
Abstract
Background
Despite approximately half of the global population experiencing this life transition, little research has considered the psychological impacts of perimenopause and menopause. Even less consideration has been given to the experiences of neurodivergent women and the complexities that may accompany hormonal transition periods for this cohort. Given the neurological and psychological complexities of perimenopause, menopause, and neurodivergence alike, research is needed to understand the perspectives and experiences of neurodivergent and neurotypical women, individually and in context to one another.
Objectives
The aim of the study was to explore how neurodivergent and neurotypical women navigate the psychological and cognitive changes associated with perimenopause and menopause, with attention to how experiences of hormonal change are constructed and understood.
Design
This research adopted a qualitative social constructionist methodology that prioritised understanding how women construct their experiences of perimenopause and menopause, alongside constructions of neurodivergence.
Methods
Individual semi-structured interviews were conducted with twelve female-identifying participants. Data was analysed using reflexive thematic analysis.
Results
Six themes were constructed including: (i) intersecting contexts and dual marginalities; (ii) evolving expressions of neurodivergence; (iii) unmasking and self-reclamation; (iv) physiological experiences of menopausal transition and positions on treatment; (v) positive experiences with healthcare professionals, and (vi) frustration over medical ambiguity.
Conclusion
Findings indicate that more education, greater emphasis on spousal support, earlier interventions, and a biopsychosocial approach to treatment and management is needed to encompass the complex needs of neurodivergent and neurotypical women alike during menopausal transitions. Further exploration is needed to understand the intersections between menopause and neurodivergence, as well as the process of identity disruption and reconstruction for women in menopausal transition.
Introduction
Different menopausal stages can encompass biological, cultural and social changes. This, linked with the combination of changes that may occur in the middle adulthood phase of a women’s life, mean that the disentanglement of psychological impacts for women during this time can be complex. 1 This is true for all women, however, neurodivergent women are particularly vulnerable to a range of disruptive hormonal symptoms as well as additional challenges and barriers in accessing appropriate support and treatment.2,3 Perimenopause refers to the transition phase during which women experience an imbalance of oestrogen and progesterone, while menopause is considered reached when a woman has not had a menstrual cycle for a 12-month period. 4 Pre-menopause refers to the period prior to when a woman enters perimenopause. 5 Many women experience their first symptoms of perimenopause in their mid-forties and can experience symptoms for up to 10 years before reaching menopause. 4
Neurodivergence refers to the natural variation in the ways in which our brains function, 2 but more specifically often refers to how people with autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD), dyslexia, dyspraxia, dyscalculia, and Tourette’s syndrome process information and interact with the world around them. 2 Obsessive-Compulsive Disorder (OCD) has been classified in different ways, but increasingly is positioned within the neurodivergence paradigm, given both how OCD can alter how a person interacts in the world and the notion that neurodivergence itself is not a static, fixed concept and new permutations of neurodivergence must therefore be recognised accordingly.6,7 Woman often find themselves navigating the challenges associated with perimenopause and menopause with little knowledge of what to expect nor ways of managing both the physiological and psychological changes that occur.1,8
Although almost all women will go through menopause, an alarming number report feeling ill equipped to manage the transition due to a lack of knowledge and understanding.9,10 Most pre-menopausal women report gaining the little knowledge they have from friends and relatives while peri and post-menopausal women were more likely to seek information through websites and their health practitioners.5,9,10 Results of previous research suggest that most women only begin to seek information at the onset of symptoms, however, due to the complex nature of perimenopausal symptoms many women live through varying levels of discomfort and even distress before seeking support. 9
A common frustration of women in all menopausal stages is lack of education and training of healthcare professionals (HCPs). 11 Past research has highlighted the negative experiences women have had when accessing medical advice and intervention to relieve their symptoms.8,12 Neurodivergent people often report poor relationships with HCPs as a result of anxiety arising from prior experiences, diagnostic overshadowing for those with diagnoses, service fatigue, and fear of repercussions, which reduce the likelihood that they will seek future medical support. 13 Neurotypical women often report seeing multiple professionals who have little knowledge or understanding of perimenopause and menopause or find that the symptoms they present with are often misdiagnosed or trivialised. 12
Further complicating the experience for neurodivergent women is diagnostic overshadowing, wherein a prior diagnosis of neurodivergence or other another diagnoses is focused on by medical professionals as an explanatory framework for any new medical symptoms, meaning new symptoms are not properly explored. 13 Both cohorts report negative experiences in the form of medical gaslighting, misdiagnosis, incorrect or unhelpful advice, difficulties obtaining prescriptions for hormone replacement therapy (HRT), and feelings of frustration and shame.9,11 There has been an ‘intergenerational silence’ with regards to the menopausal transition, creating a sense of stigma and marginalisation. 9 For neurodivergent women this results in intersecting marginalities in that both neurodivergence and menopause are underrepresented in both public and academic discourse. 2 Furthermore, the research that does exist around neurodivergence and the menopausal transition currently focuses on ASD and ADHD, excluding those on the neurodivergence spectrum who may have other diagnoses or subscribe to a particular neurotype. 2 The recent zeitgeist around the topic highlights the need for more research to determine how perimenopause and menopause are positioned in education, the media, and health care settings.
