
Abstract
Background
The menstrual cycle (MC), the use of combined oral contraceptives (COCs), and the presence of menstrual pain have long been overlooked factors in female athletes’ health. The influence of hormonal fluctuations and pain may not only alter perceived performance and trainability but could also induce changes in brain network connectivity.
Objectives
This study aimed to investigate whether resting-state functional connectivity (rsFC) differs between phases across the MC and COC cycle, as well as between naturally cycling (NC) subjects and COC users. A secondary goal was to explore associations between menstrual pain as a covariate and rsFC.
Design
Observational, longitudinal study.
Methods
NC women (n = 24) and COC users (n = 17) underwent a resting-state EEG recording during the early follicular phase (EFP) and pre-ovulatory phase (POV), and the active pill phase (pill phase) and inactive phase (pause), respectively. Mean characteristic path length (mCPL), clustering coefficient (CC), and mean debiased weighted phase lag index (mdWPLI) were computed for 37 participants (NC = 21; COC = 16). Phase and group differences were examined using mixed MANOVA, while mixed MANCOVA assessed the influence of menstrual pain as a covariate.
Results
No significant differences between MC or COC phases, as well as between groups, were found. Including menstrual pain as a covariate revealed significant phase*pain interactions for mCPL and CC, as well as significant group*pain interactions in mdWPLI. Post-hoc tests revealed a significant increase in mCPL from the pause to the pill phase.
Conclusion
The preliminary findings suggest that menstrual pain may influence baseline brain network states, which may have potential implications for performance and injury risk in female athletes. Therefore, considering menstrual pain is crucial in both research and applied sports contexts.
Plain Language Summary
Women’s health in sports research has long been underrepresented, especially regarding the menstrual cycle and hormonal contraceptive use. Many female athletes experience menstrual pain, yet its impact on the brain has not been well studied. Brain activity at rest (for example, while sitting quietly) shows how the brain organizes and processes information without a task. If this resting activity is altered, it may change how prepared the brain is for movement — with possible effects on performance and injury prevention. In this study, we recorded brain activity using electroencephalography (EEG) in 37 young women—some with natural menstrual cycles and some using combined oral contraceptives. Each participant was measured twice, at different phases of their cycle. We analyzed how efficiently different brain regions communicated with each other, focusing on whether pain during menstruation influenced these patterns. We found no overall differences in brain connectivity between menstrual cycle phases or contraceptive phases. However, when we took menstrual pain into account, changes appeared. The pain was linked to shifts in how the brain networks were organized. Specifically, pain seemed to alter the balance between communication across the whole brain and communication between adjacent regions. These patterns suggest that pain and hormonal phase together shape how the brain is “set up” at rest. Our findings indicate that menstrual pain is more than just a minor side effect of menstruation—it may alter brain states in ways that could potentially influence coordination, decision-making, and motor control during sport. However, our study did not test movement or sport performance directly, so we cannot determine whether these brain changes actually affect athletic performance. Nevertheless, the results highlight the importance of considering menstrual pain in both research and applied sport settings to better understand women’s health and performance.
Introduction
Men and women are biologically different in various ways, one of the most significant being the onset of the menstrual cycle (MC) in women at puberty. The MC involves fluctuations of the steroid hormones oestrogen and progesterone that may influence numerous physiological and behavioural factors. 1 In addition, menstrual disorders such as dysmenorrhea can occur and negatively affect participation in training and competition. 2 However, menstrual health is among the key health domains specific to cis-gender female athletes that have often been overlooked. 3 As a consequence, knowledge about the influence of the MC and dysmenorrhea on the central nervous system (CNS) as a key instance of motor control 4 is sparse.
Interestingly, the presence of oestrogen receptors in the CNS as well as the influence of oestrogen on the neurotransmitters glutamate and γ-aminobutyric acid (GABA) may already alter brain activity in the absence of movement.5,6 This state, referred to as the resting state, describes ongoing metabolic and electrical activity of neurons in the absence of a task or stimuli. 7
Resting-state network analysis, especially resting-state functional connectivity (rsFC), provides essential insights into the modulations in brain networks induced by intensive activities, 8 or sport-related injuries.9–11 Moreover, it is proposed that rsFC might reflect a ‘readiness’ state for movement, which could serve as an objective marker for regeneration in athletes.8,12 Thus, rsFC may represent an alternative to subjective questionnaires or objective motor assessments to evaluate general readiness for sport that is not biased by sports-related (e.g., fatigue, movement-related) artifacts.13,14 Assessing rsFC with electroencephalography (EEG) has the additional advantage of being non-invasive, cost-effective, and portable in the field.15,16 However, despite its potential for decision-making in training and therapy, to the best of the authors’ knowledge, no study has examined rsFC across the MC with EEG, representing a critical research gap.
Previous neuroscientific studies examining spontaneous EEG activity across the MC used frequency and power analyses17–21 and are mainly restricted to alpha frequency17,18,22,23 and specific electrode sites. 17 Although a comparison of results is challenging due to significant methodological differences (e.g., definition and verification of the MC phase, selection of electrodes), the available body of literature suggests that resting-state EEG activity may vary across the MC. However, reducing MC groups merely to hormone fluctuations ignores MC-related disorders that could influence brain activity, such as menstrual pain.
In previous studies, menstrual pain has often been examined in samples with diagnosed dysmenorrhea (e.g.24). The term dysmenorrhea refers to pain occurring before or during menstrual bleeding and is absent during the remainder of the MC. In the absence of pelvic pathology, menstrual pain is primarily attributed to increased prostaglandin production, which promotes uterine hypercontractility, reduced uterine blood flow, and subsequent ischemic cramping. This form is defined as primary dysmenorrhea and represents the most common gynaecological condition among individuals with a MC. 25 When menstrual pain is attributable to an underlying pelvic pathology, it is classified as secondary dysmenorrhea. 25 Among female athletes, dysmenorrhea is the most frequently reported menstrual disorder, with approximately one-third experiencing painful menstruation. 26
Pain modulates neural processes involved in the selection, planning, execution, and adjustment of action. 27 Consequently, pain affects motor behaviour by impairing motor control28,29 and, subsequently, pain-induced impairments in motor control could affect performance through inefficient selection, conduction, and correction of movement. 27 Thus, periodic pain like dysmenorrhea could significantly impact training and competition in female athletes.
Preliminary evidence from Liu et al. 24 comparing women with and without dysmenorrhea with functional magnetic resonance imaging (fMRI) suggests that rsFC is altered in brain regions associated with sensory and motor processing, including areas of the motor cortex and the cerebellum. Therefore, dysmenorrhea has been linked to deficits in motor control, as reflected by reduced postural control.30,31 Consistent with these proposed motor control alterations, athletes who reported a marked negative impact of the MC on overall physical performance during the early follicular phase (EFP) were more often affected by menstrual pain than those who perceived unchanged or positive effects during this phase. 2 However, current evidence about the menstrual impact of athlete performance either focuses on behavioural or CNS changes. One reason for this separation may be that much of the existing literature relies on MRI studies, which inherently restrict whole-body movement and complex motor task execution. In contrast, EEG can be implemented in mobile recording configurations, during movement, 16 allowing for the assessment of dysmenorrhea-related functional brain changes and their potential influence on motor control. However, a prerequisite is to establish whether EEG-based measures are sufficiently sensitive to detect dysmenorrhea-related alterations in rsFC under controlled conditions, thereby reducing the risk of misattributing connectivity changes observed during movement paradigms to menstrual pain rather than task-related or other confounding influences.
In a study of Ekenros et al., 2 13 % of the included elite athletes took oral contraceptives (OCs) to treat dysmenorrhea. OCs contain exogenous hormones that suppress the natural MC and are the second most common hormonal profile in cis-gender women of reproductive age. 32 The most common OCs are monophasic combined oral contraceptives (COC), which contain a synthetic progestin and a synthetic oestrogen. 33 It has been observed that synthetic hormones in COCs differ in their receptor binding affinity, metabolites, structure, functions, and pharmacodynamics from endogenous sex steroid hormones. 34 Hence, differences between COC users and individuals with a natural MC should be considered.
