
Abstract
Gestational Weight Gain (GWG) affects maternal and fetal health. Vitamin D insufficiency, common during pregnancy, may impact weight control via metabolic, inflammatory, and endocrine pathways. However, the association between maternal vitamin D and GWG remain unclear. Therefore, this narrative review’s objective is to integrate existing evidence on the correlations between maternal vitamin D and GWG, examine the effect of pre-pregnancy Body Mass Index (BMI), assess the cumulative effects of vitamin D deficiency and inadequate GWG on pregnancy outcomes, and assess the efficacy of vitamin D supplementation. A narrative review was conducted in accordance with SANRA 2.0 principles, with the search strategy reported in line with PRISMA-S guidance. A literature review was conducted in PubMed, Scopus, and Google Scholar to identify studies examining gestational weight gain (GWG) and serum 25-hydroxyvitamin D status published between January 2015 and November 2025. Observational and interventional studies were eligible for inclusion. After eliminating duplicates, reviewers independently evaluated 1,395 records; 14 studies were included. The prevalence of vitamin D deficiency and its bidirectional associations with maternal weight, gestational weight gain as a modifier of vitamin D’s metabolic effects, combined effects on fetal and offspring outcomes, and supplementation trial evidence were narratively synthesized. Vitamin D insufficiency affected 30-85% of pregnant women worldwide. Bidirectional vitamin D-GWG relationships differed among studies, with prepregnancy BMI as a substantial effect modifier. In overweight women, low first trimester vitamin D levels were associated with 3.70 kg higher total GWG. Vitamin D’s insulin resistance protection was greatly reduced by excessive GWG. High-dose supplementation (1600 IU/day) met biochemical needs but did not affect GWG. In one cohort, both low vitamin D and suboptimal GWG independently predicted small-for-gestational-age births. The association between maternal vitamin D status and gestational weight gain remains inconsistent across the current evidence base. Pre-pregnancy BMI may modify this relationship, with the strongest associations observed among overweight and obese women. Integrated strategies addressing both vitamin D adequacy and appropriate gestational weight gain, particularly among women with elevated pre-pregnancy BMI, should be explored in future research.
Plain language summary
Vitamin D supports skeletal health and also contributes to immune and metabolic function. In pregnancy, achieving recommended gestational weight gain is important because both inadequate and excessive gain are linked to adverse outcomes for mothers and infants. This narrative review summarises global evidence on whether maternal vitamin D status is associated with gestational weight gain and whether pre-pregnancy body weight influences this relationship. We searched major bibliographic databases for studies published between 2015 and 2025 that measured vitamin D during pregnancy and reported gestational weight gain. Across studies, results were inconsistent. Some reported associations between lower vitamin D status and higher or lower gestational weight gain, while others found no clear relationship. Methodological differences likely explain part of this variability, including timing of vitamin D assessment, definitions of deficiency, measurement of weight gain, and adjustment for key factors such as pre-pregnancy body mass index, season, diet, physical activity, and supplementation. Although evidence remains mixed, higher pre-pregnancy adiposity is frequently associated with lower circulating vitamin D and may also relate to a greater likelihood of non-recommended gestational weight gain and metabolic complications. These overlapping risks highlight the importance of considering baseline maternal weight status when interpreting the vitamin D and gestational weight gain literature. Overall, current evidence does not establish a consistent causal link between vitamin D status and gestational weight gain. Robust prospective studies and adequately powered trials are needed to clarify directionality and determine whether optimising vitamin D status, within comprehensive antenatal care, supports healthier gestational weight trajectories.
Keywords
Introduction
Gestational weight gain (GWG) is a critical indicator of maternal nutritional status and fetal development, reflecting the complex physiological changes necessary to support a healthy pregnancy. The Institute of Medicine (IOM) established evidence-based guidelines for optimal GWG based on prepregnancy body mass index (BMI) defining categories of GWG as inadequate, adequate, or excessive. For example, the IOM recommends 11.5-16 kg total gain for women with normal BMI prepregnancy, with adjusted ranges for underweight, overweight, or obese women. 1 Globally, suboptimal GWG has become increasingly prevalent. Recent systematic reviews indicate that excessive GWG occurs in approximately 47% of pregnancies worldwide, 2 while inadequate GWG occurs in up to 23% of pregnancies, with substantial regional variation. 2
Both inadequate and excessive GWG carry important clinical implications. Excessive GWG is associated with gestational diabetes mellitus (GDM), hypertensive disorders, cesarean delivery, postpartum weight retention, macrosomia, and increased risk of later life obesity in offspring.1,3,4 Conversely, inadequate GWG increases the risks of preterm birth, small-for-gestational-age (SGA) infants, and fetal growth restriction. 5 Given these far-reaching consequences for both maternal and child health, GWG has emerged as a globally significant indicator of pregnancy outcomes and achieving optimal weight gain represents a key public health goal in maternal fetal medicine. 2
Multiple determinants contribute to GWG variability across populations. Prepregnancy BMI remains the strongest predictor, with women who are overweight and obese more likely to exceed IOM recommendations, while underweight women are more likely to gain inadequately. 6 Dietary quality, caloric intake, and physical activity patterns also influence GWG, with energy-dense diets and sedentary lifestyles linked to excessive gains. 7 Sociodemographic factors, including maternal education, parity, and socioeconomic status, have been shown to modify GWG trajectories in diverse settings.8,9 While these traditional determinants have been well documented, emerging research suggests that micronutrient status, particularly vitamin D, may also influence maternal weight gain patterns. 10
Vitamin D has attracted increasing scientific attention due to its metabolic, inflammatory, and endocrine roles during pregnancy, as shown in Figure 1. Beyond its classical function in calcium homeostasis and bone metabolism, vitamin D plays regulatory roles in adipogenesis, insulin sensitivity, lipid metabolism, and systemic pathways closely linked to maternal fat deposition and weight regulation.
