
Abstract
Background
Couples experiencing infertility often seek medical help to achieve a pregnancy using assisted reproductive technology, which might cause stress and affect their quality of life.
Objectives
The purpose of the current study was to investigate the mutual effects of optimism and stress on fertility-related quality of life among women and their husbands during the process of in vitro fertilization (IVF), as well as the success of the treatment.
Design
A cross-sectional study with a prospective outcome assessment design aimed at assessing psychological variables, with a short-term prospective follow-up, among 51 couples undergoing IVF treatment.
Methods
Participants completed questionnaires on fertility-related stress, optimism, and fertility-related quality of life. Two weeks after embryo transfer they were contacted by a researcher to check for pregnancy. The dyadic associations were analyzed using the Actor–Partner Interdependence Mediation Model (APIM).
Results
Women’s fertility-related quality of life correlated negatively with their stress (r=-.67; p<.01) and positively with their husbands’ fertility-related quality of life (r=.31; p<.05). Husbands’ fertility-related quality of life correlated positively with their optimism (r=.35; p<.05) and negatively with their stress (r=-.56; p<.01) and their wife’s stress (r=-.33; p<.01). A positive correlation was found between women’s optimism and their husbands’ optimism. Women’s stress was higher and their fertility-related quality of life lower than those of their husbands. The APIM analysis revealed actor (B=.22, p<.001) and partner (B=.12, p=.02) effects of optimism on fertility-related quality of life. The only predictor of pregnancy was younger age.
Conclusions
Both spouses experience stress during IVF treatments, therefore psychological support should be offered to both during this time, including stress management interventions and couple-based support aimed at strengthening dyadic coping. The positive correlations between women’s fertility-related quality of life and that of their husbands, and between women’s fertility-related quality of life and their husbands’ optimism, highlight the importance of spouses’ support for each other.
Background
Fertility treatments are widely acknowledged as a complex and demanding process for couples. Previous studies consistently underscore a decline in the fertility-related quality of life (FertiRQoL) experienced by most couples undergoing fertility treatments. The decrease in FertiRQoL is often attributed to heightened levels of stress induced by the treatment itself.1,2
Psychosocial and cultural context of infertility and of fertility treatments
Infertility is the inability to conceive after one year of unprotected intercourse. 3 It has been recognized by the World Health Organization as a global health problem. 4 In recent years there has been an increase in the number of couples experiencing infertility. It is estimated that the prevalence of infertility in high-income countries ranges between 9.3 and 11.6 percent. 5 Moreover, 35–50% of infertility cases are caused by male fertility problems.,3,6
Couples experiencing fertility problems often seek medical help and may achieve a pregnancy using assisted reproductive technologies.
7
The many fertility treatments include hormonal treatments, insemination treatments, surgery, procedures to produce sperm, and in vitro fertilization (IVF). Such fertility treatments may cause stress among couples diagnosed with infertility.
8
In Israel, IVF treatments for delivering up to two children are covered as part of the national health basket provided by the Ministry of Health through the health maintenance organizations (HMOs). This includes diagnostic tests, hormonal treatments, egg retrieval, fertilization, and embryo transfer, with no limit on the number of attempts until achieving this goal. Supplemental insurance may provide coverage for IVF-related services beyond the basic HMO basket
Beyond the medical aspects, infertility and its treatment take place within broader psychosocial and cultural contexts that may intensify the distress of those involved. Studies show that infertility involves interrelated mental, 10 social, 11 cultural, 12 and interpersonal factors.13,14 The Israeli culture is pronatalist; women are expected to become mothers and childbirth is considered part of the “national mission”, aimed at increasing the Jewish population that was significantly reduced in World War II. 15 Having children is an important goal for most Israelis. 16 For example, the average birth rate among Jewish women in Israel is 2.89 children per woman, 17 versus 1.7 children per woman in the United States and 1.5 children per woman in European countries. 18 Hence, it can be assumed that Israeli couples experiencing infertility feel increased stress to become parents. 19
Fertility–related quality of life
Quality of Life is defined as one’s personal perception related to the cultural context and value system in which one lives, with reference to their goals, expectations, and standards. 4 While QoL often refers to subjective well-being and life satisfaction, in the present study we relate to fertility-related QoL as defined by Boivin et al. (2011). Specifically, fertility quality of life consists of four personal domains: emotional, social, body-mind, and relational. 20
Infertility and fertility treatment can substantially affect individuals’ psychological well-being and quality of life. 20 Previous research has demonstrated gender differences, with women often reporting a greater emotional and physical burden than men. 21 These differences may partly reflect the unequal experiences associated with fertility treatments, as women typically undergo more intensive medical procedures, including hormonal stimulation, frequent monitoring, and invasive interventions. 22 In contrast, men’s experiences of infertility are often less medically invasive but may involve psychological distress related to stigma, identity concerns, and relationship dynamics.
Many women experiencing infertility do not share the diagnosis with their friends or family, thus intensifying their psychological vulnerability, which can impede their QoL. 23 From a gender perspective, a systematic review related to the QoL of people experiencing infertility found that women reported lower QoL than men. 24 This was supported by later studies such as one that included 750 couples from fertility clinics in Germany, Hungary, and Jordan, which found that men received higher scores than women on social, emotional, and mental FertiRQoL. 12 Another study examining infertile couples took a dyadic approach and found that women reported significantly lower QoL than their partners. 2
While previous research has primarily focused on women’s stress and its association with their quality of life,25,26 and a meta-analysis compared psychological distress and quality of life between men and women in infertile couples, 27 limited attention has been given to examining positive psychological resources such as optimism within a dyadic framework during IVF treatment.
Stress during fertility treatments
Stress is an emotional experience that is based on the individual’s continuous cognitive assessment of their situational demands and of their available resources for coping. 28 According to Lazarus and Folkman, stress occurs when these demands are incompatible with the individual and with the resources available to deal with them. 29 Fertility treatments are also emotionally demanding for couples. 30 Moreover, couples undergoing fertility treatments may experience loss of control, 23 resulting in stress. For example, one study found a high level of stress among couples undergoing fertility treatments, with women reporting more stress. 31 In addition, women undergoing IVF treatments face negative emotions, 2 which may have a negative effect on fertility, 32 on the success of fertility treatments, and on the success of IVF in particular. 33 Moreover, high stress levels were found related to lower FertiRQoL.1,34
Can optimism serve as a psychological resource for individuals experiencing infertility and undergoing fertility treatments?
Optimism has been found related to more positive health outcomes. Indeed, studies have found that optimistic people demonstrate improved health outcomes and better obstetric outcomes.35,36 A study that evaluated the relationship between optimism and the success of fertility treatments found a positive relationship between optimism and the ovarian response to treatment in women undergoing fertility treatments. 37
Some studies have reported that optimism can help alleviate the stress associated with fertility treatments.11,38 For instance, a study surveying Arab Israeli mothers after fertility treatments reported a negative association between their feelings of optimism and of stress. 38 Moreover, it has been reported that resilient women undergoing fertility treatments are characterized by higher levels of self-esteem, self-efficacy, and optimism, and that possessing high levels of resilience helps them cope with stress and is associated with higher FertiRQoL. 11
Can optimism, stress, and quality of life predict the success of fertility treatments?