Given insights from brain research in sports science and recognizing that both the MC and COC may influence this activity through hormonal fluctuations and dysmenorrhea, exploring rsFC in this population is a crucial direction for future sports science research in female populations. To investigate the influence of the MC and COC on rsFC beyond endocrinological functions alone, comparisons between phases across the MC and the COC cycle might provide valuable insights as they represent different states regarding both, oestrogen levels and the presence or absence of pain. Therefore, this exploratory study aimed to investigate whether rsFC differs between MC phases and COC phases and between subjects with a natural MC and COC users. The secondary aim was to examine menstrual pain as a potential confounding factor in neurophysiological MC research.
Method
This observational study with a repeated-measures design was conducted between July 15, 2023, and May 13, 2024, at the Exercise Neuroscience Laboratory at Paderborn University. The study procedure was approved by the Ethics Committee of Paderborn University and conducted in accordance with the principles outlined in the Declaration of Helsinki. All subjects provided written informed consent before participation. The reporting of the study procedures and results adhered to the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist. 35
Participants
Recruitment took place in parallel with data collection between July 2023 and April 2024, utilizing flyers and posters at Paderborn University, as well as social media. Participants could register for the study without obligation via an online survey tool (LimeSurvey, LimeSurvey Community Edition, Version 3.28.17, LimeSurvey GmbH, Hamburg). During registration, they were asked to answer a series of screening questions to verify their eligibility for study enrolment. Eligible individuals received a standardized e-mail with detailed information about the study procedure.
This study was designed as an exploratory longitudinal investigation of brain activity across the MC and COC cycle, with the primary aim of characterizing temporal patterns and generating hypotheses rather than testing a single primary endpoint. At the time of study planning, there were insufficient data on expected effect sizes and within-subject variability for the specific EEG outcomes across the MC to support a robust a priori sample size calculation. Instead, the sample size was determined pragmatically based on feasibility, taking into account the longitudinal design and the participant burden associated with repeated measurements. Recruitment remained open throughout the data collection period to include as many eligible participants as possible within the available timeframe and resources.
Participants were eligible for inclusion if they were either naturally cycling (NC) individuals with a regular MC or COC users. NC was defined as having a regular MC not influenced by exogenous hormones (e.g., hormonal contraceptives) for at least nine months before participation. 36 A regular MC was characterized by a cycle length between 21 and 35 days, with a maximum variation of 7 days between cycles, 37 as well as confirmation of a luteinizing hormone (LH) surge and a correct hormonal profile at both testing appointments, as described below. To ensure regular MCs according to this definition, participants were asked to provide the onset dates of their three previous cycles. These data were transferred to a pre-customized Excel sheet, which included formulas for calculating mean, minimum, and maximum MC length, and MC length variability.
Eligibility criteria.
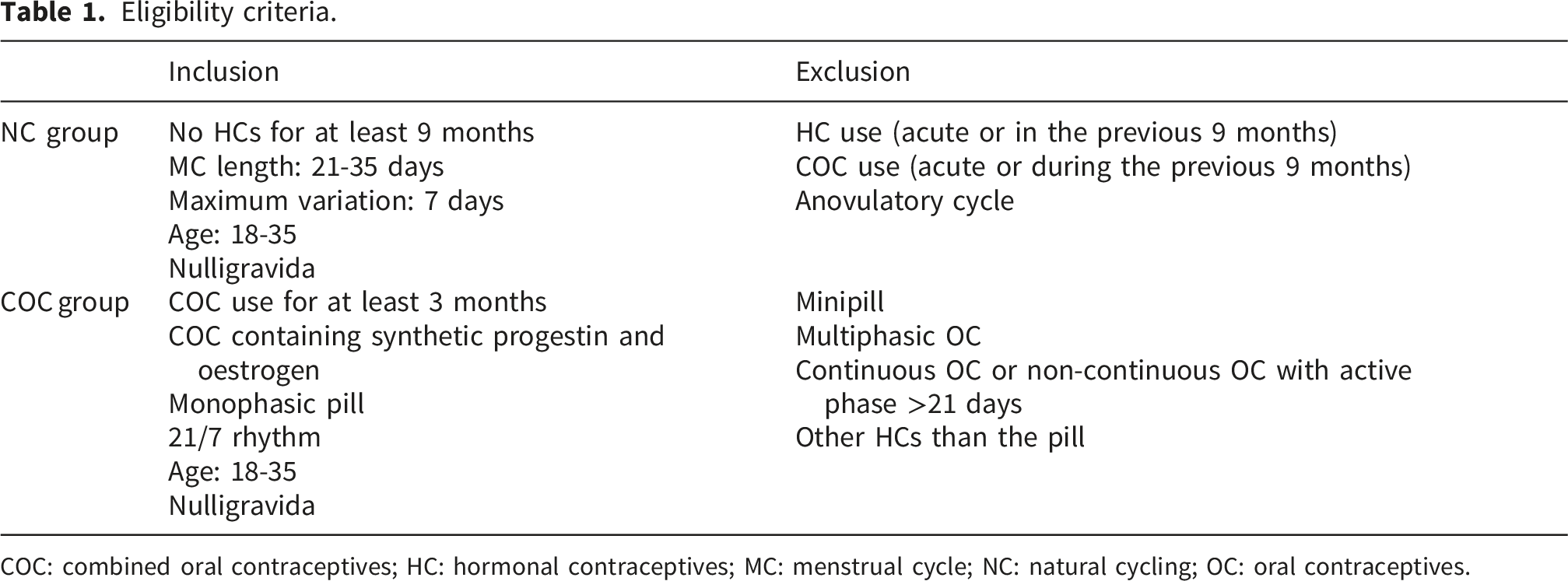
COC: combined oral contraceptives; HC: hormonal contraceptives; MC: menstrual cycle; NC: natural cycling; OC: oral contraceptives.
For both groups, participants were required to be nulligravida (i.e., individuals who have never been pregnant) and between 18 and 35 years of age. Exclusion criteria included a history of neuromuscular, vestibular, endocrinological, psychiatric, or neurological disorders. Additionally, participation was prohibited in cases of acute lower limb injury or any lower limb injury within the previous six months.