11
Biologically, vitamin D receptors are expressed in adipocytes, and the active metabolite 1,25-dihydroxyvitamin D modulates adipocyte differentiation and function. Vitamin D also influences insulin signaling, glucose metabolism, and inflammatory cytokine production, mechanisms that theoretically position it as a potential modulator of GWG. Vitamin D activation pathway during pregnancy and its proposed maternal–infant effects.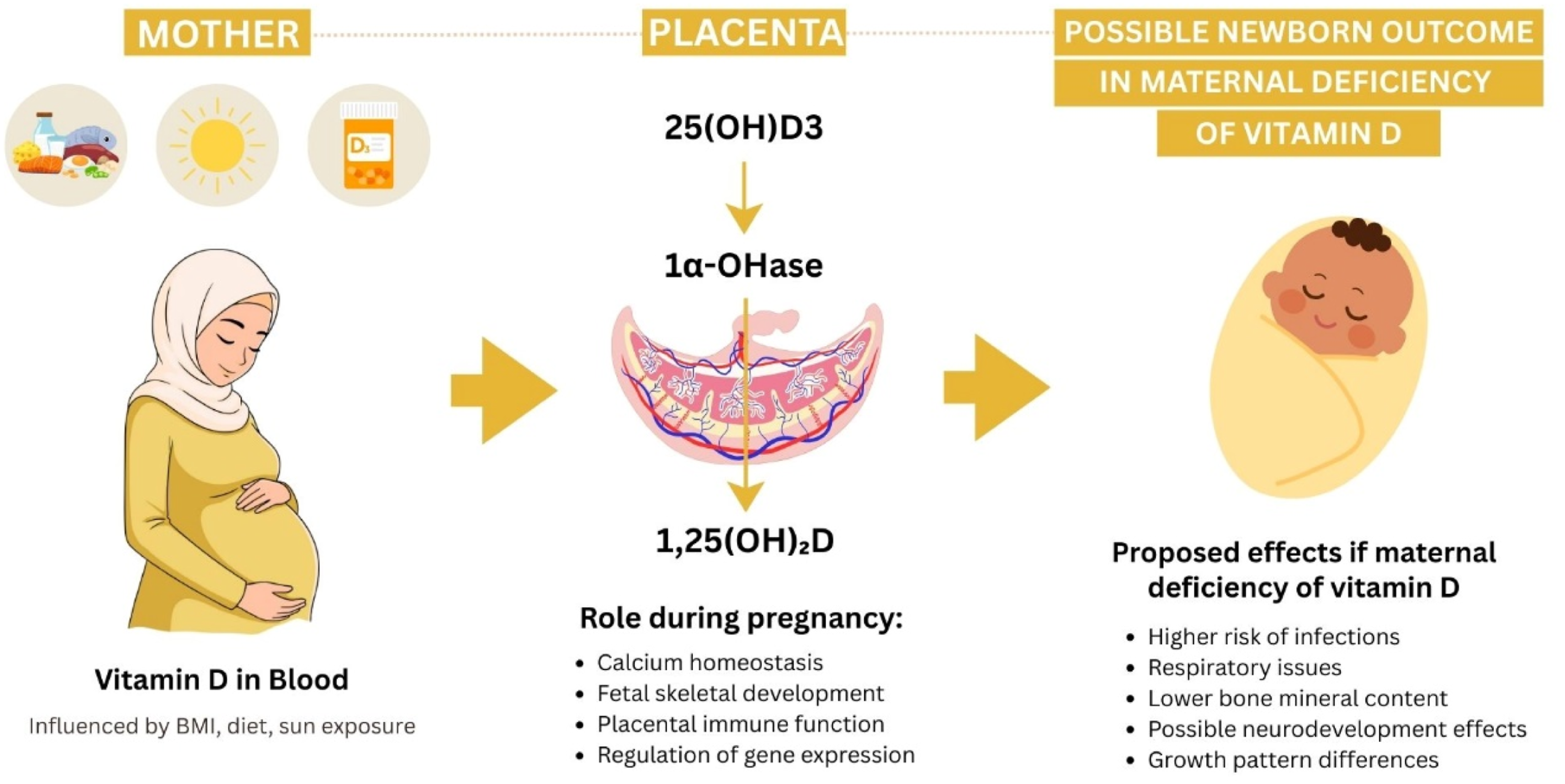
Evidently, vitamin D deficiency is highly prevalent during pregnancy and disproportionately affects women with overweight and obesity, creating a potential overlap with risk factors for excessive GWG.
12
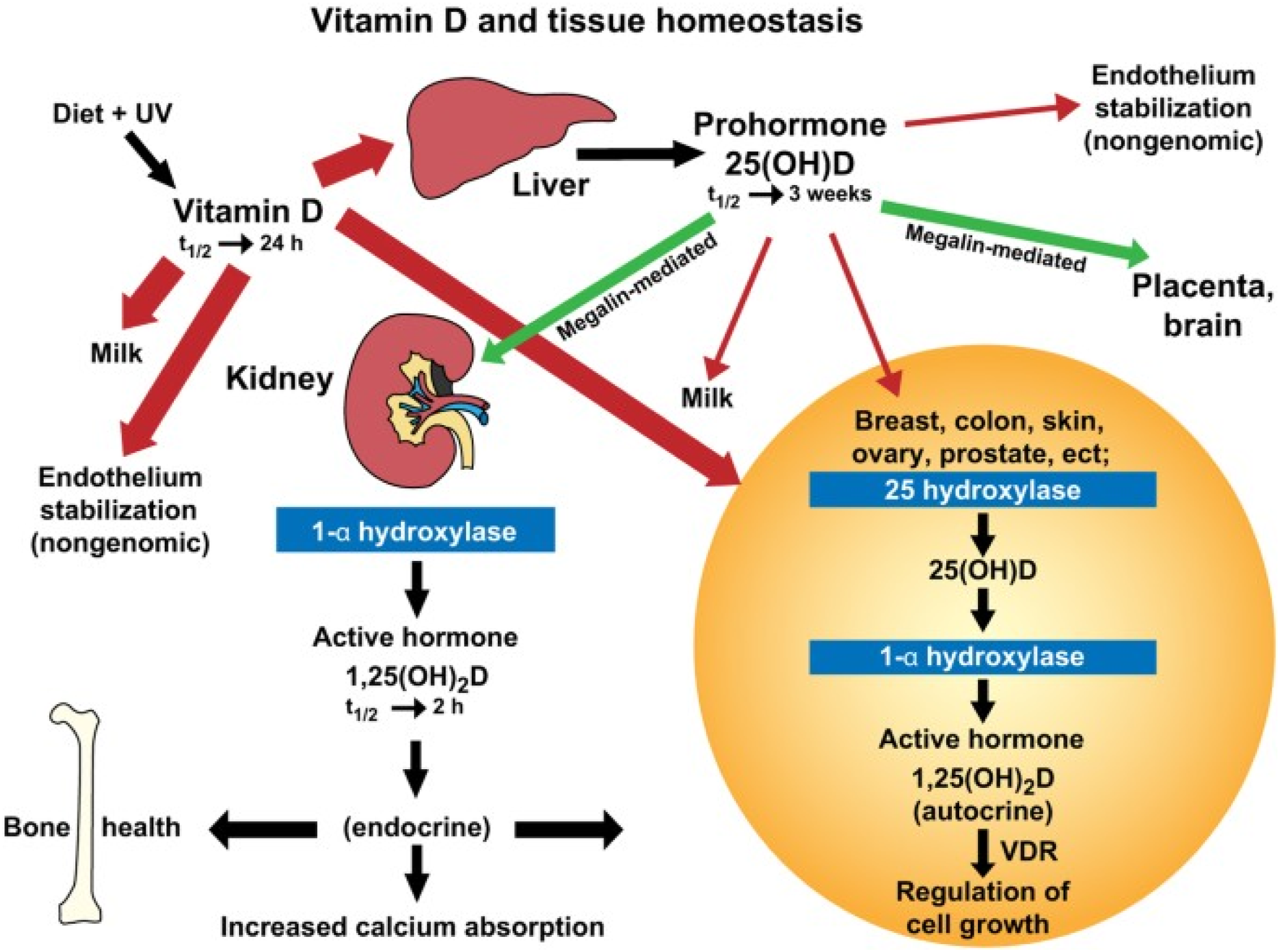
This overlap may reflect volumetric dilution in expanded plasma volume, sequestration of fat-soluble vitamins in adipose tissue, or altered vitamin D metabolism in obesity. Serum 25-hydroxyvitamin D 25(OH)D serves as the primary biomarker of vitamin D status, with a half-life of 2 to 3 weeks, making it suitable for assessing maternal vitamin D adequacy. During pregnancy, placental and decidual production of 1α-hydroxylase increases local synthesis of the active form to meet maternal and fetal demands, and 25(OH)D readily crosses the placenta to support fetal development, as shown in Figure 2.11,13 However, optimal serum 25(OH)D concentrations during pregnancy remain debated, with current recommendations extrapolated from general population guidelines rather than pregnancy-specific evidence.13,14 There is currently no universally accepted serum 25-hydroxyvitamin D [25(OH)D] threshold for defining vitamin D deficiency or insufficiency during pregnancy. The American College of Obstetricians and Gynecologists (ACOG) consider a serum 25(OH)D level of at least 20 ng/mL (50 nmol/L) necessary to avoid bone problems.15,16 Earlier Endocrine Society guidance commonly defined vitamin D deficiency as <20 ng/mL (50 nmol/L) and insufficiency as 20–30 ng/mL (50–75 nmol/L); however, the 2024 Endocrine Society guideline emphasizes that pregnancy-specific 25(OH)D thresholds linked to clinical outcomes have not been established and suggests against routine 25(OH)D testing in generally healthy pregnant individuals.