A meta-analysis that examined the relationship between stress and the outcomes of fertility treatments found that successful achievement of pregnancy rose as stress levels decreased. 39 However, a more recent meta-analysis did not indicate a connection between such distress during fertility treatments and successful achievement of pregnancy. 40
Most of the studies on infertility have addressed mainly women. 41 Aslzaker et al. (2016) examined the relationship between fertility treatment-related stress, psychological symptoms, women’s QoL during fertility treatments, and treatment success. The study concluded that women experience negative feelings while waiting for treatment results, and this in turn affects the success of the treatment. 42 A longitudinal cohort study among 686 women living in Taiwan who underwent IVF treatments between 2012–2017 found that emotional QoL measured before embryo transfer significantly predicted pregnancy outcomes. 43
The current study aimed to 1). investigate the mutual effects of optimism and stress on FertiRQoL among women and their husbands within a dyadic framework and, 2) examine whether the optimism, stress, and FertiRQoL of women and their husbands predict the success of their fertility treatments.
Research hypotheses
H1: Significant differences will be found in the stress and FertiRQol levels of women and their husbands during fertility treatments. Women will show higher stress and lower FertiRQoL levels in the context of fertility treatments than will their husbands. H2: The optimism of women and their husbands will associate negatively with the stress experienced by them and their husbands during fertility treatments. Woman’s and their husbands’ stress in turn will predict higher levels of FertiRQoL among themselves and their husbands. H3: The stress levels, optimism, and FertiRQoL of women and their husbands will predict the success of their fertility treatments. Lower stress levels and higher levels of optimism and FertiRQoL will predict the success of fertility treatments (i.e., of achieving a pregnancy).
Methods
Design
The reporting of this study conforms to the STROBE statement for cross-sectional studies. 44 A cross-sectional design was utilized to assess psychological variables, with a short-term prospective follow-up to determine pregnancy achievement. Participants were recruited during their IVF treatment cycle. At baseline, women and their husbands were asked to complete self-report questionnaires. Two weeks after embryo transfer, participants were contacted by phone to obtain information regarding the outcome of the treatment, specifically serum β-hCG levels, and thus determine pregnancy status.
Sample size
The sample size was calculated using G*Power software for multiple regression analysis (APIM), examining predictors of FertiRQol. 45 A sample size of 41 couples was required to obtain 80% power, a small to medium effect size, and 95% confidence level. The final sample included 51 couples undergoing IVF (N = 102 participants).
Procedure
Participants were recruited using a non-probability sampling method, through two closed Facebook groups for women undergoing IVF treatment. Prior to recruitment, approval was obtained from the group administrators to post an invitation to participate in the study. Women interested in participating contacted the research team directly.
Inclusion criteria were heterosexual Jewish couples currently undergoing an IVF cycle, fluency in Hebrew, both partners’ consent to participate, and providing a telephone number for follow-up regarding treatment outcomes. Exclusion criteria were women younger than 25 or older than 50 and women without a spouse.
Fifty-eight women contacted the research team via email. Of these, 55 met the inclusion criteria and received a unique family code and a link to the questionnaires via Google Forms. Fifty-one couples completed the full set of questionnaires.
Women were asked to invite their male partners to complete the questionnaires using the same link. Each couple used a shared link and unique code so that husbands’ responses could be matched. Partners were instructed to complete the questionnaires separately and to answer all items without skipping. Only data from couples where both partners completed all measures were included in the analyses.
Participants received a written explanation of the study’s purpose and procedures and provided informed consent prior to participation. They were assured that participation is voluntary, that they can withdraw at any time, and that all data would remain confidential, securely stored, and accessible only to the research team. No identifying details were recorded.
Data were collected between April and June 2022. Questionnaires were administered while participants were actively undergoing IVF treatment, between the first day of menstruation in the current cycle and the day of egg retrieval. Two weeks after embryo transfer, participants were contacted by phone to report treatment outcomes based on serum β-hCG levels. Of the 55 eligible women, 51 couples (102 participants: 51 women and 51 husbands) completed all measures and were included in the final sample. Of the four couples who did not complete the questionnaires and were therefore excluded, two did not complete the IVF cycle.
Research measures
The study included four questionnaires.
Questionnaires on socio–demographics and fertility–related data
The sociodemographic and fertility questionnaires utilized were developed for the purpose of the current study. Sociodemographic data included items commonly used for sample characterization, such as age, sex, and years of education. The fertility questionnaire was developed in collaboration with clinical experts (physicians and nurses working in IVF clinics). It was based on studies describing the development of similar research tools, 46 including two instruments used in the present study,20,47 as well as on published research examining couples or women undergoing fertility treatments.48,49 Content validity was then assessed and confirmed by the same expert physicians and nurses. Notably, a marital status item was included to verify that participants met the inclusion criteria, specifically that they were part of a couple. The questionnaire included 15 items, including among others age, marital status, length of marriage in years, fertility difficulties, and types of treatments the couple underwent previously.
Fertility problem stress scale
This 12-item validated instrument was developed by Andrews, Abbey, and Halman 47 to assess the stress wives and husbands may experience due to infertility. The questionnaire was translated into Hebrew and validated by Plazenshlov. 50 It comprises two identical questionnaires, differentiated only by grammatical gender (one for women and the other for their spouses). The original questionnaire also includes one item on ovulation tracking, which was omitted as the research participants did not perform this activity. Hence, the tool currently consisted of 11 items. Sample item: “How stressful has it been for you to deal with this fertility problem?”. Items were rated on a 5-point Likert-type scale ranging from 1 (“not at all”) to 5 (“a great deal”), indicating participants’ agreement with each item. The last item asked participants to note their absence from work following the fertility treatments on a scale ranging from 1 (never) to 5 (11 times or more). Specifically, for this item participants who did not work had the option of noting “not relevant”. The internal consistency of the original scale was Cronbach’s α = 0.86;50 in the present study Cronbach’s α was = 0.87.
Fertility–related quality of life (FertiRQoL)
This validated questionnaire is the first internationally validated tool for evaluating FertiQoL, developed by Boivin et al. 20 Twenty-seven experts from 11 countries constructed the questionnaire. It was translated into numerous languages by professional translators and then reviewed by medical and psychological experts fluent in each relevant language. Porat-Katz (2008) translated the questionnaire to Hebrew (https://sites.cardiff.ac.uk/fertiqol/download/). The FertiQoL includes 26 items, of which two items capture an overall evaluation of physical health and satisfaction with QoL, which are not calculated in the overall score. These two items provide the background health and life satisfaction context for evaluating FertiQoL.
The remaining 24 items are rated on a five-point Likert scale and divided into four subscales: 1) Emotional, with six items; sample item: “Do you feel drained or worn out because of fertility problems?”; 2) Social, with six items; sample item: “Are you satisfied with the support you receive from friends with regard to your fertility problems?”; 3) Body-mind, with six items; sample item: “Do you experience grief and/or feelings of loss about not being able to have a child (or more children)?”; and 4) Social, with six items; sample item: “Have fertility problems had a negative impact on your relationship with your partner?”
