
Abstract
Background
The protective period is the ideal time for folic acid supplementation to prevent neural tube defects. It supplements at least one month before conception up to three months after conception. World health organization recommends 0.4 mg daily for women from preconception through the first trimester, yet utilization remains challenged.
Objective
To assess protective folic acid utilization and associated factors among women attending antenatal care units in Illuababor Zone public facilities.
Design
Institutional based cross-sectional study was conducted.
Methods
This study was conducted among 714 pregnant women attending antenatal care units in public health facilities of the Illuababor zone, selected through a systematic random sampling technique. The data were collected using a semi-structured interviewer-administered questionnaire. Bi-variate and multivariate logistic regression analyses were undertaken, and the association was declared at 95 CI and p-value less than 0.05.
Results
A total of 714 pregnant women participated in the study, resulting in a 97.4% response rate. Only 119 (17%), [95% CI: (14.0, 19.6)] women had utilized protective folic acid. Residence (AOR: 2.16, 95% CI: 1.38, 3.40), history of family planning utilization (AOR: 2.65, 95% CI: 1.23, 5.71), gravida (AOR: 2.07, 95% CI: 1.17, 3.64), gestational age of antenatal care booking (AOR: 8.77, 95% CI: 5.33, 14.45), and knowledge about folic acid (AOR: 2.99, 95% CI: 1.90, 4.71) were identified as significant predictors of folic acid utilization.
Conclusions
Folic acid utilization in the protective period stands at just 17%. Key positive predictors are urban residence, prior family planning use, primigravida status, early first-trimester ANC booking, and strong knowledge of folic acid. Enhancing uptake demands multifaceted strategies addressing knowledge gaps and rural access barriers through targeted education and healthcare services.
Background
The protective period is the ideal time for folic acid supplementation to prevent neural tube defects, from at least one month before conception up to three months after. 1 Folic acid, also known as vitamin B9, is essential for numerous bodily functions, particularly in cell division and the production of DNA. 2 It plays a crucial role in the development of the neural tube, which eventually forms the brain and spinal cord in a developing fetus. 3 Adequate folic acid intake before and during early pregnancy is vital for preventing neural tube defects (NTDs). 4 Despite its known benefits, compliance with folic acid supplementation can be low in some regions, including Ethiopia, where educational initiatives and healthcare access may be lacking. 5 Efforts to improve awareness about the importance of folic acid and provide resources for supplementation could significantly impact maternal and child health by reducing the incidence of preventable birth defects.6–8
Globally, around 300,000 infants are born with NTDs each year, resulting in about 88,000 deaths and leaving millions with disabilities. 9 In 2022, sub-Saharan Africa, congenital anomalies significantly contributed to infant mortality, accounting for 17% to 42% of infant deaths. 10 Each year, around 240,000 newborns die within their first 28 days due to these anomalies, representing one in ten perinatal deaths and one in four neonatal deaths.11,12 The incidence of NTDs is four times higher in developing countries, with NTDs accounting for up to 29% of neonatal deaths. 13 While NTD rates have decreased in high-income countries over the past thirty years, 14 they continue to present a major public health challenge in low-income countries, including Ethiopia.15,16
The protective period folic acid supplementation reduces the risk of first occurrence and recurrence of NTDs by approximately 60-70%. 1 And also folic acid fortification of daily staple foods reduces the incidence of NTD (up to 46%).7,8,17 The World Health Organization (WHO) recommends that all women start taking a folic acid supplement of 400 micrograms (0.4 mg) of folic acid daily before conception and during early pregnancy to significantly reduce the risk of having a baby with NTDs. 18 Women who had a history of adverse pregnancy outcomes (APOs), like higher risk due to personal or family history of NTD, diabetes mellitus, and miscarriage, were recommended to take high-dose (5 mg) folic acid daily.5,6,8,19,20
Although folic acid supplementation is proven to prevent a large proportion of NTDs, pregnant women in low-income countries still do not follow the WHO recommendations. 21 Due to this, only 23% of the folic acid-preventable NTDs are prevented.22,23 Evidence from Sub-Saharan Africa shows that the proportion of women using folic acid during the preconception period ranges from about 1.9% to 45.2%. 5 Moreover, numerous studies have shown that women with poor knowledge about folic acid are expected to use folic acid supplements.24–28