17
Therefore, this review included studies using varying definitions of vitamin D deficiency and insufficiency, as reported by the original authors. Vitamin D activation during pregnancy adapted from hollis & wagner 2017 (bone res 5:3, CC BY 4.0).
18
Emerging international studies have started exploring the relation and possible association between maternal vitamin D status and GWG.12,19,20 Several observational studies have reported associations between low maternal 25(OH)D concentrations and altered GWG patterns, as well as increased risk of GDM.11,13 However, findings have been inconsistent across populations, and interventional trials of vitamin D supplementation have yielded mixed results. The relationship appears to be influenced by multiple factors, including prepregnancy BMI, baseline vitamin D status, geographic location, and timing of assessment.19,21
Despite the biological plausibility linking vitamin D to weight regulation pathways and growing clinical interest, the relationship between maternal vitamin D status and GWG remains inadequately characterized. Existing studies are limited in number, demonstrate substantial geographic variability, lack a comprehensive synthesis, and have not systematically examined how prepregnancy BMI modifies this relationship. Furthermore, the potential synergistic effects of combined vitamin D deficiency and suboptimal GWG on maternal metabolic outcomes and offspring health remain poorly understood.
Given these knowledge gaps and the potential clinical implications, a narrative review is needed to evaluate the existing evidence systematically and identify priorities for future research. This review addresses four key research questions: 1. What is the prevalence of vitamin D deficiency in pregnancy, and how do maternal anthropometric factors (prepregnancy BMI and GWG) influence vitamin D status? 2. What is the association between maternal vitamin D status and GWG patterns across diverse populations, and does prepregnancy BMI modify this relationship? 3. Do vitamin D deficiency and suboptimal GWG have combined or synergistic effects on maternal metabolic outcomes (insulin resistance, GDM) and fetal/offspring growth trajectories? 4. Is vitamin D supplementation during pregnancy effective in modulating GWG, and what dose is safe and efficacious?
By integrating recent observational and interventional studies alongside expert recommendations, this review aims to provide a comprehensive synthesis of current evidence on the complex interplay between vitamin D status and GWG worldwide. The findings will inform healthcare providers and policymakers about the clinical significance of vitamin D assessment in the context of weight management during pregnancy, identify high-risk subgroups who may benefit from targeted interventions, and highlight critical gaps that should guide future research priorities. Ultimately, this evidence synthesis seeks to contribute to optimizing prenatal care strategies that promote appropriate GWG and address the implications of vitamin D deficiency for maternal and child health globally.
Methodology
This narrative review was conducted in accordance with the SANRA 2.0 (Scale for the Assessment of Narrative Review Articles) 22 recommendations to ensure transparent and high-quality reporting. SANRA 2.0 guided the review structure by ensuring explicit justification of the review’s importance, formulation of concrete research questions, comprehensive description of the literature search strategy, appropriate referencing of key statements, consideration of evidence levels across study designs, and thorough presentation of quantitative data. 22 A completed SANRA 2.0 checklist is provided as supplementary material. Elements of the PRISMA-S (Preferred Reporting Items for Systematic Reviews and Meta-Analyses - Literature Search Extension) 23 were incorporated to document the search strategy, including specification of databases searched, search terms used, date restrictions applied, and language limitations. No prospective protocol was registered, and no quantitative meta-analysis was undertaken, consistent with the narrative review design.
Search strategy
A comprehensive literature search was performed across three databases: PubMed, Scopus, and Google Scholar, as shown in Figure 3. The exact search period covered studies published between January 2015 and November 2025 examining the association between vitamin D status and gestational weight gain (GWG) in pregnant women. Given that Google Scholar does not support structured Boolean search syntax and does not allow exportation of large result sets, screening was limited to the first 50 results per search string, which is consistent with published guidance on the use of Google Scholar as a supplementary search source. Searches were limited to human studies involving pregnant women of any age, with no restrictions on parity, gestational age at enrollment, or geographic location. Search terms combined Medical Subject Headings (MeSH) and free-text keywords in three domains: • • • Study selection flow diagram for narrative review examining of maternal vitamin D status and gestational weight gain.
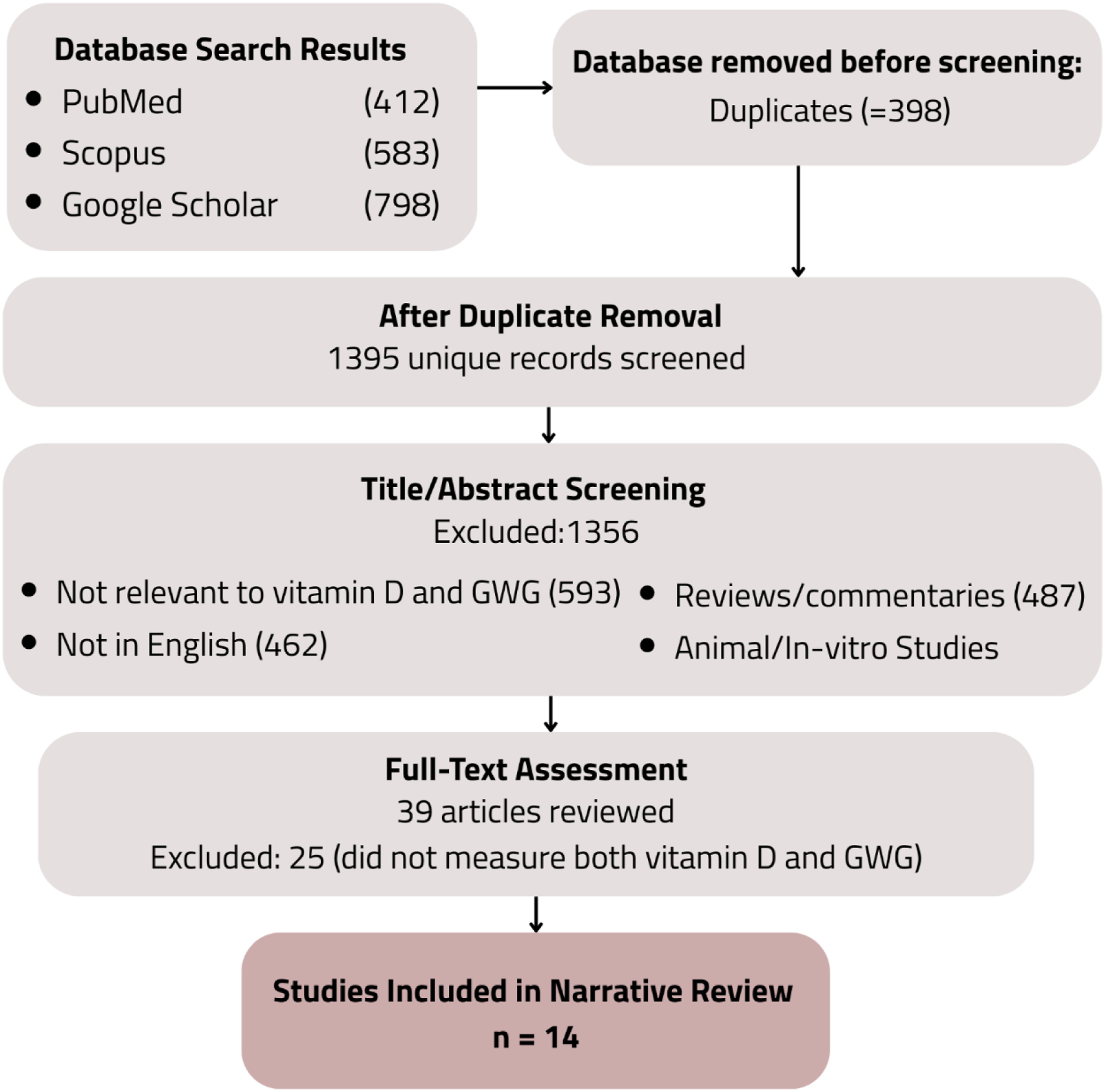
Boolean operators (AND, OR) were used to combine search terms across domains. Reference lists of relevant systematic reviews and included studies were manually screened to identify additional eligible articles. Grey literature, preprints, conference abstracts, and non-peer-reviewed sources were excluded to ensure methodological rigor, two reviewers independently screened all titles and abstracts for eligibility, followed by full-text assessment of potentially relevant articles, and a third reviewer was consulted when consensus could not be reached.
