
Abstract
Background
Unintended pregnancy remains a major public health concern in Sierra Leone, where stigma, misconceptions, and access barriers hinder the timely use of emergency contraception (EC).
Objectives
To estimate the prevalence of EC use, assess related knowledge and attitudes, and identify associated factors among female university students in Sierra Leone.
Design
A cross-sectional study using convenience sampling.
Methods
Conducted in 2024 among 366 female undergraduate students at Njala University, Sierra Leone, using convenience sampling and a structured, self-administered questionnaire to assess sociodemographic characteristics, EC utilisation, knowledge, and attitudes. The knowledge and attitudes were scored and categorised based on the mean scores. Descriptive statistics, logistic regression, and Pearson’s and Spearman’s correlations were used for analysis.
Results
Among participants, 68.3% (n=250) reported ever using EC, with 36.5% (n=91) of ever-users using it within the past four weeks and 29.5% (n=74) between one and three months prior to the survey. Of participants, 53.0% (n=194) had good knowledge, and 49.7% (n=182) had a positive attitude toward EC. Ever-use was more likely among students aged 26–30 years (AOR 3.58; 95% CI 1.42–8.90) and in year two (AOR 2.64; 95% CI 1.25–5.55), but less likely with poor knowledge (AOR 0.16; 95% CI 0.09–0.30) and negative attitudes (AOR 0.19; 95% CI 0.10–0.36). No prior history of EC use was associated with lower odds of both good knowledge (AOR 0.20; 95% CI 0.10–0.41; p < 0.001) and positive attitude (AOR 0.23; 95% CI 0.11–0.46; p < 0.001). Knowledge and attitudes were strongly correlated (r=0.659; rho=0.611; p<0.001).
Conclusion
EC use is widespread among sampled students but is influenced by knowledge and attitudes. These exploratory findings suggest that targeted, peer- and provider-led education to address misconceptions and improve service navigation could enhance informed contraceptive choices and reduce unintended pregnancies in this context.
Keywords
Introduction
Unintended pregnancy among adolescents and young adults remains a major public health concern globally and across sub-Saharan Africa, with implications for maternal morbidity and mortality, educational attainment, and socioeconomic outcomes.1–3 In West Africa, adolescent birth rates remain among the highest worldwide, with an estimated rate of 115 births per 1,000 women aged 15–19 years.4,5 The average unmet need for contraception in the region is approximately 22% among women of reproductive age. 6 Sierra Leone has one of the highest maternal mortality ratios globally, estimated at 1,120 deaths per 100,000 live births in 2020, 7 with unintended pregnancy contributing significantly to unsafe abortions, particularly among young, unmarried women, though national estimates on abortion burden remain limited. 8 Young women in this context face structural, social, and informational barriers to effective pregnancy prevention.9–11 Within this context, university students represent a key population at risk of unintended pregnancy due to evolving sexual behaviours, inconsistent use of routine contraceptive methods, and limited access to youth-friendly reproductive health services.10,11
Emergency contraception (EC) provides an important second-chance method to prevent pregnancy after unprotected intercourse, contraceptive failure, or sexual assault.12,13 Levonorgestrel (LNG) EC pills are most commonly used and are effective when taken as soon as possible, ideally within 72 hours of unprotected sex, with diminishing efficacy thereafter; ulipristal acetate extends the effective window up to 120 hours.12,14,15 The copper intrauterine device (IUD) is the most effective EC method and can be inserted within five days of ovulation or unprotected intercourse and then continued as an ongoing contraceptive.12,16 International guidelines consider EC safe for most users, with no serious long-term health risks, and emphasise that EC does not interrupt an established pregnancy and does not protect against sexually transmitted infections (STIs).12,17 Despite safety and effectiveness, EC utilisation is often constrained by knowledge gaps, misconceptions (such as fears of infertility or conflation with abortion), stigma, cost, and access barriers, including pharmacy and clinic availability and provider attitudes.18–21
University settings offer a strategic platform to assess EC-related knowledge, attitudes, and practices, and to tailor interventions that address the specific needs of young adults. Studies from various African countries report substantial awareness of EC but variable accuracy of knowledge, with common misconceptions about timing, dosing, and side effects, and variable patterns of use, including repeat use and reliance on EC instead of ongoing contraception.22–25 Peer networks, intimate partners, and health professionals are frequently cited as sources of information and recommendations, while institutional education and formal curricula often play a limited role.22,23 Furthermore, repeated EC use may signal both the accessibility of EC and gaps in uptake of effective routine methods, underscoring the importance of integrating EC access with counselling and referral for ongoing contraception.12,26 In Sierra Leone, there is limited published evidence on EC utilisation and its determinants among university students. Understanding the prevalence of EC use, the accuracy of knowledge, prevailing attitudes, and the social and structural factors influencing behaviour is essential for informing campus-based health services, educational programs, and national policy.
In Sierra Leone, emergency contraception, primarily levonorgestrel pills, is available over-the-counter at pharmacies with typical costs ranging from 5,000 to 10,000 Leones (approximately 0.25–0.50 USD), though pharmacist counselling is often required. National youth and sexual reproductive health (SRH) programs provide limited free access to EC, and availability through public facilities varies. At university settings like Njala Campus, health services offer EC sporadically, often with inconsistent stock and limited affordability for students, necessitating reliance on private pharmacies. These details on availability and cost are based on local health policy reports and surveys conducted in Sierra Leone. 14
This study aimed to estimate the prevalence of EC use among female university students in Sierra Leone; to assess EC-related knowledge and attitudes, including common misconceptions; and to identify factors associated with EC utilisation. We further sought to characterise sources of EC recommendation and perceived barriers to access. By generating context-specific evidence, our findings are intended to support targeted, youth-friendly strategies to improve accurate EC knowledge, reduce stigma, and strengthen access to both EC and effective routine contraceptive methods within university settings in Sierra Leone.