Ethiopia has updated its national preconception care guidelines. Key recommendations include daily supplementation of 0.4 mg folic acid alone or with 30–60 mg elemental iron for all women, starting at least three months before conception and continuing through the first trimester (at least 90 days). The guidelines also emphasize expanded screening for chronic diseases and better integration of preconception care into existing health systems. 19
Despite the recommendations for folic acid supplementation, implementing these guidelines poses significant challenges of implementation in various healthcare settings. 29 There is a considerable burden of folate deficiency among women of reproductive age, with a pooled prevalence of 20.8%, ranging from 1.9% to 46%, indicating a serious public health issue. 30 Consequently, the incidence of neural tube defects (NTD) is recorded at 63-83 per 10,000 births in Ethiopia. 31 Various studies have identified factors associated with the prevalence of NTDs, including inadequate periconceptional folic acid intake, 32 lack of staple food fortification, 33 high-risk lifestyles, 34 advanced maternal age, 33 low education, family history, 33 and rare prenatal screening. 33 Healthcare shortages limit surgery to major hospitals; late myelomeningocele treatment causes hydrocephalus, meningitis, and deficits. Outcomes are poor, leading to high in-hospital mortality; 75% of infants die before age 5, survivors face lifelong disabilities, plus elevated perinatal/infant mortality.32,33,35
Despite prior studies, a systematic review reveals persistently low pooled prevalence rates of 14.10% across Sub-Saharan Africa, with regional variations. In Ethiopia, folic acid utilization ranges from 1.9% to 11.4 %,36,37 indicating poor utilization. Several context-specific factors contribute to this issue, including low awareness of folic acid and inadequate antenatal care visits.
Ethiopia has updated two key recommendations for optimal folic acid utilization to protect pregnancy outcomes, aligning with Sustainable Development Goals (SDGs); strengthening preconception care and promoting early antenatal care (ANC) booking before 12 weeks of gestation. These periods are crucial because the health of the woman and the outcome of her pregnancy are largely determined during this time. Preventing and treating NTDs will be essential to achieving SDG 3.2, which aims to end preventable deaths of newborns and children under 5 years of age. Therefore, this research aims to assess the utilization and associated factors of folic acid during these protective periods following the initiation of preconception care and the introduction of the new eight-contact ANC model, which encourages women to attend their first ANC contact within the first trimester.
Methods and materials
Study design and period
A facility-based cross-sectional study design was carried out in Illuababor Zone public health facilities from November to December 2024. Illuababor is located in Southwest Ethiopia in the Oromia region. Its capital town is Metu town, located at a distance of about 600 km from Addis Ababa. Illuababor Zone has one town administration and 14 rural districts with a projected total population of 921,217. 38 It has one referral and one district hospital, forty health centers, and 273 health posts to serve the population of the zone. 39
Population
Pregnant women who attending ANC follow-up in the selected public health facilities were study population.
Eligibility criteria
Inclusion criteria
Pregnant women aged 18 years and above, were registered for regular ANC follow-up at any gestational age, and provided informed consent during the data collection period were included in the study.
Exclusion criteria
Pregnant women who with speaking difficulties due to severe illness and those referred from other health facilities were excluded. And also those comes for the first contact before 12 weeks of gestational age were excluded.
Sample size determination
The sample size was determined using second objective (factors associated with folic acid utilization), a double population proportion formula using the Open Epi Info version 7 statistical software package. The following assumptions were considered: 95% confidence interval, 80% power, two comparison population ratio 1:1. From the factors associated with preconception folic acid utilization, history of unsuccessful pregnancy in lifetime was one factor (p1=99% and p2=95%), based on a cross-sectional study conducted in Adama hospital medical college (Ethiopia), 36 the sample size with 10% non-response rate was 733.
