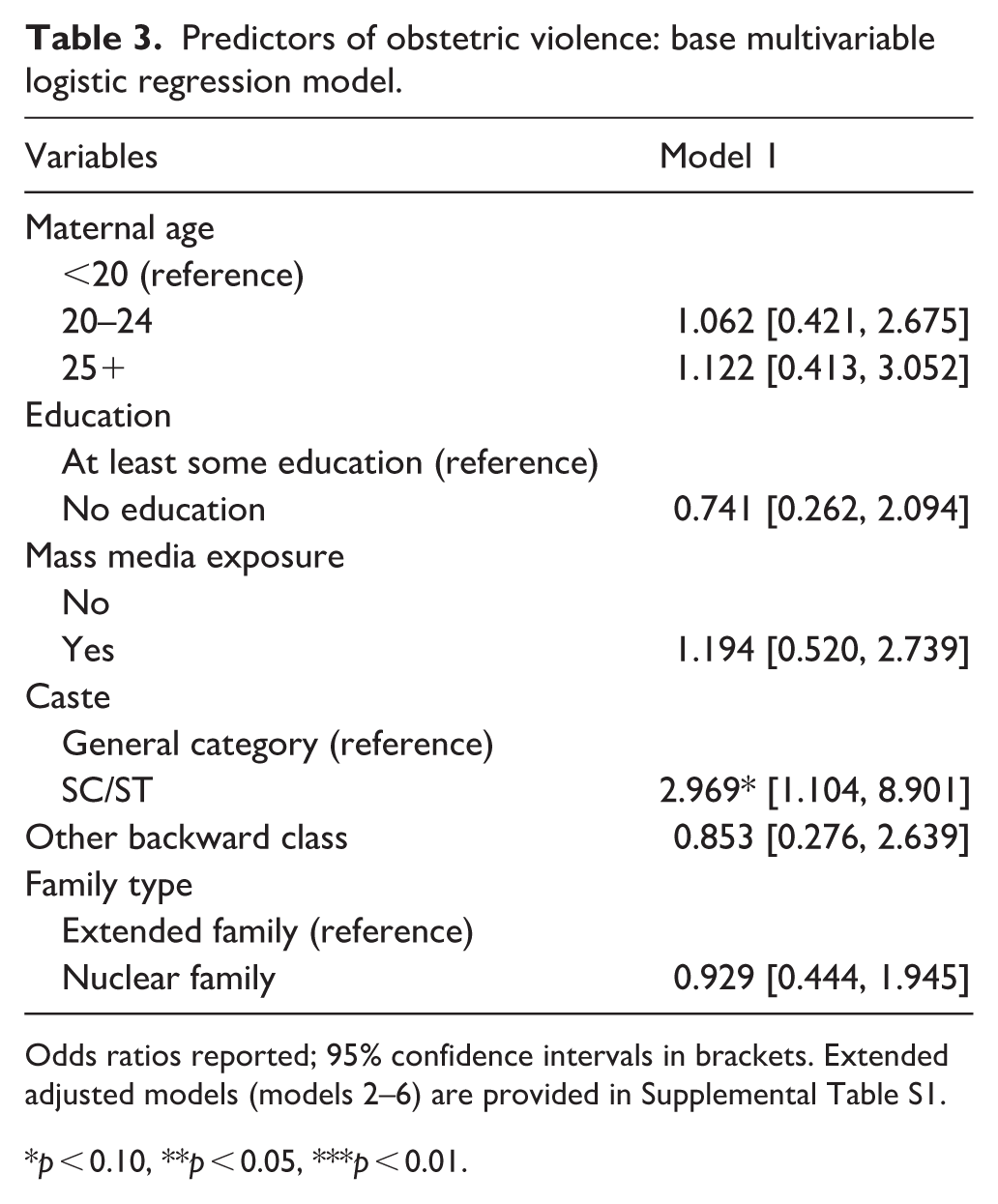
Odds ratios reported; 95% confidence intervals in brackets. Extended adjusted models (models 2–6) are provided in Supplemental Table S1.
p < 0.10, **p < 0.05, ***p < 0.01.