Social support has been noted as a protective factor for women experiencing severe symptoms of perimenopause, however, themes have emerged in qualitative research where women report having support from female friends or partners but a lack of support from male partners.14,15 Social support among women may be grounded in shared experience and the solidarity that comes from the knowledge that even if they are not currently experiencing perimenopause or menopause, they will be likely to at some point. 15 Conversely, when it comes to male partners women note that due to their lack of knowledge and understanding men fail to show empathy which results in women feeling isolated within heterosexual relationships.9,15 Furthermore, as menopause occurs during midlife, it often coincides with a re-evaluation of relationships, creating and exposing extant relational fragilities.9,15,16
Cognitive problems are among the symptoms commonly reported by women experiencing perimenopause, 17 although self-report and/or objective performance-based measurements are often contradictory and/or inconclusive. 17 Verbal learning and verbal memory appear the most affected cognitive functions, however processing speed, attention, and working memory problems have also been associated with perimenopause. 17 Emerging evidence suggests that perimenopause can exacerbate or mimic ADHD-related cognitive symptoms, such as attentional difficulties, disorganisation, procrastination, and memory problems. 18 The fact that these problems often peak during the menopausal transition can prompt first-time ADHD diagnosis, 19 creating complexities in distinguishing between symptoms of menopause and ADHD.
Much research has been dedicated to women’s mental health during the different menopausal stages, with concerns raised around the high numbers of women who experience emotional distress during this time.1,8,20,21 This elevated risk is referred to as a window of vulnerability22,23 and studies suggest that greater risks are present for neurodivergent women.3,19 Many women are at risk of not only first onset but recurrent episodes of depression during perimenopause, 23 while the severity of perimenopausal symptoms, both physiological and psychological, has been noted as a contributing factor.20,22,23 For neurodivergent women additional health inequities must be considered given the higher proportion of transgender and gender-diverse people in the autistic population. 24
Rationale and aim for current study
There is a paucity of research in Australia that specifically explores the perspectives of women undergoing the menopausal transition 8 and even less research that has considered neurodivergent women’s experiences. 2 This research aimed to explore neurotypical and neurodivergent women’s experiences of this life transition, and in particular, the shared and distinct psychological and mental health impacts of perimenopause and menopause.
Methods
Research design
A qualitative research approach was used to explore and understand how perimenopause and menopause is constructed and experienced by neurodivergent and neurotypical women. Social constructionism formed the epistemological foundation of the study, allowing us to explore how meaning is shared and socially constructed. 25
Method
Demographic information on participants.
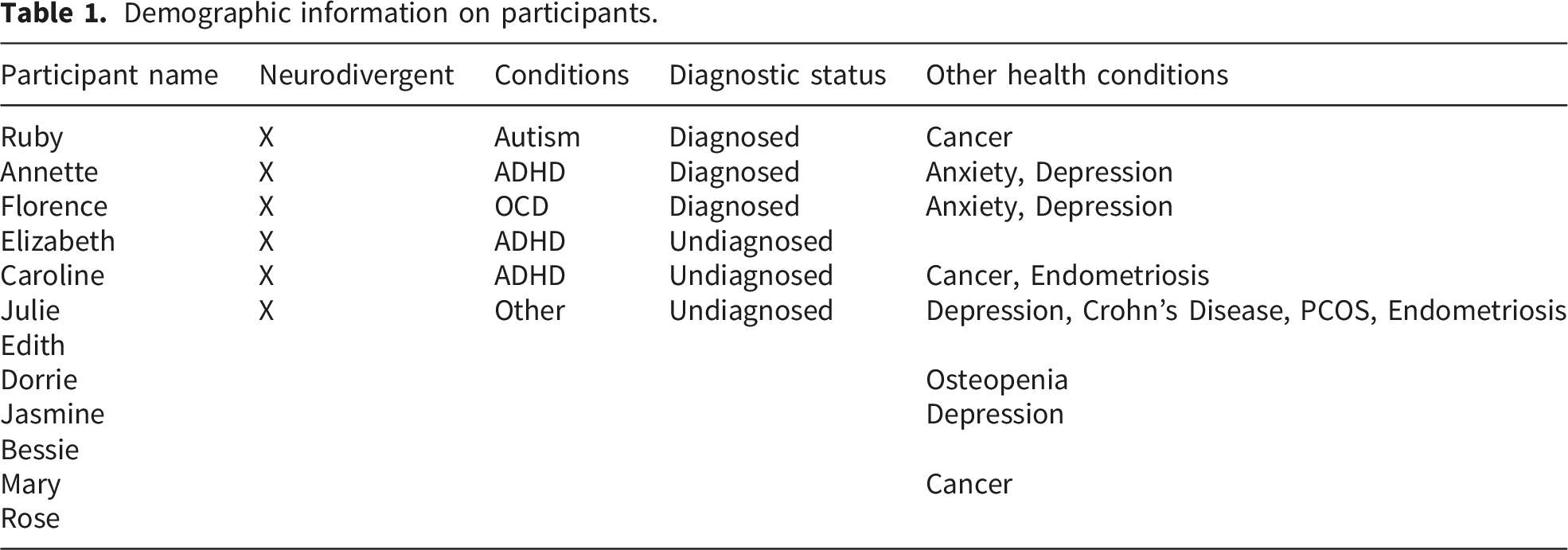
Notably, no screening tools were used to assess the neurodivergence of undiagnosed participants, nor were diagnosed participants who indicated they had a formal diagnosis required to provide evidence of the diagnoses.