Sampling techniques
First of all, six districts were selected from a total of 15 districts (Mettu, Alle, Becho, Bure, Hurumu, and Yayo districts). Ten health centers were selected using a simple random sampling technique from the selected districts, such as Tulube HC, Kemise HC, Gore HC, Hurumu HC, Yayo HC, Senbo HC, Becho HC, Leka HC, Bure HC, and Sibo HC. Additionally, one hospital was selected (Metu Karl Comprehensive Specialized Hospital). Then, the sample size was allocated proportionally to each facility based on their pregnant women flow on the ANC ward. The study participants were selected through a systematic random sampling method using a Kth interval, K = N/n, where N = the total average number of new pregnant women attending antenatal care per study period (two months) in the selected health facilities. MKCSH (306/149= 2.053), Tulube HC (120/58= 2.069), Kemise HC (95/46=2.065), Gore HC (132/64= 2.063), Hurumu HC (107/52= 2.058), Yayo HC (145/70= 2.071), Senbo HC (115/56= 2.054), Becho HC (120/58= 2.069), Leka HC (103/50= 2.06), Bure HC (142/69= 2.059), and Sibo HC (125/61= 2.049). It was approximately 2. Women were interviewed every other woman. The first woman was selected by the lottery method. After this, the sample was allocated proportionally. Data collectors then selected the first pregnant woman in the ANC unit according to the order of their cards and interviewed every other woman (skipping one woman) until the ward closed.
Data collection tools and procedures
The questionnaire was constructed from different literature sources in line with the objectives of this study.22,25,36,37,40,41 Items were primarily adapted from validated instruments used in prior studies and modified for the context of the study population. The questionnaire included socio-demographic characteristics, obstetric factors, knowledge, and practice related to folic acid. Ten BSc midwives collected the data under the supervision of two supervisors. Data were collected through a semi-structured face-to-face interviewer-administered questionnaire. The questionnaire was prepared in English and translated to two languages, such as Oromic and Amharic, by language experts. After taking informed consent, the participant was interviewed in the waiting area before entering the ANC unit. The women take their informed consent based on their preferred language.
Data quality assurance techniques
Two-day training was given to the data collectors and supervisors to familiarize them with the tools and procedures. A pretest was conducted on 37 (5%) of women two weeks before the actual data collection period in the nearby Bedelle hospital to identify the clarity of questions, the sequence of questionnaires, and gaps in data collection. Following the pretest analysis, the questionnaire items were reordered, and content modifications were made to improve fluency and facilitate easier data entry. The coefficient of reliability, Cronbach’s alpha, was calculated, resulting in 0.784. To enhance recall accuracy of interviews on folic acid utilization, data collectors employed several standardized strategies like visual aid of folic acid tablets and probing. Moreover, the English version of the questionnaire was translated into Amharic and Oromic languages and then back to English by two language experts. Daily supervision was implemented to verify data completeness and consistency throughout the study period. Data completeness was checked daily by the supervisor and principal investigator.
Variable
Operational and term definitions
Ethics and consent information
The research proposal was reviewed and approved by the Research and Ethics Review Committees of the midwifery department at Mattu University, bearing the reference number MDD/373/2024. A letter of permission was obtained from the Illuababor Department of Health. Participants received a brief overview of the study’s benefits and risks, followed by an opportunity to ask questions. Prior to data collection, the interviewer read the consent form aloud to each participant, addressed their questions, and confirmed full comprehension before proceeding. Once participants agreed to join, the interviewer documented (coded) their consent, including the date and time, on their behalf. All participants provided written informed consent prior to study enrollment. Participants’ autonomy to participate or withdraw at any time during the interview was fully respected. No minor participants were participated in this study. Confidentiality of information was obtained from the study participant and assured by all data collectors and the principal investigators. Personal identifiers were not included in the written questionnaires to ensure participants’ confidentiality.