Each subscale comprises six items. For overall subscale scores, the sum of all items in each domain is multiplied by 25 and divided by 6. Each domain’s scores range from 25 to 125, with a higher score indicating better FertiQoL. The maximum total score (for the entire questionnaire) is 500. Boivin et al. found internal reliability of α = 0.92. 20 In the present study, the internal consistency for all 24 items (total score) was α = 0.90.
Revised life orientation test
This validated questionnaire is a six-item self-report measure (with the addition of four filler items), evaluating trait optimism by assessing generalized expectancies for positive versus adverse outcomes, was developed by Scheier et al. 51 The questionnaire was translated into Hebrew by Horowitz-Primor 52 for a study conducted among 330 women experiencing infertility, which found Cronbach’s alpha reliability coefficients of 0.62 for dispositional optimism and 0.73 for dispositional pessimism. In another study conducted by Tzur-Peled 53 among nurses working in intensive care units, the questionnaire’s internal reliability was examined and Cronbach’s alpha of 0.745 was found.
Respondents were asked to indicate their degree of agreement with the statements on a 5-point Likert scale ranging from 0 (strongly disagree) to 4 (strongly agree). Sample item: “In uncertain times, I usually expect the best”. Three of the six items are worded positively and three negatively. The negative items were reverse scored. In their study, Scheier et al. found Cronbach’s α = 0.78, test-retest reliability of α = 0.79, and strong convergent and discriminative validities. 51 In the current sample, internal consistency was α = 0.57 for the total score. One item (the second negative item) was deleted to obtain higher reliability. The new reliability was found to be adequate, with Cronbach’s α = 0.71.
Data analysis
All data were complete, with no missing values for any of the research variables. Accordingly, no imputation or data replacement procedures were necessary. First, the normality of the data was assessed using skewness, kurtosis, and Shapiro-Wilk normality test, 54 using IBM SPSS-28. Variables with skewness and kurtosis values between -1 and +1 and non-significant outcomes in the Shapiro-Wilk normality test were considered normally distributed. The full details of the variables’ descriptive statistics are presented in Supplementary Table 1. Then, confirmatory factor analyses (CFA) were conducted using AMOS-25, to examine the factorial validity of the measurement model.
Following Hoyle and Panter, 54 the model fit with the data was evaluated using four goodness of fit indices: the χ2 statistic, the root mean square error of approximation (RMSEA), and the comparative fit index (CFI). 54 An RMSEA below 0.06 in combination with CFI above 0.95 indicates excellent fit, whereas RMSEA values below 0.08 and CFI above 0.90 indicate adequate fit. All items were specified to load on their respective latent constructs based on theoretical expectations. Maximum likelihood estimation was used. Then, we examined the Pearson’s correlations between stress, optimism, FertiRQoL, and treatment success for women and their husbands, and socio-demographic variables, using SPSS-28.
The three main hypotheses were then examined. The first hypothesis, regarding differences in stress, optimism, and well-being between women and their husbands, was examined through t-tests for dependent samples, using SPSS-28. The second hypothesis, regarding dyadic associations between stress, optimism, and well-being, was examined through the Actor-Partner Interdependence Model (APIM) for dyadic relationships using structural equation modeling (SEM) in the R Lavaan package. 55 This analysis allowed us to investigate two-person relationships and to account for the effects within couples.56,57 In this analysis, an “actor effect” refers to the association between variables separately for women and their husbands, whereas a “partner effect” refers to the association between actor variables and partner variables. The APIM examines the actor and partner effects simultaneously while accounting for shared variance. We then investigated whether the optimism of women and their husbands predicted their own and their partners’ stress and FertiRQoL, using APIM analyses for mediation models.
We treated dyads as distinguishable by gender and tested distinguishability by comparing constrained vs. unconstrained models for equality of actor and partner paths, as recommended by Cook and Kenny. 56 Model fit indices (e.g., CFI, RMSEA) were used to evaluate the overall adequacy of the model. Finally, the third hypothesis, whereby optimism, stress, and well-being would predict the success of the fertility treatment, was examined using a logistic regression.
Ethical considerations
The study protocol was approved by the Tel Aviv University Ethics Committee (#0001606-1), which granted an exemption from signing an informed consent form as data were collected online, no sensitive information was obtained, and there was only minimal risk to participants. The research participants expressed their consent to participate in the study by confirming the statement: “I agree to participate in the study on quality of life during IVF treatments”. Only then were they directed to the research questionnaire.
Results
Participants
Socio–demographic characteristics of the sample.
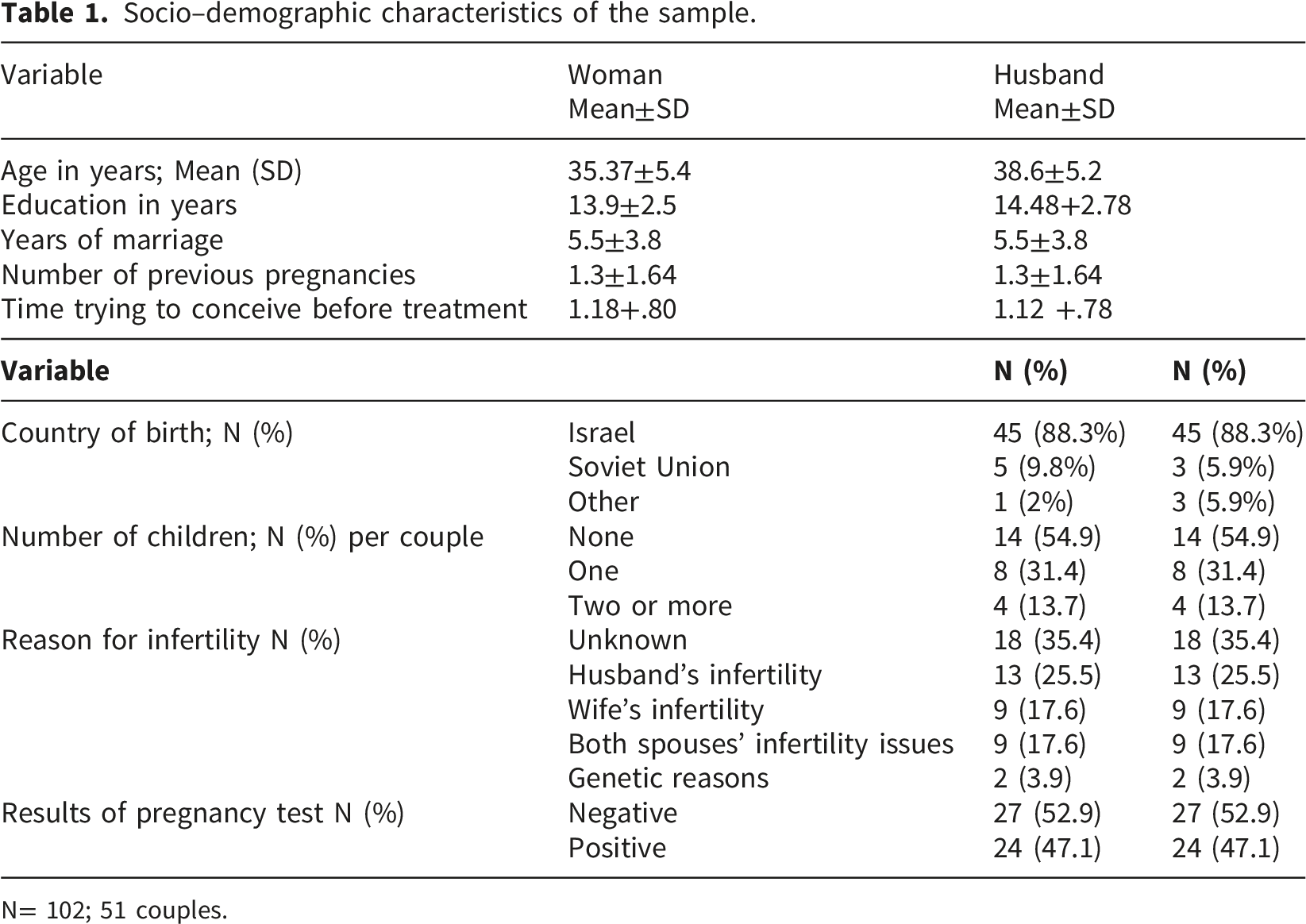
N= 102; 51 couples.
