
Abstract
Objectives
Deep brain stimulation (DBS) is a well-established treatment for Parkinson’s disease (PD). Despite its proven efficacy, women are less likely to receive DBS. This study examined sex differences across the multistage clinical pathway to identify stage-specific factors contributing to disparities in utilization.
Design
Retrospective cohort study using longitudinal clinical data from a single, high-volume neurological care center.
Methods
Data were drawn from 4,308 patients with PD treated between 2012 and 2024. Progression through the DBS pathway was modeled as four conditional stages: (S1) referral, (S2) multidisciplinary evaluation among those referred, (S3) recommendation among those evaluated, and (S4) DBS surgery among those recommended. Stage-specific Firth penalized logistic regression models were used to estimate sex differences while adjusting for demographic and clinical characteristics, including age, race, comorbidities, marital status, levodopa use, and tremor status. Sex-by-predictor interactions were assessed to identify differential effects across stages.
Results
Among the cohort (2,866 males, 1,442 females), 186 (4.3%) received a referral for evaluation; 180 (97%) received an evaluation; and 159 (88%) received DBS. Adjusting only for sex, compared to males, females were less likely to be referred (OR=0.97, CI=0.71, 1.32), evaluated given referral (OR=0.88, CI=0.1, 5.17), and receive DBS given recommendation (OR=0.61, CI=0.17, 2.38), but more likely to receive a recommendation after evaluation (OR = 1.55, CI = 0.59–4.70). Sex-Predictors odds ratios differed [male- S1: age (OR=0.95, CI=0.93, 0.97), comorbidities (OR=1.19, CI=1.00, 1.41); S2: comorbidities (OR=0.51, CI=0.20, 0.87); S3: age (OR=0.91, CI=0.84, 0.97), non-white (OR=0.29, CI=0.09, 0.88), comorbidities (OR=1.90, CI=1.09, 3.73); S4: non-white (OR=0.15, CI=0.02, 0.91); [females- S1: unmarried (OR=0.71, CI=0.38, 0.92); S2: levodopa (OR=1.24, CI=1.06, 1.90); S3: non-white (OR=0.01, CI=0.00, 0.31); S4: tremors (OR=1.55, CI=1.04, 1.87)].
Conclusion
Stage-specific regression showed that differential characteristics were associated with sex disparities in DBS utilization, highlighting potential targets for equity interventions.
Plain language summary
Parkinson’s disease (PD) is a condition that affects movement and can make everyday activities difficult. For some people, a treatment called deep brain stimulation (DBS) can greatly improve symptoms when medications no longer provide symptom relief. DBS is a type of brain surgery that helps control movement problems such as tremors and stiffness. Even though DBS is effective, women are less likely than men to undergo this treatment. This study examined why sex differences DBS receipt occur by analyzing data from over 4,000 patients with PD who received care at a specialized neurological center. Following patients through four key steps: being referred for DBS, completing a detailed evaluation, being recommended for surgery, and ultimately receiving the procedure. This analysis showed that differences between men and women occured at multiple points along this pathway. For example, women were less likely to be referred for evaluation, and social factors such as marital status appeared to play a role. At later stages, clinical factors such as medication use and symptom type influenced whether patients moved forward with surgery, and these factors affected men and women differently. Overall, these findings suggest that unequal access to DBS is not caused by a single issue but instead resulted from a combination of social, clinical, and healthcare system factors. Understanding where these differences occur can help doctors and health systems design targeted strategies to ensure that all patients who could benefit from DBS have an equal opportunity to receive it.
Keywords
Introduction
Deep brain stimulation (DBS) is a well-established treatment for individuals with Parkinson’s disease (PD) who experience disabling motor complications despite optimized dopaminergic therapy. 1 Randomized trials demonstrate that DBS improves motor function and quality of life compared to the best medical therapy. 2 Despite its proven efficacy, DBS remains underutilized and unevenly accessed. 3 Although PD is more prevalent among men than women, women remain disproportionately underrepresented among patients receiving DBS, even among insured cohorts 4 —a disparity that persists even after accounting for underlying differences in disease prevalence, suggesting that factors beyond epidemiology contribute to inequities in access to advanced therapies.
Proposed contributors include differences in referral patterns, counseling practices, patient preferences, and system-level access. 5 Studies show that women are underrepresented at the referral stage, even though they are more likely candidates for the surgery. 6 Contributing factors to the sex disparities include: a) later in the disease course and later selection for surgery, 7 b) differential patterns of non-motor symptoms, 8 c) greater risk of developing treatment-related complications, 9 d) less support during decision-making, 10 e) less confident in selecting treatments, 11 and f) more significant caregiving duties, greater competing demands, and less social support. 12 There is also evidence of sex-related personal preferences that impact DBS likelihood. 3 However, studies cannot localize where inequities arise along the clinical pathway (e.g., referral, evaluation, recommendation, or scheduling for surgery). Understanding the specific processes and decisions that contribute to these differences is important, given observed sex differences in post-surgical outcomes—women having less support after surgery, 10 greater post-surgical anxiety, 12 and experiencing greater distress from changes in intimate relationships. 13
The process from receiving DBS for PD has four stages (Figure 1). Clinical pathway for patients undergoing deep brain stimulation (DBS) evaluation for Parkinson's disease. The sequential process includes referral, multidisciplinary evaluation, recommendation and surgical approval, and DBS surgery. This framework guided the sequential pathway analysis of sex differences in progression through each stage of the DBS care continuum.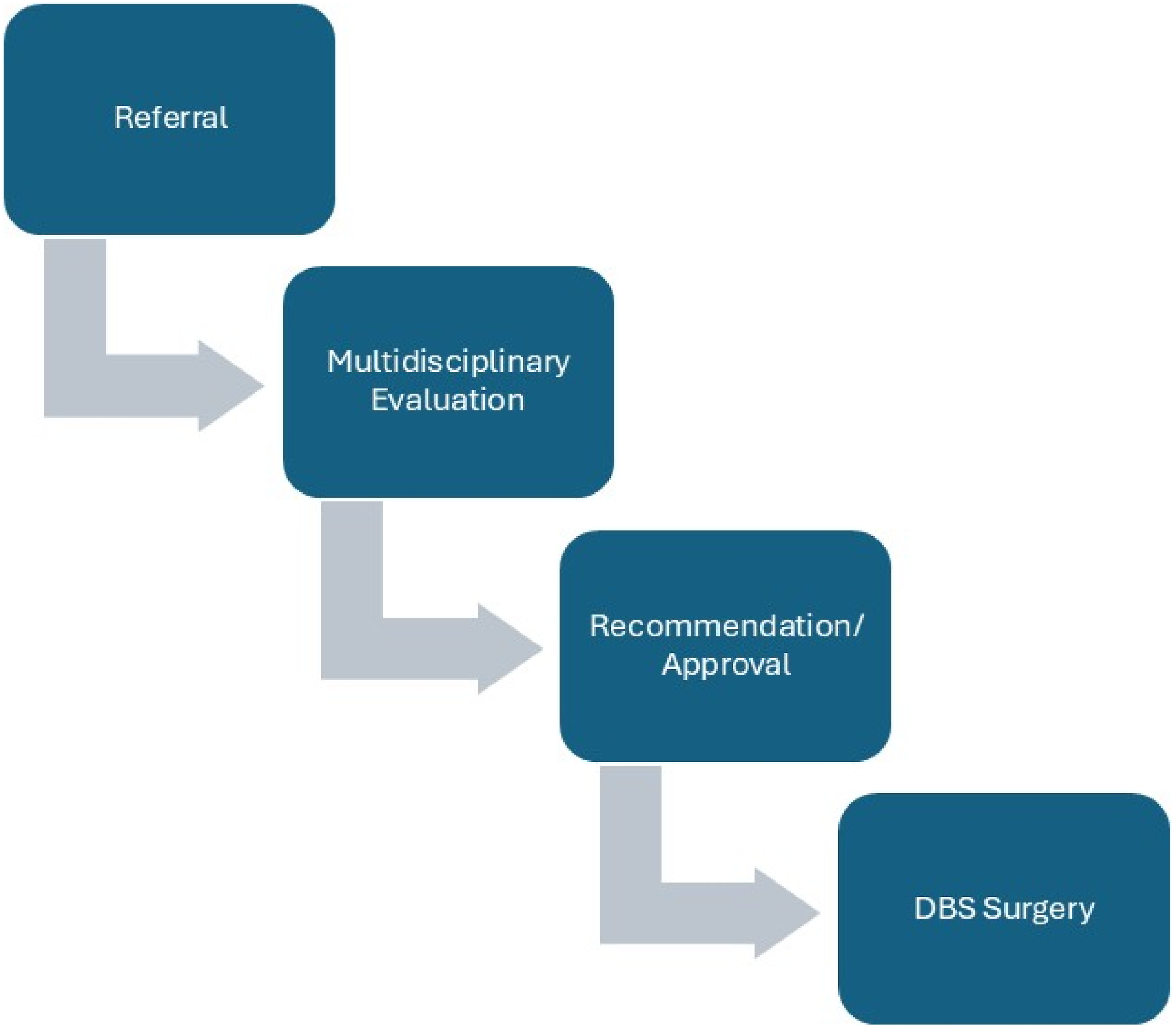
Stage 1: Referral
Patients with idiopathic, levodopa-responsive PD with optimized medication are typically referred for DBS consultation when they develop one or more of the following: troublesome motor fluctuations, levodopa-induced dyskinesias, or medication-refractory tremors.