Statistical analysis
After data collection, the data were checked for completeness, edited, coded, and entered into EPI Data version 3.1 and exported to Statistical Package of Social Sciences (SPSS) version 25 for analysis. Multicollinearity among variables was assessed using variance inflation factor (VIF) values. The VIF across all predictors was ranged from 1.07 to 9.15, with an overall mean VIF of 2.58. The logistic regression method was used. In the bivariate analysis, variables with a p-value < 0.25 were selected as candidates for multivariable analysis. Then, multivariable analysis was done to determine the presence of a statistically significant association between explanatory variables and the outcome variable (FA utilization). A p-value less than 0.05 and an OR with 95% CI were used to measure the presence and degree of association between independent and outcome variables, respectively. Descriptive statistics, such as tables with frequencies, percentages, and odds ratios, as well as text and graphs, were computed to describe the study population in relation to relevant variables.
Results
Socio-demographic characteristics
Sociodemographic characteristics of women who attend antenatal care units of Illuababor Zone public health facilities, 2024.
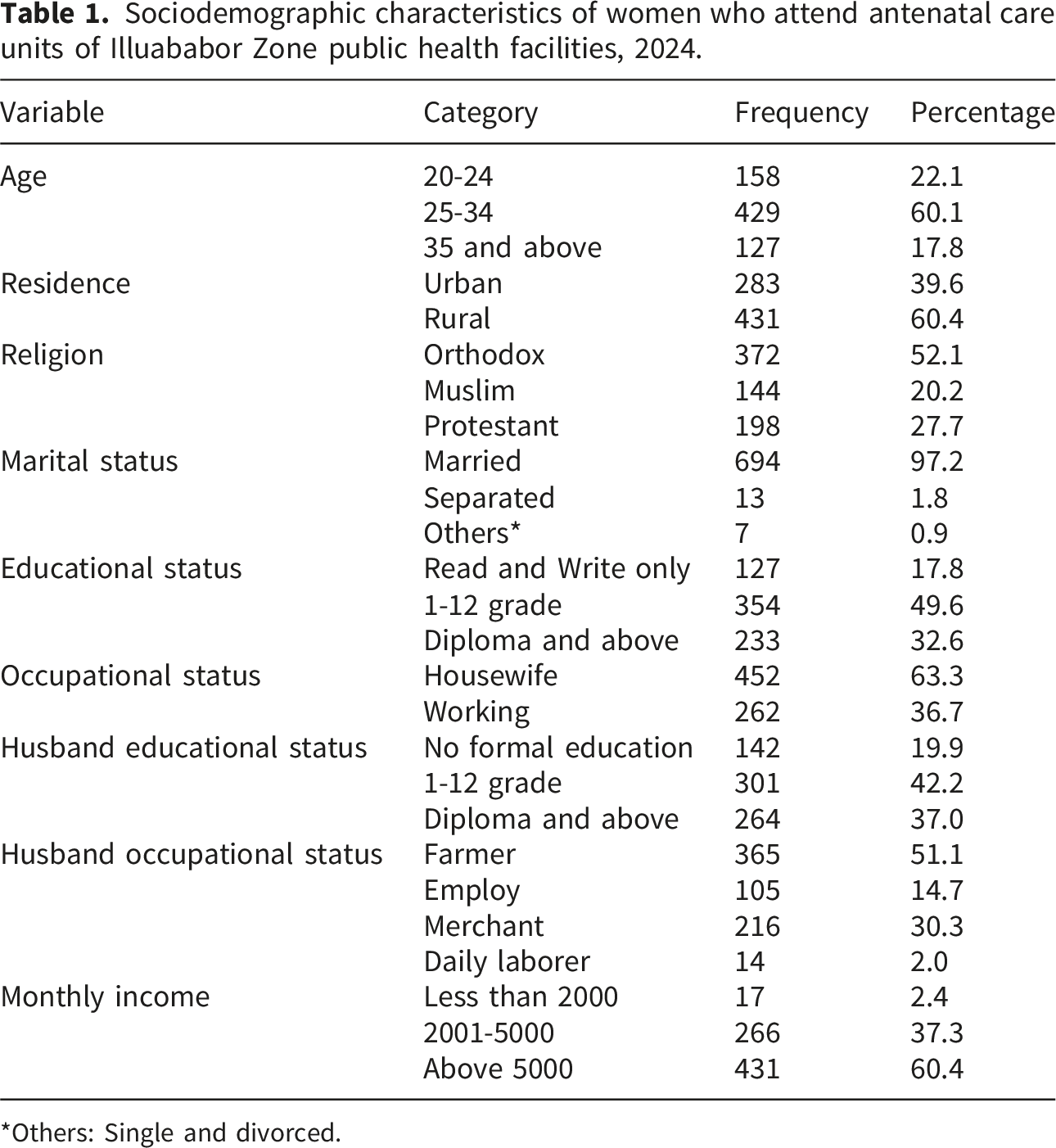
*Others: Single and divorced.