Methods
Study design and setting
This study employed a cross-sectional design to assess the utilisation, knowledge, and attitudes toward emergency contraceptives among female university students. The research was conducted in 2024 at the Njala Campus of Njala University, a prominent public university located in Sierra Leone. The campus hosts students from diverse socioeconomic and cultural backgrounds across the country, making it a suitable setting for examining the health behaviours and knowledge of young, educated women. The reporting of this study conforms to the STROBE statement. 27
Study population and sampling
The study population comprised registered female undergraduate students from various faculties at Njala University, including Agriculture, Environmental Sciences, Social Sciences, Technology, Education, and Natural Resources Management. Inclusion criteria included being a female undergraduate student, aged 16 years or older, and willing to provide informed consent. Among those meeting the inclusion criteria, exclusion criteria applied to female undergraduate students unwilling to participate or unable to complete the questionnaire due to language or other barriers.
A convenience sampling technique was utilised due to resource constraints and the exploratory nature of this study, allowing rapid data collection among a diverse student population. Data collectors approached potential participants in common areas on campus, such as lecture halls, libraries, and hostels, between March and April 2024. This non-probability sampling technique involved data collectors visiting high-traffic campus locations during break hours to maximise diversity in representation across faculties and academic years. They explained the study purpose to all female students present in these areas and invited voluntary participation from those who met the inclusion criteria, without pre-selection or specific quotas, until the target sample size was reached. A total of 366 students consented and completed the questionnaire. A formal power analysis for sample size calculation was not conducted due to the exploratory focus and resource limitations; the sample size was based on feasibility and prior studies in similar settings.22,24 This limitation is acknowledged in the Discussion section.
Data collection instrument and procedure
Data were collected using a pre-tested, structured, self-administered questionnaire, which was developed based on a review of existing literature and the study’s specific objectives. The questionnaire was divided into four main sections. The first section collected sociodemographic information, including age, religion, marital status, faculty (department), current year of study, residence type, and average monthly allowance.
The second section focused on the utilisation of emergency contraceptives. It included questions on whether the student had ever used EC, the specific method used, the recency and frequency of use, the reasons for non-use, and the source of recommendation for using EC (e.g., friends, partner, health professional).
The third section assessed participants’ knowledge of emergency contraceptives using a series of 13 statements with “True,” “False,” or “Don’t Know” response options. These items covered key aspects such as the recommended timeframe for use (within 72 hours), effectiveness, safety, dosing, mechanism of action (e.g., use after unprotected sex, condom rupture), and limitations (e.g., protection against STIs, potential for failure). The 13-item knowledge tool was adapted from existing literature on EC knowledge in African university settings,22,24 with modifications for local relevance. Items underwent expert review by reproductive health specialists at Njala University for content validity and were piloted among a small group of students (n=20) to ensure clarity, with minor wording adjustments made.
The final section was based on attitudes and perception-related assessment regarding EC using a set of 9 statements with “Agree,” “Disagree,” or “Don’t Know” options. These statements explored common myths (e.g., “EC use will cause infertility”), social perceptions (“EC creates a lack of confidence between partners”), religious acceptance, and support for broader access. The full questionnaire is provided as Supplemental File 1: Study Questionnaire.
Study variables and outcome measures
The primary outcome variable was ever-use of emergency contraception, a binary variable with the options ‘Yes’ or ‘No’. Secondary outcomes included recent use of EC, defined as use within a mutually exclusive stated period (four weeks, three months, six months, and twelve months), and repeat use, defined as using EC two or more times in the last six months.
For regression analyses, binary outcomes were coded as follows: ever-use of emergency contraception (EC) was coded as 1 for ‘Yes’ and 0 for ‘No’; recent use of EC (within the past three months) was coded as 1 for ‘Yes’ and 0 for ‘No'.
To assess knowledge and attitudes, composite scores were created and analysed both as continuous measures (for correlation) and dichotomised variables (for regression). The knowledge score was calculated by summing the number of correct answers to a core set of knowledge items. Knowledge items had response options ‘True,’ ‘False,’ and ‘Don’t Know’ (coded as 1 if correct, 0 if incorrect or ‘Don’t Know’). The total obtainable knowledge score was 13 (100%), representing the maximum possible score if all 13 knowledge items were answered correctly. The knowledge scores were then categorised into ‘Good knowledge’ = 1 and ‘Poor knowledge’ = 0; based on the mean score (48.6%), which served as the cut-off point, justified by the exploratory nature of the study and lack of prior validated cut-offs in this context. The internal consistency of the knowledge scale was assessed using Cronbach’s Alpha, which was found to be 0.789.
Similarly, an attitude score was generated by summing responses to the attitude and perception-related items. Items were coded such that a higher score indicated a more positive attitude towards EC. For positively worded questions, ‘Agree’ was coded as 1 and ‘Disagree’ as 0; for negatively worded items, the coding was reversed (‘Agree’ = 0, ‘Disagree’ = 1). ‘Don’t Know’ responses were coded as 0.5 to represent a neutral stance for both positive and negatively worded questions, and reverse coding did not apply to this. This approach created a quasi-continuous scoring system rather than a strictly dichotomous one, and we acknowledge that assigning 0.5 to ‘Don’t Know’ departs from conventional psychometric practice and may introduce measurement imprecision. The total obtainable attitude score was 9 (100%), with Cronbach’s Alpha of 0.661. For regression analyses, scores were dichotomised based on the mean attitude score (46.6%), with participants scoring above the mean categorised as having a ‘Positive attitude’ (coded as 1, outcome of interest) and those scoring at or below the mean categorised as having a ‘Negative attitude’ (coded as 0). Intermediate scores, particularly those influenced by ‘Don’t Know’ responses, should be interpreted cautiously as reflecting uncertainty rather than a definitive positive or negative stance.
Data management
Completed questionnaires were reviewed for completeness of responses and consistency before data entry. The data were entered, cleaned, and analysed using the Statistical Package for the Social Sciences (SPSS) version 25.0. Data cleaning involved standardising categorical labels and managing missing values.