Preliminary analyses
Measurement model
To examine the convergent and discriminant validity of the measures, we conducted a confirmatory factor analysis (CFA) on the primary research variables: optimism (woman and husband), stress (woman and husband), and FertiRQoL (woman and husband). To assess construct validity, men and women were analyzed together in a single, combined measurement model, rather than separately as in the main dyadic analyses. All items were constrained to load only on their designated latent factors. No equality constraints were imposed on the factor loadings, and all covariances between latent factors were freely estimated. The measurement model demonstrated an acceptable fit with the data: χ2(74) = 174.16, p < .001, CFI = .91, RMSEA = .09.
All standardized factor loadings were significant (p < .05) and above the conventional threshold of .35, indicating acceptable convergent validity. A full description of factor loadings is presented in Supplementary Table 2.
Correlations among the research variables
Results of Pearson’s correlations among research variables for women and their husbands.
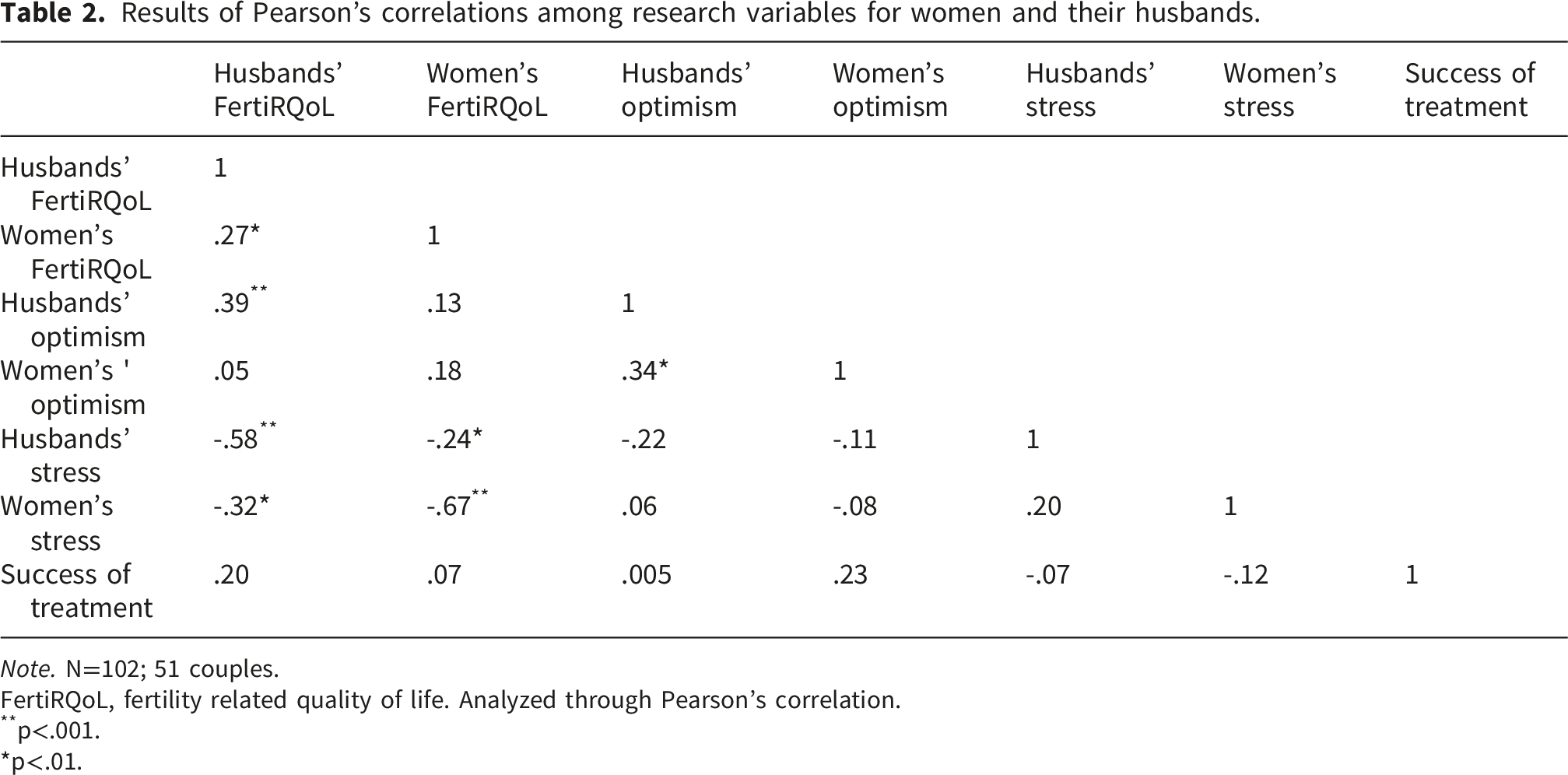
Note. N=102; 51 couples.
FertiRQoL, fertility related quality of life. Analyzed through Pearson’s correlation.
**p<.001.
*p<.01.
Associations between socio–demographic variables and the research variables
Correlations between socio–demographic variables and research variables.