The recruitment strategy and inclusion criteria resulted in the enrolment of 90 subjects. Of those, 49 agreed to participate in the study and were enrolled in either the NC group (n = 29) or the COC group (n = 20). Out of the subjects who completed both measurements (NC = 24; COC = 17; Figure 1), one in the COC group was excluded because of poor electrode connection and three of the NC group because their hormonal profiles could not be assigned to the intended MC phases, leading to a total sample of 37 (NC = 21; COC = 16). COC: combined oral contraceptive; EFP: early follicular phase; HC: hormonal contraceptive; MC: menstrual cycle; NC: naturally cycling; POV: pre-ovulatory phase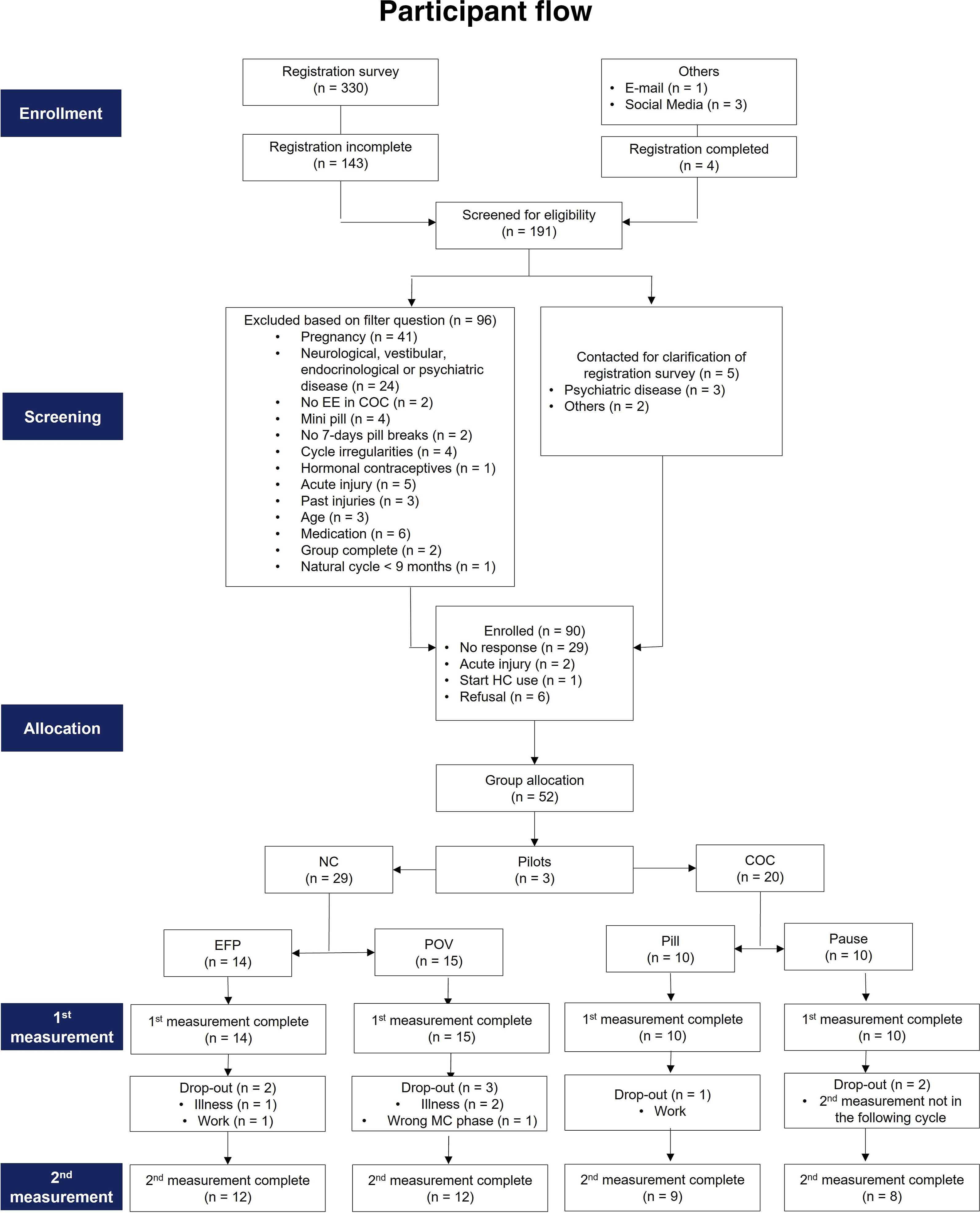
Procedure
Determination appointments
The EFP and the pre-ovulatory phase (POV) in the NC group, as well as the pill pause and pill phase in the COC group were analysed. These phases were selected for analysis due to their potential relevance to female athletes (i.e. self-perceived performance, menstrual pain),
2
and their distinct hormonal profiles
38
(Figure 2). A) Hormonal fluctuation during a menstrual cycle based on data from Stricker et al.
39
(scaled to a 28-day cycle for better comparability) B) Hormonal fluctuations during a 28-day oral contraceptive cycle for monophasic oral contraceptives containing ethinyl oestradiol, based on the data from Rodriguez et al.
40
Created in BioRender. Pohle, C. (2025) https://BioRender.com Yellow solid line: oestradiol; Blue solid line: progesterone; Yellow dashed line: ethinyl oestradiol; Blue dashed line: progestin; Grey shaded: measurement appointments; EFP: early follicular phase; pause: inactive/placebo phase; pill: active pill phase; POV: pre-ovulatory phase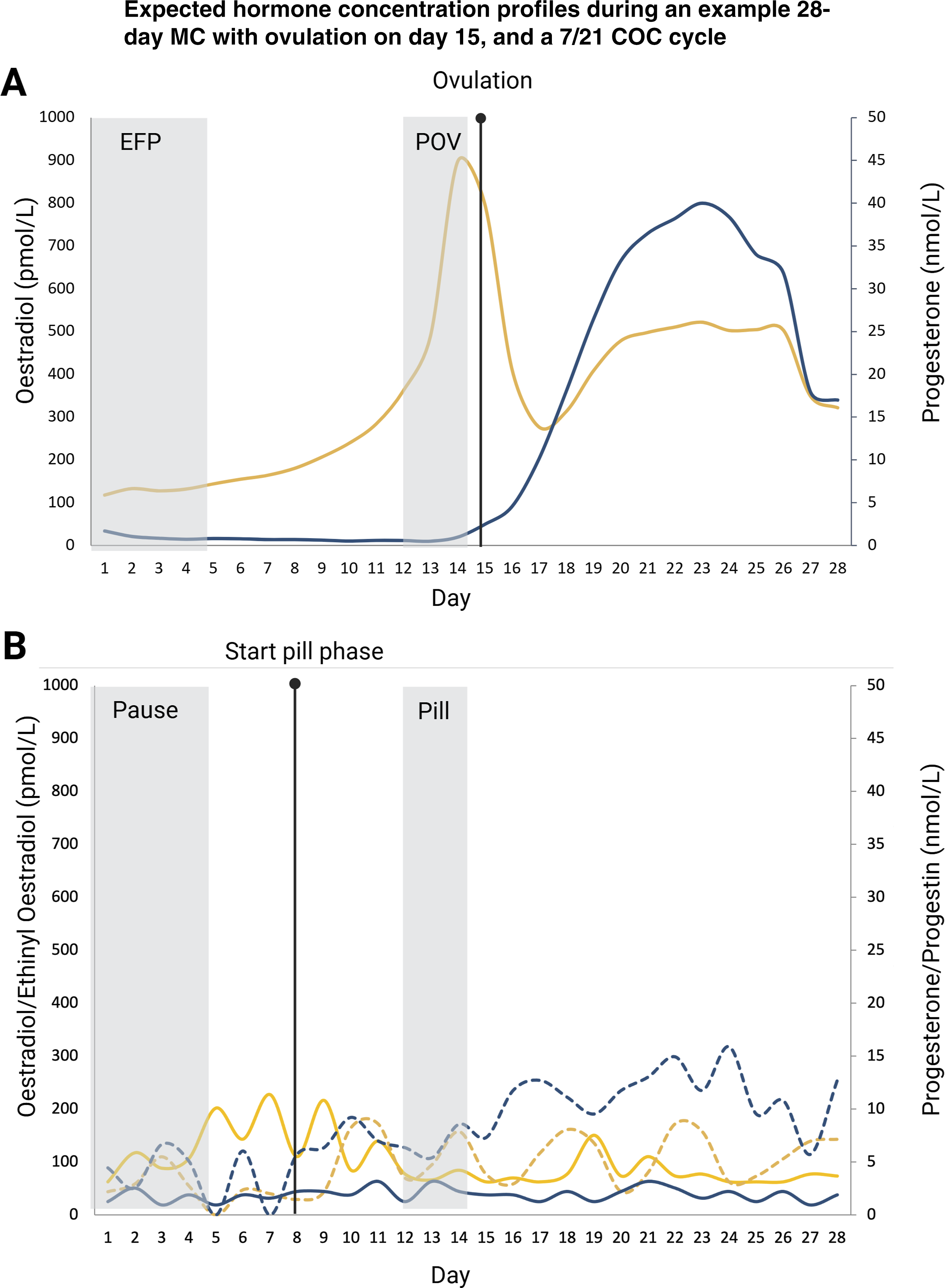
Start phases were randomized, with half of the participants starting in the EFP/pause and half in the POV/pill phase. To schedule the first appointment, participants in the NC group provided information about the start dates of their previous three MCs. Based on this information, the expected start dates of the next EFP and POV were estimated. Ovulation tests (OTs) with 99 % accuracy were used to detect the increase in LH concentration to determine POV (TESTAmed® DIAGNOSTICS Ovulation Test, Sebapharma GmbH & Co KG, Germany). The starting point for OT use was determined using the formula from Schmalenberger et al. 41 :
MC length – (expected luteal phase length + 4).
In this formula, MC length refers to the mean length of the participant’s three previous cycles. The expected luteal phase (LP) length was determined based on data from Bull et al.
42
. • MC length 21–24 days: LP = 11 days • MC length 25–30 days: LP = 12 days • MC length 30–35 days: LP = 13 days
.