Statistical analysis
Descriptive statistics summarised sample characteristics, with frequencies, percentages, and 95% confidence intervals (CIs) reported for categorical variables using the Wilson score interval method. Multivariable logistic regression models were used to assess binary outcomes, including ever-use and recent use of EC, knowledge, and attitudes. Outcome coding and reference categories were explicitly defined and applied consistently across all models to ensure clarity: ever-use of EC (Yes = 1, No = 0; Yes as the outcome of interest), recent use (Yes = 1, No = 0; Yes as the outcome of interest), knowledge (good = 1, poor = 0; good knowledge as the outcome of interest), and attitude (positive = 1, negative = 0; positive attitude as the outcome of interest). This consistent coding was maintained across all tables and narrative interpretations to ensure directional clarity.
Confounder selection was based on literature review and univariate associations (p<0.2), with adjusted models including age, academic year, residence, religion, marital status, knowledge, and attitude as appropriate. Missing data were handled via complete case analysis, with minimal missingness (<5%) for primary outcomes. Model diagnostics included Hosmer-Lemeshow goodness-of-fit test (p>0.05 indicating adequate fit), Nagelkerke pseudo R2, and classification accuracy. Multicollinearity was assessed using variance inflation factors (VIF<5). Correlation between knowledge and attitude scores was assessed using Pearson’s (assuming approximate continuity) and Spearman’s rank correlation (for robustness given bounded scores). A p-value <0.05 was considered statistically significant. All statistical outputs were double-checked for accuracy in point estimates and confidence intervals to ensure reliability of reported results.
Ethical considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of Njala University (Approval ID: NU/IRB/020-2024). Written informed consent was secured from all participants before questionnaire administration. The consent form explained the study’s objectives, voluntary nature of participation, and the right to withdraw at any time without consequence. For participants under 18 years, assent was obtained directly, with an explicit waiver for parental/guardian consent approved by the IRB, justified by the sensitive nature of the topic (reproductive health) and the potential for parental involvement to deter participation or breach confidentiality. No personal identifiers were collected to ensure confidentiality and anonymity, and data were stored securely, used solely for research purposes. The study adhered to the ethical principles of the Declaration of Helsinki and international standards for research involving human participants.
Results
Sociodemographic characteristics
Sociodemographic characteristics (N=366).
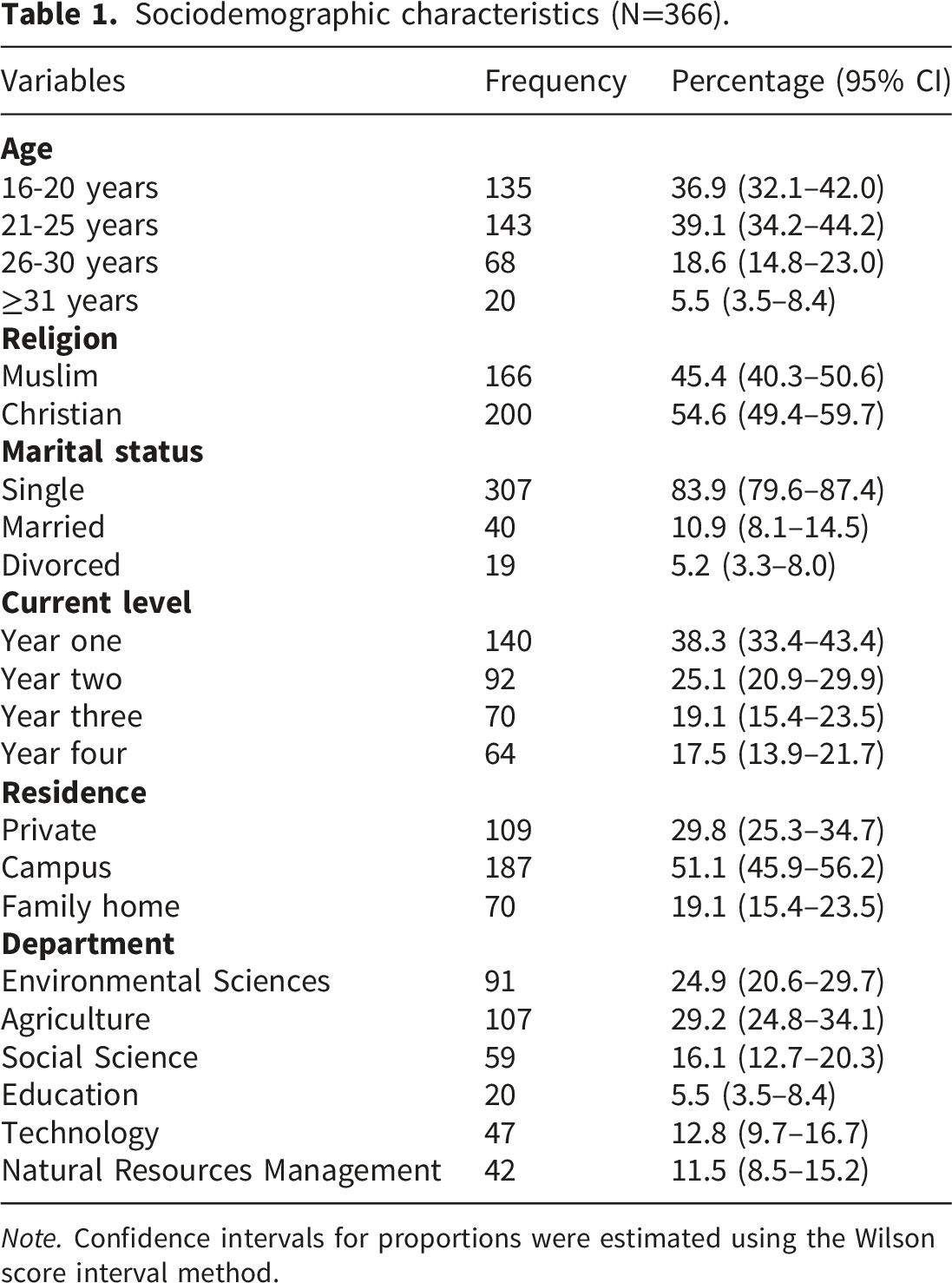
Note. Confidence intervals for proportions were estimated using the Wilson score interval method.