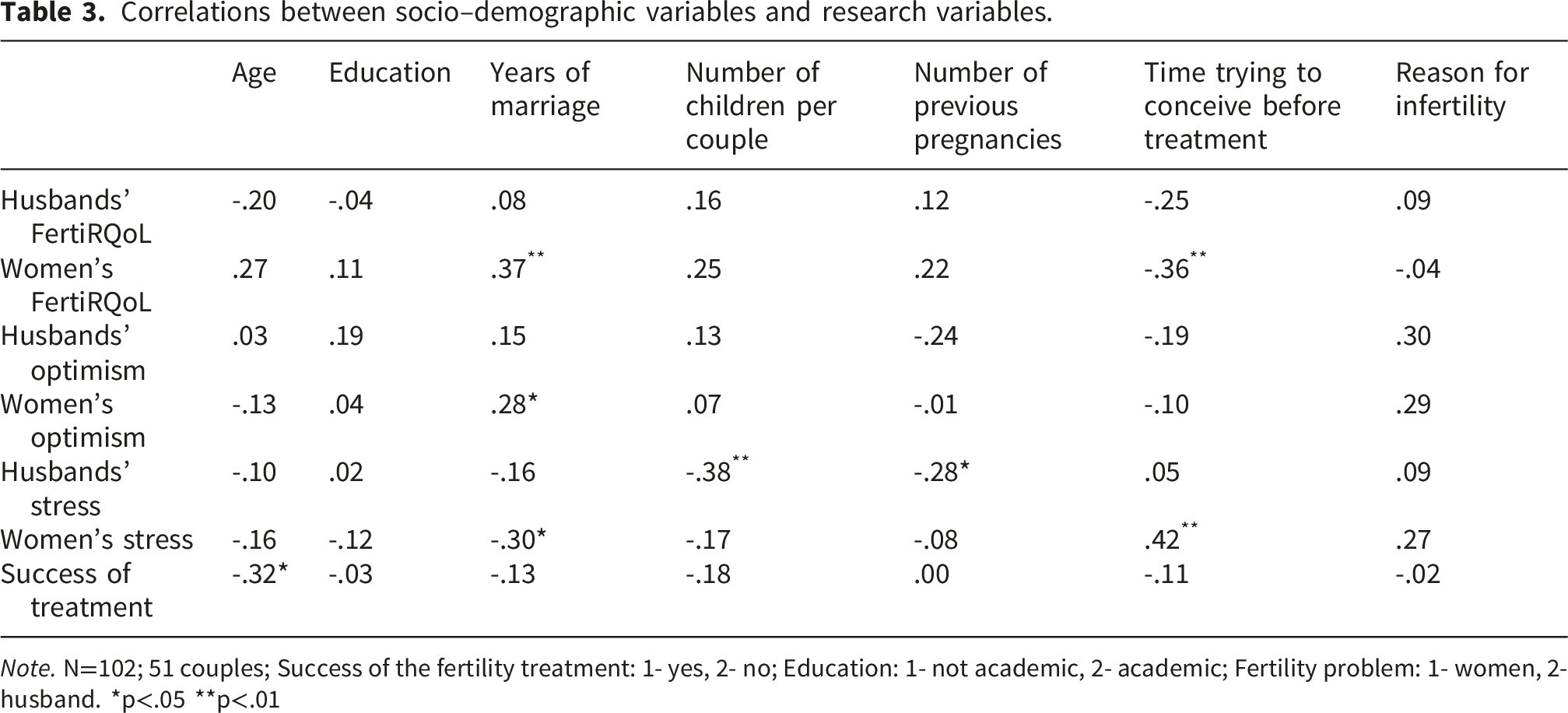
Note. N=102; 51 couples; Success of the fertility treatment: 1- yes, 2- no; Education: 1- not academic, 2- academic; Fertility problem: 1- women, 2- husband. *p<.05 **p<.01
Main analyses
Differences in stress, optimism, and FertiRQoL between women and their husbands
Differences between women and their husbands in the research variables using t–tests for dependent samples.
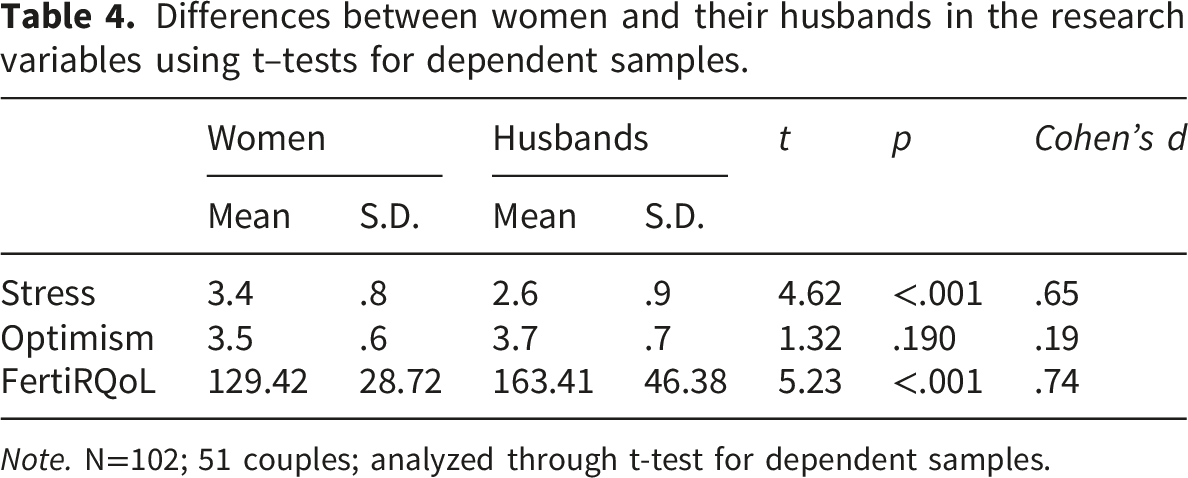
Note. N=102; 51 couples; analyzed through t-test for dependent samples.
Actor–partner interdependence mediation model analysis
To examine dyadic associations among optimism, stress, and FertiRQoL, we used the Actor–Partner Interdependence Mediation Model (APIM). The mediation model included optimism as the predictor, stress as the mediator, and FertiRQoL as the outcome variable. Actor and partner paths were simultaneously estimated using structural equation modeling in the R Lavaan package. Variables were standardized prior to analysis to ensure comparability. Dyad members were treated as indistinguishable. The test of distinguishability, which included six equal actor and partner effects across members, three equal means, and three equal variances, was not statistically significant (χ(12) = 45.86, p < .001, RMSEA = .23), indicating that the women and their husbands showed no statistical distinction.
The structural equation models were estimated using the Lavaan program with FIML to handle the missing data. The standard errors and confidence intervals for simple, direct, and total effects were based on normal theory. However, the standard errors and confidence intervals for the simple and total indirect effects use the Monte Carlo method, also called the parametric bootstrap, with 40,000 trials.
Results of the APIM mediation model predicting FertiQoL.
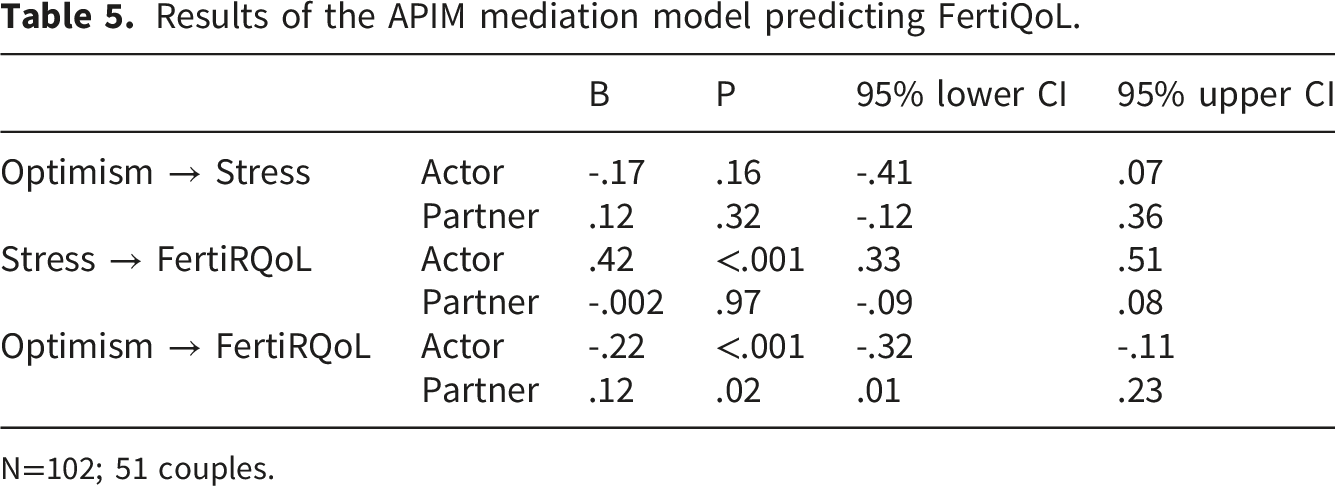
N=102; 51 couples.