Stage 2: Multidisciplinary evaluation
A multidisciplinary assessment is conducted, including a neuropsychological evaluation and a review of brain imaging to confirm suitability for electrode placement. Physical, occupational, and speech evaluations assess the patient’s mobility, balance, communication, airway protection (swallowing), and function. Their insights help predict the likelihood of patient recovery and benefit from DBS. A social worker assesses the patient’s support system, access to care, and capacity to attend the multiple postoperative appointments necessary to optimize stimulator settings and identify potential obstacles that could affect long-term outcomes.
Stage 3: Recommendation
A patient is ultimately approved/recommended for DBS for PD after 1) evaluation confirms they meet clinical and functional criteria, 2) they agree to cooperate during the procedure and follow-up, and 3) have a reliable support system. 14 Institutions performing DBS must have experienced neurosurgeons, appropriate imaging and surgical equipment, and a team trained in movement disorders.
Stage 4: Receipt
Patients who ultimately receive DBS are those with idiopathic PD who experience significant motor complications—such as dyskinesias, tremor, or motor fluctuations—that are inadequately controlled by medication. A robust and sustained levodopa response is the most consistent predictor of favorable DBS outcomes, and many centers require a formal levodopa challenge test to confirm this responsiveness. 15 Ideal candidates are typically younger than 70, healthy, have minimal cognitive impairment, and present stable psychiatric health.
This process involves multiple levels of influence by both individuals with PD and their providers that potentially contribute to observed sex differences in DBS surgery. To explore this multi-stage process, data from a large single-center cohort of patients traversing a standardized, multidisciplinary DBS pathway at a multidisciplinary, neurological care institute between 2012 and 2024 were analyzed to estimate sex differences in the conditional likelihood of progression to each stage—referral, evaluation, recommendation, and receipt—adjusting for clinical and demographic heterogeneity.
Methods
Data
This study utilized information collected in the INFORM (INstitute FOR Neurological diseases) research database, a longitudinal, clinical research database housing data on nearly 20,000 patients—maintained by the Norman Fixel Institute for Neurological Diseases (Fixel Institute) at the University of Florida (UF) Health in Gainesville, Florida. The Fixel Institute—a recognized Parkinson’s Foundation Center of Excellence—is an interdisciplinary hub offering diagnosis, advanced treatment, education, and research, providing neurology, neurosurgery, neuropsychology, psychiatry, rehabilitative therapies, genetics counseling, nutrition, and support services.
The INFORM database includes over 7,500 patients diagnosed with idiopathic PD, 2,000 with dystonia, and more with other movement disorders. Patients who attend at least one medical appointment may join the database, thereby allowing their information to be used for research purposes. The database captures standardized clinical assessments encompassing motor function, mood, cognition, medication history, and neurosurgical interventions, including DBS, referral status, pre-surgical evaluations, approval decisions, and surgical outcomes, as well as device programming and follow-up assessments.
Sample
These criterion results in 4,310 unique patients. Patient information included age, sex, race, insurance, marital status, comorbidities, and PD duration, type, and medication. Clinical PD treatment information included whether the patient was referred for multi-disciplinary evaluation, counseled for DBS surgery, received multidisciplinary evaluation, recommended for DBS, approved for DBS, or received DBS. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Sample size justification
Because this was a retrospective study using an existing clinical database, no formal a priori sample size calculation was performed. Instead, the analytic sample included all eligible unique patients with PD seen at the Fixel Institute between February 2012 and February 2024 who met study inclusion criteria. This yielded a total sample of 4,308 individuals. To ensure stable estimation in the stage-specific logistic regression models, the number of predictors included at each stage was limited according to an events-per-parameter (EPV) rule targeting approximately 10 events per parameter, an approach commonly used to support reliable inference in logistic regression with relatively rare outcomes. Given 186 referral events in Stage 1 and progressively smaller risk sets in subsequent stages, this approach provided the basis for determining the feasible complexity of the models and justified the use of the full available cohort.
Characteristics
Characteristics were chosen a priori from available factors: age, marital status, idiopathic PD, insurance status, sex, problematic tremors, levodopa use, comorbidity burden, and race/ethnicity. To improve numerical stability, continuous predictors were standardized (z-scored) within stage to reduce collinearity and scaling issues16,17 and categorical predictors with fewer than five observations were collapsed. Only type 1 diabetes mellitus (DMT1), type 2 diabetes mellitus (DMT2), hypertension, stroke, cardiovascular disease (CVD), cancer (non-skin), and respiratory disease comorbidities were available. Therefore, the comorbidity burden represented the sum of the number of these diagnoses reported by the patient. Patients without any of these diagnoses were assigned a value of 0. Each stage used complete-case analysis for the variables included in that stage’s model.
DBS pathways
Progression along the sequential DBS pathways was represented as binary stages: (S1) referral for DBS; (S2) receipt of a multidisciplinary evaluation among those referred; (S3) recommendation for DBS among those evaluated; and (S4) receipt of DBS among those recommended. Since the probability of advancing to each stage was conditional on success at the previous stage, each stage was modeled using stage-specific logistic regression. Since stages S2 through S4 were imbalanced (very few non-advancers), the predictors per stage were limited using an events-per-parameter (EPV) rule (targeting EPV=10)—a standard shown in prior work to yield stable estimates. 18
Analytic framework and statistical analysis
The pathway was represented as four sequential stage-specific logistic regressions—(S1): referral for DBS, (S2): receipt of a multidisciplinary evaluation among those referred, (S3): recommendation for DBS among those evaluated, and (S4): receipt of DBS among those approved. To address low cell counts and differential success rates between men and women, a penalized likelihood (Firth) logistic regression was used as the default estimator, with predefined fallbacks described below. For each stage s∈{1,…,4}, Ys denotes the binary outcome for the risk set eligible for stage s. The model included sex, all main effects for the characteristics (X), and sex-by-predictor interactions (see Equation (1)).

Since full interaction blocks can be non-estimable when events are rare, a two-step procedure was used. In Stage 1, each predictor Xi, was checked to see whether its effect differed between men and women, using a method that handles rare events (Firth regression). A simple, or ‘Base’, model (Equation (2a)) was fit that included sex and one factor at a time. Next, a more detailed ‘Interaction’ (Equation (2b)) model was tested, which allowed the factor’s effect to differ by sex.
Stage 1: One-at-a-time interaction scan


After both the Stage 1 base and interaction models converged via Firth regression, a penalized likelihood ratio test (PLRT) was performed to evaluate whether the extra interaction terms improved model fit. If the one-at-a-time interaction was non-estimable by Firth, a mean bias-reduced logistic regression was conducted, and a Wald block test was performed on the vector of interaction coefficients. Predictors with estimable interactions using either method were ‘accepted.’