Emergency contraceptive utilisation
Emergency contraceptive utilisation pattern.
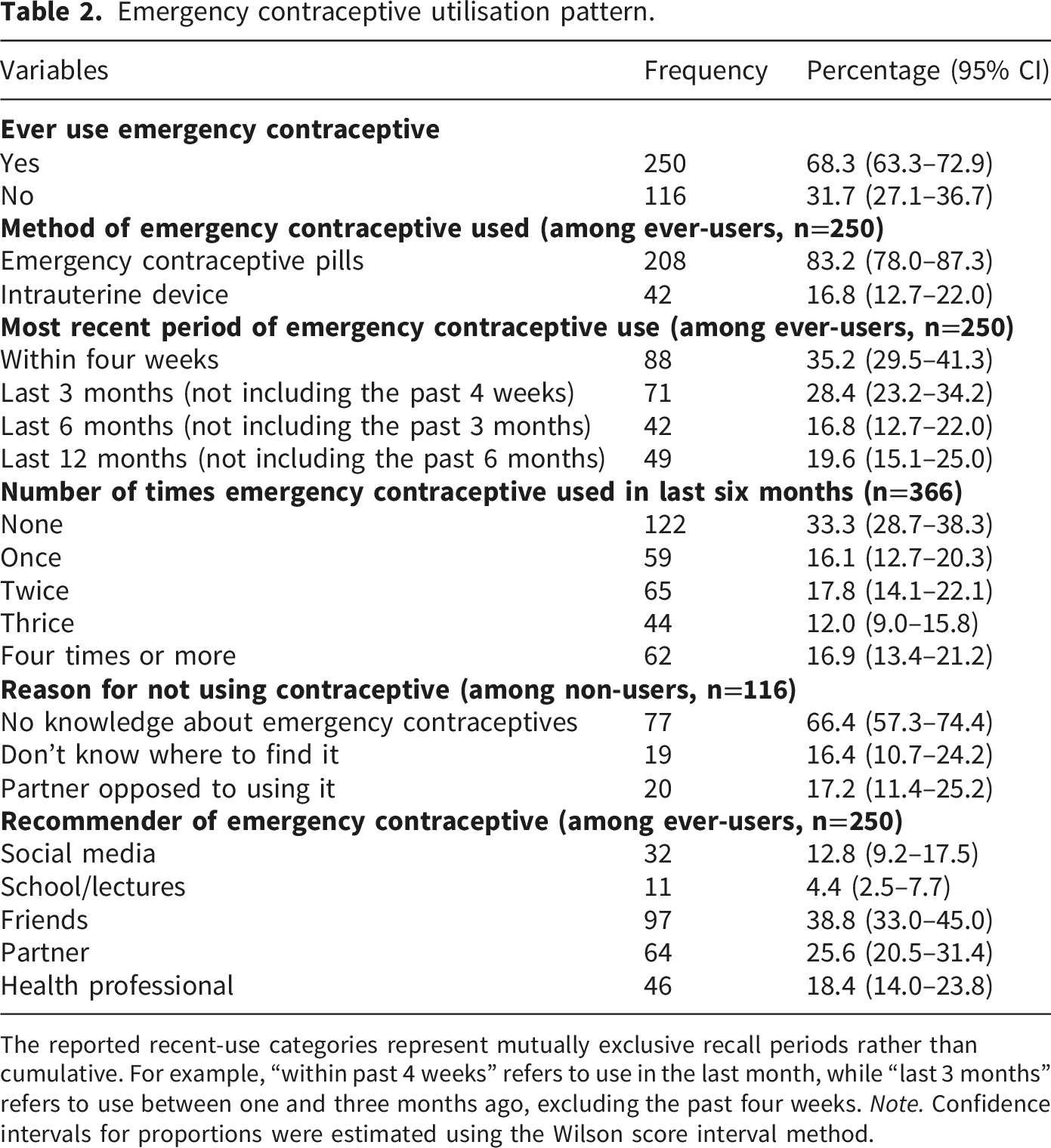
The reported recent-use categories represent mutually exclusive recall periods rather than cumulative. For example, “within past 4 weeks” refers to use in the last month, while “last 3 months” refers to use between one and three months ago, excluding the past four weeks. Note. Confidence intervals for proportions were estimated using the Wilson score interval method.
Sources of recommendation and barriers
When asked who recommended EC, respondents most often cited friends (38.8%), followed by partners (25.6%) and health professionals (18.4%). Social media (12.8%) and school or lectures (4.4%) were less common sources, indicating that peer networks and health providers play key roles in influencing EC uptake. Among non-users, the reasons for not using EC were lack of knowledge about EC (66.4%), partner opposition (17.2%), and not knowing where to find it (16.4%) (Table 2).
Factors associated with EC utilisation (ever use)
Factors associated with emergency contraceptive utilisation.