Eligibility criteria
Inclusion criteria
• • • • • •
Exclusion criteria
• Reviews, systematic reviews, meta-analyses, commentaries, editorials, and opinion pieces • Animal studies, in-vitro studies, and laboratory-only research • Studies that did not measure serum 25(OH)D or did not report GWG quantitatively. Studies were required to report gestational weight gain data in conjunction with vitamin D measurements, as the primary aim of this review was to examine these variables within the same populations rather than to provide a standalone epidemiological estimate of vitamin D deficiency prevalence in pregnancy.
Study selection and data extraction
Two reviewers independently screened all titles and abstracts for eligibility, followed by full-text assessment of potentially relevant articles. A standardized screening form was used to ensure consistency. Any discrepancies were resolved by discussion, and a third reviewer was consulted when consensus could not be reached. Data extraction was performed systematically using a standardized form capturing: • Study characteristics: first author, publication year, country, study design • Sample characteristics: sample size, maternal age, prepregnancy BMI, gestational age at enrollment • Vitamin D assessment: timing of measurement, assay method, definition of deficiency/insufficiency • GWG measurement: method of assessment, timing, categorization (adequate/inadequate/excessive based on IOM guidelines or other criteria) • Statistical approach: confounders adjusted for, analytical methods • Key findings: direction and magnitude of associations, effect estimates where available
Quality appraisal
Methodological quality was appraised qualitatively, with particular attention to: • Sample size adequacy and statistical power • Adjustment for key confounders (prepregnancy BMI, gestational age, socioeconomic factors, dietary intake) • Timing and frequency of vitamin D measurements • Standardization of GWG assessment and adherence to established guidelines • Risk of bias considerations (selection bias, measurement bias, confounding)
Given the narrative nature of this review, no formal quality scoring tool was applied. However, methodological strengths and limitations of individual studies were considered when synthesizing evidence.
Data synthesis
Due to substantial heterogeneity in study populations, vitamin D measurement protocols, GWG definitions, and analytical approaches, a quantitative meta-analysis was not feasible or appropriate. Findings were therefore synthesized narratively and organized thematically into four domains: 1. Vitamin D Deficiency Prevalence and Bidirectional Associations with Maternal Weight 2. GWG as a Modifier of Vitamin D’s Metabolic Effects 3. Combined Effects on Fetal and Offspring Outcomes 4. Evidence from Interventional Trials on Vitamin D Supplementation
Within each theme, studies were grouped by design (observational vs. interventional), and findings were compared across populations and methodological approaches. Consistency, discrepancies, and gaps in the evidence base were highlighted to inform conclusions and recommendations for future research.
Results
Summary of studies examining maternal vitamin D status and gestational weight gain. The table presents study characteristics, including design, population, sample size, vitamin D assessment methods, GWG measurement, and key findings for the 14 studies included in this narrative review. BMI, body mass index; GWG, gestational weight gain; GDM, gestational diabetes mellitus; 25(OH)D, 25-hydroxyvitamin D; IOM, Institute of Medicine; RCT, randomized controlled trial; aOR, adjusted odds ratio; SGA, small for gestational age; PPWR, postpartum weight retention.
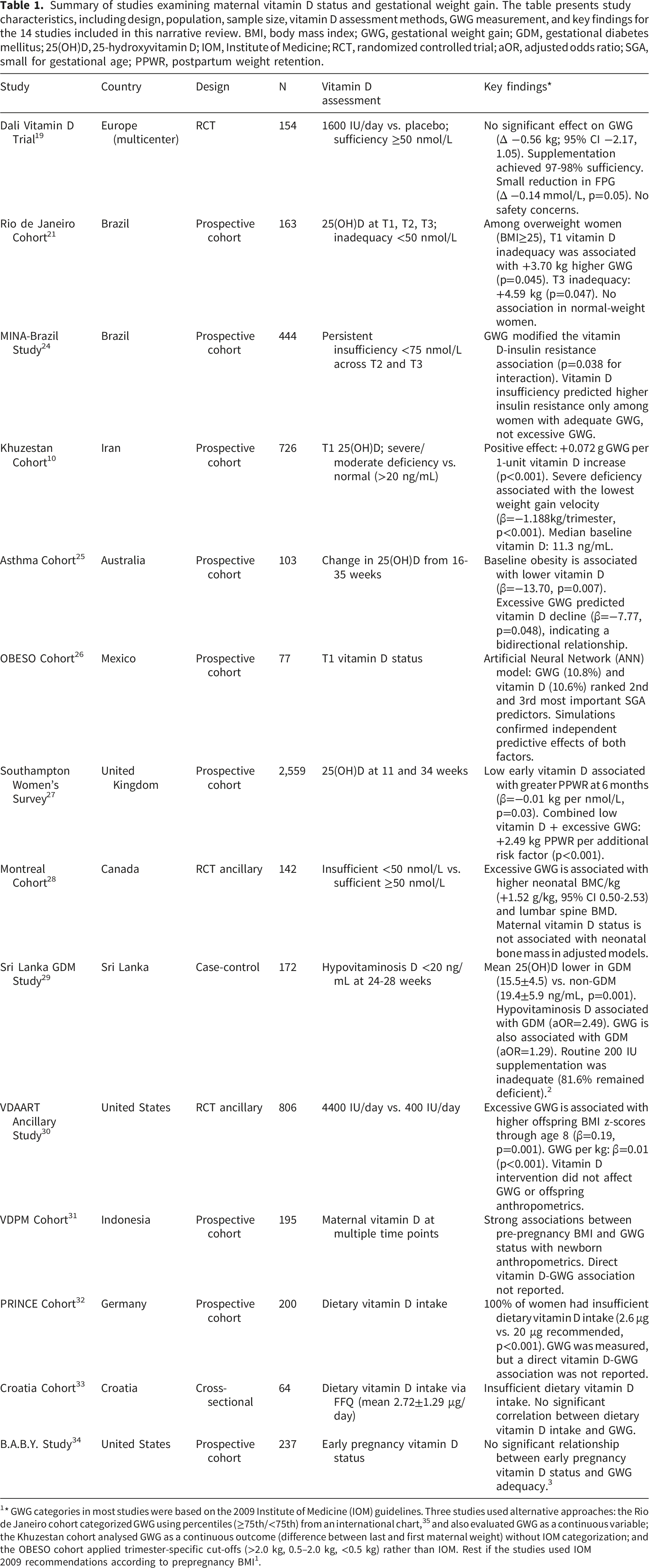
1* GWG categories in most studies were based on the 2009 Institute of Medicine (IOM) guidelines. Three studies used alternative approaches: the Rio de Janeiro cohort categorized GWG using percentiles (≥75th/<75th) from an international chart, 35 and also evaluated GWG as a continuous variable; the Khuzestan cohort analysed GWG as a continuous outcome (difference between last and first maternal weight) without IOM categorization; and the OBESO cohort applied trimester-specific cut-offs (>2.0 kg, 0.5–2.0 kg, <0.5 kg) rather than IOM. Rest if the studies used IOM 2009 recommendations according to prepregnancy BMI 1 .