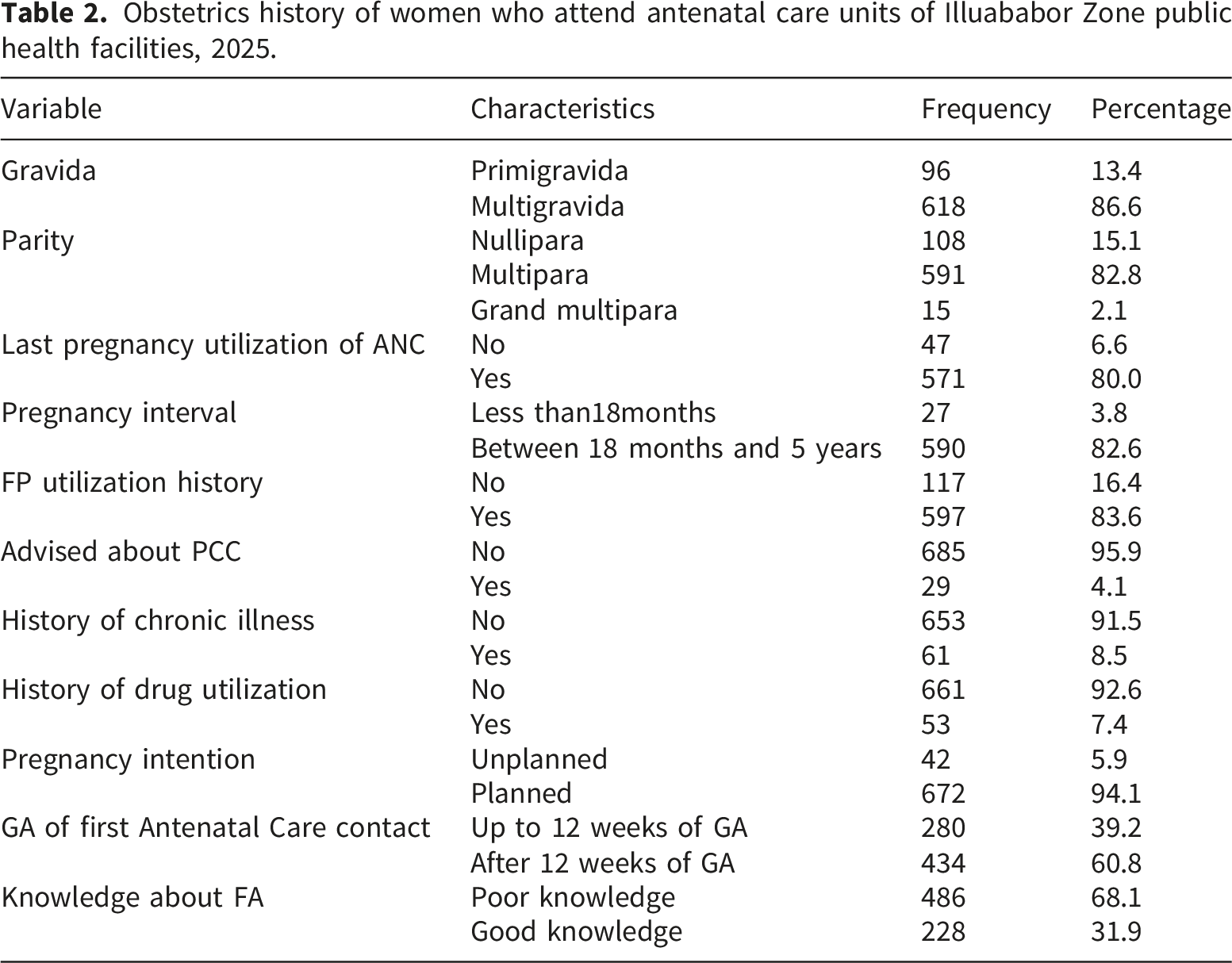
Reproductive and obstetrics history
Obstetrics history of women who attend antenatal care units of Illuababor Zone public health facilities, 2025.