Stage 2: Reduced form full interaction model
Using the full set of ‘accepted’ predictors from Stage 1, Stage 2 estimated a reduced-form interaction model that included sex, main effects for the candidate predictors, and ‘accepted’ sex-by-predictor interactions of the form in Equation (3).

If the penalized fit failed, mean-bias-reduced estimation was used. Sex-specific odds ratios (ORs) and associated 95% confidence intervals (CIs) were reported. Odds ratios (ORs) for continuous variables are reported per 1 SD increase.
19
For predictors that did not interact with sex in the reduced model, the coefficients applied equally to both sexes. For predictors with sex interactions, let
Because several stage-specific risk sets were small and imbalanced, safeguards were implemented to obtain valid estimates despite sparse cells. First, Firth’s penalized likelihood logistic regression was used as the default estimator. Firth’s correction reduces small-sample bias and is robust when standard maximum likelihood. 20 To improve stability, the number of iterations was increased to 1,000, and the maximum step size was decreased to 0.2. If Firth’s regression failed to converge, the model was respecified as a mean-bias-reduced logistic regression to obtain consistent estimates. This fallback was automatic, ensuring that differences in estimates reflected the fitting method rather than covariate adjustments. Penalized estimation and bias-reduced fallback, combined with principled level consolidation, within-stage predictor standardization, and disclosure of risk-set sizes. All analyses were conducted in R 21 using these packages: logistf 22 for Firth penalized logistic regression, brglm2 23 for mean bias-reduced logistic regression, and tidyverse 24 for data consolidation and output.
Robustness and sensitivity analyses
Three additional analyses were performed to evaluate the robustness of the results. First, sex-stratified Firth logistic models were fit to ensure that removing non-estimable interactions did not mask clinically relevant differences. These models provided sex-specific ORs that did not rely on any explicit interaction terms and corroborated the direction and approximate magnitude of the effects observed in the pooled reduced-interaction analysis. Second, the estimation was repeated using mean-bias-reduced logistic regression as the primary estimation method to validate the approach. Finally, the EPV cap was lowered to five to test the sensitivity to this limitation.
This study has been approved by the University of Florida Institutional Review Board (#IRB202300118).
Results
Sample characteristics
Sample size and characteristics by sex, stage.

S1: All.
S2: Referred=1|S1.
S3: Counsel/Multidisciplinary Evaluation=1|S2.
S4: Received/Approved=1|S3.
As seen in Table 1, among males, the mean age decreased from 74.4 (SD=10.21) years in the full cohort (S1, N=2,866) to 68.83 (SD=9.51) at referral (S2, N=125), 68.57 (SD=9.48) at evaluation (S3, N=121), and 67.72 (SD=9.24) at surgery/approval (S4, N=105). Average comorbidity burden rose from 0.26 (SD=0.79) at S1 to 1.86 (SD=1.19) at S2, 1.82 (SD=1.14) at S3, and 1.89 (SD=1.17) at S4. Tremor documentation was rare at baseline (0.2%) and remained uncommon (≈1%) in later stages. Nearly all men had idiopathic PD throughout (≥99.9%). The proportion married was consistently high, increasing slightly from 68.9% (S1) to 73.1% (S4). Lack of insurance was uncommon overall (0.6% at S1) but somewhat higher among those referred/evaluated (∼3% at S2–S4). Levodopa use increased dramatically from 12.9% at baseline to about 91% among referred/evaluated groups, remaining stable thereafter. The share classified as non-White fell sharply from 89.3% at S1 to 26–27% at S2–S3 and 23.8% at S4.
Among females, mean age decreased from 74.52 (SD=10.15) years at S1 (N=1,442) to 70.44 (SD=8.54) at S2 (N=61), 70.05 (SD=8.39) at S3 (N=59), and 69.76 (SD=8.39) at S4 (N=54). Comorbidities rose from 0.27 (SD=0.79) at S1 to 1.51 (SD=0.96) at S2, 1.54 (SD=0.95) at S3, and 1.59 (SD=0.96) at S4. Tremor documentation was rare but slightly more frequent than in males at later stages (≈1.6–1.9%). Idiopathic PD remained nearly universal (≥98–100%). Marriage rates were lower than in males at baseline (61.3%) but converged across stages (70.4% at S4). Uninsured status was uncommon (0.6% at S1) and modestly higher among referred/evaluated (∼3–4%). Levodopa use showed the same step-up pattern (from 13.9% at S1 to ∼85% at S2–S4). As with males, the proportion of non-White decreased with progression (from 89.3% at S1 to ∼28% at S2–S3 and 22.2% at S4).
Sex-only adjusted model
Sex-adjusted penalized likelihood model estimation.
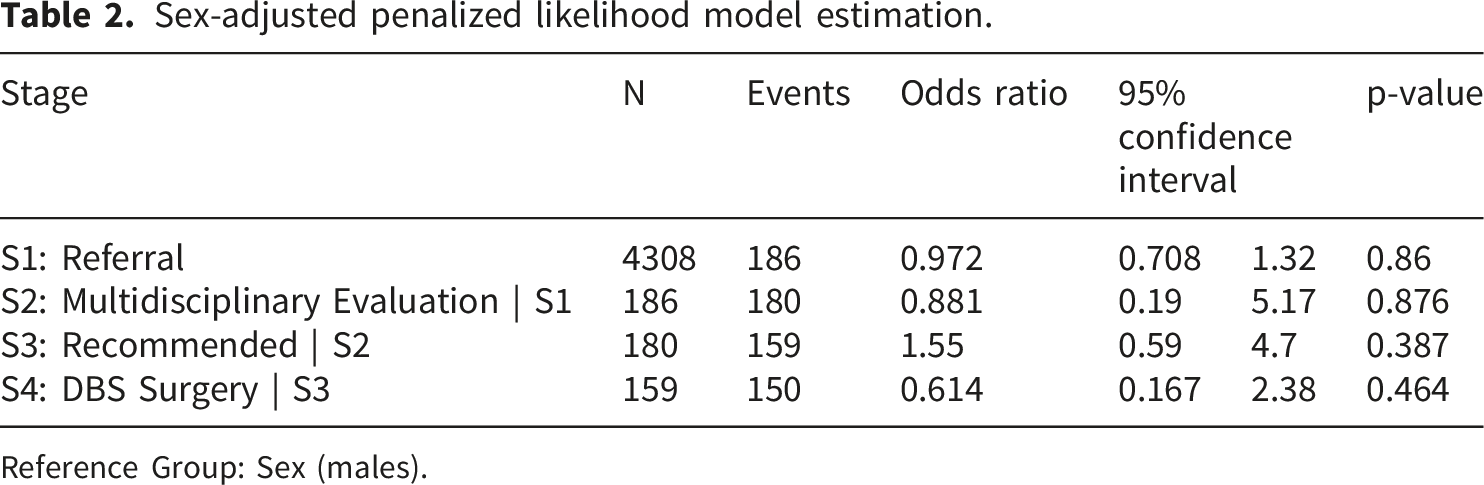
Reference Group: Sex (males).
Fully adjusted model
Adjusted penalized likelihood model estimation.