Since POV was the phase of interest, OT use began four days before the expected ovulation. 41 The combination of self-reported data and OTs is considered an effective method for prospectively estimating MC phases. 43
The EFP measurement took place during menstruation (days 1–5), corresponding to phase 1 of the MC definition proposed by Elliott-Sale et al. 44 For the POV, the appointment was scheduled between 24 and 48 hours after detecting a light test line on the OT strip, ensuring alignment with phase 2, when oestrogen levels peak. 44
To investigate if differences between subjects with a natural MC and subjects who suppress the MC exist, COC users were measured during days 1-5 of the pause and on days 6–7 of the pill phase (equivalent to days 12–13 of the new COC cycle). Originally, days 6–7 of the pill phase were planned to align with the POV. However, due to variability in ovulation timing, the measurement schedule was adjusted during data collection.
Participants in the COC group were tested at least two hours after pill intake to avoid measurements when exogenous hormone concentrations peak. 45 Assumed hormone concentrations for the respective MC and COC phases are shown in Figure 2.
Menstrual pain
In this study, menstrual pain refers to pain occurring during menstruation or withdrawal bleeding. To exclude ovulation pain or pain unrelated to the MC/COC cycle, both MC-related pain and other pain were assessed at both appointments.
Following the approach of Stallbaum et al., 31 menstrual pain was evaluated using a combination of a generic pain measure for assessing pain intensity and a drop-down selection of body regions, with an additional field for specifying other affected areas (Supplementary material A). Pain intensity for each affected body site was quantified using a numerical rating scale (NRS) ranging from 0 (kein Schmerz; English: no pain) to 10 (schlimmster vorstellbarer Schmerz; English: worst imaginable pain). The NRS has demonstrated good validity, reliability, and sensitivity in assessing menstrual pain. 46
Test procedure
Upon arrival at the laboratory, written and oral information about the study procedure, data security, and participants’ rights has been provided, and all participants signed the declaration of consent.
During the first appointment, demographic characteristics of individuals (age, body height, body mass, BMI), anamnesis and information regarding HC history were assessed.
Preparation of the subject
After completing the anamnesis, a mobile EEG system (LiveAmp, Brain Products, Germany) with 64 Ag/AgCl active electrodes on a tight-fitting cap (actiCap, Brain Products, Germany) was placed on the participant’s head to record cortical activity continuously. The cap size was selected based on the individual’s head circumference. Electrodes were positioned according to the international 10-20 system, with AFz as the ground electrode and FCz as the reference electrode. Impedance levels were kept below 25 kΩ. A wireless EEG amplifier (LiveAmp 64, Brain Products, Germany) was secured in a tight-fitting yet comfortable belt worn by the participant. To ensure consistency across repeated measurements, electrode locations relative to three anatomical landmarks (nasion, right and left preauricular points) were scanned using BrainVision CapTrack (Brain Products GmbH, Germany).
Subsequently, participants were seated comfortably in front of a white wall, with white partition walls on either side to minimize visual distractions. They were instructed to gaze at the wall with their eyes open during a 5-minute resting-state measurement.
Saliva samples
To retrospectively verify MC phases, endogenous oestradiol and progesterone levels were analysed using saliva samples. 43 Saliva samples were collected at least one hour after eating, following a mouth rinse with water. The unstimulated passive drool method was used, employing 15 ml Greiner tubes (Moonlab® Plastics, Zentrifugenröhrchen, 15 ml, steril, PP). In total, three saliva samples were taken throughout the study. The first sample was collected immediately after the resting-state EEG measurement. Samples were stored in a cooling box during the experiment and later frozen at -25°C at the Sport Science Laboratory, Paderborn University.
Before analysis, saliva samples were centrifuged twice (15 min and 10 min, respectively) at 3000 rpm using an Eppendorf 3750 centrifuge to remove particulate matter. The three samples were then pooled for the analysis. Because salivary oestradiol shows ultradian fluctuations across the whole MC,
47
combining the three samples provides a more reliable estimate of mean hormone levels across the experimental session,
48
without compromising the ability to distinguish between MC phases.
49
• Oestradiol levels were measured using the high-sensitivity Oestradiol in Saliva ELISA (Salimetrics; sensitivity: 1 pg/ml). • Progesterone levels were assessed with the Progesterone in Saliva ELISA (DeMediTec; sensitivity: 10 pg/ml).
All samples were analysed in duplicate, with re-analysis conducted if the duplicate variability exceeded 25%. Study inclusion required higher oestradiol levels during the POV than the EFP, while progesterone concentrations should not differ significantly between phases.
POV sessions were included if backward counting confirmed a cycle day between -19 and -12, and oestradiol levels were higher during the POV than the EFP. 50
Two participants were included although they had slightly higher oestradiol values in the EFP, since the backward-counting fit, and measurements occurred on day two of the MC, where oestradiol levels might be elevated from the previous MC. 49
EEG analysis
EEG data were imported into the EEGLAB toolbox v.2023.1 51 for MATLAB (Version R2023a, MathWorks Inc., Natick, USA). EEG signals were first downsampled from 500 to 256 Hz. Afterwards, sinusoidal noise was removed by applying the CLEANLINE filter 52 at 50 and 100 Hz, and the signal was then band-pass filtered using a basic finite impulse response filter between 3 and 40 Hz. Data were manually screened for artifacts, and bridged channels were removed using the eBridge function (m v0.1.01 53 ). Automated subspace reconstruction (clean_rawdata EEGLAB plugin 54 ) and interpolation of bad channels were conducted to correct transient or large-amplitude artifacts (burst criterion k = 10 55 ). EEG data were re-referenced to the common average to restore FCz, and electrode locations were replaced using data from the electrode position scan (BrainVision CapTrack, Brain Products GmbH, Germany) for more precise localization of EEG signals.
After cleaning the data, the AMICA-independent component analysis algorithm 56 was applied to decompose the preprocessed data into spatial, temporal, and functional maximally independent components. Based on the source-space decomposition, components representing non-brain activity were removed using the ICLabel toolbox. Here, components containing artifacts such as channel noise and functional, non-brain activity—including muscle activity, eye activity, electrocardiogram signals, and sweat—were removed from the data. The pruned data were then epoched into sequences of 8 seconds, with a phase overlap of 4 seconds per epoch. 8 Since most participants needed a few seconds to settle after the beginning of the recording, the first three epochs were removed from the analysis. Hence, 45 epochs were analysed per participant.
Data were transferred to the MATLAB toolbox FieldTrip for rsFC analysis (FieldTrip-lite20240111 57 ). First, a frequency analysis with multiple tapers based on discrete prolate spheroidal sequences and spectral smoothing at 2 Hz was performed to compute cross-spectra. Afterwards, the mean debiased weighted phase lag index (mdWPLI) was calculated at the scalp level for the frequency bands of interest (theta: 4-8 Hz; alpha-1: 8-10.5 Hz; alpha-2: 10.5-13 Hz), resulting in 65-by-65 matrices for each subject and condition within the respective frequency bands. 8 These frequency bands were selected because theta and alpha oscillations represent the most examined frequency ranges in resting-state EEG studies investigating neural activity across the MC and during COC use.17,19–21 In addition, prior EEG research has shown pain-related alterations in theta and alpha oscillatory activity. 58
The mdWPLI matrices were imported into the Brain Connectivity Toolbox. 59 According to Vecchio et al., 60 weighted undirected networks were selected to obtain more precise information on the degree of connectivity between two nodes. To derive graph-based brain network metrics, mdWPLI values were normalized by converting them to a range from 0 to 1 based on the real range of respective mdWPLI values. 8 The mdWPLI is a measure of functional connectivity that indexes phase synchronization between two sources (e.g., brain regions). Its low sensitivity to noise and volume conduction enables accurate identification of true phase synchronization. 61
The graph measures mean characteristic path length (mCPL) and clustering coefficient (CC) were computed for each epoch. The average value across all channels was calculated to obtain the global graph measures. To normalize mCPL and CC, individual values were divided by the mean of all other values across the respective frequency bands. 60 The mCPL is a measure of network integration, computed by averaging the shortest finite distances between any two nodes. A short mCPL implies that, on average, every node can be reached from another node via a few intermediate nodes, which is characteristic of more efficient communication between nodes. 62 The CC is a measure of local segregation, describing the interconnectedness of a node’s neighbours. 62
Statistical analysis
Descriptive statistics were used to compare demographic data and menstrual pain between groups. To test for differences in demographics and hormonal status, t-tests were used. A mixed multifactorial analysis of variance (MANOVA) was used to analyse mCPL, CC, and mdWPLI, respectively, with oscillations in the theta, alpha-1, and alpha-2 frequency ranges as factors. Since frequency bands are associated with distinct, sport-relevant cognitive functions 63 and are associated with independent modulatory processes in the pain literature, 64 the explorative univariate analyses were conducted separately for each frequency band. To control for the influence of menstrual pain, pain severity (the highest score on the NRS in any body region) was integrated as a covariate in a multifactorial analysis of covariance (MANCOVA). Statistical significance was set at p ≤ 0.05. Post-hoc tests were corrected for multiple comparisons using FDR-correction, 65 as recommended by Durka et al. 66 Partial eta squared (η2) was computed to estimate effect size. According to Cohen’s (1988) convention, effect sizes were interpreted as small (0.01), medium (0.06), or large (0.14). 67
Results
Participant characteristics
The analysis of oestradiol and progesterone revealed the expected main effect of MC phase on oestradiol (F (5.194), p = 0.029) but not on progesterone (F (0.078), p = 0.781). Additionally, there was a phase*group interaction effect for oestradiol (F (35.00), p = 0.004).