Preconception folic acid utilization
From the 714 participants, only 119 (17%), [95% CI: (14.0, 19.6)] of women supplemented folic acid during the protective period.
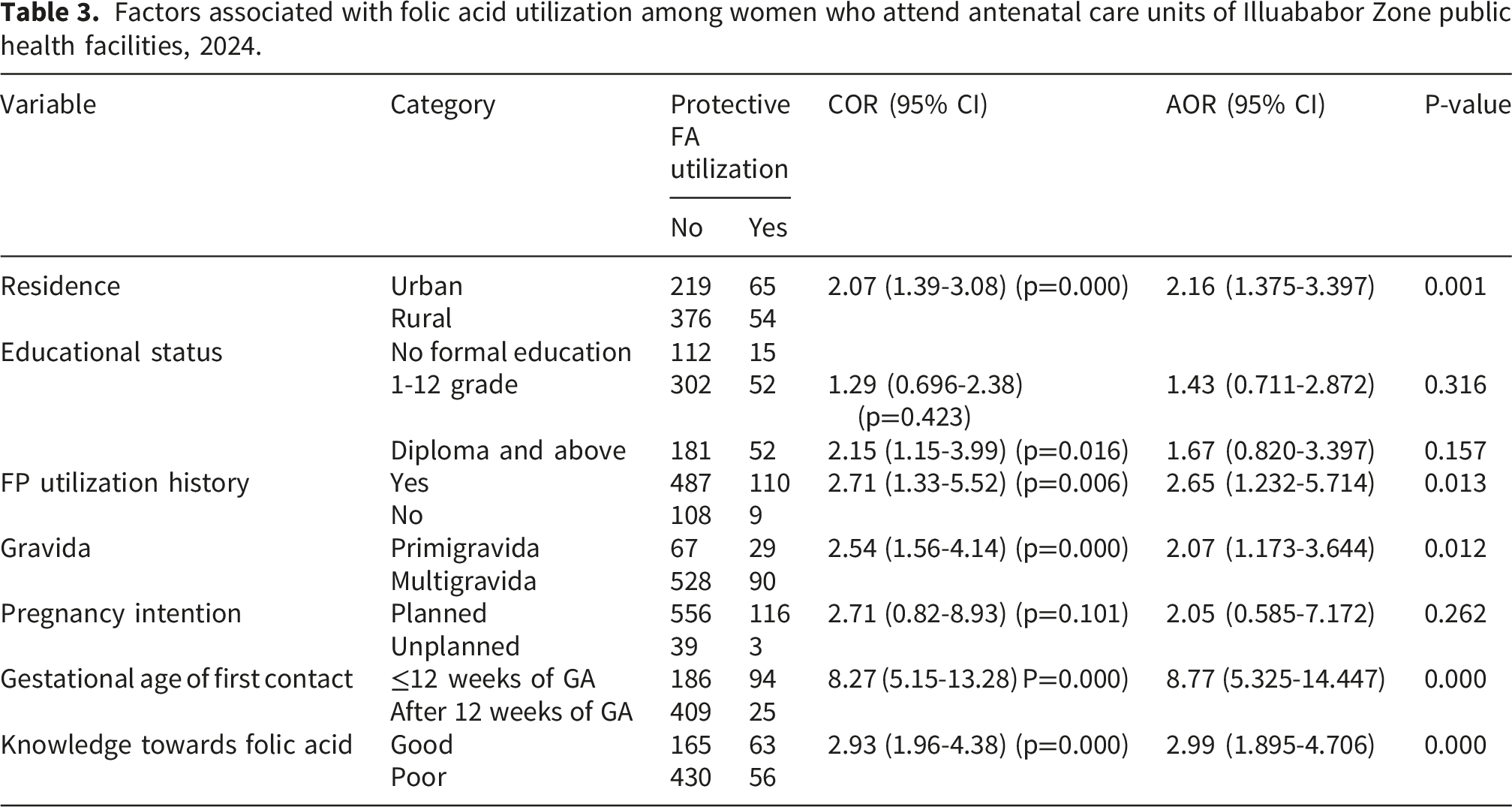
Associated variables of protective folic acid utilization
In the bivariable logistic regression analysis, seven variables such as residence, educational status, history of FP utilization, gravida, pregnancy intention, gestational age of first contact, and knowledge towards folic acid were selected for multivariable analysis with p-values of less than 0.25.