Vitamin D Deficiency Prevalence and Bidirectional Associations with maternal weight
Vitamin D deficiency was widespread among all examined populations, although prevalence rates differed significantly by geographic region and demographic characteristics. In the Rio de Janeiro cohort, vitamin D insufficiency (defined as 25(OH)D <75 nmol/L) impacted 71.8% of women in early pregnancy, declining to 33.9% by the third trimester, while vitamin D inadequacy (<50 nmol/L) reached its zenith at 16.6% in the first trimester. 21 The Khuzestan cohort in Iran exhibited severe deficiency, with a median baseline vitamin D level of merely 11.3 ng/mL (IQR 8, 16.5). 9 In Sri Lanka, hypovitaminosis D (<20 ng/mL) impacted 84.9% of GDM mothers and 60.5% of non-GDM mothers, notwithstanding regular prenatal supplementation. 29
Dietary vitamin D intake was universally insufficient across populations. In the German PRINCE cohort, 100% of pregnant women failed to meet the recommended daily intake from food alone, with a mean consumption of 2.6 μg versus the recommended 20 μg (p<0.001). 32 Similarly, the Croatian study found a mean dietary intake of only 2.72±1.29 μg/day, well below recommended levels. 33
Prepregnancy BMI was strongly associated with vitamin D status. In the Australian cohort of pregnant women with asthma, baseline obesity (BMI≥30 kg/m2) was significantly associated with lower 25(OH)D levels (β=-13.70, p=0.007). 25 Evidence also suggested that excessive weight gain during pregnancy influences vitamin D concentrations. In the same cohort, excessive GWG independently predicted a significant decline in 25(OH)D levels from 16 to 35 weeks of gestation (β=-7.77, p=0.048), indicating a potential bidirectional relationship. 25
The association between vitamin D status and GWG patterns varied considerably across studies and appeared modified by prepregnancy BMI. In the Rio de Janeiro cohort, vitamin D inadequacy in the first trimester was associated with higher total GWG among overweight women (BMI≥25 kg/m2), with inadequate vitamin D status predicting an additional 3.70 kg of weight gain (p=0.045) compared to women with adequate vitamin D. 21 This association strengthened when vitamin D was measured in the third trimester (β=4.59 kg, p=0.047). Importantly, no such association was observed among normal-weight women, indicating BMI-dependent modification of the vitamin D-GWG relationship. 21
The Khuzestan cohort in Iran exhibited a more intricate pattern. The modified total effect of vitamin D on gestational weight gain (GWG) was favorable, with each one-unit increase in vitamin D, a 0.07kg rise in mean GWG (p<0.001) was observed. 10 However, women with severe vitamin D deficiency had significantly lower weight gain velocity across pregnancy trimesters compared to those with moderate deficiency or normal levels (β=-1.188, p<0.001), suggesting a non-linear relationship. 10 In contrast, two studies found no association between vitamin D status and GWG. The prospective B.A.B.Y. Study reported no significant relationship between early pregnancy vitamin D status and GWG adequacy, 34 and the Dietary and Lifestyle Intervention for gestational diabetes prevention (DALI) randomized trial found that vitamin D supplementation achieving near-universal sufficiency did not affect total GWG. 19
GWG as a modifier of vitamin D’s metabolic effects
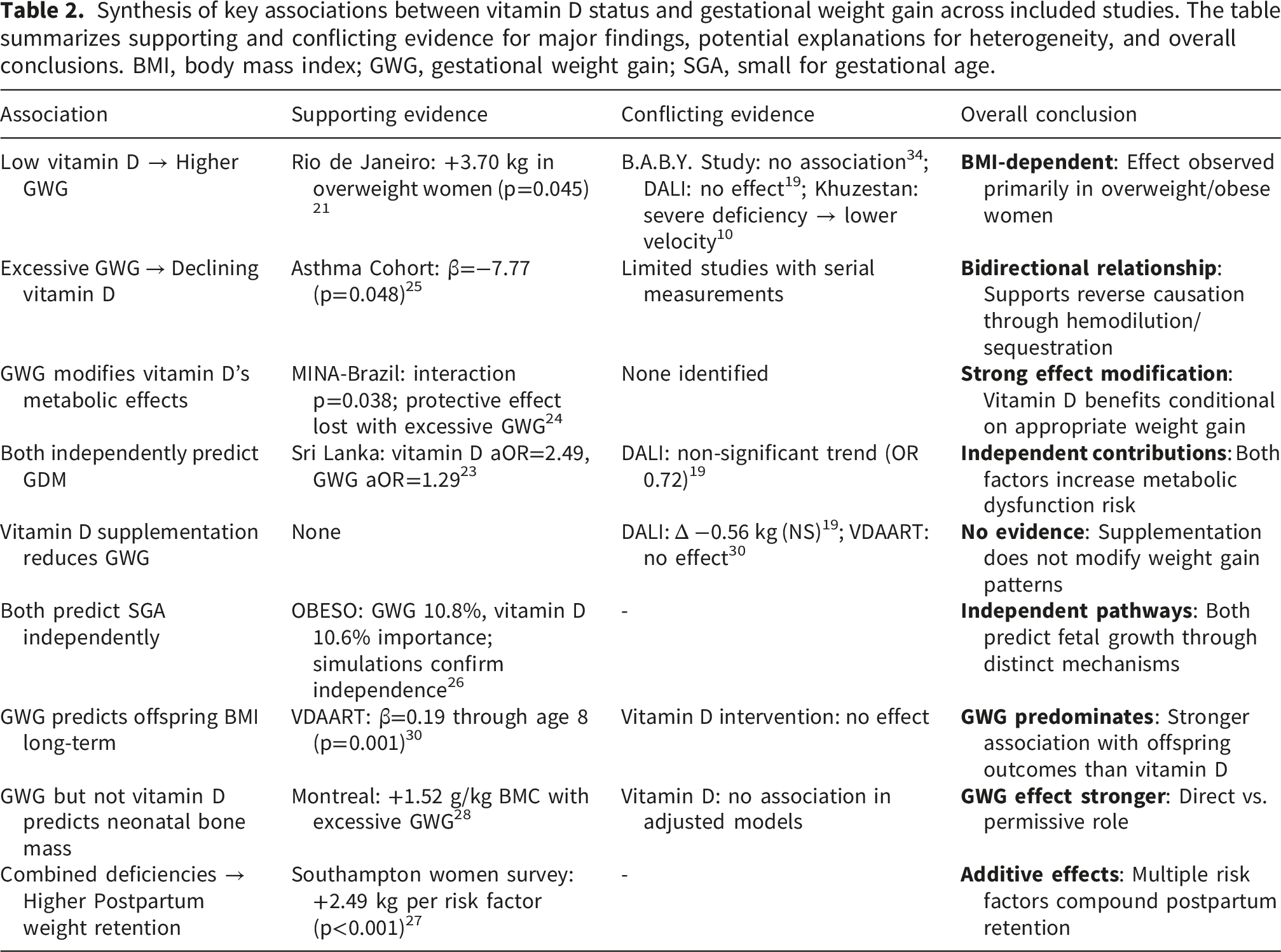
Synthesis of key associations between vitamin D status and gestational weight gain across included studies. The table summarizes supporting and conflicting evidence for major findings, potential explanations for heterogeneity, and overall conclusions. BMI, body mass index; GWG, gestational weight gain; SGA, small for gestational age.