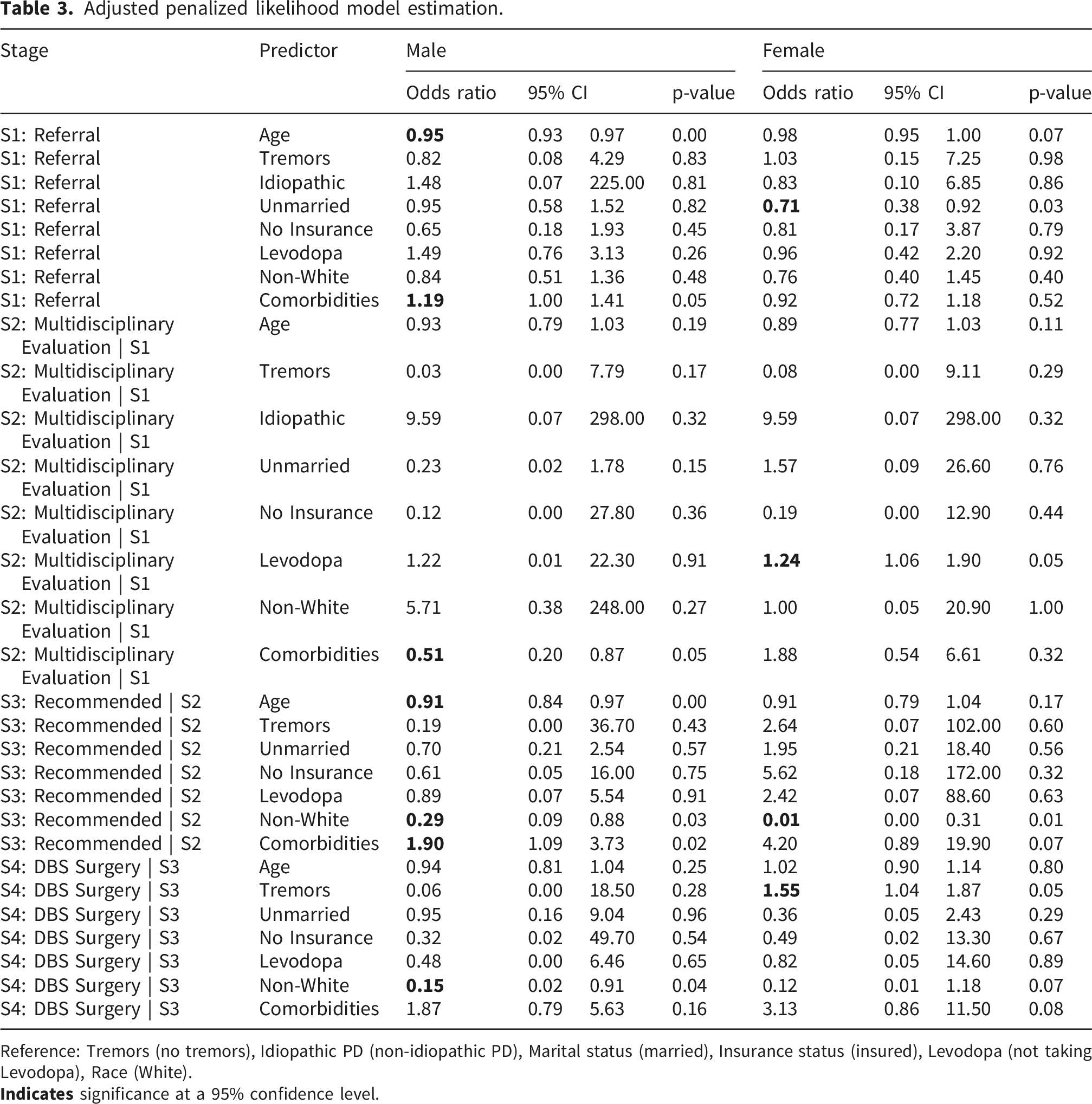
Reference: Tremors (no tremors), Idiopathic PD (non-idiopathic PD), Marital status (married), Insurance status (insured), Levodopa (not taking Levodopa), Race (White).
(S2) In men, more comorbidities predicted lower odds of completing evaluation (OR = 0.51, CI=0.20, 0.87, p=0.05). In women, levodopa therapy was associated with higher odds of evaluation (OR = 1.24, CI=1.06, 1.90, p=0.05). All other effects were imprecise with wide CIs at this stage.
(S3) For men, older age again predicted lower odds of recommendation (OR = 0.91, CI=0.84, 0.97, p<0.01), non-White race predicted lower odds (OR = 0.29, CI=0.09, 0.88, p=0.03), and comorbidities predicted higher odds (OR = 1.90, CI=1.09, 3.73, p=0.02). For women, non-White race was strongly associated with lower odds of recommendation (OR = 0.01, CI=0.01, 0.31, p=0.01); other predictors were not significant.
(S4) Among men, non-White race was associated with lower odds of surgery (OR = 0.15, CI=0.02, 0.91, p=0.04). Among women, tremor predicted higher odds of proceeding to surgery (OR = 1.55, CI=1.04, 1.87, p=0.05). Other effects at S4 were not statistically significant.
Robustness and sensitivity analyses
Appendix Table 1 presents the results of the sex-stratified first logistic regression models. (S1) Among men, older age was linked to lower odds of referral (OR = 0.95, CI=0.93, 0.97, p<0.001); higher comorbidity burden showed a borderline increase in referral (OR = 1.19, CI=1.00, 1.41, p=0.05). Among women, age was also inversely associated with referral (OR = 0.97, CI=0.94, 0.99, p=0.02). In addition, being unmarried was associated with lower referral odds (OR = 0.27, 0.13–0.55, p<0.001), while levodopa therapy was strongly associated with higher referral odds (OR = 13.60, CI=5.33, 36.91, p<0.001). (S2) Among men, comorbidities predicted lower odds of completing evaluation (OR = 0.51, CI=0.20, 0.91, p=0.05). In women, levodopa was associated with higher odds of evaluation (OR = 2.43, CI=2.20, 2.52, p=0.05). (S3) For men, older age again reduced the odds of recommendation (OR = 0.91, CI=0.84, 0.97, p<0.01), non-White race was associated with lower odds (OR = 0.29, CI=0.09, 0.88, p=0.03), and comorbidities increased the odds (OR = 1.90, CI=1.09, 3.73, p=0.02). For women, non-White race showed a marked reduction in recommendation (OR = 0.02, CI=0.01, 0.25, p<0.001). (S4) Among men, non-White race remained associated with lower odds of surgery (OR = 0.15, CI=0.02, 0.91, p=0.04). Among women, tremor predicted higher odds of proceeding to surgery (OR = 1.11, CI=1.01, 1.21, p=0.05), and non-White race again indicated lower odds (OR = 0.09, CI=0.02, 0.13, p=0.05).
Appendix Table 2 presents the results of the sensitivity analysis, using mean-bias-reduced logistic regression as the primary estimation method. (S1) Among men, higher age was associated with lower odds of referral (OR = 0.95, CI=0.93, 0.97, p<0.001). Greater comorbidity burden showed a small, borderline increase in referral likelihood (OR = 1.19, CI=1.00, 1.41, p=0.05). (S2) In men, higher comorbidity burden was associated with lower odds of advancing to evaluation (OR = 0.51, CI=0.25, 1.00, p=0.05). In women, no predictors were significant. (S3) For men, older age again predicted lower odds of recommendation (OR = 0.91, CI=0.86, 0.97, p=0.01). Non-White men were less likely to be recommended (OR = 0.29, CI=0.10, 0.85, p=0.02), whereas greater comorbidity burden increased the odds (OR = 1.90, CI=1.07, 3.38, p=0.03). For women, race was strongly associated with recommendation; Non-White women had markedly lower odds (OR = 0.01, CI=0.00, 0.31, p=0.01). (S4) Among men, Non-White race remained associated with lower odds of receiving DBS (OR = 0.15, CI=0.03, 0.76, p=0.02). Among women, no predictors were statistically significant.
Appendix Table 3 presents the results of the final sensitivity analysis, in which the EPV was set to 5. These results differ little from those presented above.
Discussion
This study showed that women were less likely to be referred, evaluated, and, once referred, to receive DBS, even when it had been recommended. While the lower likelihood of receiving DBS among women may reflect the higher prevalence of PD among men, the persistence of differences across stages of the DBS pathway suggests that disparities in access are not solely attributable to underlying epidemiology. Baseline disease prevalence imbalance should be considered when interpreting the magnitude and generalizability of sex-specific findings, as well as those of other studies that also demonstrate sex disparities in DBS utilization.6,7,9,11,25
The observed male predominance in the analytic sample reflects the established higher prevalence of Parkinson’s disease among men and is consistent with prior epidemiologic studies. While this imbalance may influence the absolute number of individuals progressing through each stage of the DBS pathway, the analytic approach used in this study models conditional progression at each stage, thereby evaluating relative likelihoods of advancement rather than absolute counts. As such, the findings are less likely to be driven by differences in baseline sex distribution alone. Nevertheless, the smaller number of women, particularly in later stages with limited risk sets, may contribute to reduced statistical precision and wider confidence intervals for female-specific estimates. This should be considered when interpreting sex-stratified results, and future studies with larger and more balanced samples are warranted to confirm these findings.