Factors associated with folic acid utilization among women who attend antenatal care units of Illuababor Zone public health facilities, 2024.
Discussion
Ethiopia’s National Preconception Care Guideline (2024) explicitly promotes folic acid supplementation at 400μg daily (combined with iron) during preconception and during early pregnancy for all reproductive-age women, with 5 mg doses for those with adverse pregnancy outcome histories. 19 However, studies reveal stark implementation gaps, with preconception folic acid utilization as low.36,37 The findings from this study reveal a notably low utilization of folic acid during the protective period, with only 119 (17%) of women reporting use. This low uptake is concerning, given the well-established benefits of folic acid supplementation in preventing neural tube defects and other adverse pregnancy outcomes when taken before conception and during early pregnancy. This result is higher than the findings of a previous study conducted in Ethiopia, which was 1.92% in Adama, 36 11.4% in Addis Ababa 42 and 14.1% of the pooled prevalence of the systematic review result in Sub-Saharan Africa. 5 The reason will be the time difference and the updating of different recommendations. Additionally, our study differs from the Addis Ababa in terms of utilization period. Our study included utilization of a protective period in both the preconception and early pregnancy, whereas the Addis Ababa study focused solely on the preconception period. As a result, its findings are possibly less comprehensive than those of our study. It is consistent with a cross-sectional study conducted in Egypt, in which 18.8% of women utilized it in the protective period. 43
This study finding is lower than a cross-sectional study conducted in eastern Sudan, which revealed that protective folic acid utilization was 58.8%. 44 And also less than other findings in Cameron, 45 Ireland, 46 Lebanon, 47 the Netherlands, 22 and China. 48 The possible reasons will be differences in awareness and accessibility of folic acid supplementation programs, variations in healthcare infrastructure, and differences in local health policies targeting women. Most of the time, possible differences across the countries will be differences in supplementation due to requirement; it may not be required in developed countries, as their diets are rich in FA sources.
Residence was significantly associated with protective period FA utilization. Women residing in urban areas were more than twice as likely to use folic acid in the protective period compared to those in rural areas. The possible reason is that urban areas have better access to health information, access to media and health facilities, more frequent contact with healthcare providers, and greater availability of supplements compared to those in rural settings.
History of family planning utilization was a strong and significant predictor. Women who had previously used FP methods were 2.65 times more expected to utilize protective period FA compared to those who had no FP utilization history. The possible reason will be that those women who utilized FP may be more knowledgeable about reproductive health, have greater exposure to health information, and have a higher tendency to seek care and advice from providers during the protective period.