Procedure for data collection
Interviews were conducted in person and online and were recorded and transcribed for analysis. Names and any other identifying information were de-identified to protect participants’ privacy and confidentiality, with each participant assigned a pseudonym.
Data analysis
Thematic Analysis (TA) was used to analyse the data. 28 This involved familiarisation with audio and written recordings of the interviews, including reading and re-reading transcripts. Semantic and latent codes were then generated via thorough examination of each individual transcript and by making comparisons across transcripts. Next, codes were mapped thematically, these themes were then examined for coherence and were reviewed in relation to the entire dataset to determine if they adequately reflected the meanings evident in the data,28,29 a process that resulted in the construction of six themes.
Results
Data analysis resulted in six themes including, (i) intersecting contexts and dual marginalities; (ii) evolving expressions of neurodivergence; (iii) unmasking and self-reclamation; (iv) physiological experiences of menopausal transition and positions on treatment; (v) positive experiences with healthcare professionals and (vi) frustration over medical ambiguity. The first, third, and fourth themes are germane to neurodivergent and neurotypical participants alike, while the second, fifth, and sixth themes address issues specific to neurodivergent participants.
Intersecting contexts and dual marginalities
Both neurodivergent and neurotypical participants described menopause as intersecting with other impacting factors in their lives. Those who did not have any known conditions reflected on the life stressors that exist for them simply due to the roles they fulfill in their lives. For example, Edith, who identifies as neurotypical, noted: Just daily life, yeah. Because you’ve got your hormones, like the fluctuation in your hormones…So I was like, the doubt and insecurity and all that kind of stuff that starts to manifest is then, compounded by just what’s going on in your life at the time, like if you’re not doing well at work or if your relationships with your partner or children or friends are, if you’re struggling there, then it just escalates,
For neurodivergent and neurotypical participants alike, conditions such as endometriosis, polycystic ovarian syndrome (PCOS), Crohn’s disease, and osteopenia were cited as some of the health-related challenges that impacted the ways in which participants understood and managed their menopausal transition. For neurodivergent participants, the menopausal transition was automatically marginalised due not only to the taboo nature of menopause but the invisibility of neurodivergence in common health narratives. 2 Ruby stated, “so you turn the estrogen off, and you have a neurodiverse brain…No one’s even studied this”, exemplifying the complexity of and intersectionality between menopause and neurodivergence.
Evolving expressions of neurodivergence
For neurodivergent participants, notable changes in their neurodivergent experiences across the menopausal transition were evident. Ruby was diagnosed with autism at a young age and her menopause was surgically induced due to endometrial cancer. She described her brain as “fast-wired”, noting: Your typical brain has dial-up, and I have DSL, so I could be talking to you, I could be writing a thesis in my brain and thinking about if… I mean, I can do all those things [at once]. That, to me, is like a yoga class for my brain.
Because of her cancer experience, Ruby knew definitively when she entered menopause, and of her neurological functioning, she noted, “[it’s like] someone’s just turned the faucet off [in my brain] overnight”, further noting, “[my brain] is not the same as it was before I had surgery”. Here she describes the change in her functionality: I was very high functioning, right? It's not like I had ADHD, where I couldn't focus and get something done, but generally… if it was something that I was interested in, you know, I'd be an expert on it, and the things that didn't interest me, I could get those tasks done… Now [in perimenopause], if it's something that doesn't interest me, and I really don't want to do it. But I have to do it. Um, I will put it off like someone that has ADHD…until it's the 11th hour, I won't do it. Whereas before, I was like, okay, these are things I have no patience to do, I don't like to do them, but I'd get them done first, so it's out of the way, so it's not going to annoy me. Now, I cannot do that. Now I'll put it off, and I will put it off, and I will put it off. And I don't have ADHD. But my brain has changed now that I can’t knock those things out of the park the way I used to. I'll only seek out things that bring me joy, and things that I want to do.
Despite the commonality Ruby highlights here between perimenopause and ADHD, not all participants considered the symptomatology of both conditions so synonymous. Annette was diagnosed with ADHD in later life and was careful to contrast the difference between her experiences of ADHD such as disorganisation and forgetfulness with menopausal brain fog. Whilst Annette had become accustomed to her neurodivergence, the experience of brain fog left her feeling disoriented: Just being in that space where you just can't get your shit together because you don't know. And being ADHD as well. [Partner’s name] like that’s just you anyway, but just absolutely forgetting. And not being able to navigate my day-to-day. That was… that was… that's horrible. I hate that.
Annette described this as a new experience as opposed to an amplification of her ADHD, in contrast to extant research which has drawn a connection between ADHD and the cognitive symptoms often experienced throughout perimenopause.