Among women who attained sufficient gestational weight gain (GWG) in accordance with IOM guidelines, chronic vitamin D deficiency correlated with a predicted probability of insulin resistance at 0.345, in contrast to 0.134 for women with adequate vitamin D levels. However, in women with excessive GWG, the predicted probabilities for insulin resistance did not significantly differ based on vitamin D status, suggesting that excessive weight gain diminished the protective effect of sufficient vitamin D on insulin sensitivity. 24
Multiple studies documented associations between vitamin D deficiency and gestational diabetes mellitus risk. In the Sri Lankan case-control study, mean serum 25(OH)D was significantly lower in GDM mothers (15.5±4.5 ng/mL) compared to non-GDM controls (19.4±5.9 ng/mL, P=0.001). 29 Among GDM mothers, serum 25(OH)D showed significant inverse correlations with fasting plasma glucose (r=-0.267, P=0.013) and HOMA-IR (r=-0.249, P=0.021). After adjusting for confounders, including age, BMI, family history, and GWG, hypovitaminosis D remained independently associated with GDM (adjusted OR=2.49), and GWG was also independently associated (adjusted OR=1.29). In the DALI trial among overweight and obese women, vitamin D supplementation showed a non-significant trend toward reduced GDM incidence (OR 0.72, 95% CI 0.33 to 1.59). 19
combined effects on fetal and offspring outcomes
Machine learning analysis from the OBESO cohort in Mexico (n=77) identified both GWG and vitamin D as critical predictors of adverse fetal growth outcomes. 26 Using first-trimester maternal data, an Artificial Neural Network model identified GWG (10.8% relative importance) and vitamin D status (10.6%) as the second and third most important predictors of SGA births, ranking just below protein oxidation (12.7%). Simulation modeling confirmed independent predictive effects: setting GWG to a simulated value of 2.5 kg (inadequate gain) predicted SGA even with adequate vitamin D status, while setting vitamin D to simulated value of 10 ng/mL (severe deficiency) predicted SGA regardless of GWG or maternal redox status. 26
Long-term offspring anthropometric outcomes were examined in the vitamin D Antenatal Artificial Asthma Reduction Trial (VDAART) ancillary study, a randomized trial originally designed to evaluate high-dose vitamin D supplementation for asthma prevention in offspring, which followed children through 8 years of age. Findings should be interpreted with caution, as the trial’s primary focus on asthma outcomes and its enrollment criteria may limit generalizability to the broader pregnant population. Maternal GWG analyzed as a continuous variable showed independent positive associations with offspring BMI z-scores from birth through 8 years (β=0.01 per kg GWG, 95% CI 0.01 to 0.02, p<0.001). 30 When categorized by IOM adequacy, excessive GWG was associated with significantly higher offspring BMI z-scores compared to adequate GWG (β=0.19, p=0.001). Maternal prepregnancy BMI demonstrated even stronger associations, with maternal obesity predicting β=0.49 higher offspring BMI z-scores (p<0.001). Notably, the vitamin D intervention arm (4400 IU/day versus 400 IU/day) did not significantly affect offspring anthropometric outcomes. 30
Neonatal bone mass outcomes were assessed in the Montreal cohort. 28 Maternal GWG categories showed modest but significant associations with neonatal bone parameters. Infants born to mothers with excessive GWG had 1.52 g/kg greater whole-body bone mineral content per kilogram body weight (95% CI 0.50 to 2.53) compared to the adequate GWG reference group, along with significantly higher lumbar spine bone mineral content and bone mineral density. In contrast, maternal 25(OH)D status (insufficient <50 nmol/L versus sufficient ≥50 nmol/L) was not independently associated with neonatal bone mass outcomes in adjusted models. 28 The Indonesian VDPM cohort similarly found strong associations between prepregnancy BMI and GWG status with newborn anthropometrics, though direct associations between maternal vitamin D status and newborn size were not reported. 31
Evidence from vitamin D supplementation trials
The DALI trial, which included 154 overweight and obese pregnant women (BMI≥29 kg/m2) from various European locations, demonstrated that 1600 IU of vitamin D per day was highly effective in achieving biochemical sufficiency. 19 In the intervention group, 97% to 98% of participants attained vitamin D sufficiency (≥50 nmol/L) during evaluations at 24-28 weeks and 35-37 weeks of gestation, in contrast to reduced rates observed in the placebo group. Even though vitamin D sufficiency was achieved in nearly all participants, supplementation didn’t significantly affect total GWG from the first to the third trimester. The adjusted difference in total GWG between the intervention and placebo groups was -0.56 kg (95% CI -2.17 to 1.05), which was not statistically significant. The intervention led to a modest yet significant decrease in fasting plasma glucose at 35-37 weeks (Δ-0.14 mmol/L, p=0.05). There were no cases of hypercalcemia or other negative events, confirming the safety of this dosing regimen. 19
The VDAART trial tested an even higher dose, randomizing women to receive either 4400 IU/day or 400 IU/day vitamin D3 from early pregnancy through delivery. 30 Consistent with DALI findings, high-dose supplementation showed no significant effect on maternal GWG patterns. The ancillary analysis examining offspring outcomes found no differences in offspring BMI z-scores through 8 years of age between the high-dose and standard-dose arms, and no safety concerns emerged with the higher supplementation dose. 30
Observational data from the Southampton Women’s Survey provided evidence linking vitamin D status to postpartum weight retention. 27 Lower serum 25(OH)D concentration in early pregnancy (11 weeks), analyzed continuously, was independently associated with greater postpartum weight retention at 6 months (β=-0.01 kg per unit vitamin D increase, p=0.03). When examining the combined effect of modifiable risk factors, women with low early pregnancy vitamin D and excessive GWG retained an additional 2.49 kg (95% CI 2.16 to 2.82, p<0.001) for each additional risk factor present at 6 months postpartum. 27
The inadequacy of low-dose routine supplementation was documented in the Sri Lankan study. 29 Women receiving routine prenatal supplements containing 200 IU of cholecalciferol showed no significant difference in serum 25(OH)D levels compared to non-supplemented women (P>0.05). Among GDM mothers who had taken these routine supplements, 81.6% still had vitamin D levels below 20 ng/mL, meeting criteria for deficiency. This finding demonstrated that commonly prescribed low-dose prenatal supplementation is insufficient to achieve or maintain vitamin D adequacy during pregnancy. 29
Discussion
Principal findings
This narrative evaluates synthesized evidence from 14 studies investigating the correlation between maternal vitamin D levels and gestational weight gain in various global populations. Four main findings came out. First, vitamin D deficiency is still very common during pregnancy, affecting 30–85% of women depending on where they live, the time of year, and the characteristics of the population. Women who are overweight or obese are especially likely to have low levels of vitamin D. Second, the correlation between vitamin D status and gestational weight gain (GWG) seems to be bidirectional but varies across studies. Prepregnancy body mass index (BMI) has been identified as a significant effect modifier, with the most robust associations found in overweight and obese women. Third, too much GWG greatly reduces the protective metabolic effects of having enough vitamin D, especially when it comes to insulin resistance. This suggests that these two risk factors work together. Fourth, although vitamin D supplementation at doses of 1600 IU/day effectively attains biochemical sufficiency, existing evidence does not endorse its application as a primary intervention to alter GWG trajectories. A summary of supporting and conflicting associations across studies is presented in Table 2.