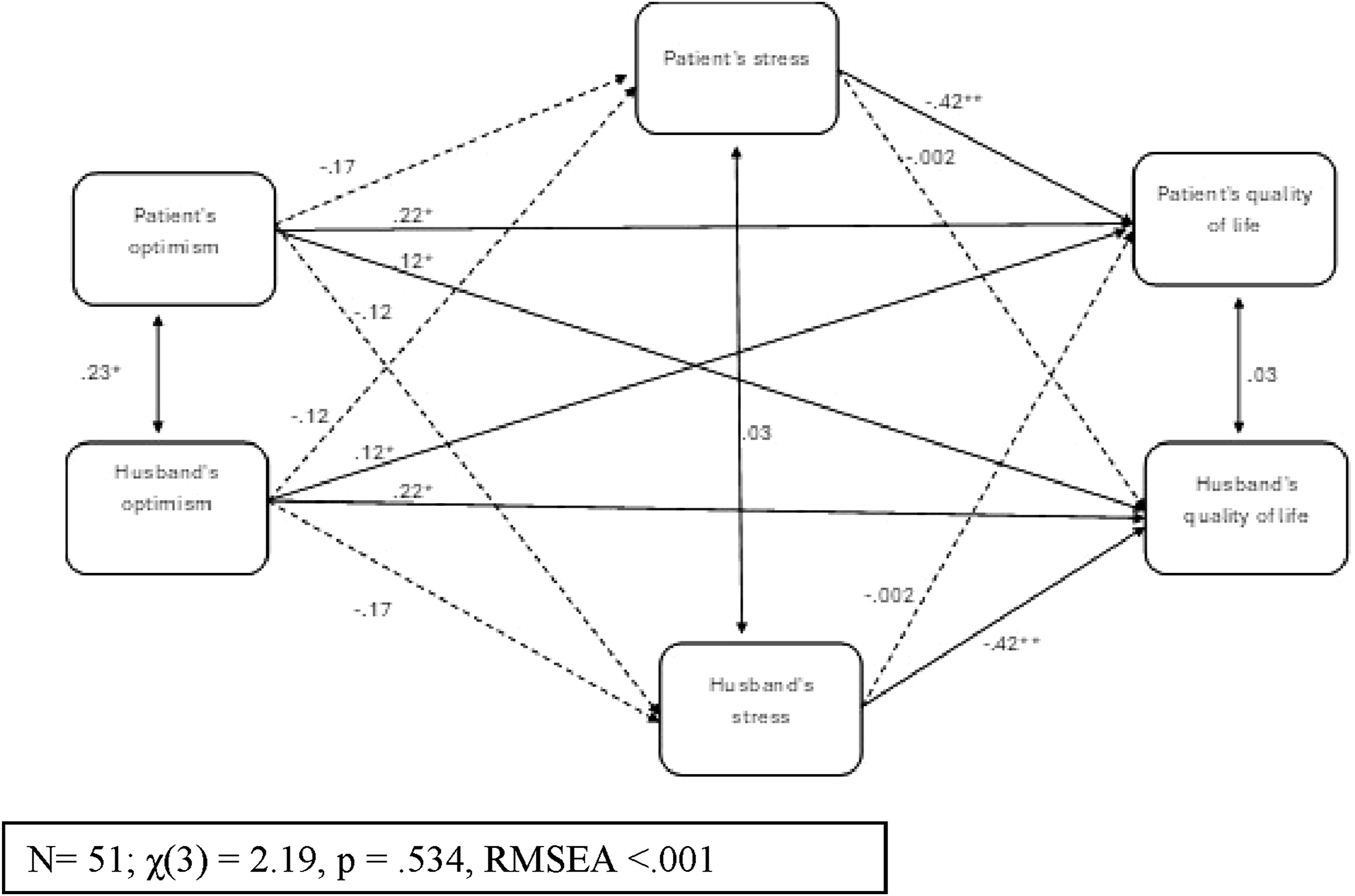
Actor–partner interdependence mediation model analysis investigating women’s and husbands’ FertiQoL.
Total and indirect actor and partner effects.
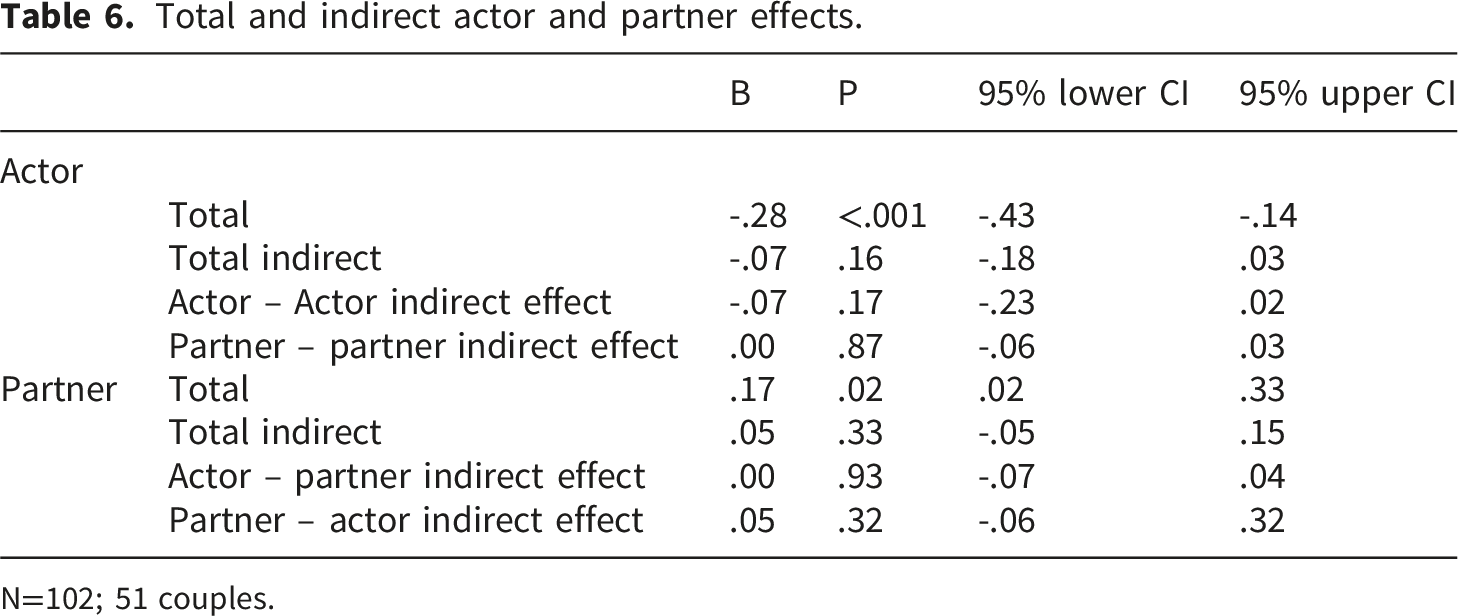
N=102; 51 couples.