Pairwise comparisons confirmed higher saliva oestradiol levels in the POV (1.394 ± 0.113) compared to the EFP (1.029 ± 0.122; b = 0.354; SEb = 0.09; p < 0.001) in the NC group, while no significant differences were observed for progesterone. The NC and COC groups differed in oestradiol concentration during the POV/pill phase, with higher values in the NC group (b = 0.455; SEb = 0.171; p = 0.012). As expected, there were no significant differences between phases for oestradiol or progesterone concentrations in the COC group.
Demographic data of the study population.
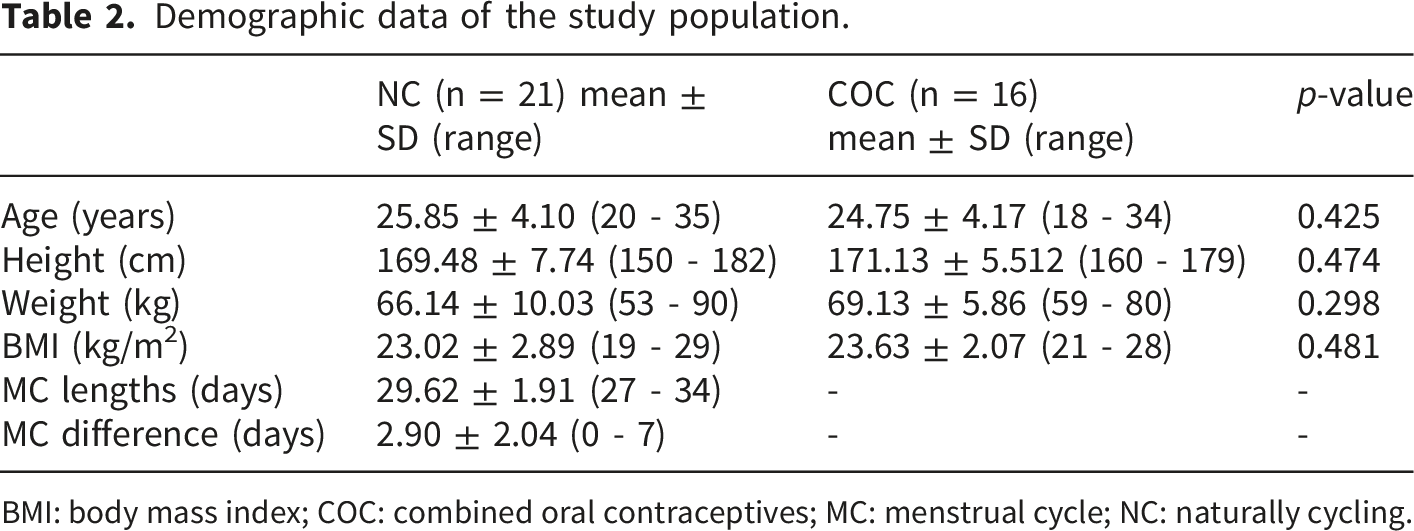
BMI: body mass index; COC: combined oral contraceptives; MC: menstrual cycle; NC: naturally cycling.
In the COC group, all participants used a COC containing ethinylestradiol as a synthetic form of oestradiol. Most participants used androgenic COCs (n = 12; 75%), while the remaining participants used anti-androgenic COCs. Most COC users took second-generation pills (n = 13; 81.3%), followed by first-generation pills (n = 2; 12.5%), and one participant used a third-generation pill, based on the classification by Pletzer et al. 68
Ten participants in the NC group had used hormonal contraceptives at least once in their lives, with most having used COCs. In contrast, only one participant in the COC group had used another type of hormonal contraceptive before their current one.
The groups showed no significant differences in age, height, weight, or BMI (Table 2).
Prevalence, location, and intensity of pain in the NC and COC groups.
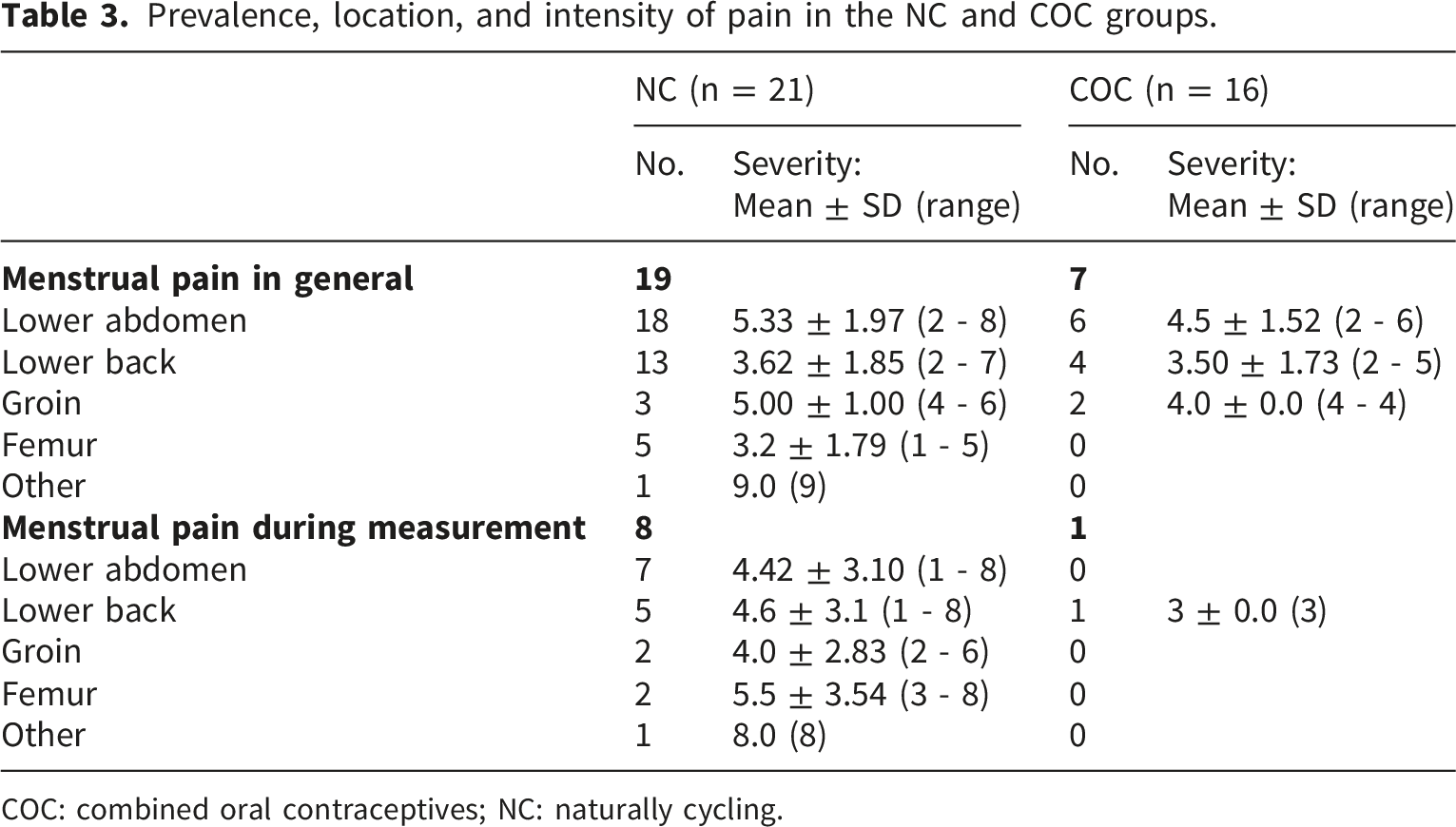
COC: combined oral contraceptives; NC: naturally cycling.