To further examine the contextual factors related to OV, an additional five adjusted models were created and analyzed, each using one of the previously identified childbirth or facility-related factors, along with all covariates from the original model. The results of these analyses are presented in Supplemental Table S1. Gravidity was included in model 2. However, gravidity did not significantly affect the likelihood of OV. In model 3, the question of bribery was introduced, and it showed a strong, significant association with the OV. Women who were asked for bribes were much more likely to report experiencing OV (ORs = 8.05; p < 0.01). In model 4, deliveries attended by ASHA workers, nurses, midwives, and/or LHV’s had much greater odds of experiencing OV than deliveries attended by a physician (AOR = 9.34; p < 0.01). Finally, women who delivered in public facilities were shown to have much greater odds of experiencing OV than women who delivered in private facilities (AOR = 8.77; p < 0.01). Finally, model 6 showed that vaginal delivery was strongly associated with OV, with women undergoing vaginal birth being more likely to report mistreatment than those who had cesarean sections (AOR = 10.25; p < 0.01).
Together, these findings indicate that while sociodemographic factors play a limited role, facility-level and care-related characteristics, bribery, provider type, place of delivery, and vaginal birth are strongly associated with OV in rural Jharkhand.
Correlation analysis revealed a significant association between OV and PND. Women who experienced OV were more likely to report depression (55.66%) than those who did not (28.92%), with a p-value of 0.000. Physical abuse (p = 0.001), non-dignified care (p = 0.000), neglected care (p = 0.000), and lack of privacy (p = 0.007) were strongly associated with PND. The strongest association was with neglected care, where 74.29% of affected women reported depression. However, discrimination, detention, and non-consensual care did not correlate significantly (Supplemental Table 3).
Table 4 presents the results of seven logistic regression models examining the factors associated with PND and the influence of OV on maternal mental health. In all models, maternal age, education, and low birth weight were not considerably associated with PND.
Multivariate logistic regression models of postnatal depression.
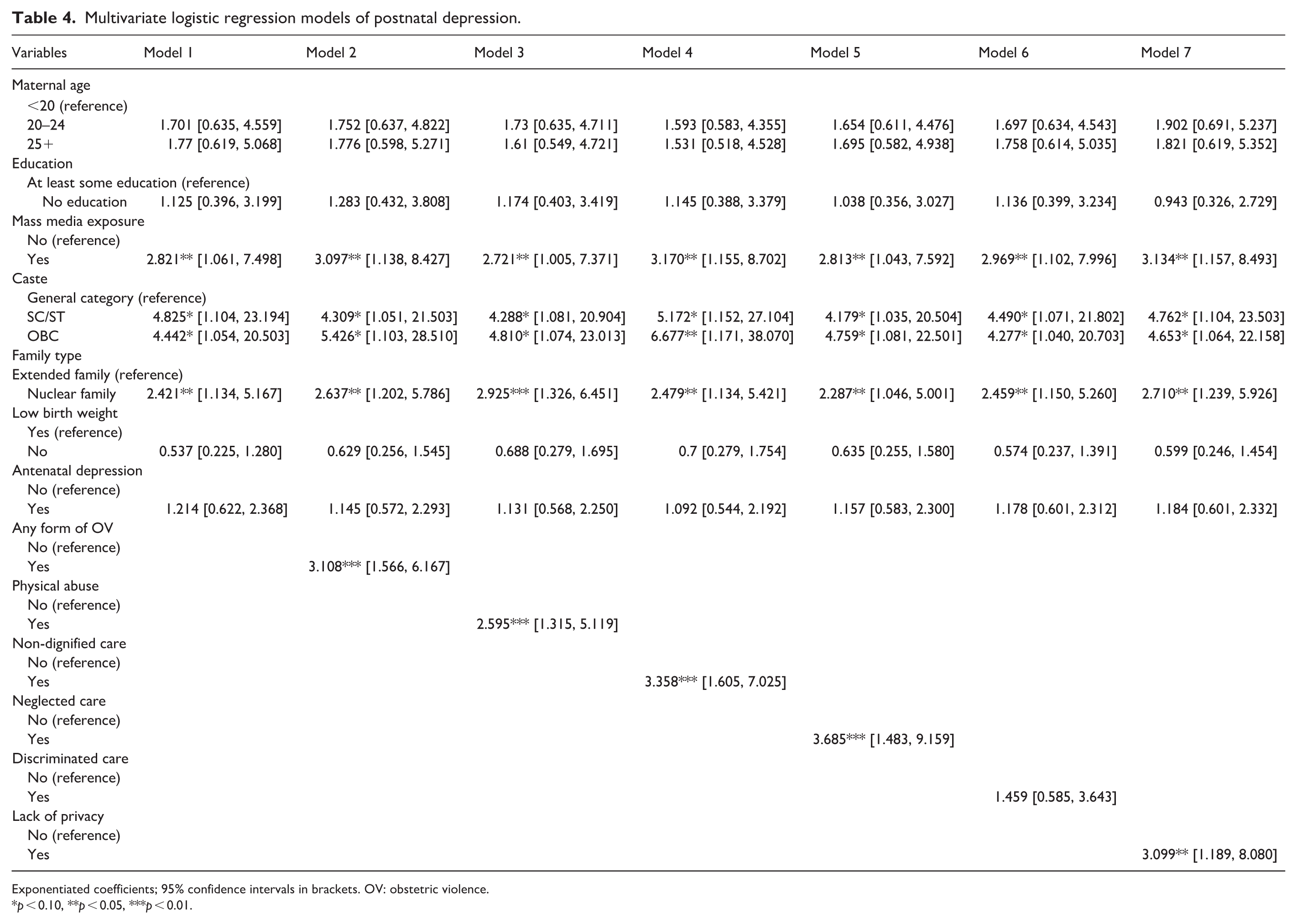
Exponentiated coefficients; 95% confidence intervals in brackets. OV: obstetric violence.