Prediction of success in fertility treatments
To examine whether the stress levels, optimism, and FertiRQoL of women and their husbands predicted the success of their fertility treatments, logistic regression was computed. Participants’ age was included, since the correlation between age and success of the fertility treatment was significant. In contrast to H3, the results showed that the logistic regression model was not significant (χ 2 (7) = 11.09, p = .13, R 2 = .20) and correctly classified 74% of the cases. Only age was found to be a significant negative predictor of success in the fertility treatments (B = -.17, SE = .08, Wald = 4.76, p = .02, OR = .84); among younger participants the treatments were more likely to succeed.
Discussion
The purpose of the present study was to examine the influence of stress and optimism among women and their husbands undergoing IVF on their FertiRQoL, and the associations of these variables with the success of the IVF treatment. The results show that the stress experienced by women and their husbands was negatively associated with their own FertiRQoL. Husbands’ FertiRQoL was positively associated with their own optimism and negatively with the women’s stress. Also, husbands’ FertiRQoL was positively associated with women’s FertiRQoL. Confirming Hypothesis H1, women expressed more stress and lower FertiRQoL than their husbands. Interestingly, analysis of the APIM revealed a mutual effect of the dyad member’s optimism on their partner’s FertiRQoL.
The negative association between stress and QoL is well documented in healthy young adults 58 and in various diseases such as cancer. 59 Few studies have measured the association between stress and FertiRQoL among couples undergoing fertility treatments, and those that did focused mainly on the women. For example, studies reported a negative association between stress and FertiRQoL among women who conceived through artificial reproduction technology.10,60 One study conducted among infertile couples found a negative correlation between stress and FertiRQoL. 2
Women’s FertiRQoL exhibited a positive correlation with their husbands’ FertiRQoL. This suggests that the well-being of one partner is linked to the well-being of the other. This relationship between spouses’ FertiRQoL was also reported in other studies. 2 In addition, the current results show that women’s optimism correlated positively with their husbands’, indicating the effect of spouses’ psychological state on each other. A recent review supports these findings by suggesting that infertile couples’ optimism might serve as an important factor in their coping. 13
Interestingly, husbands’ FertiRQoL correlated negatively with women’s stress, showing that women’s psychological distress negatively affects their spouses’ quality of life. This is supported by a previous study investigating infertile couples, which found that wives’ depression was associated with their husbands’ FertiRQoL. 2 These findings emphasize the mutual influence of partners on each other and how important it is that health workers support both spouses when undergoing IVF treatments.
The first hypothesis predicted significant differences between women’s and husbands’ levels of stress and FertiRQoL. The hypothesis was confirmed, with women reporting more stress and lower FertiRQoL compared to their husbands. The difference in stress was moderate in magnitude, whereas the difference in FertiRQoL was large, indicating a meaningful disparity between partners’ psychological experience of fertility treatments. These findings suggest that the experiences of women and their husbands during IVF treatment may differ not only statistically but also in magnitude, reflecting distinct emotional and experiential aspects of the fertility treatment process. This finding was not surprising, since in many cases IVF puts women through more difficult treatments, both physically and mentally, compared to their husbands. For example, when infertility is attributed to a female factor, women typically undergo blood tests, hormonal treatments, ultrasounds, oocyte retrieval under anesthesia, and embryo transfer, whereas men are often only required to provide a sperm sample. 22
Nevertheless, infertility-related distress should not be conceptualized as predominantly female. In our sample, male- and female-factor infertility were similarly prevalent (Table 1), and certain male-factor diagnoses (e.g., azoospermia) may require invasive procedures such as testicular sperm extraction and intracytoplasmic sperm injection, which are associated with increased stress and reduced quality of life. 61 As previously reported, lower FertiRQoL in women is further exacerbated by the fact that in many cases women do not tell relatives and friends that they are undergoing fertility treatments or that they are experiencing accompanying emotional distress. 62
Regarding stress, the current finding is consistent with the research literature, according to which female infertility patients report higher levels of fertility-related stress than their partners.23,31 This difference may also stem from the fact that fertility procedures overburden women’s bodies, possibly leading women to feel that they inadequately meet the demands of the procedure, a situation that may create increased stress. In the Israeli context, it can be assumed that women’s stress levels exceed those of their husbands, due to the importance of motherhood and childbirth as a central value associated with women in Israel. 63 This is reflected in Israel’s highest fertility rate of all OECD countries. 17
The second hypothesis predicted dyadic associations between stress, optimism, and FertiRQoL. Using the APIM, the dyadic analysis found that the stress of both women and their husbands was negatively associated with their own lower FertiRQoL, although the effect on their partner was not significant. Although one study found that each partner’s distress influences the other’s, 64 the current study did not find evidence of both partners’ stress affecting each other. It appears that during fertility treatments each spouse is immersed in their own experiences and difficulties, without considering the difficulties and experience of their partner. As a result, each of them experiences the psychological consequences of the process alone. This may stem from how stress is experienced and managed between genders.
Recent studies suggest that during fertility treatments husbands and wives use different coping strategies to adapt to infertility. Consequently, the impact of the treatments on each partner is experienced differently.64,65 These differences may contribute to the lack of dyadic associations between spouses’ stress. Another possibility is that the dynamics within the dyadic relationship, such as levels of support, trust, and closeness, affect how spouses interact emotionally. 65 If one spouse feels more supported or has stronger coping resources within the relationship, they may be less affected by the other’s emotions. 66 Further studies to identify factors related to dyadic relationships during IVF treatments are recommended.
The predicted dyadic association between optimism and FertiRQoL was found to be significant. It is widely believed that patients with a positive outlook cope more effectively with health challenges, suggesting that positive expectations can have beneficial effects on well-being. The present results add a new dimension to the reciprocal effect of optimism among women and their husbands on their spouses’ FertiRQoL. This suggests that optimism may serve as a resource that helps couples cope and maintain a sense of normalcy during fertility treatments. Indeed, research has shown that optimism is related to better marital satisfaction among couples experiencing infertility.65,67
According to Lazarus and Folkman, a positive outlook may encourage individuals to engage in behaviors that promote good health, such as using coping strategies that support recovery. 29 The dyadic effect of optimism on FertiRQoL underscores its importance in everyday interactions between spouses. Being optimistic can significantly affect how couples manage their day-to-day experiences, especially when dealing with fertility issues. Dyadic coping strategies, which involve both partners working together to handle critical and stressful experiences, can enhance the sharing of feelings and thoughts related to infertility. 65 Optimism may further facilitate this sharing among couples. Additionally, an optimistic approach may enhance mutual support between spouses, which can in turn reduce stress 66 and thus elevate QoL. It can be concluded that optimism serves as a vital resource for couples undergoing fertility treatments, positively affecting how they share feelings and thoughts and thereby enhancing FertiRQoL.