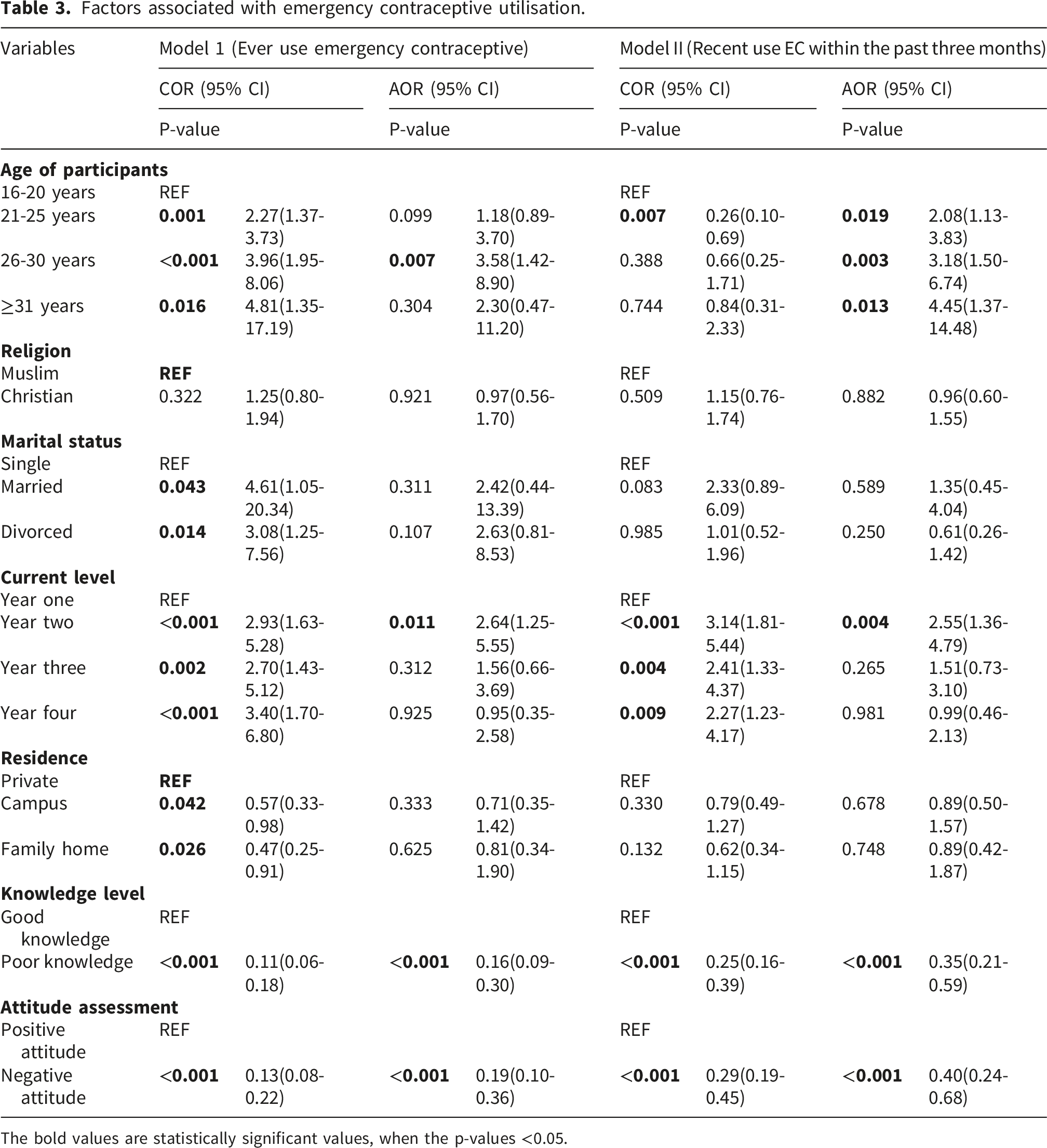
The bold values are statistically significant values, when the p-values <0.05.
Factors associated with recent EC use
In model II, which assesses the factors associated with EC use within the past three months, older age groups were more likely to report recent use compared with the 16–20-year reference group. Adjusted odds increased with age: 21–25 years (AOR 2.08; 95% CI 1.13–3.83; p=0.019), 26–30 years (AOR 3.18; 95% CI 1.50–6.74; p=0.003), and ≥31 years (AOR 4.45; 95% CI 1.37–14.48; p=0.013). Students in year two also had higher odds of recent use compared with year one (AOR 2.55; 95% CI 1.36–4.79; p=0.004). Consistent with the ever-use model, students with poor knowledge had significantly lower odds of recent EC use compared to those with good knowledge (AOR 0.35; 95% CI 0.21–0.59; p<0.001), and students with negative attitudes had significantly lower odds of recent EC use compared to those with positive attitudes (AOR 0.40; 95% CI 0.24–0.68; p<0.001). Religion and residence were also not associated with recent use in the adjusted analyses. Further information is provided in Table 3.
Knowledge assessment
Factors associated with knowledge about Emergency contraceptives.
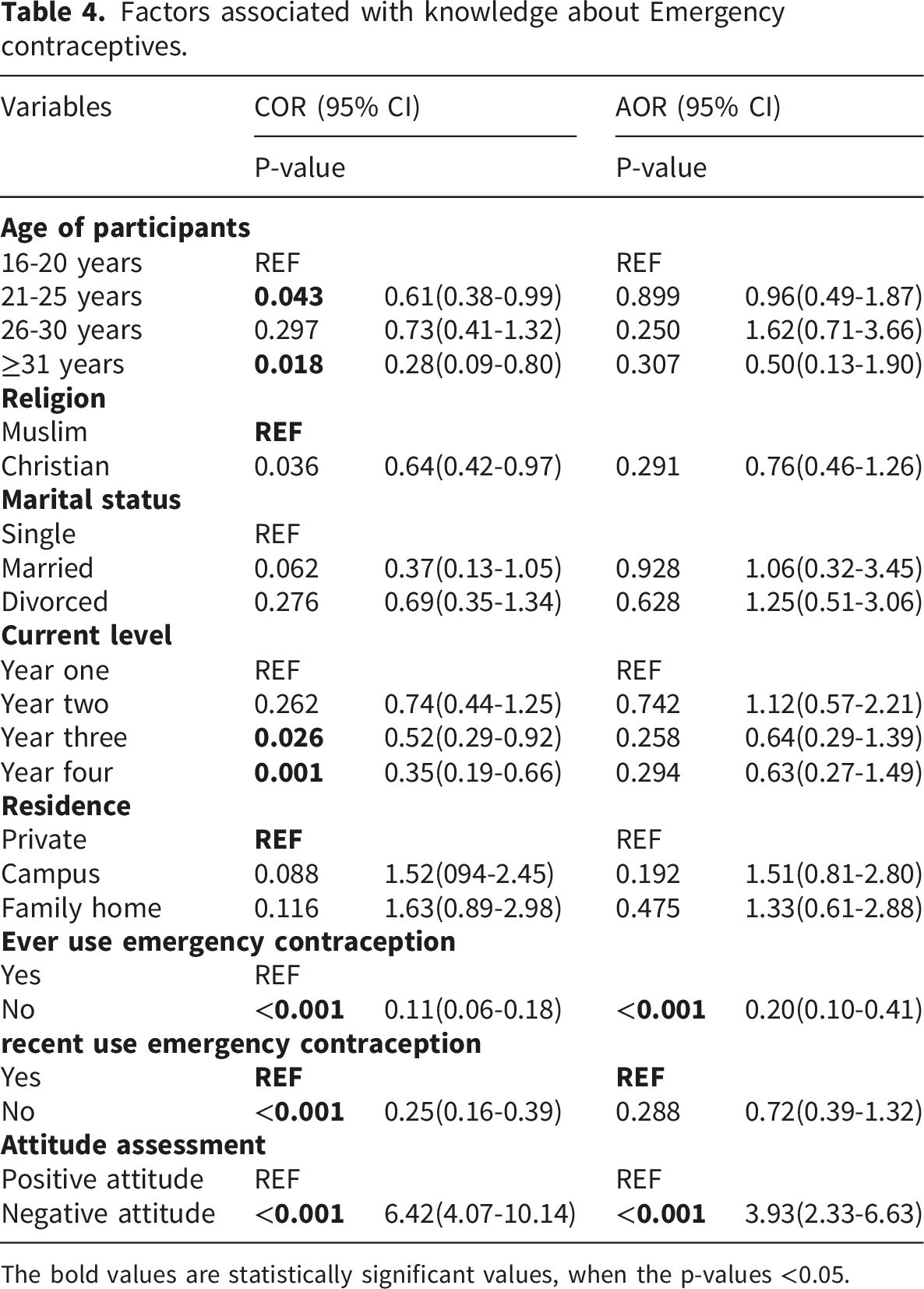
The bold values are statistically significant values, when the p-values <0.05.