The findings of this study align with a growing body of literature documenting persistent sex disparities in DBS utilization for Parkinson’s disease. Multiple studies have shown that women are consistently underrepresented among DBS recipients, comprising only 23–30% of surgical cases despite representing a substantially larger proportion of the PD population.10,26 Importantly, this disparity is not fully explained by differences in disease prevalence or clinical eligibility, as women demonstrate comparable, and in some cases greater, post-surgical benefit relative to men. 3 Prior research suggests that disparities emerge at multiple points in the care pathway, including lower referral rates, differences in patient decision-making, and structural barriers to access.3,9 For example, women have been shown to be less likely to be referred for DBS evaluation and more likely to decline surgery due to concerns about risks, caregiving responsibilities, and the need for social support.27,28 Additionally, differences in symptom presentation and disease progression have been proposed as contributing factors, although the evidence suggests they do not fully account for the observed disparities.3,29 The current study extends this literature by demonstrating that these disparities are not attributable to a single decision point but instead reflect distinct, stage-specific barriers that differentially affect men and women across the DBS pathway. It also indicated that women are more likely than men to receive a DBS recommendation. DBS referral is a complex process influenced by both clinical and non-clinical factors. Candidacy may include good, future, or poor candidates due to neurological or medical contraindications. 10 Prior work indicates a lack of consensus among physicians regarding disease duration and timing of DBS referral, which may influence referral decisions. 30
Physician hesitancy or misalignment with referral guidelines can affect both the likelihood and timing of referral discussions. Cabrera et al. 30 found that many neurologists lacked strict criteria for treatment response before referral, leading to variation in clinical judgment. Referral patterns also differed by specialty: movement disorder specialists were less likely than neurologists to refer patients without levodopa responsiveness or with severe cognitive impairment, consistent with multidisciplinary consensus. Approximately 20% of respondents believed DBS deserved consideration only after exhausting all medication options, and most viewed DBS within 1–2 years of diagnosis as premature. 30
Referral decisions also involve shared decision-making with patients whose beliefs and attitudes influence outcomes. One study identified three patient approaches: taking initiative, agreeing when offered, or hesitating. 31 Men were more likely to take the initiative or agree when offered, whereas women were more likely to express fear of complications or to consult friends and family before deciding. 31
Additional studies support the existence of sex differences in decision-making. Fullard et al. found differences in information needs, support, and risk–benefit assessment. 10 Women valued peer discussions with women who had undergone DBS, whereas men prioritized numerical information and expressed fewer concerns about support. Limited access to female peers may contribute to differential referral rates during early shared decision-making.
By isolating progression at each stage, our findings provide a more granular understanding of how previously documented disparities arise, offering a framework for identifying targeted intervention points within the DBS care continuum. Further research implementing mixed-methods approaches could identify intervention points to reduce disparities and better understand sex-specific decision-making. Such work should also account for predictors identified in this study, including comorbidities, age, race, marital status, levodopa use, and tremor status. Age-related considerations should distinguish biological from chronological age, alongside disease severity and duration at referral. 32 Additionally, hormonal influences deserve consideration, given their influence on higher rates of disability among women, such as osteoporosis, 11 and how that might affect perceptions of DBS candidacy.
Limitations
Seven methodological and conceptual limitations should merit consideration when interpreting these findings. First, although the INFORM database offers detailed, prospectively collected information on patients progressing through the DBS pathway, it represents a single, high-volume tertiary center in Florida; therefore, findings may not generalize to other institutions with different referral networks, demographic compositions, or multidisciplinary workflows. Second, the database does not capture several clinical indicators that may influence candidacy—such as disease severity, motor fluctuation profiles, neuropsychological test scores, symptom duration, or levodopa challenge responses—limiting the study’s ability to account for all relevant determinants of referral, evaluation, and surgical recommendation. Third, the operationalization of “race” as White versus non-White and reliance on a limited set of comorbidities restricts the conceptual richness of social and clinical heterogeneity that may shape DBS decision-making; similarly, unmeasured psychosocial factors (e.g., caregiving burden, treatment preferences, social support) that are known to differ by sex could not be evaluated. Fourth, this study was conducted at a single, high-volume tertiary care center with a standardized, multidisciplinary DBS pathway, which may limit the generalizability of findings to other clinical settings with differing referral patterns, patient populations, and care structures. Future multicenter studies applying similar stage-specific analytical approaches across diverse institutions are needed to validate these findings and enhance their external validity, potentially advancing understanding of disparities in DBS access. Fifth, although the sequential logistic modeling strategy allows for stage-specific estimation, the small risk sets at later stages yielded sparse data structures, necessitating the use of penalized likelihood (Firth) and mean-bias-reduced logistic regression. Sixth, while these approaches mitigate separation and small-sample bias, they result in wide confidence intervals, reduced statistical power, and limited precision for subgroup effects and interaction terms. Finally, the conditional modeling framework assumes measured and appropriately specified confounders at each stage; if unobserved factors influence both advancement through the pathway and sex differences in care, residual confounding may persist. Together, these limitations suggest caution when interpreting stage-specific estimates and highlight the need for multicenter, mixed-methods research that incorporates richer clinical, psychosocial, and structural determinants of DBS access.
Conclusions
In this single-center cohort study, a thorough, stage-specific analytical framework identified where sex differences emerge along the DBS care pathway. Although sex disparities in DBS persisted, findings showed that the factors influencing progression differ significantly by sex across decision points, indicating that these differences arise from multiple, stage-specific barriers. Findings demonstrated that sex disparities in DBS utilization arose from distinct, stage-specific barriers across the care pathway. Women faced reduced likelihood of referral associated with social factors such as marital status, while clinical indicators like levodopa use and tremor influenced later-stage progression differently by sex. Additionally, non-White race was a significant barrier at the recommendation stage, particularly among women. Together, these findings highlighted that disparities were driven by a combination of social support constraints, differential clinical presentation and evaluation, and structural inequities in decision-making, underscoring the need for targeted, stage-specific interventions to improve equitable access to DBS.
Footnotes
Ethical considerations
This study was approved by the University of Florida Institutional Review Board (IRB #IRB202300118). The study utilized data from the INFORM (Integrated Neurological Focus on Outcomes and Research Metadata) database, an IRB-approved clinical research repository at the Norman Fixel Institute for Neurological Diseases (UF Health). All data were derived from patient electronic health records and were analyzed in accordance with applicable ethical guidelines and regulations.
Consent to participate
Given the retrospective nature of the study and the use of de-identified data, the requirement for informed consent was waived by the Institutional Review Board.
Consent for publication
Not applicable. This study used de-identified data from an institutional research database and does not include any individual person’s identifiable information.
Author contributions
MJ: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Data curation, Writing- original draft, Writing-reviewing and editing, Funding acquisition. KH: Writing- original draft, Writing-reviewing and editing, Funding acquisition. NH: Writing- Reviewing and Editing. QF: Writing- Reviewing and Editing. CE: Conceptualization, Writing- Original Draft, Writing- Reviewing and Editing, Funding acquisition
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the American Parkinson’s Disease Foundation Diversity in Parkinson’s disease Research Grant [# AGR DTD, 7-12-2023].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study were obtained from the INFORM (Integrated Neurological Focus on Outcomes and Research Metadata) database at the Norman Fixel Institute for Neurological Diseases, University of Florida (UF Health). INFORM is an institutional, IRB-approved research repository that captures longitudinal clinical data on over 20,000 patients with movement and related neurological disorders. Because these data are derived from patient electronic health records and contain sensitive, personally identifiable health information, they are subject to strict privacy protections under institutional review board (IRB) policies and applicable regulations. As a result, the raw data is not publicly available. Access to the INFORM database is available to authorized faculty and trainees affiliated with the University of Florida or to investigators through approved collaborations who meet institutional and regulatory requirements. Researchers interested in accessing the data for replication or related studies may contact the Norman Fixel Institute for Neurological Diseases to inquire about data access procedures, subject to IRB approval and data use agreements.