The third hypothesis predicted that optimism, FertiRQoL, and stress would predict the success of the IVF treatment. The results show that only age predicted the treatment’s success. The finding regarding age is not surprising, as it is well known that younger age is associated with better fertility and IVF success. 68 However, the results showing that stress, optimism, and FertiRQoL of women and their husbands were not related to the success of IVF treatments may be explained by the small sample consisting of 51 couples, although more participants were included than required by the statistical power analysis (41 couples). According to the Israeli Ministry of Health, the success rate of IVF is 25%, 69 so it is also probable that IVF treatment may exert many different emotional responses connected to the success of IVF which were not measured in this study. Hence, conducting a larger study that will include a larger sample and examine a wider range of variables is recommended.
Implications for clinical practice
The findings of this study have several implications for clinical practice in the context of fertility treatments. First, the significant associations between optimism and FertiRQoL for both patients and their partners underscore the potential value of incorporating psychological support interventions aimed at fostering optimism and emotional well-being during the IVF process. Such interventions may include individual counseling, cognitive-behavioral therapy (CBT) aimed at enhancing adaptive coping and cognitive restructuring, stress management programs (e.g., relaxation training or mindfulness-based interventions), and couple-based therapy focused on strengthening dyadic coping and communication. The direct association of stress with lower FertiRQoL suggests that ongoing stress monitoring and management is important for couples undergoing IVF treatment. Clinics may consider implementing brief evidence-based psychosocial interventions at key stages of the IVF process to reduce stress and enhance coping resources.
Also, the finding that demographic factors such as age and marriage duration are associated with psychosocial outcomes may guide practitioners to tailor support based on couples’ background and fertility history. These insights collectively highlight the importance of integrating psychological assessments and support into routine fertility care to enhance patients’ quality of life. In this context, the routine use of validated measures such as the Fertility-Related Quality of Life (FertiRQoL) questionnaire for ongoing monitoring of stress and quality of life during IVF treatment may help identify couples at higher risk of psychological distress and allow for timely referral to appropriate psychosocial services.
Limitations and strengths
The present study has several notable strengths. First, the use of a dyadic design allowed examination of both partners’ experiences during IVF treatment, providing a more comprehensive understanding of how psychological factors operate within couples. Second, the study employed validated and widely used measures, including the fertility-specific quality-of-life instrument (FertiRQoL), which enhances the reliability and relevance of the findings. Third, participants were recruited from multiple IVF clinics across the country, increasing the external validity of the study and reflecting real-world treatment contexts.
Despite these strengths, several limitations should be acknowledged. The study employed a cross-sectional design, with all variables assessed at a single time point, which precludes conclusions about temporal ordering or causal processes. Accordingly, the mediation analyses should be interpreted as reflecting indirect associations consistent with the proposed theoretical framework rather than evidence of causal or longitudinal mechanisms. Future research using longitudinal or experimental designs is needed to more rigorously examine the directionality of these relations
Although the sample size exceeded that required according to the sample size calculation, it may still have limited the ability to detect some relationships between the research variables. Also, recruitment via IVF Facebook groups may introduce self-selection bias, as women who join such groups may differ in their help-seeking behavior or psychological engagement from those who do not. However, in our national context these groups are a common and widely used support resource during IVF treatment, and spouses were recruited independently by the women who agreed to participate, rather than through the groups. Another limitation relates to sample heterogeneity and generalizability. Participants were receiving treatment at IVF clinics across the country, and while some variation in treatment protocols between clinics may exist, this could have influenced participants’ responses and introduced a degree of heterogeneity within the sample.
In addition, the dyadic data collection approach might have caused bias, as only couples in which both partners agreed to participate were included. This might have excluded couples in conflict, those with less communication or where one partner is less engaged, limiting the generalizability of the findings. Also, cultural differences in perceptions of infertility, stress, optimism, and quality of life may limit the generalizability of these findings to other populations. One more limitation is the reliance on self-reported data, lacking access to objective clinical records. While self-report measures provide valuable insight into participants’ perceptions and experiences, they may be subject to inaccuracies, particularly regarding clinical outcomes.
Furthermore, the study may not have fully controlled for all potential confounding variables affecting stress, optimism, FertiRQoL, and treatment success, such as individual health factors, financial strain, or relationship dynamics. Finally, an additional limitation concerns the confirmatory factor analysis (CFA) conducted to examine the measurement model. Although the sample size (N = 102) was adequate for the primary APIM regression analyses, it is relatively modest for structural equation modeling procedures. While the model demonstrated acceptable overall fit indices, the RMSEA value slightly exceeded conventional cutoffs, suggesting that the measurement model should be interpreted with caution. Future studies with larger samples are needed to further validate the factorial structure of the constructs examined in the present study.
Conclusions
The study indicates a negative association between stress and FertiRQoL among couples undergoing IVF treatment, adding to the literature that demonstrates this association in various healthy and non-healthy populations. The positive correlations found in the study between the FertiRQoL of women and their husbands and between women’s FertiRQoL and their husbands’ optimism highlight the importance of spouses’ support for each other. Although women experienced more stress than their husbands, the results show that both experience stress; therefore, consideration should be given to providing support to both partners during IVF treatment rather than solely to women.
The finding that the stress of wives or husbands did not influence their spouses’ FertiRQoL further indicates not only the importance of providing support to both spouses but also the benefits of joint plans, so that during IVF treatments spouses can provide support to each other. The dyadic effect of optimism on FertiRQoL points to the importance of optimism for maintaining everyday life. Traditionally, optimism is considered a trait, however Millstein et al. suggested that it may change and develop over time. 70 Hence, it is important to assess optimism throughout fertility treatments and to teach couples mechanistic tools such as positive psychology interventions 71 and positive imagination, 72 which can induce optimism. Lastly, we recommend carrying out a broad follow-up study to evaluate additional psychological factors that may be related to the success of IVF treatments.
Supplemental material
Supplemental material - Couples’ optimism, stress, and quality of life when undergoing fertility treatments: A cross–sectional study with prospective outcome assessment
Supplemental material for Couples’ optimism, stress, and quality of life when undergoing fertility treatments: A cross–sectional study with prospective outcome assessment by Gal Tarasov, Rinat Cohen, Sigalit Warshawski, and Sivia Barnoy in Women's Health.
Footnotes
Acknowledgements
The authors sincerely thank the research participants for their willingness to share their experiences and emotions.
Ethical considerations
The study protocol was approved by the Tel Aviv University Ethics Committee (#0001606-1), which granted an exemption from signing an informed consent form as data were collected online, no sensitive information was obtained, and there was only minimal risk to participants.
Consent to participate
The research participants expressed their consent to participate in the study by confirming the statement: “I agree to participate in the study on quality of life during IVF treatments”. Only then were they directed to the research questionnaire.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used to support the findings of this work are available on request from the authors.
Artificial intelligence usage
The authors used ChatGPT (OpenAI) for language editing of the manuscript. The authors reviewed and approved all content and take full responsibility for the final version.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.