Attitude assessment
Correlates of attitude towards Emergency contraceptives.
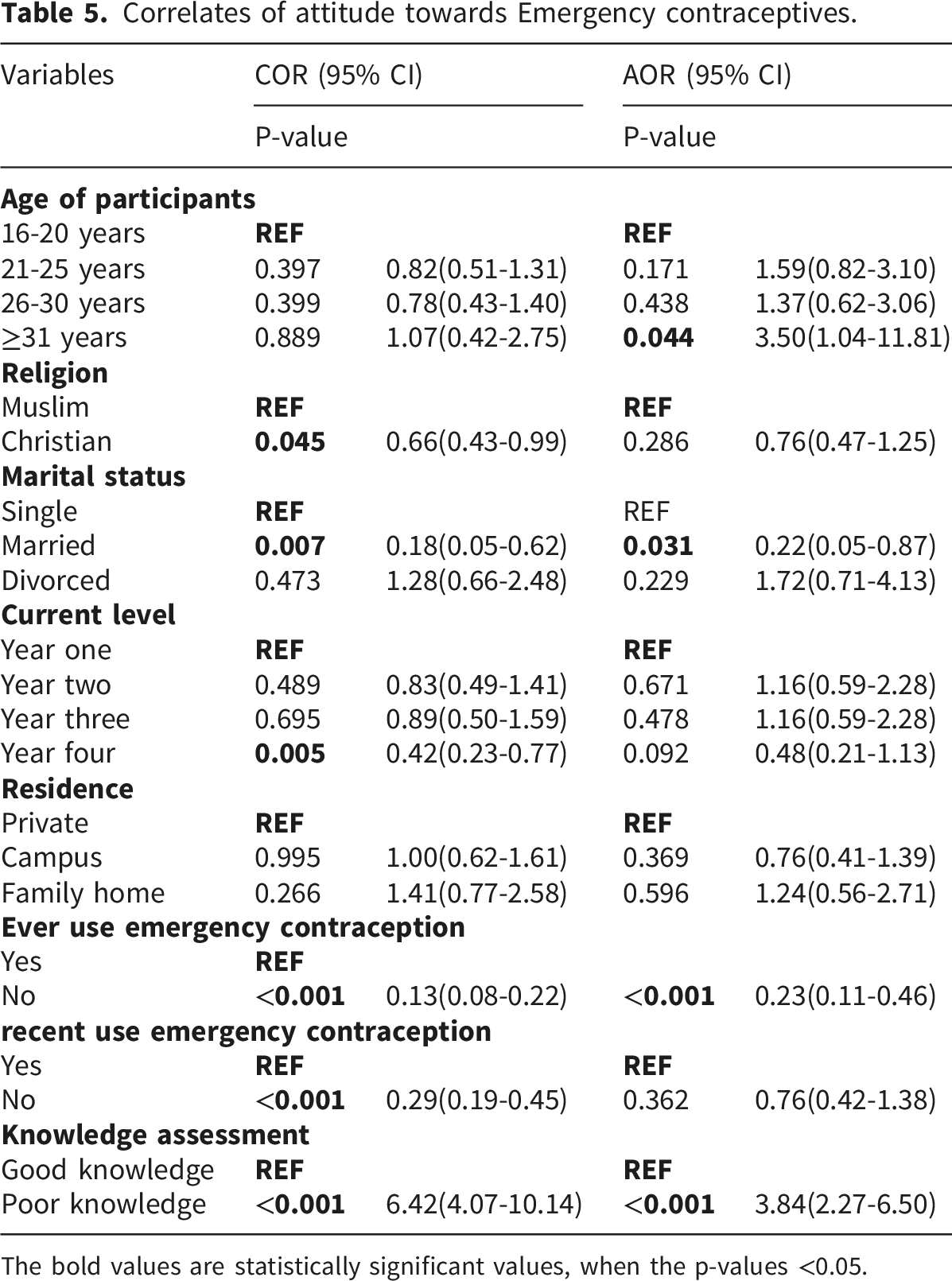
The bold values are statistically significant values, when the p-values <0.05.
Correlation between knowledge and attitudes
Knowledge and attitudes towards EC were strongly correlated, as demonstrated by Pearson’s correlation (r=0.659; p<0.001) and Spearman’s rank correlation (rho=0.611; p<0.001), confirming the robustness of the relationship. The multivariable regression models corroborated this relationship. In the Knowledge model (Table 4), negative attitudes were associated with higher odds of good knowledge (AOR 3.93; 95% CI 2.33–6.63; p < 0.001). In the Attitude model (Table 5), poor knowledge was associated with higher odds of a positive attitude (AOR 3.84; 95% CI 2.27–6.50; p < 0.001).