Resting-state functional connectivity analysis
Except for mCPL alpha-2, all variables met the assumptions of mixed MANOVA and MANCOVA, respectively. For mCPL alpha-2, tests for normal distribution, homogeneity of variance, and Box’s test indicated a violation of MANOVA assumptions. Therefore, all mCPL variables were log10-transformed, and the following results are reported for the log-transformed data (mCPLlog).69,70
For some variables, outliers were identified. Statistical tests showed that these outliers did not influence the results. Thus, they were included in the data analysis, as high inter-individual variability is assumed to be characteristic of the population.
Mixed MANOVA
Estimated means and standard error of means of mixed MANOVA within and between groups.
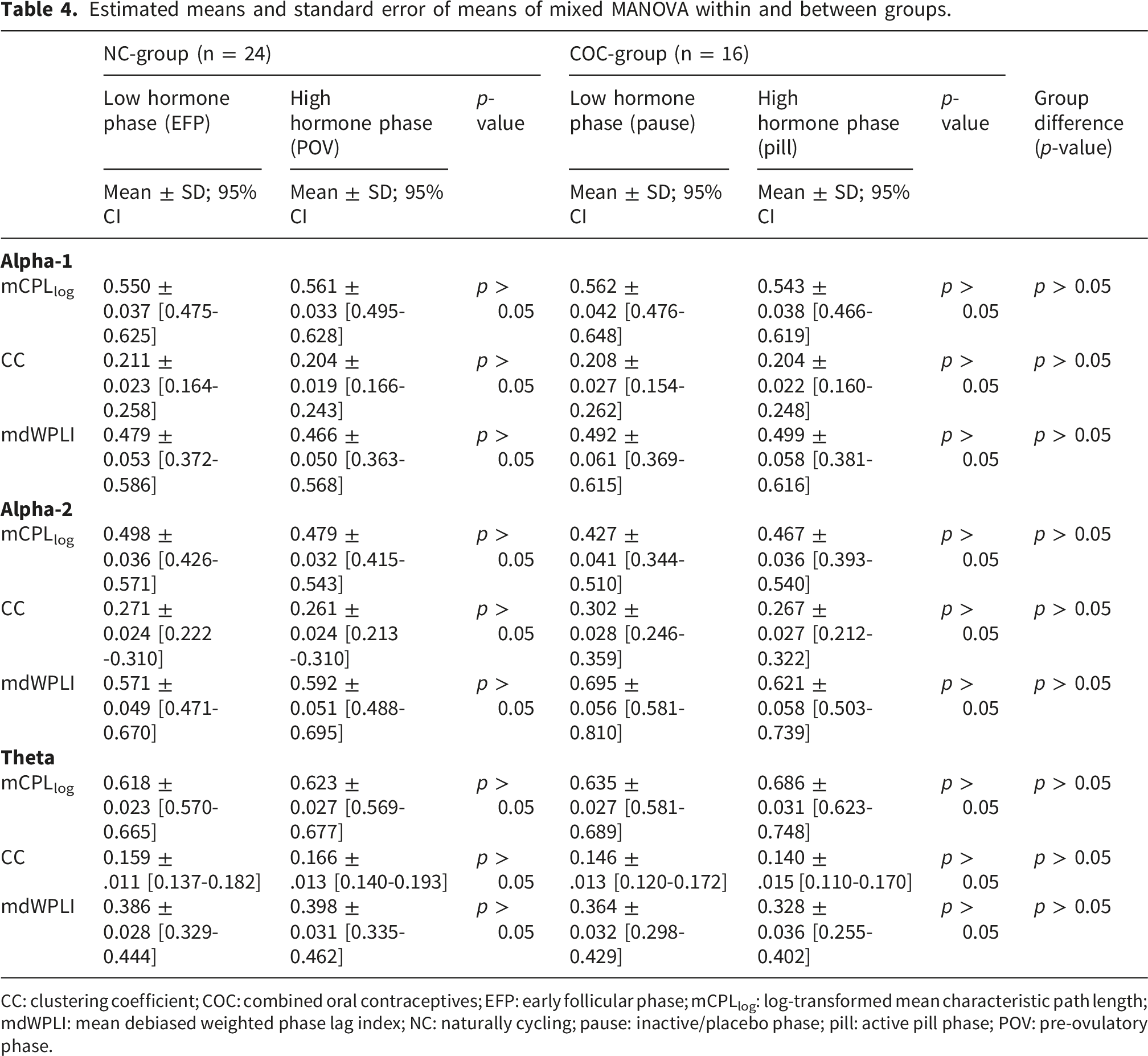
CC: clustering coefficient; COC: combined oral contraceptives; EFP: early follicular phase; mCPLlog: log-transformed mean characteristic path length; mdWPLI: mean debiased weighted phase lag index; NC: naturally cycling; pause: inactive/placebo phase; pill: active pill phase; POV: pre-ovulatory phase.
Mixed MANCOVA
After adjusting rsFC data for pain severity, a significant phase*group interaction was observed for mdWPLI (F (3,32) = 3.041, p = 0.043, η2 = 0.222). Univariate analysis revealed a trend for a phase*group interaction in alpha-1 (F (1,34) = 3.842, p = 0.058), as well as a trend for a phase*pain severity interaction in theta (F (1,34) = 3.999, p = 0.054). However, post-hoc tests did not identify significant differences between groups or phases.
For mCPLlog, univariate analysis revealed a significant phase*pain severity interaction in the theta band (F (1,34) = 4.383, p = 0.034, η2 = 0.114). As depicted in. Figure 3(A), higher scores of pain intensity in the low hormone phase (EFP, pause) co-occured with lower predicted values for mCPLlog in that phase, while they were paralleled with higher predicted values for mCPLlog in the high hormone phase (POV, pill). FDR-corrected post-hoc tests showed a significantly higher mCPLlog during the pill phase compared to the pause in the COC group (p = 0.04, M
Diff
= -0.079, 95% CI [-0.154 – -0.003]; Figure 3(B)). A) Univariate analysis revealed a significant phase*pain interaction in mCPLlog in the theta frequency B) Alterations in mCPLlog in the theta frequency between phases in the COC group A) Blue dots: Individual data points observed during EFP/pause; Grey dots: Individual data points observed during POV/pill; Blue and grey lines: Model-predicted values from the MANCOVA across levels of pain intensity for EFP/pause (blue) and POV/pill (grey) B) Blue line: Alterations in mCPLlog with standard error COC: combined oral contraceptives; mCPLlog: mean characteristic path length (log transformed); EFP: early follicular phase; pause: inactive/placebo phase; pill: active pill phase; POV: pre-ovulatory phase
Although no main effect of pain severity on CC was observed, univariate analysis revealed a significant phase*pain severity interaction for CC in the theta band (F (1,34) = 4.801, p = 0.035, η2 = 0.124). Figure 4 shows that this interaction has a contrary pattern compared to the phase*pain interaction for mCPLlog. Thus, higher pain scores during the low hormone phase co-occurred with higher predicted values for CC in that phase, whereas they were paralleled by lower predicted values in the high hormone phase (Figure 4). However, post-hoc tests did not show any significant differences. Blue dots: Individual data points observed during EFP/pause; Grey dots: Individual data points observed during POV/pill; Blue and grey lines: Model-predicted values from the MANCOVA across levels of pain intensity for EFP/pause (blue) and POV/pill (grey) CC: clustering coefficient; EFP: early follicular phase; pause: inactive/placebo phase; pill: active pill phase; POV: pre-ovulatory phase
Discussion
The present study explored whether rsFC differs between MC and COC phases, as well as between the NC and COC groups. The primary finding was that resting-state brain network characteristics did not differ significantly between groups and remained unchanged across phases. The secondary aim was to investigate menstrual pain as a potential confounding factor in the study of brain network efficiency in NC and COC samples. Here, the current study revealed significant interactions between group and pain intensity in the theta frequency for mdWPLI, as well as significant interactions between phase and pain intensity for mCPLlog and CC in the theta frequency range. In the COC group, covariate analysis revealed increased mCPLlog in theta frequency during the pill phase compared to the pause.