18
In contrast to Annette and in line with extant literature, Florence had diagnoses of OCD, depression, and anxiety, and framed the intersectionality of those conditions and menopause as “constant” and “bloody exhausting”. For Florence, menopause exacerbated her extant mental health and neurodivergence-related challenges, while for Annette a clear distinction existed between the two. For Florence, this symptom exacerbation was intense and debilitating: Brain fog, oh my god…I sit there and I’m like what the fuck was I doing. Like I’ll sit at my computer screen, how do I even go into that to look that up, “oh my god Florence” and then it comes to you, but it is, it’s intense.
Neurodivergent participants understood themselves deeply in relation to their various diagnosis, but for some, menopause amplified their existing neurodivergence and mental health symptoms, while for others, menopause was a distinct experience, even accounting for a degree of interaction and amplification between symptoms. This meant that menopause disrupted self-understanding and was consequently constructed as a confusing and at times distressing period, capable of shifting how participants functioned and behaved, and fundamentally, how they saw and understood themselves.
Unmasking and self-reclamation
This theme explores the ways in which the menopausal transition prompted a re-evaluation of the self for both neurodivergent and neurotypical participants. Neurodivergent participants framed this in terms of unmasking and accepting their authentic selves, while neurotypical participants tended to focus more on relational and role-based adjustments. For example, Annette spoke about her ADHD and how she experienced rejection sensitivity dysphoria (RSD). She positioned this in relation to her perceived need to mask her symptoms not only of her ADHD but also perimenopause: I went through a stage of like wanting to… try and kind of hide that, and… you know, dress in a particular way, and act in a particular way, so that, you know, because, you know, you're getting more mature.
Florence, who was also neurodivergent, echoed this struggle when discussing her management of both her mental health and her perimenopausal symptoms: Because we’re strong independent women and we don’t like to let anybody know that we're failing, or feeling down, I don’t anyway. Um and when you go through something like this, you do, you put that façade up. And it’s like “nah I’m fine”. And then that creeps in the panic attacks, that creeps in, you go home and you’re an arsehole because out in the world you’ve been this great amazing person all day.
For Annette, the perception of women in menopause was, “just crazy bitches” but when she became fatigued from masking her symptoms she was able to accept that, while that may be the perception, “that’s not my reality” and she became empowered to embrace who she was becoming: I think that's where I am at this point …I'll just put on more black eyeliner and dress even more like a witch, and get out there and just, you know, hobble around. So, yeah, it's kind of…I'm in my crone stage. You know, the maiden, mother, crone, I'm now transitioning into crone, and I have wisdom to share.
Similarly, Julie constructed herself as transitioning from insecurity to empowerment through menopause, noting, “I’ve been a wife, I’ve been a mother…the whole menopause thing, that’s given me…the reason to say, you know what? This is my time, and it’s my turn”. It was common among both neurodivergent and neurotypical participants to experience a disruption of identity, resulting in a reassessment of self. Neurodivergent participants experienced this more at an individual level whilst neurotypical participants positioned the disruption as a relational entity. Edith, who did not identify as neurodivergent, highlighted the relationality of her experience, noting, “The pressure of…you’re supposed to be this everything to everyone, but to yourself you’re nothing”. There was a spoken and at times unspoken sense of negotiation between the self and others, which for Rose, a neurotypical participant, manifested in context to her roles as mother, stepmother, and wife.
Neurodivergent participants often positioned themselves in opposition to prescriptive gender norms and generational silence around menopause. Their narratives emphasised resistance, rebellion, and self-definition in contrast to neurotypical participants who viewed cultural change as a gradual social evolution. For many, menopause symbolised an act of resistance against expectations of emotional regulation, productivity, and femininity. Annette highlighted the generational shift from tolerance of suffering, or as she describes it, “just going through it”, to revolt: ….if we… if we can get this stuff [understandings of menopause] right, and if we can start to talk about it, like, that's why I say, you know, Gen X, we're not taking this shit lying down anymore. My sisters are boomers, so it's like… in that generation, where I think there was a lot more… [we] would we just go through this? Um, whereas I think, yeah, seeing women in podcasts that on, you know, in different videos talking about this stuff, I was like, yeah, you… you're stomping your feet and lighting a match, because we're not being told anymore. The way we should be behaving, and the way that we should be reacting and acting with what we're going through in our bodies, particularly now.
Physiological experiences of the menopausal transition and positions on treatment
Physiological symptoms.