Appendix
Sex-stratified firth logistic model estimation. Reference: Tremors (no tremors), Idiopathic PD (non-idiopathic PD), Marital status (married), Insurance status (insured), Levodopa (not taking Levodopa), Race (White).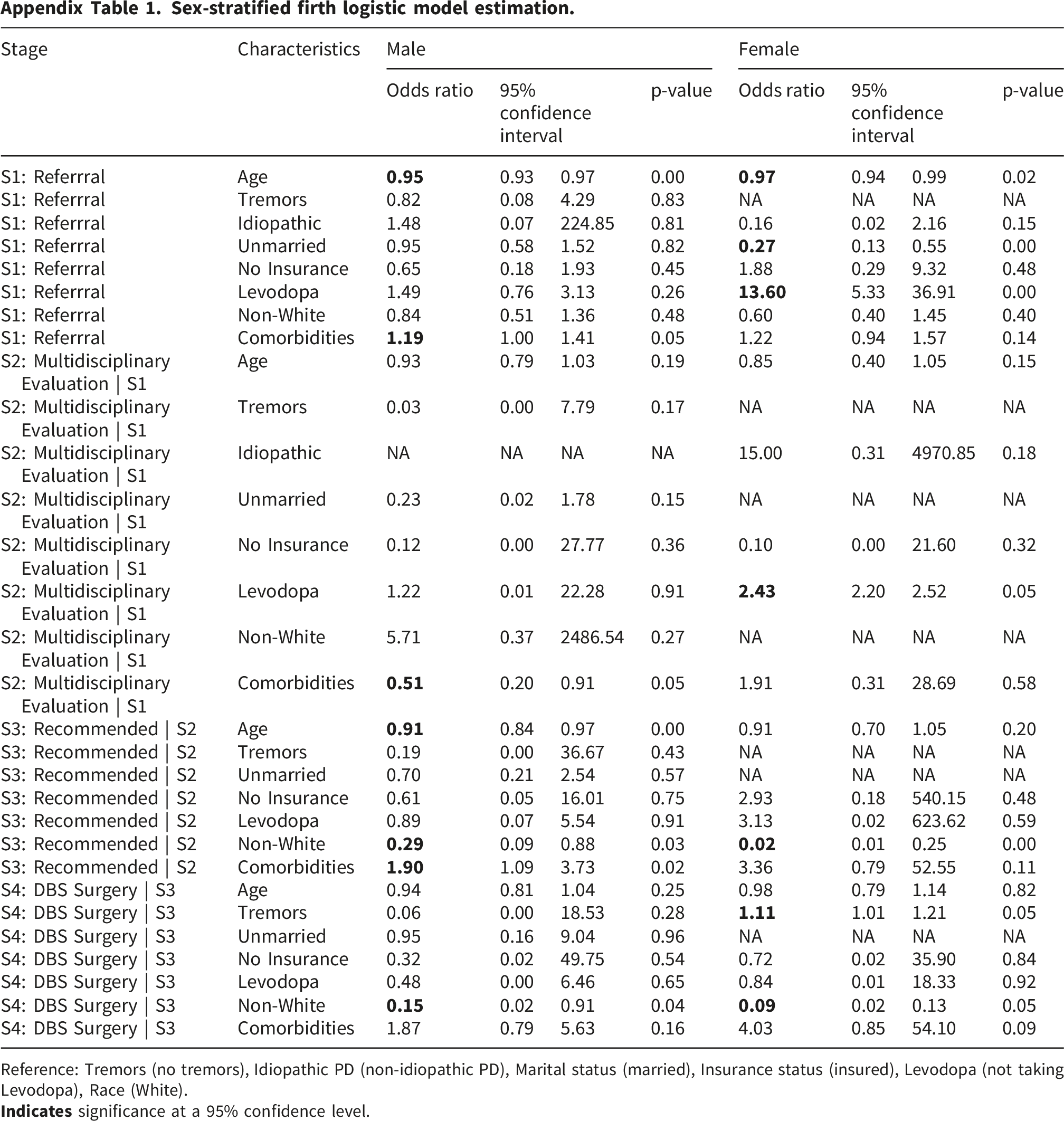
Stage
Characteristics
Male
Female
Odds ratio
95% confidence interval
p-value
Odds ratio
95% confidence interval
p-value
S1: Referrral
Age
0.93
0.97
0.00
0.94
0.99
0.02
S1: Referrral
Tremors
0.82
0.08
4.29
0.83
NA
NA
NA
NA
S1: Referrral
Idiopathic
1.48
0.07
224.85
0.81
0.16
0.02
2.16
0.15
S1: Referrral
Unmarried
0.95
0.58
1.52
0.82
0.13
0.55
0.00
S1: Referrral
No Insurance
0.65
0.18
1.93
0.45
1.88
0.29
9.32
0.48
S1: Referrral
Levodopa
1.49
0.76
3.13
0.26
5.33
36.91
0.00
S1: Referrral
Non-White
0.84
0.51
1.36
0.48
0.60
0.40
1.45
0.40
S1: Referrral
Comorbidities
1.00
1.41
0.05
1.22
0.94
1.57
0.14
S2: Multidisciplinary Evaluation | S1
Age
0.93
0.79
1.03
0.19
0.85
0.40
1.05
0.15
S2: Multidisciplinary Evaluation | S1
Tremors
0.03
0.00
7.79
0.17
NA
NA
NA
NA
S2: Multidisciplinary Evaluation | S1
Idiopathic
NA
NA
NA
NA
15.00
0.31
4970.85
0.18
S2: Multidisciplinary Evaluation | S1
Unmarried
0.23
0.02
1.78
0.15
NA
NA
NA
NA
S2: Multidisciplinary Evaluation | S1
No Insurance
0.12
0.00
27.77
0.36
0.10
0.00
21.60
0.32
S2: Multidisciplinary Evaluation | S1
Levodopa
1.22
0.01
22.28
0.91
2.20
2.52
0.05
S2: Multidisciplinary Evaluation | S1
Non-White
5.71
0.37
2486.54
0.27
NA
NA
NA
NA
S2: Multidisciplinary Evaluation | S1
Comorbidities
0.20
0.91
0.05
1.91
0.31
28.69
0.58
S3: Recommended | S2
Age
0.84
0.97
0.00
0.91
0.70
1.05
0.20
S3: Recommended | S2
Tremors
0.19
0.00
36.67
0.43
NA
NA
NA
NA
S3: Recommended | S2
Unmarried
0.70
0.21
2.54
0.57
NA
NA
NA
NA
S3: Recommended | S2
No Insurance
0.61
0.05
16.01
0.75
2.93
0.18
540.15
0.48
S3: Recommended | S2
Levodopa
0.89
0.07
5.54
0.91
3.13
0.02
623.62
0.59
S3: Recommended | S2
Non-White
0.09
0.88
0.03
0.01
0.25
0.00
S3: Recommended | S2
Comorbidities
1.09
3.73
0.02
3.36
0.79
52.55
0.11
S4: DBS Surgery | S3
Age
0.94
0.81
1.04
0.25
0.98
0.79
1.14
0.82
S4: DBS Surgery | S3
Tremors
0.06
0.00
18.53
0.28
1.01
1.21
0.05
S4: DBS Surgery | S3
Unmarried
0.95
0.16
9.04
0.96
NA
NA
NA
NA
S4: DBS Surgery | S3
No Insurance
0.32
0.02
49.75
0.54
0.72
0.02
35.90
0.84
S4: DBS Surgery | S3
Levodopa
0.48
0.00
6.46
0.65
0.84
0.01
18.33
0.92
S4: DBS Surgery | S3
Non-White
0.02
0.91
0.04
0.02
0.13
0.05
S4: DBS Surgery | S3
Comorbidities
1.87
0.79
5.63
0.16
4.03
0.85
54.10
0.09