p < 0.10, **p < 0.05, ***p < 0.01.
Mass media exposure was a significant factor in all models. Women with no mass media exposure were more likely to experience PND, with odds ratios ranging from 2.721 to 3.170 and p-values <0.05 in all models. Caste was consistently associated with PND. In most models, women from the SC/ST and OBC categories had higher odds than those from the general category. In model 4, OBC women had the highest odds (OR = 6.677, p < 0.05), indicating a significant association. Family type was a significant predictor in all models. Women from nuclear families had higher odds of PND, with ORs ranging from 2.421 to 2.925 and p-values <0.05 in all models.
In model 7, the OV was a strong predictor of PND. Women who experienced any form of OV had an increased risk of PND (OR = 3.108, p < 0.01). Among specific forms of OV, physical abuse (OR = 2.595, p < 0.01), non-dignified care (OR = 3.358, p < 0.01), neglected care (OR = 3.685, p < 0.01), and lack of privacy (OR = 3.099, p < 0.05) were significant predictors of PND. Discriminated care was not significant, with an odds ratio of 1.459.
Discussion
The main aim of this research was to assess the relationship between PND and OV through a longitudinal study conducted in rural Jharkhand. This relationship was found to be substantial, suggesting women who had experienced abusive treatment during labor are highly likely to experience the same degree of postpartum depression symptoms. This is the first longitudinal evidence from rural India demonstrating that disrespectful or abusive maternity care has measurable mental health consequences in the early postpartum period. These findings contribute to the worldwide literature by showing this link in a low-resource, rural context where structural inequities, poor health-care capacity, and social vulnerabilities are likely to exacerbate the psychological impact of abuse.
The study findings are consistent with international studies that have linked negative childbirth experiences, traumatic intrapartum events, and disrespectful care with postpartum mental health difficulties, including depressive symptoms. However, most existing studies have been cross-sectional or hospital-based. By following women from pregnancy into the postpartum period, our study provides stronger evidence for a temporal relationship between OV and PND.
Our secondary goal was to investigate the prevalence and factors of abuse during childbirth, in addition to the mental health effects of OV. These contextual findings provide insight into the social and interpersonal aspects that influence women’s delivery experiences in rural Jharkhand, although they are not the primary focus of this research.