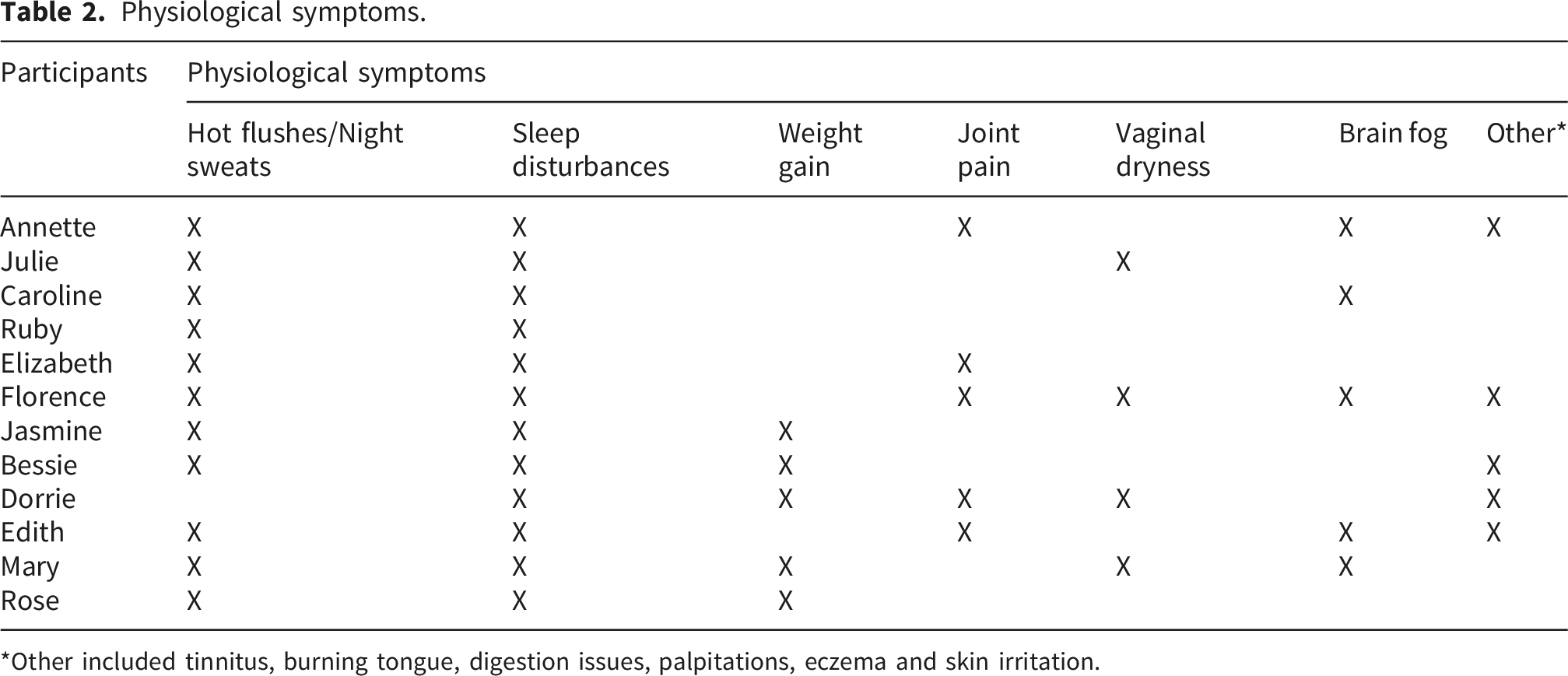
*Other included tinnitus, burning tongue, digestion issues, palpitations, eczema and skin irritation.
The only symptom notably absent for neurodivergent participants, in contrast to neurotypical women, was weight gain. Previous research suggests that neurodivergent women may have more problematic menopausal transitions with regards to physiological symptoms, however, the findings of the current study suggest no notable differences in number or severity of symptoms, in contrast to extant literature.2,3
The most notable treatment for perimenopausal and menopausal symptoms is HRT.
9
Dorrie was a huge advocate of HRT and called it “a little miracle”, while many of the other participants were ineligible for HRT. Gaps in medical knowledge created a double jeopardy problem for neurodivergent participants. As one example of this, Ruby was apprehensive to use treatments like HRT that are under researched with regards to neurodivergence: …even with, say, supplements, or even medical interventions, that's not studied on people who are neurodivergent. And so, like, for me, a cup of coffee makes me sleepy, right? It's the opposite. So, it's the same when I had surgery. They didn't even consider some of the drugs they wanted to give me, what it would do to my brain. And so, it's another reason why I don't like to take pills, because, I don't know, they don't test them on neurodiverse people before…so…no!
Both neurodivergent and neurotypical participants used a mixture of herbal and natural remedies, exercise, diet and lifestyle changes to manage menopausal symptoms. These management strategies suggest that both neurodivergent and neurotypical women alike are positioning themselves in a more active role when navigating the treatment and management of perimenopause and menopause.
Positive experiences with HCPs
Interestingly, many of the neurodivergent women in this study had positive relationships with their HCPs, perhaps reflecting continuity of care that may in some respects be more commonly experienced in regional and rural areas. For example, Annette noted a long-standing positive relationship with her doctor, and despite his lack of knowledge around the menopausal transition, she deeply valued his honesty and resourcefulness: And I like my doctor as well, because he's not one of these…he's been my doctor for over 10 years now, and he… if he doesn't know. He will say, “I don't know”. And then he'll go and find out about it.
Similarly, Ruby discussed positive relationships with multiple HCPs, both when she was living overseas and since being home in Australia, reporting feeling “understood” by the GP who first identified her perimenopausal symptoms. Here she highlights how a lack of knowledge can be offset by a constructive patient-doctor relationship: It's my GP who's been more helpful, but still, she says, “Ruby, we have nothing on neurodiversity and menopause”. She was honest.