Discussion
This cross-sectional study among female university students in Sierra Leone found a high prevalence of ever-use of emergency contraception (EC) alongside frequent recent and repeated use. Despite this widespread utilisation, overall knowledge and attitudes toward EC were moderate and evenly split, and poorer knowledge and negative attitudes were consistently associated with lower odds of EC use. These findings have important implications for campus-based reproductive health services and national strategies to reduce unintended pregnancy among young adults.
Our observed ever-use prevalence of 68.3% is higher than many reports from university populations in sub-Saharan Africa, where awareness is often high, but ever-use varies widely, typically between 20% and 50% in Nigerian, Ghanaian, Ethiopian, and Kenyan settings.22–25 The proportion reporting EC use in the past three months and repeated use over the last six months indicates that, within this setting, EC is not only known but actively relied upon by a substantial subset of students. Such reliance improves familiarity with these products; however, the persistence of misconceptions among non-users and those with negative attitudes suggests that knowledge gaps are associated with reduced likelihood of appropriate EC use.12,26 The predominance of EC pills over copper IUDs aligns with global and regional patterns, given easier access to levonorgestrel pills and the need for clinical insertion for IUDs.12,26 The low contribution of formal academic channels to EC recommendation, contrasted with the influence of peers, partners, and health professionals, underscores the social dynamics of contraceptive decision-making among university students and suggests underutilised opportunities for structured health education within institutions.22,23
The mean knowledge score was nearly 50%, with an almost even split between good and poor knowledge. This pattern mirrors prior studies showing high awareness of emergency contraception but persistent knowledge gaps, particularly in areas such as timing, dosing, mechanism of action, and lack of protection against sexually transmitted infections (STIs).18–20,22–25 Students who had never used EC had markedly lower odds of good knowledge.
Conversely, there was a strong association between good knowledge and higher odds of ever-use and recent use of emergency contraception, highlighting a reinforcing cycle in which knowledge promotes uptake, and use consolidates knowledge, underscoring the need for education alongside accessible, stigma-free services. 28 In the knowledge analysis, negative attitudes were linked to significantly higher odds of good knowledge (AOR 3.93; 95% CI 2.33–6.63; p < 0.001). Although counterintuitive, this finding reflects the broader paradox observed across analyses, suggesting that in socially contested contexts, individuals may acquire detailed knowledge even while holding unfavourable views about EC. Conversely, those with positive attitudes may rely more on normative acceptance rather than detailed knowledge. Knowledge gaps and unfavourable attitudes may be mutually reinforcing, a relationship that warrants further exploration through longitudinal or qualitative designs. In particular, well-documented misconceptions regarding infertility and the conflation of EC with abortion remain deterrents capable of shaping unfavourable attitudes and limiting utilisation.18,21
Attitudes toward EC were nearly evenly split between positive and negative. Contrary to a study done in Botswana, 29 in the present study, poor knowledge was unexpectedly linked to higher odds of positive attitudes when compared to good knowledge, suggesting that favourable attitudes were not necessarily grounded in accurate information. This is a concern, as positive attitudes built on misconceptions may not reliably translate into appropriate EC use. Participants who had never used EC were less likely to hold a positive attitude compared to ever-users (AOR 0.23), consistent with evidence that prior experience fosters familiarity and acceptance.18–21,24 The association of married status with lower likelihood of positive attitudes may reflect normative preferences for routine methods within stable relationships, perceived moral considerations, or differential exposure to EC-related messaging.19,21 Older participants (≥31 years) had higher odds of a positive attitude compared to younger participants (AOR 3.50), possibly reflecting greater life experience, longer exposure to reproductive health information, and stronger motivation to avoid unintended pregnancies given competing life responsibilities. However, this finding should be interpreted with caution, given the small size of that subgroup (n=20).
Knowledge and attitudes were significantly and positively correlated, with both Pearson’s and Spearman’s tests indicating a strong association. However, the multivariable regression models revealed paradoxical associations once the composite scores were dichotomised at the mean and adjusted for covariates. In the knowledge model, students classified as having negative attitudes had higher odds of good knowledge, while in the attitude model, students with poor knowledge had higher odds of a positive attitude.
This apparent divergence reflects methodological differences: correlation analyses capture the overall linear relationship between continuous scores, whereas regression analyses dichotomised the variables into binary categories and controlled for sociodemographic and behavioural covariates. The non-standard coding of ‘Don’t Know’ responses as 0.5 may also have contributed to intermediate scores that reflect uncertainty rather than definitive positions, influencing regression outcomes. Taken together, these findings demonstrate a complex and paradoxical interrelation, where favourable attitudes may arise despite limited accurate knowledge, and stronger knowledge does not necessarily translate into more positive views. This dynamic reflects the social, moral, and cultural contexts in which EC is understood among young women in Sierra Leone and underscores the limitations of knowledge-only interventions in shifting attitudes.
Multivariable analyses identified older age and being in the second academic year as factors associated with EC use, whereas residence and religion were not associated after adjustment. Age gradients in EC use have been reported across sub-Saharan African settings and may reflect cumulative sexual experience, autonomy in health decision-making, and greater ability to navigate access points such as pharmacies and clinics.22–25 The specific elevation of use in year two could denote a period of increased sexual activity or transition in living arrangements and social networks, though attenuated associations in later years suggest nuanced cohort dynamics that warrant qualitative exploration. The consistent negative associations of poor knowledge and negative attitudes with both ever-use and recent use reinforce the centrality of informational and perceptual determinants. Notably, lack of knowledge, partner opposition, and uncertainty about where to obtain EC were the leading reasons for non-use, mapping directly onto modifiable barriers amenable to intervention through education, partner engagement, and service visibility.12,19,20 Partner opposition, reported by 17.2% of non-users, may reflect cultural norms around male decision-making in relationships, misconceptions about EC (e.g., infertility fears), or concerns about fidelity, as noted in qualitative studies from similar West African contexts. 19 In Sierra Leone, where gender dynamics often influence reproductive choices, engaging partners through targeted education could reduce barriers to EC access.