Mean bias-reduced logistic regression as primary estimation method. Reference: Tremors (no tremors), Idiopathic PD (non-idiopathic PD), Marital status (married), Insurance status (insured), Levodopa (not taking Levodopa), Race (White).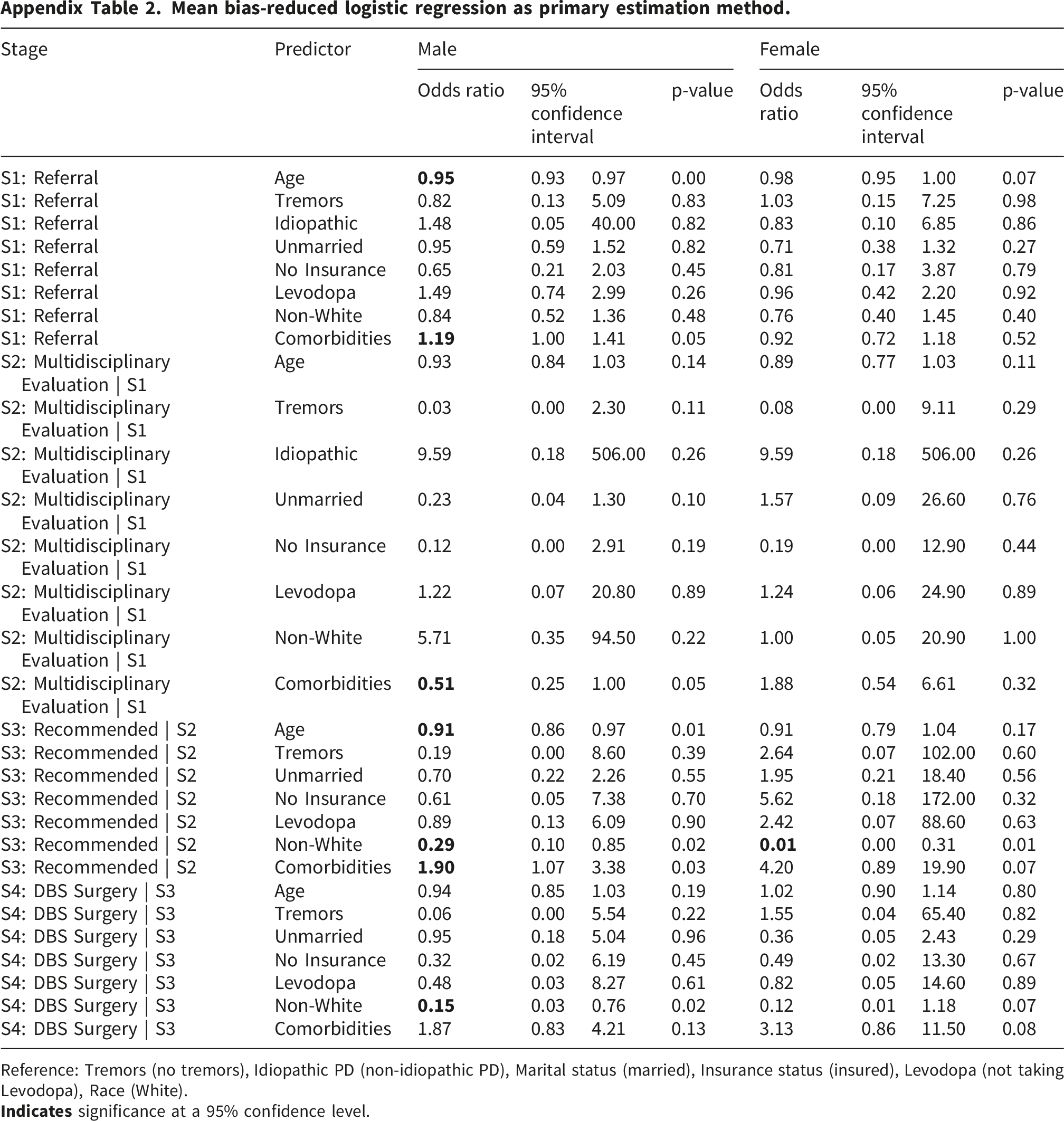
Stage
Predictor
Male
Female
Odds ratio
95% confidence interval
p-value
Odds ratio
95% confidence interval
p-value
S1: Referral
Age
0.93
0.97
0.00
0.98
0.95
1.00
0.07
S1: Referral
Tremors
0.82
0.13
5.09
0.83
1.03
0.15
7.25
0.98
S1: Referral
Idiopathic
1.48
0.05
40.00
0.82
0.83
0.10
6.85
0.86
S1: Referral
Unmarried
0.95
0.59
1.52
0.82
0.71
0.38
1.32
0.27
S1: Referral
No Insurance
0.65
0.21
2.03
0.45
0.81
0.17
3.87
0.79
S1: Referral
Levodopa
1.49
0.74
2.99
0.26
0.96
0.42
2.20
0.92
S1: Referral
Non-White
0.84
0.52
1.36
0.48
0.76
0.40
1.45
0.40
S1: Referral
Comorbidities
1.00
1.41
0.05
0.92
0.72
1.18
0.52
S2: Multidisciplinary Evaluation | S1
Age
0.93
0.84
1.03
0.14
0.89
0.77
1.03
0.11
S2: Multidisciplinary Evaluation | S1
Tremors
0.03
0.00
2.30
0.11
0.08
0.00
9.11
0.29
S2: Multidisciplinary Evaluation | S1
Idiopathic
9.59
0.18
506.00
0.26
9.59
0.18
506.00
0.26
S2: Multidisciplinary Evaluation | S1
Unmarried
0.23
0.04
1.30
0.10
1.57
0.09
26.60
0.76
S2: Multidisciplinary Evaluation | S1
No Insurance
0.12
0.00
2.91
0.19
0.19
0.00
12.90
0.44
S2: Multidisciplinary Evaluation | S1
Levodopa
1.22
0.07
20.80
0.89
1.24
0.06
24.90
0.89
S2: Multidisciplinary Evaluation | S1
Non-White
5.71
0.35
94.50
0.22
1.00
0.05
20.90
1.00
S2: Multidisciplinary Evaluation | S1
Comorbidities
0.25
1.00
0.05
1.88
0.54
6.61
0.32
S3: Recommended | S2
Age
0.86
0.97
0.01
0.91
0.79
1.04
0.17
S3: Recommended | S2
Tremors
0.19
0.00
8.60
0.39
2.64
0.07
102.00
0.60
S3: Recommended | S2
Unmarried
0.70
0.22
2.26
0.55
1.95
0.21
18.40
0.56
S3: Recommended | S2
No Insurance
0.61
0.05
7.38
0.70
5.62
0.18
172.00
0.32
S3: Recommended | S2
Levodopa
0.89
0.13
6.09
0.90
2.42
0.07
88.60
0.63
S3: Recommended | S2
Non-White
0.10
0.85
0.02
0.00
0.31
0.01
S3: Recommended | S2
Comorbidities
1.07
3.38
0.03
4.20
0.89
19.90
0.07
S4: DBS Surgery | S3
Age
0.94
0.85
1.03
0.19
1.02
0.90
1.14
0.80
S4: DBS Surgery | S3
Tremors
0.06
0.00
5.54
0.22
1.55
0.04
65.40
0.82
S4: DBS Surgery | S3
Unmarried
0.95
0.18
5.04
0.96
0.36
0.05
2.43
0.29
S4: DBS Surgery | S3
No Insurance
0.32
0.02
6.19
0.45
0.49
0.02
13.30
0.67
S4: DBS Surgery | S3
Levodopa
0.48
0.03
8.27
0.61
0.82
0.05
14.60
0.89
S4: DBS Surgery | S3
Non-White
0.03
0.76
0.02
0.12
0.01
1.18
0.07
S4: DBS Surgery | S3
Comorbidities
1.87
0.83
4.21
0.13
3.13
0.86
11.50