In our findings, more than half (56.1%) of the women experienced some form of OV (physical abuse, non-dignified care, neglected or abandoned care, discriminated care, lack of privacy, and non-consented care). While this prevalence is high, other studies have reported even higher rates: 99% in India,19,33 97% in Pakistan, 34 and 98% in Nigeria. 35 The variation in the prevalence rate can be attributed to several factors, such as the inclusion of only 4–6 weeks postpartum women, which could increase reporting bias. Furthermore, various survey instruments were used. The need for standard measurement tools to enable comparability in the definition of OV, the time of the survey to assess the same, and observed versus perceived abuse by women is therefore important. However, even if standardized methods are applied, differences in prevalence rates can be attributed to differences in facilities and other environmental factors. Therefore, it is important to consider the situation at the local level. 36
Our study’s findings are similar to those of another study conducted in India. A study of women who had given birth in health facilities in the unregulated settlements of Lucknow, India, indicated that over half of the women (54.7%) were mistreated during the delivery process. The most frequent form of mistreatment was verbal abuse (28.6%), followed by requests for money or bribes (24.2%). 16 A similar study from rural North India found that 84.3% of women experienced some form of disrespect or abuse during childbirth. 13 Widespread OV during labor and delivery, particularly verbal and physical abuse, has been documented in studies in various countries, including India, Brazil, and sub-Saharan Africa, highlighting systemic issues in maternity care.13,36–39
In our study, physical violence was by far the most commonly reported form of OV (47.6% of the entire sample), which raises great concern about the safety of women in the confines of the delivery rooms. Physical abuse is one of the most harmful and unjustifiable forms of mistreatment in maternity care; however, it is often normalized and underreported by women, especially in developing countries. This is because it is frequently seen by expecting mothers and medical professionals as a safe and efficient method of assisting women in pushing for a safe delivery.3,40,41 The influence of sociocultural values may be responsible for this finding. Therefore, more research is required to understand how sociocultural norms affect the behaviors of healthcare professionals and women giving birth.
Our findings also align with prior research from India. For example, Bhattacharya and Sundari Ravindran, in a study conducted in Varanasi, northern India, reported that 28.8% of women experienced some form of disrespect or abuse during childbirth. 9 Although this is lower than our estimate of 56.08%, the forms of mistreatment reported, such as physical abuse (47.62%) and shouting (36.16%), show consistent patterns across settings. 9 Specifically, they found that 17.3% of women experienced shouting or scolding, and 13.4% reported physical abuse; these rates are lower than those found in our study. Similarly, Sando et al. observed physical abuse in 5% of cases, which was notably lower than our findings, possibly due to differences in study settings and definitions of abuse. 36
In addition to verbal and physical abuse, our study documented several other forms of OV. For instance, approximately 3.7% of women in our study reported non-consented care, such as examinations performed without adequate explanation. Although lower than the 35% reported by Altahir et al., who found that many healthcare providers omitted consent or introductions before treatment, both findings point to persistent deficits in informed, respectful care. 42
Interestingly, our findings indicate that while allegations of mistreatment, such as verbal abuse and forced operations, increase during the second stage of labor, consensual care is more likely to be provided during the first stage. This supports the concern that, as delivery progresses, provider stress and institutional norms may undermine patient-centered procedures. 42
Privacy violations were another significant concern. In our study, 15.8% of women reported a lack of privacy during examinations in the labor room, and 14.3% noted they were not covered with any cloth or screen during delivery. Similar privacy violations have been reported in both Indian and international contexts. For instance, studies from Tanzania and India have documented compromises of privacy and a lack of dignity in labor wards of public health facilities.36,43,44 This includes cases where women were examined or delivered without adequate coverings or where non-medical personnel were present during delivery, highlighting a systemic disregard for respectful maternity care. 45 Our study identified a strong relationship between caste and OV, similar to other studies. Scheduled Castes and Scheduled Tribes women are more likely to experience OV, which could result from cultural discrimination, socioeconomic disadvantages, and structural biases.14–16,19
Our study revealed a higher prevalence of OV among women who were asked for extra money beyond the official cost. Bribery and corruption remain major problems in public institutions in India, and healthcare institutions are no exception. According to Sharma et al.’s study in India, over 65% of the women acknowledged being demanded for bribes, such as small informal payments (locally referred to as bakshish) within public health facilities during childbirth. 43 Similarly, Bhattacharya and Sundari Ravindran and Rajkumari et al. observed a high percentage of inappropriate money demands in the hospital setting (90.5%).9,46 Bribery and corruption inevitably predict the quality of services that women will receive from healthcare professionals, and also mistreatment. Studies outside India reported similar results. For example, in Ghana, Yalley et al. also found a correlation between OV and bribery, but the proportion of cases was much lower. 3