Taken together, these findings emphasise that high EC utilisation does not necessarily equate to adequate knowledge or uniformly positive attitudes. Interventions should therefore adopt a multifaceted approach: delivering accurate, myth-busting information on EC timing, dosing, mechanism, and STI non-protection; normalising EC as a safe, postcoital method that does not interrupt established pregnancy; and embedding counselling pathways to facilitate transition to effective routine contraception, including long-acting reversible contraceptives (LARC) where appropriate.12,17,26 Peer-led education and collaboration with campus health services may be particularly impactful, given the prominent roles of friends and health professionals as recommenders in this context.22,23 Addressing partner opposition through inclusive communication strategies could further reduce barriers to timely EC use.19,21 Strengthening service navigation, clear information on where and how to obtain EC, and routine methods can improve timely access and reduce reliance on repeated EC for ongoing pregnancy prevention.12,26
Our results contribute to a sparse evidence base on EC among university students in Sierra Leone, a country with high maternal mortality and documented challenges related to unintended pregnancy and unsafe abortion.8,9,30 By quantifying prevalence, characterising knowledge and attitudes, and identifying associated factors of EC use, this study provides actionable insights for campus health programs and national policy. Integration of EC within broader sexual and reproductive health services, ensuring youth-friendly, confidential access, aligns with international guidance and has the potential to reduce unintended pregnancies and their sequelae among young women.12,17
Limitations
Several limitations must be acknowledged. First, the cross-sectional design precludes causal inference; associations between knowledge, attitudes, and EC utilisation may reflect reverse causation (e.g., users may acquire better knowledge through experience). Second, self-reported behaviours are subject to recall and social desirability bias, particularly for sensitive topics like sexual activity and contraceptive use. Third, the use of convenience sampling at a single university is a fundamental design limitation that restricts the generalisability of findings to other institutions, regions, or populations in Sierra Leone. This study is explicitly exploratory in nature, and findings should be interpreted as context-specific to the sampled participants at Njala University. Probability-based, multi-site sampling designs are recommended for future confirmatory research. Additionally, the attitude scale’s treatment of ‘Don’t Know’ responses as neutral (coded 0.5) represents a deliberate but non-standard psychometric decision. While this approach was chosen to avoid penalising genuine uncertainty, it may artificially inflate attitude scores and affect the internal validity and comparability of the attitude construct. Future studies should employ validated scales with clearly defined response options and higher internal consistency to improve measurement precision and enable cross-study comparisons. Fourth, a formal power analysis for sample size calculation was not performed, which may limit statistical power to detect smaller effect sizes. Fifth, the adopted attitude assessment scale, originally labelled as ‘attitudes’, comprised both evaluative items and misconception-based beliefs, which may blur construct boundaries. Although the label was revised to ‘perceptions and attitudes’ to reflect this mixed content, the absence of subscale separation remains a limitation and underscores the need for future psychometric refinement. Finally, the attitude scale’s internal consistency was modest (Cronbach’s alpha 0.661), suggesting scope for item refinement to better capture dimensions like stigma and moral beliefs.
Future research
Future research should include item-level analyses to pinpoint specific misconceptions, qualitative studies to explore social and partner dynamics influencing EC decisions, and intervention trials to test peer-led education, provider training, and service-navigation aids. Evaluations that integrate EC access with counseling and provision of routine methods, including LARC, could assess whether reliance on EC decreases and overall contraceptive effectiveness improves over time. Multi-institutional studies would enhance generalisability and inform national strategies.
Conclusion
In this exploratory study, EC use among female university students at Njala University, Sierra Leone, was found to be widespread and often recent or repeated, yet knowledge and attitudes remained moderate and paradoxically interrelated. Poor knowledge and negative attitudes consistently reduced the likelihood of EC use, while prior utilisation experience reinforced understanding and acceptance. These findings emphasise that high utilisation does not equate to informed or uniformly positive engagement. However, findings are context-specific and should not be generalised beyond the sampled population without further confirmatory research. Addressing persistent myths, engaging peer and partner networks, and improving service visibility, while facilitating transitions to effective routine contraception, should be priorities for campus health programs and national policy. Such efforts align with global guidance on EC and have the potential to reduce unintended pregnancy and its adverse consequences among young women.
Supplemental material
Supplemental material - Emergency contraception among female university students in Sierra Leone: An exploratory study of use, knowledge, attitudes, and associated factors
Supplemental material for Emergency contraception among female university students in Sierra Leone: An exploratory study of use, knowledge, attitudes, and associated factors by Augustus Osborne, Camilla Bangura and Ahmed Vandy in Women’s Health.
Supplemental material
Supplemental material - Emergency contraception among female university students in Sierra Leone: An exploratory study of use, knowledge, attitudes, and associated factors
Supplemental material for Emergency contraception among female university students in Sierra Leone: An exploratory study of use, knowledge, attitudes, and associated factors by Augustus Osborne, Camilla Bangura and Ahmed Vandy in Women’s Health.
Footnotes
Acknowledgements
We are grateful to the female students at Njala University, Sierra Leone, who participated in the study.
Ethical considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of Njala University (Approval ID: NU/IRB/020-2024). Written informed consent was secured from all participants before questionnaire administration. For participants under 18 years, assent was obtained directly, with an explicit waiver for parental/guardian consent approved by the IRB, justified by the sensitive nature of the topic and potential confidentiality concerns. The study adhered to the Declaration of Helsinki and international ethical standards.
Author contributions
AO and CB contributed to the study design and conceptualisation. AV performed the analysis. AO developed the initial draft. All authors critically reviewed the manuscript for intellectual content, read and amended drafts, and approved the final version. AV had the final responsibility to submit it for publication. No Generative Artificial Intelligence (AI) tools were used in creating this manuscript; all content was authored by the listed contributors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data used for this study is available upon request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.