Interpretation in the context of existing literature
Prevalence and determinants of vitamin D deficiency
The significant prevalence of vitamin D deficiency identified in this review corresponds with global estimates, suggesting that hypovitaminosis D impacts around 54% of pregnant women worldwide, exhibiting considerable regional variation. 36 The negative correlation between maternal adiposity and vitamin D status is well-documented and probably results from several mechanisms: volumetric dilution due to increased plasma volume, sequestration in adipose tissue, and possibly modified vitamin D metabolism in obesity. Our findings corroborate that prepregnancy BMI is not only the most robust predictor of GWG adequacy but also substantially affects baseline vitamin D status, establishing a complex interaction between these two modifiable risk factors.
For most individuals, cutaneous synthesis via UVB radiation from sunlight is the predominant source of vitamin D, the observation that 100% of pregnant women in the German PRINCE cohort failed to meet recommended intake from food alone underscore the inadequacy of dietary sources in isolation, particularly populations with limited sunlight exposure, and highlights the need for targeted supplementation or fortification strategies in pregnancy seasonal variation, skin pigmentation, and geographical latitude must be considered when interpreting the findings. 32
The vitamin D-GWG relationship: Biological plausibility and inconsistent evidence
The biological mechanisms linking vitamin D to weight regulation are well-characterized. Vitamin D receptors are expressed in adipocytes, and 1,25-dihydroxyvitamin D regulates adipogenesis, influences insulin sensitivity, modulates systemic inflammation through cytokine production, and affects leptin expression. These pathways theoretically position vitamin D as a potential modulator of maternal fat deposition and weight gain during pregnancy. 12 However, the evidence synthesized in this review reveals substantial inconsistency in observed associations.
The Rio de Janeiro cohort demonstrated that first-trimester vitamin D inadequacy led to approximately 3.70 kg higher total GWG specifically among overweight women, 21 while the Khuzestan cohort found that severe vitamin D deficiency was associated with slower weight gain velocity. 10 Conversely, the B.A.B.Y. Study and the DALI trial found no significant associations between vitamin D status and GWG.19,34 These discrepancies likely reflect several factors: differences in baseline vitamin D status across populations (the DALI cohort had relatively high baseline levels, potentially limiting the observable effect), timing of vitamin D assessment (first-trimester measurements may capture different biological windows than third-trimester assessments), varying definitions of vitamin D deficiency and GWG adequacy, and importantly, the modifying effect of prepregnancy BMI.19,34
The bidirectional nature of the relationship adds further complexity. The Australian asthma cohort demonstrated that excessive GWG independently predicted declining vitamin D levels across pregnancy, possibly due to hemodilution effects from expanded plasma volume or increased sequestration in newly deposited adipose tissue. This bidirectional relationship suggests that interventions targeting either factor may have reciprocal effects, though current evidence remains insufficient to confirm this hypothesis. 25
Prepregnancy BMI as a critical effect modifier
Perhaps the most clinically relevant finding from this review is the consistent emergence of prepregnancy BMI as an effect modifier. The vitamin D-GWG association appears strongest, and in some studies exclusively present, among women with overweight and obesity. This BMI-dependent relationship has important mechanistic and clinical implications.
Mechanistically, women with obesity have lower bioavailable vitamin D due to adipose sequestration and may have altered vitamin D metabolism. They also face greater metabolic demands during pregnancy and are at higher risk for insulin resistance and inflammatory states, conditions that vitamin D may influence. The observation that vitamin D inadequacy specifically predicted higher GWG in overweight women from the Rio de Janeiro cohort suggests that this subgroup may be particularly vulnerable to the metabolic consequences of vitamin D deficiency. 21
Clinically, these findings suggest that universal vitamin D supplementation may be less effective than targeted approaches. Women with elevated prepregnancy BMI represent a high-risk subgroup who might benefit most from combined interventions addressing both vitamin D status and weight management counseling. 21
Synergistic effects on metabolic and offspring outcomes
The MINA-Brazil Study provided crucial evidence that GWG modifies the relationship between vitamin D and maternal metabolic outcomes. 24 Among women with adequate GWG, persistent vitamin D insufficiency was associated with substantially higher odds of insulin resistance. However, among women with excessive GWG, this protective effect was lost; vitamin D status no longer predicted insulin resistance risk. This interaction suggests that the metabolic benefits of vitamin D sufficiency are conditional upon appropriate weight gain and highlights the importance of addressing both factors concurrently rather than in isolation.
For offspring outcomes, the evidence indicates that both maternal vitamin D status and GWG independently predict fetal growth trajectories, with GWG generally showing stronger direct effects. The OBESO artificial neural network modeling demonstrated that while both factors rank among the top predictors of SGA births, simulations confirmed their independent predictive power. 26 One ancillary analysis of the VDAART trial suggested that excessive GWG predicts higher offspring BMI z-scores through 8 years of age, with effect sizes comparable to or exceeding those of maternal prepregnancy BMI; however given the asthma focused design and specific enrollment population of VDAART, these findings require replication in general obstetric cohorts before broader conclusions can be drawn. 30 In contrast, maternal vitamin D status showed more modest or inconsistent associations with offspring anthropometrics.
These findings collectively suggest that while vitamin D plays a role in pregnancy outcomes, optimizing GWG may be the more impactful intervention target for improving both immediate and long-term offspring health. However, given the interaction effects suggested by limited observational data, integrated approaches addressing both factors simultaneously warrant investigation.
Clinical and public health implications
For clinical practice
The evidence synthesized in this review suggests several clinical considerations. First, it is important to note that routine vitamin D screening in pregnancy is not currently recommended as standard clinical practice, and the evidence from this review is insufficient to support changes to existing screening policy. However, risk stratified assessment may be most informative for women with elevated prepregnancy BMI, given that this subgroup demonstrates the strongest associations between vitamin D status and adverse metabolic outcomes.