Where women deliver could greatly influence their experiences of mistreatment. 47 In this study, we found that the risk of OV in public health facilities was much higher than in private facilities (OR = 8.77, p = 0.000). In addition, the study also found that women were more likely to be mistreated by staff nurses and auxiliary nurse midwives (ANMs) than by doctors. 48 Hameed et al. have reported similar results. This could be due to greater patient loads and unfavorable patient-provider ratios in public hospitals.13,34,49 The majority of people in India (68.8%) live in rural areas (Census, 2011). In these areas, public health facilities such as primary health centers and community health centers provide most childbirth care. Healthcare providers in these settings are usually nearby health workers like ANMs and staff nurses, rather than doctors, with vaginal births being the norm. The correlation between the method of delivery (vaginal versus cesarean) and risk of OV is consistent with research on low-resource settings. Women who deliver vaginally through public health services generally have longer interactions with nursing staff and attendants during labor; therefore, there may be greater chance of experiencing mistreatment in the form of verbal abuse, disrespectful care, and neglect during labor. In contrast, cesarean section deliveries are typically performed by doctors under more stringent clinical protocols and monitoring, within relatively sanitary and controlled surgical settings, which may reduce exposure to behaviors associated with OV. As a result, there may be a lower chance of direct mistreatment and shorter patient-provider relationships. Additionally, rural hospitals in Jharkhand may have systemic challenges (e.g., over-crowded labor rooms, limited staff, and power-differentiated hierarchies), and these high levels of stress may cause staff to use more coercive and disrespectful treatment.50,51 Cultural norms that frame labor pain as a natural and expected part of childbirth may also lead to the normalization of harsh communication toward women during labor. Hence, poor rural women who give birth in public health facilities, with their babies delivered vaginally by ANMs and staff nurses, in resource-constrained public facilities may face a higher likelihood of experiencing OV. 52
Several emotional and social factors link OV to PND.24,53–56 Women can experience fear, humiliation, and loss of dignity as a result of disrespectful, neglectful, or abusive treatment during labor. Such traumatic experiences can erode a woman’s self-esteem, sense of security, and emotional health following childbirth.4,56,57 Women may develop negative memories of childbirth or experience ongoing anxiety after giving birth through obstetrical violence, which can lead to decreased mood and coping ability during the early postpartum period. 58 Emotional responses are well-documented to contribute to increased risk of being diagnosed with PND. 59
OV in many different forms can significantly impact a woman’s risk of developing PND.24,58 For example, women who experience verbal abuse, scolding, and being blamed during labor may feel humiliated or afraid of losing their dignity, and as a result, they do not feel emotionally safe. 59 Women experience powerlessness when health care providers disregard their requirements and speak to them in an unpleasant manner.60,61 When women are unattended to or neglected during their labor, this can intensify their feelings of anxiety and distress during an already vulnerable period of time.62,63 By coercive means, such as pressuring women into accepting procedures without adequate explanation as well as without informed consent, the resulting outcome will lead to the continued feeling of being violated as well as a continued loss of control over their bodies.20,64,65 Physical mistreatment or rough handling during labor is experienced as a traumatic event, which can lead to intrusive memories or emotionally numbing feelings associated with PND.34,53,66 Discrimination based on caste, socio-economic status, and social identity may worsen pre-existing psychosocial stressors and reinforce internalized feelings of inferiority or hopelessness.61,67,68 The combination of all of these forms of OV can threaten a woman’s psychological well-being and ultimately result in the development of PND.58,69
Our analysis of the correlation between OV and PND revealed that verbal and physical abuses during childbirth were significantly associated with a higher risk of PND, with slightly higher odds observed for physical abuse. Furthermore, experiences of undignified and neglected care were also linked to a boosted risk of PND. Harsh and scolding language, including threats against birthing women, is commonly used. Previous research indicates that women who are verbally abused during the antenatal and perinatal periods, even if they do not show symptoms of emotional distress, are more likely to experience PND. Similar results were found in our research.69–71 Souza et al. conducted a population-based cross-sectional study with 287 postpartum women in Brazil. They found that experiences of institutional violence in obstetric care, including physical abuse, were significantly associated with higher rates of postpartum depression. 69 Similarly, Janevic et al. conducted a survey-based study involving 1437 postpartum women in the United States during the COVID-19 pandemic. Their findings showed that perceived healthcare discrimination and lack of dignity in care were linked to lower childbirth satisfaction and poorer postpartum mental health outcomes. 47 These findings highlight the critical role of respectful maternity care and the quality of relations between women and health practitioners during delivery.