Honesty and candour conveyed respect and so too did listening attentively, with Julie stating that her “great female doctor” was “wonderful…she actually believes me”. Caroline, a neurodivergent participant with a terminal cancer diagnosis, commented that her medical team were “fantastic”. This theme sits in contrast with extant research that suggests that neurodivergent people tend to have negative experiences with HCPs, and to a greater degree than their neurotypical counterparts due to negative prior experiences and diagnostic overshadowing.13,30 Possible explanations for these findings could be the rural context noted above and the continuity of care, as well as the care and management of already recognised diagnoses. 31 In small regional Australian towns, single GP medical practices are not uncommon, and while resources may be fewer in regional areas, greater continuity and relationality of care may also exist compared to metropolitan contexts. These findings suggest strong doctor-patient relationships and continuity of support may be fundamental to providing menopausal support, especially for patients with extant medical, mental health, and neurodivergence diagnoses.
Frustration over medical ambiguity
Counter to the previous theme, for neurodivergent participants, frustration over medical ambiguity and lack of clarity in the menopausal diagnostic processes existed. This frustration stemmed from a need for logic, clarity, and empirical grounding. These needs currently conflict with the medical system’s lack of definitive diagnostic tools, as Julie articulated: I think my biggest issue. And I brought it up early, and it's the one that, you know? Gets to me the most is the fact that there is no test. You know, if I have the flu, I can go to the doctor, get a test done…and having knowledge is power, and I can say, you know what, I'm feeling bad because I have the flu.
Julie further reflected that a lack of certainty breeds self-doubt to the point where she would tell herself, “You’re being lazy, you’re being silly!”, because she could not attribute her symptoms to a concrete diagnosis. Ruby’s frustration was due to the lack of education women are given in detecting signs of the transition themselves, alongside a lack of preparation from HCPs. Ruby likened this type of conversation and preparation to the kinds of care and preventative measures taken for women’s cancers, noting that just like with mammograms, “maybe these are yearly conversations that we should be having with the GP, but they don’t really exist”.
Discussion
This study explored the psychological impacts of perimenopause and menopause for both neurodivergent and neurotypical women, using thematic analysis framed within a social constructionist epistemology. Six core themes were constructed, and together highlight how the menopausal transition is navigated by women, with the themes intersecting contexts and dual marginalities, unmasking and self-reclamation, and physiological experiences relevant to the experiences of neurodivergent and neurotypical women. The themes, evolving expressions of neurodivergence, positive experiences with HCPs, and frustration over medical ambiguity, explored the specific experiences of neurodivergent women. Findings illuminated how both cohorts experienced the menopausal transition as not only a physiological event but a socially, psychologically, and culturally mediated transition with behavioural and identity-based implications. Our findings align with extant research that indicates that women find it difficult to disentangle the biological, psychological, and social factors relating to their menopausal transition.1,11
For neurodivergent participants, different subject positions were articulated in context to the relationship between symptoms of neurodivergence and perimenopause and menopause. For some, symptoms were positioned as overlapping and interconnected and this made it harder to understand how best to interpret physical, psychological, emotional, and medical experiences of perimenopause and menopause. For others, and in contrast to extant research, a distinction existed between menopausal symptoms and symptoms of neurodivergence, notable in the line Annette drew between menopausal brain fog and ADHD forgetfulness.18,19 These symptoms and how they were interpreted and attributed could result in a rupture to one’s sense of self for neurodivergent women and this required identity work to process, especially given fluctuations in menopausal symptom intensity. These findings highlight the implications of menopausal symptoms and experiences for female identity and demonstrate the complexity of navigating identity during this life transition. The complexity of this process may be heightened for neurodivergent women, however, given neurodivergence can lead to self-exploration aimed at making sense of one’s identity, 32 it may also be that neurodivergent women are better equipped to navigate identity renegotiation a second time.
Both neurodivergent and neurotypical women highlighted the impact of intersecting contexts and how their menopausal transition co-occurred with other health conditions or life circumstances evolving at the same time. For neurodivergent participants this intersection was amplified by the overlapping invisibility of menopause and neurodivergence, while some participants experienced neurodivergence, menopause, and a life-threatening diagnosis simultaneously. This invisibility likely stems from the male and neurotypical orientation of health settings.19,24 Furthermore, both neurodivergent and neurotypical participants highlighted their lack of knowledge because of the taboo nature of menopause. Many participants credited the little knowledge they had pre-menopause to other women in their lives. For many of the participants a lack of knowledge led to negative attitudes around the transition which in turn could increase the severity of symptoms. 5 Whilst lack of knowledge was a concern, participants also noted a cultural shift in the availability of information, with greater media coverage and peer-to-peer conversations increasingly taking place, normalising the transition.