0.08
Adjusted penalized likelihood model estimation with EPV of 5. Reference: Tremors (no tremors), Idiopathic PD (non-idiopathic PD), Marital status (married), Insurance status (insured), Levodopa (not taking Levodopa), Race (White).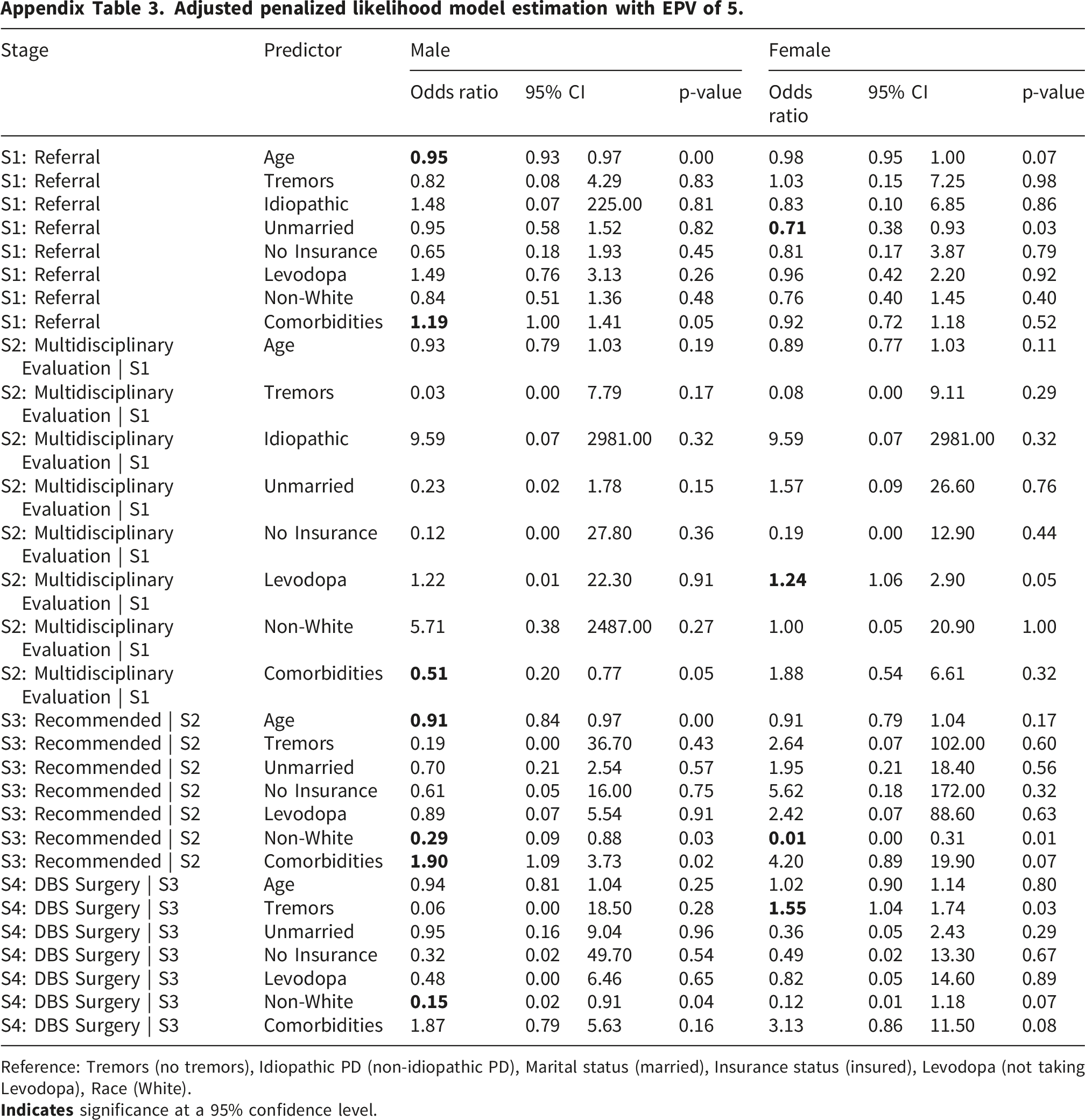
Stage
Predictor
Male
Female
Odds ratio
95% CI
p-value
Odds ratio
95% CI
p-value
S1: Referral
Age
0.93
0.97
0.00
0.98
0.95
1.00
0.07
S1: Referral
Tremors
0.82
0.08
4.29
0.83
1.03
0.15
7.25
0.98
S1: Referral
Idiopathic
1.48
0.07
225.00
0.81
0.83
0.10
6.85
0.86
S1: Referral
Unmarried
0.95
0.58
1.52
0.82
0.38
0.93
0.03
S1: Referral
No Insurance
0.65
0.18
1.93
0.45
0.81
0.17
3.87
0.79
S1: Referral
Levodopa
1.49
0.76
3.13
0.26
0.96
0.42
2.20
0.92
S1: Referral
Non-White
0.84
0.51
1.36
0.48
0.76
0.40
1.45
0.40
S1: Referral
Comorbidities
1.00
1.41
0.05
0.92
0.72
1.18
0.52
S2: Multidisciplinary Evaluation | S1
Age
0.93
0.79
1.03
0.19
0.89
0.77
1.03
0.11
S2: Multidisciplinary Evaluation | S1
Tremors
0.03
0.00
7.79
0.17
0.08
0.00
9.11
0.29
S2: Multidisciplinary Evaluation | S1
Idiopathic
9.59
0.07
2981.00
0.32
9.59
0.07
2981.00
0.32
S2: Multidisciplinary Evaluation | S1
Unmarried
0.23
0.02
1.78
0.15
1.57
0.09
26.60
0.76
S2: Multidisciplinary Evaluation | S1
No Insurance
0.12
0.00
27.80
0.36
0.19
0.00
12.90
0.44
S2: Multidisciplinary Evaluation | S1
Levodopa
1.22
0.01
22.30
0.91
1.06
2.90
0.05
S2: Multidisciplinary Evaluation | S1
Non-White
5.71
0.38
2487.00
0.27
1.00
0.05
20.90
1.00
S2: Multidisciplinary Evaluation | S1
Comorbidities
0.20
0.77
0.05
1.88
0.54
6.61
0.32
S3: Recommended | S2
Age
0.84
0.97
0.00
0.91
0.79
1.04
0.17
S3: Recommended | S2
Tremors
0.19
0.00
36.70
0.43
2.64
0.07
102.00
0.60
S3: Recommended | S2
Unmarried
0.70
0.21
2.54
0.57
1.95
0.21
18.40
0.56
S3: Recommended | S2
No Insurance
0.61
0.05
16.00
0.75
5.62
0.18
172.00
0.32
S3: Recommended | S2
Levodopa
0.89
0.07
5.54
0.91
2.42
0.07
88.60
0.63
S3: Recommended | S2
Non-White
0.09
0.88
0.03
0.00
0.31
0.01
S3: Recommended | S2
Comorbidities
1.09
3.73
0.02
4.20
0.89
19.90
0.07
S4: DBS Surgery | S3
Age
0.94
0.81
1.04
0.25
1.02
0.90
1.14
0.80
S4: DBS Surgery | S3
Tremors
0.06
0.00
18.50
0.28
1.04
1.74
0.03
S4: DBS Surgery | S3
Unmarried
0.95
0.16
9.04
0.96
0.36
0.05
2.43
0.29
S4: DBS Surgery | S3
No Insurance
0.32
0.02
49.70
0.54
0.49
0.02
13.30
0.67
S4: DBS Surgery | S3
Levodopa
0.48
0.00
6.46
0.65
0.82
0.05
14.60
0.89
S4: DBS Surgery | S3
Non-White
0.02
0.91
0.04
0.12
0.01
1.18
0.07
S4: DBS Surgery | S3
Comorbidities
1.87
0.79
5.63
0.16
3.13
0.86
11.50
0.08