Among the various forms, neglected care emerged as the strongest predictor of PND.24,58 Women who were ignored or left without assistance during childbirth were more likely to experience depressive symptoms in the postnatal period. A similar study in Nagpur highlighted how neglect by family members and healthcare providers were associated with poorer maternal quality of life and postnatal mental health outcomes, indirectly suggesting a risk pathway for postpartum depression. 48 Violations of privacy also significantly increased the likelihood of PND, suggesting that exposure or lack of physical dignity in the labor room may leave lasting emotional distress. A 2017 study in Uttar Pradesh involving over 2600 women found that non-confidential care was among the most frequent forms of mistreatment. It was associated with increased odds of postpartum complications and indicated a high-stress birth environment likely to affect mental health outcomes. 15
In our sample, discriminatory care did not show a statistically significant association with PND. This is likely because structural caste-based inequalities are already captured through caste dummy variables in the model, limiting any additional explanatory value of reported discriminatory care. Qualitative studies have shown that marginalized women often normalize or underreport mistreatment.11,14,43,61,72 This cultural dimension may be more relevant to understanding reporting behavior than statistical associations in our analysis. This cultural dimension may be more relevant to understanding reporting behavior than statistical associations in our analysis.
Additionally, limited awareness of patient rights and low expectations from public healthcare services might reduce the psychological impact of discriminatory treatment, especially when compared to more direct and interpersonal forms of abuse, such as physical violence or neglect. 73 The emotional numbness or detachment reported by women who have faced chronic social discrimination can lead to lower scores on distress scales like the EPDS, not because the impact is lower, but because it is unacknowledged or unarticulated emotionally. One study from Pune showed that even though nearly 70% of women faced condemned or non-dignified care, many did not describe it as “abuse” because it was consistent with prior life experiences. 74
Strengths and limitations of the study
The study was based on a community-based longitudinal design, which allows for the evaluation of prenatal and postnatal experiences and strengthens the findings’ temporal relevance, one of its main advantages. Using standardized and validated instruments, including an adapted 4DSQ for mental health and a typology-based OV scale, ensures reliability and consistency in data collection. The study also contributes to the conversation on reproductive health equality by focusing on a marginalized group: women from Scheduled Castes, Scheduled Tribes, and low-income households. It gives important insight into the social determinants of maternal health outcomes. The findings are further supported by the strong internal consistency of both scales employed in this study (Cronbach’s alpha >0.90).
Despite these strengths, the study has some limitations. First, the sample size, though statistically adequate, was drawn from a single district, which may limit the generalizability of the findings to other regions or urban settings. The findings should be interpreted with caution and may not be directly generalizable to other regions of India where health system contexts and socio-cultural norms may differ. Second, self-reported data on depression may be subject to recall bias or social desirability bias, particularly given the stigma associated with both mental health. Third, due to the sensitive nature of the topic, some forms of mistreatment, especially discriminatory or non-consented care, may have been underreported. Additionally, the sample size was calculated based on prevalence estimation rather than a formal power analysis (see “Materials and methods” section). As a result, the study may have limited statistical power for subgroup analyses and for detecting associations with less prevalent forms of OV. This study follows a longitudinal design; causality cannot be definitively established, and unmeasured confounding factors, such as prior trauma or access to psychosocial support, may influence the relationship between OV and PND. Although the sample shared key sociodemographic characteristics with the rural population of Jharkhand, a direct comparison with all state- or national-level indicators was not possible; therefore, full representativeness cannot be assumed.
Future research
More research needs to be done on how OV (the mistreatment of women during childbirth) influences the mental health of women, especially those living in poverty-stricken rural areas, and over an extended time frame. Additional longitudinal studies are required to learn how disrespectful maternity care continues to affect mothering after the immediate postpartum period. Qualitative research is needed to gain a greater understanding of the experiences of women who have been victims of OV and to determine the local causes and contributors to OV that occur within the public health system. Additionally, to determine the effectiveness of training health care providers, improving working conditions in hospital labor rooms, or increasing provider accountability on eliminating OV and the resulting mental health consequences, intervention studies need to be conducted. A comparison of the experiences of women residing in different districts or states will also help determine whether systemic and cultural contributors exist that increase the risk of OV against women.
