
Abstract
We study intentions and behavior associated with use of the oral supplement of the EyeScience Computer Eye Strain formula for computer vision syndrome. Participants (n = 588) completed a survey with variables including Theory of Planned Behavior content, demographics, symptoms, behaviors related to supplements, and eye devices placed in eyes. We found that 4.9% used the EyeScience Computer Eye Strain formula. Variables associated with intentions included increased attitudes, social norms, confidence to use, symptoms, use of eye supplements, and preference to swallow an eye supplement instead of using eye drops. Variables associated with use included increased intentions, received treatment for computer vision syndrome, and used eye drops for computer vision syndrome. We recommend that marketers of oral eye treatments for computer vision syndrome consider as part of their advertising campaign including content about computer vision syndrome related symptoms. Also, those who previously used eye drops are a potentially receptive market segment.
Introduction
Computer vision syndrome is an ocular condition that results from the extended use of computers. 1 The prevalence of computer vision syndrome ranges from 25 to 93%. 2 Those with computer vision syndrome experience symptoms such as headaches, eyestrain, dry eyes, burning sensation in the eye, pain in the neck, back and shoulder areas, and double vision. 3 Limiting the amount of time spent in front of a computer, using certain angles to view computers, having proper lighting, using proper seat posture, and using appropriate viewing distances can reduce or even eliminate these symptoms.1,3
Dry eye syndrome is discomfort to the eye that is caused by an abnormality of tear film and excessive tear evaporation. 4 Temporary relief may occur through the use of artificial tears. Essential fatty acids such as omega-3 and omega-6 may increase the tear film lipid layer and reduce tear evaporation. Essential fatty acids also have anti-inflammatory properties. 4 There are mixed results about the benefits of omega-3 and omega-6 fatty acids with regard to improving dry eyes. One clinical trial of those with Sjogren’s syndrome reports that oral supplementation of omega-6 fatty acids as compared to placebo significantly reduced eye dryness over one month and this was maintained in the 15-day follow-up after omega-6 fatty acid discontinuation. 5 However, other clinical trials have different findings. Another clinical trial of those with dry eye syndrome assessed the use of oral supplementation three times daily of either omega-3 or omega-6 fatty acids versus placebo. 6 The study found that HLA-DR-positive cells percentage did not significantly decrease between the groups when using the full sample, while there was a significant greater decrease for the fatty acid group when using a per-protocol analysis. Also, there were significant decreases in fluorescence intensity for HLA-DR AUF in the fatty acid group as compared to placebo but no significant differences between the groups for global subjective dry eye score. In a pilot study comparing omega-3 fatty acid supplementation versus placebo, although significant trends were seen for a number of outcomes including tear flow and tear volume, this did not meet the level for formal statistical significance. 7
Carotenoids such as lutein and zeaxanthin have potential benefits for controlling vision and visual acuity and aid in the protection of eye photo damage. 8 One clinical trial of oral supplementation compared adding omega-long-chain polyunsaturated fatty acids to those taking both zeaxanthin and lutein versus a control group of those taking just zeaxanthin and lutein over six months. There were no significant differences between the groups for serum zeaxanthin concentration, serum lutein concentration, and best-corrected visual acuity. 9 A clinical trial of age-related macular degeneration patients compared oral supplementation of zeaxanthin, zeaxanthin + lutein, and lutein over one year. 10 For foveal vision, the zeaxanthin group had significantly greater visual acuity than the zeaxanthin + lutein group, followed by the least visual acuity for the lutein group. Also, lutein had better outcomes for foveal vision as compared to the zeaxanthin and zeaxanthin + lutein groups. Another type of carotenoid is astaxanthin which has a similar structure to lutein and zeaxanthin but is a stronger antioxidant and has a greater UV-light protection. 11 A review of astaxanthin as it relates to vision and eye fatigue reports that taking 6 mg/day results in improved visual sharpness in both healthy and non-healthy individuals. 12
Individuals may find it beneficial to use oral supplements containing carotenoids. There is an oral soft gel supplement named the EyeScience Computer Eye Strain Formula. Each gel contains 200 mcg zeaxanthin, 4 mg lutein, and 6 mg of astaxanthin. 13 The company markets the product to consumers who are concerned about computer vision syndrome. We are not aware of any studies on intentions for use of oral supplements in general for computer vision syndrome. We are also not aware of any studies on the intention to use the EyeScience Computer Eye Strain Formula nor on use of the EyeScience Computer Eye Strain Formula. We study variables associated with both intention and use of the EyeScience Computer Eye Strain Formula. We include a number of different variables as possible predictors from the areas of demographics, symptoms, behaviors related to supplements, and eye devices placed in eyes. We also include variables based upon the psychological theory of the Theory of Planned Behavior.
Method
Participants
We approached 660 students to participate in our survey at a public college located in New York City. Of those approached, 20 declined to participate. Also, 20 completed surveys were deemed invalid. The response rate of 93.9% was computed from the 620 completed surveys [(620/660) × 100%]. In our sample, we excluded 32 people above the age of 36 to have a young adult sample. The data were analyzed from 588 participants. The study received IRB approval and was conducted according to the ethical framework of the Declaration of Helsinki. Informed consent was obtained from the participants. All participants were surveyed from April 2012 through August 2012.