No influence of the menstrual cycle on resting-state functional connectivity
First, the results of this study suggest that the investigated rsFC measures do not differ between the EFP and POV. In accordance, a systematic review by Dubol et al. 5 reported no alterations in rsFC between the EFP and POV measured with fMRI, although changes between the EFP and the LP were observed. Hence, it might be suggested that the increase of oestradiol and its actions as an excitatory neurosteroid in the brain 6 alone does not influence the investigated rsFC measures.
In contrast to the present findings, fMRI studies by Hidalgo-Lopez et al. 71 and Pletzer et al. 72 reported alterations between the EFP and POV in subcortical structures (i.e., fronto-striatal, basal ganglia), as well as in cortical components (e.g. supplementary motor area) that are related to motor control. 72
While Hidalgo-Lopez et al. 71 and Pletzer et al.71,72 reported functional connectivity changes in specific regions of interest or particular networks, respectively, this study investigated whole-brain functional connectivity. Therefore, alterations confined to specific regions or networks may not be as evident when analysing whole-brain functional connectivity at the scalp level, as in the present study.
While fMRI signals record metabolic changes at low frequencies, EEG signals record electrical activity at higher frequencies. 15 Hence, another factor contributing to the discrepancies in results might be the neuroscientific method chosen for investigating rsFC.
Previous resting-state EEG studies using power analysis reported a decrease in alpha activity between the EFP and ovulatory phase only in mediotemporal and central, 23 and frontal areas 21 but not in occipital or parietal regions. However, those analyses did not consider the interconnection between brain oscillations, as was done in this study, but instead analysed power in the alpha frequency band. Hence, it might be that power in specific regions alternates between those phases, while the communication within and between neuronal populations remains unchanged. It has to be mentioned that neither Solís-Ortiz et al. 21 nor Vasil’eva 23 verified MC phases with hormone assays. Thus, changes in EEG power spectra cannot be attributed to hormone fluctuations or MC phase with certainty. 73
Studies that verified MC phases with blood samples and investigated theta power reported alterations across the MC only in comparison to the LP, and not between the EFP and POV.19,20 Thus, it might be that neither power nor the synchronized oscillatory activity in the theta frequency is affected by the transition from the EFP to the POV.
As the present exploratory study did not find alterations in rsFC between the EFP and POV, it may be suggested that rsFC analysis with EEG is not affected by MC-induced modifications in brain activity that have been observed with other neurophysiological methods (e.g., fMRI). Thus, future studies should investigate rsFC measured with EEG across MC phases, as it might be less prone to bias originating from MC fluctuations. Given the exploratory nature of this study, the interpretation of these findings should be approached with caution.
The interaction of menstrual cycle phase and pain intensity is associated with resting-state functional connectivity
The secondary aim was the examination of menstrual pain as a covariate in neurophysiological research investigating rsFC in samples consisting of NC persons. This investigation reveals significant phase*pain interactions for mCPLlog and CC after adjusting for pain intensity. The interaction effect indicates that both network integration and segregation vary between phases when pain intensity is accounted for. More precisely, with increasing pain score during the EFP, mCPLlog decreased (Figure 3(A)), while CC increased (Figure 4). The contrary pattern has been observed for the POV, where mCPLlog increased with increasing pain intensity (Figure 3(A)), while CC decreased (Figure 4). Both parameters provide information about the efficiency of information processing, with high clustering and short path length representing a highly efficient network. 62 Hence, the association between menstrual pain and network efficiency may alter depending on the MC phase.
As the interaction between pain intensity and both mCPLlog and CC was more pronounced during the EFP, it might be speculated that hormonal status is a prerequisite for the pain-sensitivity of network efficiency. Thus, menstrual pain might be an essential factor in MC research, as the number of subjects affected by menstrual pain in the sample may lead to stronger or weaker effects of the MC phase on rsFC.
Two previous resting-state fMRI studies investigated rsFC in women with dysmenorrhea using a graph theory approach.74,75 While both reported alterations in rsFC between individuals with dysmenorrhea and healthy controls, only Wu et al. 74 revealed lower CC and characteristic path length in persons with dysmenorrhea during the POV, compared to individuals without dysmenorrhea. Hence it might be that the CC decreases in the POV if pain is present during the EFP. Given that the reverse pattern emerged during the EFP in the current analysis, distinguishing between MC phases may be important in dysmenorrhea research, even when data are collected during pain-free intervals.
In the present study, the phase*pain interactions in mCPLlog and CC were only observed in the theta frequency range. In previous pain research, oscillations in the theta frequency are mainly associated with chronic or recurring pain.58,76 Furthermore, rsFC in the theta frequency is altered in patients with chronic pain. 77 Hence, the interactions between pain and phase in the theta frequency might emerge from abnormal pain modulatory processes that are associated with chronic pain.58,76
Our findings add to previous evidence showing that menstrual pain is not a minor side effect of the MC. These findings may have important implications for women’s performance and injury risk in sports. The changes in brain network integration and segregation linked to menstrual pain suggest that both MC phase and pain can influence baseline brain states. Such shifts in network efficiency, even at rest, could translate into altered readiness for motor coordination, sensorimotor integration, and cognitive control during physical activity. Given that efficient neural communication is crucial for rapid decision-making, 78 balance, 79 and movement precision, 80 menstrual pain-related changes in rsFC may contribute to variability in performance outcomes and potentially increase susceptibility to sports injuries. However, as these are exploratory first results, further research is needed to confirm and expand on these findings. This highlights the need to account for menstrual pain in both research and applied settings in female athletes, where MC-related pain may interact with neurophysiological processes underlying performance and sports injuries.
Differences in rsFC across COC phases
Next to the investigation of rsFC across the MC, this investigation aimed at examining the influence of the COC phases on network connectivity. The main analysis did not find alterations between COC phases. This is in accordance with previous EEG studies using power analyses that reported no alterations across the OC cycle in alpha and theta power.19,20 In contrast, Brötzner et al. 17 observed a higher alpha centre frequency in parieto-occipital electrodes during the active pill phase in two different samples, compared to the pause. Varying results across studies might be explained by the androgenic features of the synthetic progestins contained in the OCs used by the study samples. 68 As both the present study and the samples of Brötzner et al. 17 included participants using a variety of COCs without subgroup analysis—and some studies did not report COC features 19 —it might be that the mixture of included COCs contributes to discrepancies in the results.
Region-specific changes across COC phases have been observed in a previous fMRI study. Petersen et al. 81 reported higher connectivity in the left middle frontal gyrus—investigated as part of the executive control network (ECN)—during the pause compared to the pill phase. However, the same study reported no alterations in the default mode network (DMN). 81 Additionally, Bondt et al. 82 did not report connectivity alterations in either the ECN or the DMN in resting-state fMRI due to OC use. As mentioned before, differences in COC composition (i.e. contained progestin) and the half-life of synthetic hormones may contribute to the inconsistencies in results and limit comparisons between studies. 68 Hence, future studies should differentiate between OC types with different pharmacokinetic and pharmacodynamic characteristics and assess the level of both, progestin and synthetic oestrogen in addition to the endogenous hormone levels, for a better interpretation of the influence of COCs on rsFC.
No differences in resting-state functional connectivity between the MC and COC use
In addition to the non-significant alterations in rsFC across the MC and COC cycle, our findings indicate that there are no group differences in rsFC between MC and COC phases. Although previous resting-state EEG studies using power analysis reported group differences between NC persons and OC users,17,19 some of them were only observed in comparisons with the LP and were inconsistent across comparisons. 17
Hence, there is no consensus in the current literature on whether alterations between OC phases or differences between MC and OC groups exist in resting-state EEG. In accordance with the present findings, resting-state fMRI studies revealed no differences between groups in the DMN and ECN. 82 In contrast, Petersen et al. 81 reported differences between subjects in the follicular phase compared to COC users.