The current study broadly aligns with emerging evidence that perimenopause can exacerbate or mimic ADHD-related cognitive symptoms, such as attentional difficulties, disorganisation, procrastination, and memory problems. 18 Some participants experienced newly emerging or intensified difficulties with task initiation, cognitive load, and executive functioning that paralleled ADHD symptomology despite there being no history of these challenges prior to perimenopause. In contrast to this, one participant clearly differentiated perimenopause brain fog from ADHD inattention, complicating assumptions of symptom continuity and raising questions about the extent to which cognitive changes throughout the menopausal transition should be conceptualised as extensions of neurodivergent profiles versus distinct phenomena in their own right. 33
These constructions of neurodivergence and menopausal symptoms highlight the need for further research to explore the neurodivergence-menopause nexus, particularly in relation to ADHD. The temporality with which an ADHD, ASD, OCD, or other related diagnosis is received relative to the beginning of perimenopause warrants attention, given our findings on identity navigation in this study and considering the different forms of identity navigation that may take place when a neurodivergence and perimenopause diagnosis co-occur, compared to when one diagnosis precedes the other. As Chapman et al. 19 highlight, the cognitive symptoms of perimenopause can prompt a first-time ADHD diagnosis, however, as diagnoses of ADHD become more normative for women, more women are likely to be diagnosed with ADHD prior to the beginning of perimenopause.
The theme of unmasking and self-reclamation illustrates the disruption and reconstruction of identity that was evident across the dataset, and not just for neurodivergent women, despite the term “unmasking” carrying neurodivergence connotations. For neurodivergent participants this involved an unmasking of their neurodivergence and a rejection of neurotypical expectations. Participants’ experiences presented like a journey that began with negotiating one’s identity through the lens of societal expectations, followed by the disruption to identity associated with perimenopause and/or other major life events. The final step of the journey was the reconstruction of identity from a perspective of freedom and empowerment. For neurodivergent participants this was constructed as a singular experience, an internally navigated conflict between societal expectations and one’s emotional reality. For neurotypical participants self-reclamation was framed more relationally, often tied to renegotiation of social roles such as daughter, mother, wife, and friend.
For neurodivergent participants, the menopausal transition acted as a site of resistance against the societal expectations imposed upon women. Annette’s declaration about generation X “not taking this shit lying down anymore” situates the menopausal transition within the broader generational rebellion against silence and compliance. This is notable given the high proportion of neurodivergent people who identify as a gender different from that assigned at birth and therefore the multiple diversity dimensions at play for those individuals. 24 Encouraging women to see the menopausal transition as a time of identity growth may promote resilience, self-acceptance, and collective empowerment, and in turn, this may promote more positive attitudes toward the transition. 5 It may be that neurodivergent women are better prepared for the identity challenges that emerge as a result of the menopausal transition, having already (re)constructed their identities through the framework of neurodivergence 24 as well as potentially navigating gender and sexual diversity. Conversely, neurodivergent women may experience identity formation fatigue as they re-negotiate their identities for a second time during the menopausal transition, and this warrants further research and consideration.
Both neurodivergent and neurotypical participants reported a range of physiological symptoms, with little variation across groups. Neurotypical women were concerned about the impact of HRT on their health; however, in addition to this concern neurodivergent women also experienced the added challenge of not knowing if the medication might have particular impacts on them, highlighting the neglect of neurodivergent women in the menopause literature and the ways in which a lack of knowledge may lead to apprehension and mistrust. 30 For neurodivergent participants, the frustration over diagnostic ambiguity was profound, with more clarity and validation regarding the menopausal transition clearly needed. This thread of dissatisfaction followed through to critiques of male-centred medical systems and reflected the inequities in research and medical treatment that women experience. Participants voiced concerns about the trivialisation of women’s health issues and how this impacts how women perceive and value their own physical and psychological suffering. For neurodivergent participants, the dual marginalities of being both a woman and neurodivergent resulted in compounded exclusion from medical discourses. Despite these issues, however, neurodivergent participants framed their experiences of HCPs as positive; relationships characterised by trust and transparency, even where knowledge was lacking. Both Ruby and Julie noted specifically that they appreciated HCPs who “believed” them. These narratives suggest that neurodivergent people often feel dismissed in medical contexts 30 but this is not always the case, and the relationality of care in regional contexts may provide a valuable model in understanding how health systems can better support neurodivergent women, and indeed, women in general.
Implications, limitations and future directions
The data from this study has implications for both neurotypical and neurodivergent women. The lack of education around both the menopausal transition and neurodivergence highlights the need for more accessible education for HCPs, particularly those working as GPs who are often tasked with providing frontline support prior to a patient seeking out specialist psychiatric or other medical support. More education would allow both menopause and neurodivergence to be normalised in public discussion, reducing the perpetuation of negative stereotypes related to the perimenopausal and menopausal experience, particularly for neurodivergent women. The medical ambiguity of perimenopause and menopause appears to undermine women’s ability to effectively identify and address both their physiological and psychological symptoms. Whilst education can increase knowledge and understanding, proactive methods such as earlier conversations with GPs and routine hormone testing could better prepare women for the transition and reduce the occurrence of confusion and frustration around the diagnostic process.