Gravidity was also significantly associated with protective folic acid utilization. Primigravida women had twice the odds of protective period FA use compared to multigravida women. It is similar to a case-control study conducted in Southern Ethiopia; primigravida mothers had 4.67 times higher odds of good compliance with iron-folic acid supplementation (IFAS) compared to multigravida. 42 The possible reason is that first-time pregnancies often involve higher compliance due to greater caution and engagement with health services. Primigravida are younger and more educated than those old women and tend to have better knowledge of preconception FA recommendations from recent education or counseling.49,50
Gestational age at first booking for antenatal care showed the strongest association with protective period FA use. Women who initiated antenatal care at or before 12 weeks of gestation were nearly nine times more potential to use folic acid than those starting later. This is consistent with the results of a study conducted in Adama, Ethiopia. 36 The best reason for encouraging women to start antenatal care (ANC) before 12 weeks of gestation is the opportunity for targeted health interventions during early visits. The first trimester is a protective period and the optimal time for folic acid supplementation. Women who attend during this window have a good chance to receive folic acid timely, whereas those who start in the second or third trimester have missed the protective period.
Knowledge about folic acid significantly increased the odds of protective utilization. Women with good knowledge about FA were about three times more to be expected to use it than women with poor knowledge, underscoring the importance of health education. This is consistent with the results of a study conducted in Adama, Ethiopia 36 and Addis Ababa. 42 Possible reasons for this finding include that increased knowledge about folic acid enhances awareness of its benefits, motivates preventive behaviour, reduces misconceptions, and empowers women to adopt recommended supplementation practices.
Conclusions and recommendations
The protective period utilization of folic acid in the study area is only one-sixth. Although this rate is higher than previous Ethiopian studies, it is still considerably lower than rates reported in a number of other countries. This study showed that there are critical gaps in protective period folic acid utilization among women attending public health facilities in the Illuababor zone. This low uptake limits prevention of neural tube defects and other adverse outcomes. Women residing in urban areas, those with an FP utilization history, primigravidas, those who booked their ANC contacts in the first trimester of pregnancy, and those with good knowledge of folic acid were positive predictors for the utilization of folic acid. Hence, we recommend enhanced awareness and educational interventions, particularly focusing on rural women and multigravida groups. Strengthening family planning services and early initiation of ANC booking will have synergistic opportunities to promote folic acid utilization among women. Therefore, initiatives with awareness creation should focus on rural and multiparous women to address barriers to protective folic acid use.
Strengths and limitations of the study
Strengths
This study addresses a significant public health issue by assessing protective folic acid utilization among pregnant women, focusing on a population in a low-resource setting. Including both hospitals and health centers, especially in rural settings, ensures that the research captures the unique challenges and realities faced in underserved and remote areas. Furthermore, incorporating a relatively larger sample size, the study enhances the reliability and generalization of its findings.
Limitations
The study is limited by its focus only on public healthcare facilities, which may reduce the generalization of the findings to private ones. The exclusion of women not attending antenatal care services could result in the under-representation of vulnerable groups. Since this study assesses retrospectively, it will be affected by recall bias. Due to the cross-sectional design in nature, it is difficult to make causal inferences. Additionally, we didn’t address supply and health facility-related variables.
Supplemental material
Supplemental material - Folic acid utilization and associated factors among pregnant women who attended public health facilities of illuababor zone, Southwest Ethiopia
Supplemental material for Folic acid utilization and associated factors among pregnant women who attended public health facilities of illuababor zone, Southwest Ethiopia by Getu Amsalu Erqu, Kalkidan Alemnew, Agerie Mengistie Zeleke, Solomon Seyife Alemu, Hulubante Bizuayew Fetene, Worku Getachew Dessie and Roda Mehadi Ibrahim in Women's Health.
Footnotes
Acknowledgments
The authors would like to thank the department of midwifery at Mattu university for reviewing and approving this research. We also extend our gratitude to the Illuababor Zone health department, the data collectors, and the study participants for their invaluable cooperation and contributions to this study.
Ethical considerations
The research proposal was reviewed and approved by the Research and Ethics Review Committees of the midwifery department at Mattu University, bearing the reference number MDD/373/2024. A letter of permission was obtained from the Illuababor Department of Health.
Consent to participate
All participants gave their written informed consent to participate in this study.
Consent for publication
In this study, no individual person’s privacy, photographs, or videos are used.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors will provide access to the raw data underlying the findings of this article upon request, without unnecessary restrictions.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.