Although current resting-state EEG studies and the emerging literature on rsFC remain limited and do not reveal a clear distinction between the NC and COC groups, they offer valuable insights for guiding future research.
Differences in rsFC between the NC- and COC group after adjusting for pain intensity
In the current study, the inclusion of pain intensity as a covariate revealed a significant interaction between group and phase for mdWPLI. Hence, the communication between neuronal assemblies might alter across the phases depending on the group when mdWPLI has been adjusted for pain intensity. Thus, group differences in information processing may exist when pain intensity is included as a covariate.
Moreover, adjusting mCPLlog for pain intensity revealed a significant increase in mCPLlog from pause to pill phase in the theta band, while no significant alterations between MC phases were observed. The increase in mCPLlog could reflect a reduction in global integration and, thus, less effective communication between brain regions. 62 Hence, the pill phase may be associated with reduced efficiency of information transfer between nodes, thereby altering network function. Because these effects were observed in the theta frequency range, which has been consistently linked to attentional control and executive functions, 83 alterations in network organization within this band may indicate changes in the efficiency of cognitive processing. Given the relevance of these functions for performance-related cognitive demands in sport contexts84,85 such network changes could be functionally meaningful. However, direct cognitive or behavioural outcomes were not assessed in the present study and should be addressed in future work.
To the best of the authors’ knowledge, no published study has investigated the effect of COC phase on rsFC with EEG while including pain intensity as a covariate. Previous fMRI studies investigating the influence of dysmenorrhea on rsFC have only included persons with an MC.86,87 However, Bondt et al. 82 reported alterations in DMN connectivity in COC users with premenstrual symptoms that were not observed in the MC group. They hypothesized that symptoms between groups emerge from different origins and therefore only influence connectivity in the COC group. Thus, it might be that pain during the withdrawal bleeding emerges from different underlying mechanisms than dysmenorrhea.
Key findings and recommendations for future research
In summary, the results of this explorative study indicate that rsFC assessed with EEG is not influenced by MC phase or COC phase. Based on this finding, it might be assumed that assessing rsFC with EEG can be conducted in the EFP and POV, as well as in the pill phase and during the pause, without recording hormone-induced alterations. However, including menstrual pain as a covariate seems to be necessary—not only for the application of neurophysiological measures in the context of sports science but also due to the influence of pain on various aspects of motor behaviour, i.e., postural control,28,88 locomotion,89,90 or motor strategies for voluntary movement.91,92 Additionally, the reduction of mCPLlog in the theta band during the pill phase may indicate altered processing associated with sport-related cognitive demands, although direct effects on cognitive outcomes were not assessed. Although the effect of menstrual pain on brain functional connectivity during movement has not yet been investigated, the results of the present exploratory study—as well as findings from pain research in sports science—may support the assumption that menstrual pain can influence motor control at both a central and behavioural level. The inclusion of pain as a covariate might be of particular importance when a COC group is investigated, as this group might be more prone to alterations in rsFC when pain intensity is taken into account. Therefore, the current findings should encourage researchers to include menstrual pain as a covariate when EEG is applied in studies investigating alterations across the MC and COC cycle.
Limitations
When interpreting the results and the derived assumptions, the reader must be aware that a covariate analysis was conducted, which adjusts the group means for the effect of the covariate (i.e., pain intensity). 93 Within the scope of this exploratory analysis, menstrual pain was modelled as a continuous rather than a categorical variable to preserve variance and increase statistical sensitivity. 94 Consequently, this approach does not permit conclusions regarding the effect of clinically diagnosed dysmenorrhea on rsFC, nor can it reveal underlying mechanisms of a potential impact. Addressing these questions would require study designs that explicitly compare subgroups with and without dysmenorrhea. Such subgroup classification should follow established diagnostic guidelines (e.g., 95 ) and distinguish between primary and secondary dysmenorrhea, given their differing aetiologies and clinical implications. However, as the most common gynaecological disorder affecting approximately one third of athletes, 26 it might not always be possible to divide the sample into subgroups (e.g., if teams, elite athletes, or only specific types of sport are analysed). For those populations, the results of this study might be a first indication that menstrual pain should be assessed as a covariate in neurophysiological research, especially if alterations in the theta frequency band are of interest.
Additionally, some limitations must be considered when interpreting the results. Taking only one saliva sample during the POV cannot verify whether the measurement occurred close to the oestradiol peak, which could hinder the discovery of phase differences. 96 Thus, future studies should collect additional hormone samples on the days before and after the measurement for better interpretation of results.
As a cross-sectional study, the present investigation might be subject to sampling bias, as long-term users of COC are often those with marginal or no side effects, while previous COC users often quit usage due to adverse effects. In this study, nearly 50% of the NC group had used hormonal contraceptives at some point in their lives, while only one person in the COC group had used a different type of COC before starting with the current one. Hence, pre-existing differences or alterations in the brain that are attributed to prior COC use cannot be excluded. 68 In addition, it was not requested whether COC users had suffered from menstrual pain before the onset of COC use. As OCs are the second-line treatment for dysmenorrhea 97 requesting the history of menstrual pain is important to get the unmasked prevalence of menstrual pain in the study sample. Furthermore, it is unclear if previous recurrent menstrual pain already induces chronic or long-lasting alterations in rsFC that might not be reversible within the three months of COC use that were the minimum requirement for study enrolment. Additionally, although the number of androgenic and anti-androgenic COCs, as well as the generation is known, the specific progestins included are unknown. As some progestins have a half-life of up to 96 hours, 68 it might be that for some included subjects in the COC group the wash-out period for the progestins was too short. Given known differences in pharmacodynamics and pharmacokinetics across progestins, future studies should record the specific progestin formulation and schedule measurements during the pill-free phase after an adequate washout period. When such information is available, progestin type should be considered as an additional covariate or examined in sensitivity analyses. Consequently, future studies should assess the reason for refraining from COC use, the duration of usage, the history of dysmenorrhea as well as the synthetic progestin contained in the COC for a better interpretation of the results.
Finally, the findings cannot be generalized across all performance levels. Given reported differences in pain threshold, pain intensity, and pain tolerance between athletes and non-athlete control groups, 98 it is plausible that the magnitude of pain-related EEG alterations may vary with training and performance level. As the present sample consisted predominantly of recreationally active women, the observed effects may differ from those in higher-level or elite athletes. Future studies should therefore more precisely characterize and stratify participants according to performance level, for example by applying established athlete classification frameworks such as the tier system proposed by McKay et al. 99
Conclusion
This exploratory study is the first to investigate MC and COC phase differences in rsFC using EEG in NC women and COC users. The results indicate that global integration, local segregation, and phase synchronization do not significantly differ between MC and COC phases, nor between groups. However, the inclusion of pain intensity as a covariate revealed significant multivariate and univariate interaction effects, particularly in the theta frequency range, as well as a reduction in global integration during the pill phase compared to the pause. These findings suggest that menstrual pain may confound the relationship between hormonal phase and rsFC, potentially masking phase-dependent differences. This consideration may be particularly relevant for athletic populations, where menstrual pain has been reported to influence motor control, perceived performance, and training participation, thereby representing a possible important factor in future connectivity studies in sport contexts. As this is the first EEG study to include menstrual pain as a covariate in the context of rsFC, further research is needed to confirm these preliminary results. Nonetheless, the findings underscore the importance of considering menstrual pain as a covariate or grouping variable in future studies investigating brain functional connectivity in both NC individuals and COC users.
Supplemental material
Supplemental material - Uncovering a hidden modulator for women in sports: An exploratory study of menstrual pain and brain connectivity
Supplemental material - Uncovering a hidden modulator for women in sports: An exploratory study of menstrual pain and brain connectivity by Carina Pohle, Daniel Büchel, Silvana Bucher Sandbakk, Øyvind Sandbakk, Belinda Pletzer and Jochen Baumeister in Women's Health.
Footnotes
Acknowledgement
I acknowledge support for the publication cost by the Open Access Publication Fund of Paderborn University.
Ethical considerations
This study was approved by the Ethics Committee of Paderborn University (Ethics Code: 38/2023) on 19 June 2023. All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to participate
Participants completed written consent to participate in this study, and consent included consent for publication.
Authors contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.