Once detected perimenopause should be treated by way of the biopsychosocial (BPS) model. 34 This model is concerned with not only the biological but the psychological and social aspects of health 34 and emphasizes the need for integration of biological, psychological, and social factors when providing support. Using this lens HCPs in all fields may better address the complex nature of perimenopause and the intersecting factors that shape individual experience. Given the intersectionality of issues that may impact upon the menopausal transition, such as pre-existing or emerging mental or physical health issues, relational issues, financial stress, parenting/caring responsibilities, and neurodivergence, the biopsychosocial model may provide a valuable contextual lens to healthcare for women and their HCPs. Use of this model may reduce the financial and time burden faced by HCPs and their patients in determining the most effective interventions for women. 12
In contextualising the findings of this study, it is important to note that one limitation was the predominance of ADHD in the sample of neurodivergent participants, compared to other forms of neurodivergence. Given the particular relationship that may exist between ADHD and menopausal symptoms, study findings must be interpreted cautiously, and research is warranted to further explore the relationship between menopause and other forms of neurodivergence. Participants were also drawn from regional and rural communities in Australia, and the regional healthcare context of these participants may not be reflective of rural and regional healthcare practices in other countries. Furthermore, it must be noted that participants were predominantly white, middle-class women who experienced potential disadvantage in their geographic location and for some in their neurodivergence, but also experienced economic and cultural privilege. The findings of this study do not necessarily apply to the experiences of culturally diverse and/or economically disadvantaged women, as medical marginalisation likely uniquely affects women of colour during menopause and this warrants further exploration, alongside issues of racial bias.
Finally, participants in this study were not required to have a formal diagnosis which allowed us to include important perspectives from a range of participants who might otherwise have been excluded from research, however, this did limit our ability to explore the impact of a formal diagnosis of ADHD, ASD, OCD, or other related condition, in context to menopause. Future research might distinguish between the menopausal experiences of formally diagnosed and self-diagnosed neurodivergent women, especially when exploring the influence of medication and identity navigation. Much of the previous research around neurodivergence and the menopausal transition has focused on autism. 2 Studies that focus on ADHD note the increase in late diagnosis of ADHD and raise questions around whether this is due to the similarities in cognitive symptoms between ADHD and menopause. 19 Future research should consider individual forms of neurodivergence separate to one another in order to develop a full, nuanced understanding of the connection between neurodivergence and menopause. Previous research suggests that neurodivergent women will experience more severe symptoms and potentially earlier onset and longer menopausal transitions than neurotypical women. 35 Given we did not find such a pattern in our study, further research is warranted to explore this.
Finally, future research would benefit from moving beyond cross-sectional designs to longitudinal studies that capture the menopausal transition for neurodivergent women over time, including exploration of the identity arc of disruption to empowerment described earlier. This would allow for more in-depth knowledge and understanding of the psychological and cognitive experiences of neurodivergent women. Collaborative research designs in which neurodivergent women are directly involved in shaping the research would also provide richer and more authentic insights that challenge the dominance of male-centred, neurotypical medical frameworks.
Conclusion
This study provides new insights into the psychological and identity-related impacts of perimenopause and menopause for both neurotypical and neurodivergent women. Across the dataset, participants described the menopausal transition as a multifaceted experience shaped by the interaction between biological changes, social expectations, and existing mental health or neurodivergent profiles. For neurodivergent women in particular, menopause often disrupted familiar cognitive and emotional patterns, leading to uncertainty about how to interpret changes in memory, attention, and mood. While some participants experienced an overlap between menopausal symptoms and neurodivergent traits, others drew clear distinctions, highlighting the need for more nuanced clinical frameworks that do not assume symptom continuity. 33 Identity disruption and reconstruction emerged as central processes, with many participants describing menopause as destabilising but ultimately transformative. Crucially, these findings point to gaps in education, support, and clarity that leave all women, but especially neurodivergent women, navigating the transition with insufficient guidance. Improved healthcare communication, earlier anticipatory conversations, and a biopsychosocial approach to care may help to reduce confusion and foster more responsive support. Future research should prioritise longitudinal and participatory approaches to deepen understanding of the intersections between menopause and neurodivergence and ensure that the voices of women shape emerging knowledge and policy.
Footnotes
Acknowledgements
We would like to say a big thank you to our wonderful participants. Thank you for graciously taking the time to chat with us about your experiences and share the journey you took through the different stages of menopause.
Ethical considerations
The Charles Sturt University Human Research Ethics Committee approved the research reported herein (approval/protocol number: H25165) on 19/06/2025. Respondents gave written consent before starting interviews.
Consent for publication
Participants gave their written informed consent for their data/data extracts to be published.
Author contributions
All authors contributed to the study conception and design. All authors read and approved the final manuscript. Conceptualization: [Emily Johansson] [Dr Rachel Hogg]; Methodology: [Emily Johansson] [Dr Rachel Hogg]; Formal analysis and investigation: [Emily Johansson]; Writing - original draft preparation: [Emily Johansson]; Writing - review and editing: [Emily Johansson] [Dr Rachel Hogg]; Supervision: [Dr. Rachel Hogg].
Funding
Charles Sturt University provided article processing fee support for the publication of this article via their Tri-Faculty Open Access Publishing Fund.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
As interview data contains potentially identifying information, data is not available for sharing.
Artificial intelligence policy
Generative AI was not used in the development or writing of this manuscript.