Conclusion and recommendations
Findings from this study represent the first longitudinal research focused on rural India. Findings conclude that OV correlates with PND. In this study, women who received disrespectful or abusive treatment while in labor were more than twice as likely to experience depressive symptoms at the beginning of the postpartum period. Other context variables that were associated with OV were demands for bribes, giving birth in public hospitals, who provides care to the woman, and giving birth vaginally. Preventing PND requires addressing all forms of disrespect and abuse and ensuring respectful maternity care. WHO guidelines and frameworks, such as RESPECT Women, emphasize dignity, consent, and freedom from harm, while tools like the Labor Care Guide support woman-centered care. Although India has introduced a number of nationwide programs to improve maternity care, such as Janani Suraksha Yojana, the National Health Mission, and LaQshya, but implementation remains uneven, and mistreatment persists. Limited gender-sensitive mental health services and social inequalities further weaken support for PND.7,52,55,75 In this context, strengthening the health system is essential, which includes improved training, consistent ethical standards, and strong national and state-level oversight. States can drive locally adapted reforms. Routine postnatal check-ups should also include mental health screening to enable timely detection and care.
Supplemental Material
sj-docx-2-whe-10.1177_17455057261442713 – Supplemental material for Obstetric violence and its association with postnatal depression: A longitudinal community-based study in rural Jharkhand, India
Supplemental material, sj-docx-2-whe-10.1177_17455057261442713 for Obstetric violence and its association with postnatal depression: A longitudinal community-based study in rural Jharkhand, India by Deepak, Dhananjay W. Bansod, Anke Hoeffler and Abena Asefuaba Yalley in Women's Health
Supplemental Material
sj-pdf-1-whe-10.1177_17455057261442713 – Supplemental material for Obstetric violence and its association with postnatal depression: A longitudinal community-based study in rural Jharkhand, India
Supplemental material, sj-pdf-1-whe-10.1177_17455057261442713 for Obstetric violence and its association with postnatal depression: A longitudinal community-based study in rural Jharkhand, India by Deepak, Dhananjay W. Bansod, Anke Hoeffler and Abena Asefuaba Yalley in Women's Health
Footnotes
Acknowledgements
We are grateful to the community health workers for their assistance in locating the respondents and to the field investigators who helped with data collection for the study. We also thank colleagues for their advice during the creation and improvement of the questionnaire. We appreciate the time and cooperation of the participating women and their families. The authors also gratefully acknowledge the funding support received from the Zukunftskolleg, University of Konstanz, through the ZUKOnnect Fellowship Programme.
Ethical considerations
Ethical approval was obtained from the Institutional Review Board of the International Institute for Population Sciences, Mumbai (document number IIPS/ACAD/SREC/D/IO-25/2023).
Consent to participate
During the survey, eligible women were interviewed in their homes by trained research assistants after being identified with the help of local. Informed verbal consent was obtained from all participants prior to the interviews. According to Institutional Ethics Committee policies, written consent was not required due to the participant’s comfort level and understanding. Instead, verbal consent was documented by the interviewer on a standardized consent verification sheet, in accordance with the procedure approved by the Institutional Ethics Committee, ensuring privacy and confidentiality throughout the data collection process.
To ensure privacy, all interviews were held in a quiet space within the participant’s home, away from family members or others whenever possible. To reduce disruptions and improve confidentiality, interviews were scheduled at times that convinced for the participants. During the fieldwork, no significant privacy-related issues were reported.
Data were collected through one-on-one interviews conducted under the direct supervision of the first author. To address the problem of illiteracy and guarantee the same strategy for all participants, interviews were chosen as the data collection process. Each interview lasted for approximately 30 min.
To minimize bias and avoid inconsistent explanations of terms, the research assistants explained all the terms from the 4DSQ and the OV questionnaire in simple language. They were instructed to follow a guide to provide explanations when needed. The research assistants were evaluated based on their ability to use the guide correctly during the pilot and main surveys. Only those who demonstrated competence were included in the actual data collection.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Deepak gratefully acknowledges the Zukunftskolleg for providing a grant that supported his research stay at the University of Konstanz during 2024/2025. Anke Hoeffler acknowledges financial support from the Alexander von Humboldt Foundation with sincere appreciation. The funders had no direct role in influencing the research. Open-access publication of this work was supported by the Publication Fund of the University of Konstanz.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The current study’s datasets are not publicly available due to privacy issues related to sensitive research. The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Artificial intelligence
This manuscript was supported by the use of generative artificial intelligence (Grammarly, ChatGPT) for language editing, text refinement, and assistance in improving clarity and structure. No AI tools were used to generate primary content, research findings, data analysis, or references. The authors reviewed and verified all AI-assisted edits for accuracy and take full responsibility for the final content.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.