Second, vitamin D supplementation at doses of 1600 IU/day is safe, well-tolerated, and highly effective at achieving biochemical sufficiency, as demonstrated in the DALI trial. 19 However, clinicians should not expect supplementation alone to modify GWG trajectories. The small reduction in fasting plasma glucose observed with supplementation (0.14 mmol/L) suggests potential metabolic benefits independent of weight effects. Current routine prenatal supplementation doses (200 IU/day) are clearly inadequate, as shown in the Sri Lankan study, where 81.6% of women receiving such supplements remained deficient. 29
Third, prenatal care should integrate vitamin D assessment with comprehensive GWG counseling, particularly for women with overweight and obesity. The observed interaction between excessive GWG and vitamin D status on insulin resistance, as reported in a single large cohort, 24 suggests that addressing both factors at the same time may be more beneficial than targeting either in isolation. Weight management interventions should therefore be considered alongside vitamin D optimization, especially in women with overweight and obesity.
Fourth, postpartum weight retention represents an underappreciated outcome influenced by both vitamin D status and GWG. The Southampton Women’s Survey demonstrated that each additional risk factor (including low early pregnancy vitamin D and excessive GWG) contributed 2.49 kg of additional weight retention at six months postpartum, with implications for interpregnancy health and long-term cardiovascular risk. 27
For public health policy
At the population level, food fortification strategies may be more cost-effective and equitable than individual supplementation programs, particularly in regions with high deficiency prevalence. Countries with mandatory vitamin D fortification of milk, cereals, or other staple foods (e.g., United States, Canada, Finland) have achieved higher population vitamin D status.20,37,38 However, fortification alone is unlikely to achieve sufficiency in pregnancy given increased requirements. 39
Public health messaging should emphasize that achieving adequate GWG is a primary goal, while maintaining vitamin D sufficiency through supplementation and safe sun exposure supports overall metabolic health, 40 Health education programs targeting preconception and early pregnancy represent critical intervention windows, particularly for women with elevated BMI. 41
Resource allocation decisions must weigh the relative impact of vitamin D supplementation programs against weight management interventions. Given that GWG showed stronger direct associations with offspring outcomes20,38 and that vitamin D supplementation did not modify GWG in trials,19,30 investment in evidence-based GWG interventions (dietary counseling, physical activity programs, behavioral support) may yield greater population health benefits. However, vitamin D supplementation is low-cost, safe, and provides additional metabolic benefits, for populations or individuals with low baseline vitamin D status, supplementation is essential to prevent deficiency-related complications and may provide greater metabolic benefits than observed in trials with adequate baseline status. Thus, vitamin D supplementation should be included as a component of comprehensive prenatal care rather than a standalone intervention, with particular attention to ensuring adequate dosing for high-risk groups.
Strengths and limitations
Strengths
This review has several strong points. The thorough search strategy across various databases encompassed a range of study designs from different geographic areas, offering a global viewpoint on the vitamin D-GWG relationship. The incorporation of both observational and interventional studies facilitated the synthesis of associative evidence and causal inference derived from randomized controlled trials. The narrative approach was suitable due to significant heterogeneity in populations, vitamin D measurement protocols, and GWG definitions that rendered quantitative meta-analysis unfeasible. The consistent use of SANRA 2.0 guidelines ensured that the reports were clear and of high quality. Finally, the emphasis on effect modification by prepregnancy BMI and the analysis of synergistic effects on outcomes signify innovative contributions that enhance comprehension beyond mere bivariate associations.
Limitations
Some limitations need to be recognized. The narrative synthesis method is good for data that is not all the same, but it doesn’t have the same level of statistical accuracy as quantitative meta-analysis and may be biased in how it interprets the data. Publication bias may favor studies that report significant associations over those that report null findings, which could lead to an overestimation of effect sizes. The limitation of English-language publications may have omitted pertinent studies from non-English-speaking areas, especially those with significant vitamin D deficiency challenges, such as the Middle East, South Asia, and North Africa.
The methodological quality of the included studies was inconsistent, with inadequate adjustments for significant confounders (dietary intake, physical activity, socioeconomic factors), varying vitamin D assay techniques and cutoff values (from 20 to 75 nmol/L), and divergent GWG assessment protocols that hinder direct comparability. The geographic representation was biased toward high-income nations (Europe, North America), with insufficient data from low- and middle-income countries where vitamin D deficiency and inadequate GWG are significantly common. The limited number of interventional trials (n=2) constrained conclusions regarding causality and optimal supplementation strategies.
Several cohort studies had small sample sizes (from 64 to 726 participants), which may have made it harder to find small effects or interactions. Multiple studies assessed vitamin D at merely one or two times, thereby inhibiting a comprehensive evaluation of longitudinal trajectories and temporal associations. Only a limited number of studies investigated possible mediating pathways (inflammation, insulin sensitivity, adipokine profiles) that might elucidate biological mechanisms. Finally, the differences in how studies define vitamin D deficiency and how they group GWG made it harder to put together the evidence and made it harder to use the findings in clinical practice.
Future research directions
Future research should emphasize methodological enhancements, including prospective cohort studies with serial vitamin D measurements across all trimesters utilizing standardized assays and internationally recognized cutoff values, accompanied by thorough confounder adjustment; mechanistic investigations employing metabolomic and proteomic techniques to elucidate biological pathways connecting vitamin D to maternal metabolism, while examining potential mediators such as inflammatory markers and adipokines, and exploring genetic polymorphisms in vitamin D metabolism; and interventional trials assessing higher supplementation doses (2000-4000 IU/day) initiated preconceptionally alongside integrated behavioral weight management programs to evaluate synergistic effects. Geographic expansion to underserved areas in low and middle-income countries where vitamin D deficiency and inadequate gestational weight gain are common; long-term follow-up studies investigating offspring outcomes into adolescence and intergenerational health effects; implementation science research focusing on cost-effectiveness analyses and optimal delivery models, including digital health approaches; and precision medicine strategies to identify subgroups most likely to benefit from targeted interventions based on BMI, genetic background, and baseline vitamin D status to facilitate personalized prenatal care.
Conclusion
The association between maternal vitamin D status and GWG remains inconsistent across the current evidence base. Prepregnancy BMI seems to have an important effect modifier, with the strongest associations observed among women with overweight and obese BMI. Supplementation at 1600IU/day safely achieves biochemical sufficiency but does not modify GWG in trial settings, evidence from a single large observational cohort suggests that excessive GWG may weaken the association between vitamin D sufficiency and insulin resistance; this finding requires prospective replication before clinical recommendations can be made. GWG is a more consistently strong predictor of offspring anthropometric outcomes than maternal vitamin D status, although both appear to contribute independently. Integrated approaches addressing both vitamin D adequacy and appropriate weight gain, particularly in high-risk groups, warrant investigation in future interventional trials.
Footnotes
Ethical considerations
Ethical approval was not required for this narrative review as it did not involve human participants, their data, or tissue. All studies included in this review had appropriate ethical approval as reported in the original publications.
Author contributions
RBQ, MNM, and LS conceived the review, developed the methodology, and drafted the original manuscript. HH, ASA, DP, and LCI contributed to conceptualization, supervised the work, and critically revised the manuscript. All authors read and approved of the final manuscript.
Funding
No specific funding was received for this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study. All data discussed are available in the cited publications.
Acknowledgement
The authors gratefully acknowledge the support provided by the University of Sharjah.