Participants completed anonymous surveys in the college library, classes, and cafeteria. The survey began with an introductory description of both computer vision syndrome and the EyeScience Computer Eye Strain Formula. This content was based upon the marketing brochure describing the product. This content included description of computer vision syndrome and potential treatment approaches. It also included information about the soft-gel capsule EyeScience Computer Eye Strain Formula, the active ingredients in the capsule, and that it is available for purchase at retailers such as CVS and Rite Aid. A disclosure was included that the supplement was not a prescription medication and that this information was not approved by the Food and Drug Administration.
Measures
Theory of Planned Behavior
The Theory of Planned Behavior variables included intentions, attitudes, social norms, and behavioral control. Questions were created based upon the manual for creating a survey using the Theory of Planned Behavior. 14
Intentions
The intentions scale consists of three items. A Likert-style scale was used to measure all the items with a range from 1 = strongly disagree to 7 = strongly agree. A sample item is, “I expect to use the EyeScience Computer Eye Strain Formula for my eyes.” The total score was calculated by adding all three items. Greater scores indicate greater intentions. Cronbach alpha reliability in this sample was 0.92.
Attitudes
The attitudes scale consists of four items. A Likert-style scale was used to measure all the items with a range from 1 to 7 with negative and positive attitudes as the endpoints. Two items were reverse coded to be in the direction of 7 = positive. All items had the stock phrase of “Using the EyeScience Computer Eye Strain Formula for my eyes is.” A sample positive endpoint had harmful = 1 and beneficial = 7. The total score was calculated by adding all four items. Greater scores indicate greater attitudes. Cronbach alpha reliability in this sample was 0.69.
Social norms
The social norms scale consists of three items. A Likert-style scale was used to measure all the items with a range from 1 = strongly disagree to 7 = strongly agree. A sample item is, “It is expected of me that I use the EyeScience Computer Eye Strain Formula for my eyes.” The total score was calculated by adding all three items. Greater scores indicate greater intentions. Cronbach alpha reliability in this sample was 0.84.
Behavioral control
There were four behavioral control items. A Likert-style scale was used to measure all the items with a range from 1 = strongly disagree to 7 = strongly agree. A sample item is, “I am confident that if I wanted to I could use the EyeScience Computer Eye Strain Formula for my eyes.” Two items were reverse coded. These items could not be added together for a total score due to poor Cronbach alpha reliability.
Demographics
Age (years), sex (man, woman) and race/ethnicity (White, African American, Hispanic, Asian, South Asian, or other) were measured.
Symptom variables
With regard to symptom variables, there were 14 items asking about different specific symptoms of: eye strain, tired eyes, sore eyes, dry eyes, watery eyes, irritated eyes, contact lens problems, blurred vision, slowness of focus change, double vision, neck pain, back pain, shoulder pain, and headache. These symptoms were obtained from a review article on symptoms of computer vision syndrome. 15 A total score was calculated for the total number of symptoms. Another question asked about eye health condition, with the specific question of, “How would you describe the condition of your eyes?” ranging from 0 = excellent to 4 = poor. Another question asked if the participant currently or had previously received treatment for computer vision syndrome, with “yes” or “no” choices.
Behaviors related to supplements
There were a number of questions asking about behaviors related to supplements. Two questions were yes or no questions on “currently or had previously used eye supplements” and “currently or had previously used eye drops for computer vision syndrome.” Five questions used a Likert-style scale with a range from 1 = strongly disagree to 7 = strongly agree. These questions were, “use of a multivitamin is sufficient for my eye health,” “I typically use complementary/alternative medicine treatments for my health,” “I avoid supplements because I am concerned about possible side effects,” “I do not like using eye drops,” and “I would prefer taking an eye supplement that can be swallowed instead of eye drops being placed in my eyes.”
Eye devices placed in eyes
There were three separate yes/no questions about different types of eye devices placed in eyes. These were “I wear glasses for improving my vision,” “I wear contact lenses for improving my vision,” and “I wear contact lenses for cosmetic purposes.”
Use of EyeScience Computer Eye Strain formula
One yes/no question asked, “I currently have or have previously used the EyeScience Computer Eye Strain Formula for my eyes.”
Statistical analysis
Descriptive statistics of mean and standard deviation were used for the continuous variables and percentage and frequency for the categorical variables. Linear regression analysis studied the outcome of intentions to use the Eye Science Computer Eye Strain formula. Predictors included the Theory of Planned Behavior variables, demographic variables, eye symptom variables, behaviors related to supplements variables, eye device variables, and use of the Eye Science Computer Eye Strain formula. Logistic regression analysis studied the outcome of use of the Eye Science Computer Eye Strain formula. Predictors included all the above variables except for use of the Eye Science Computer Eye Strain formula. All analyses used IBM SPSS version 20. All p-values were two-tailed.
Results
Sample characteristics of 588 college students.
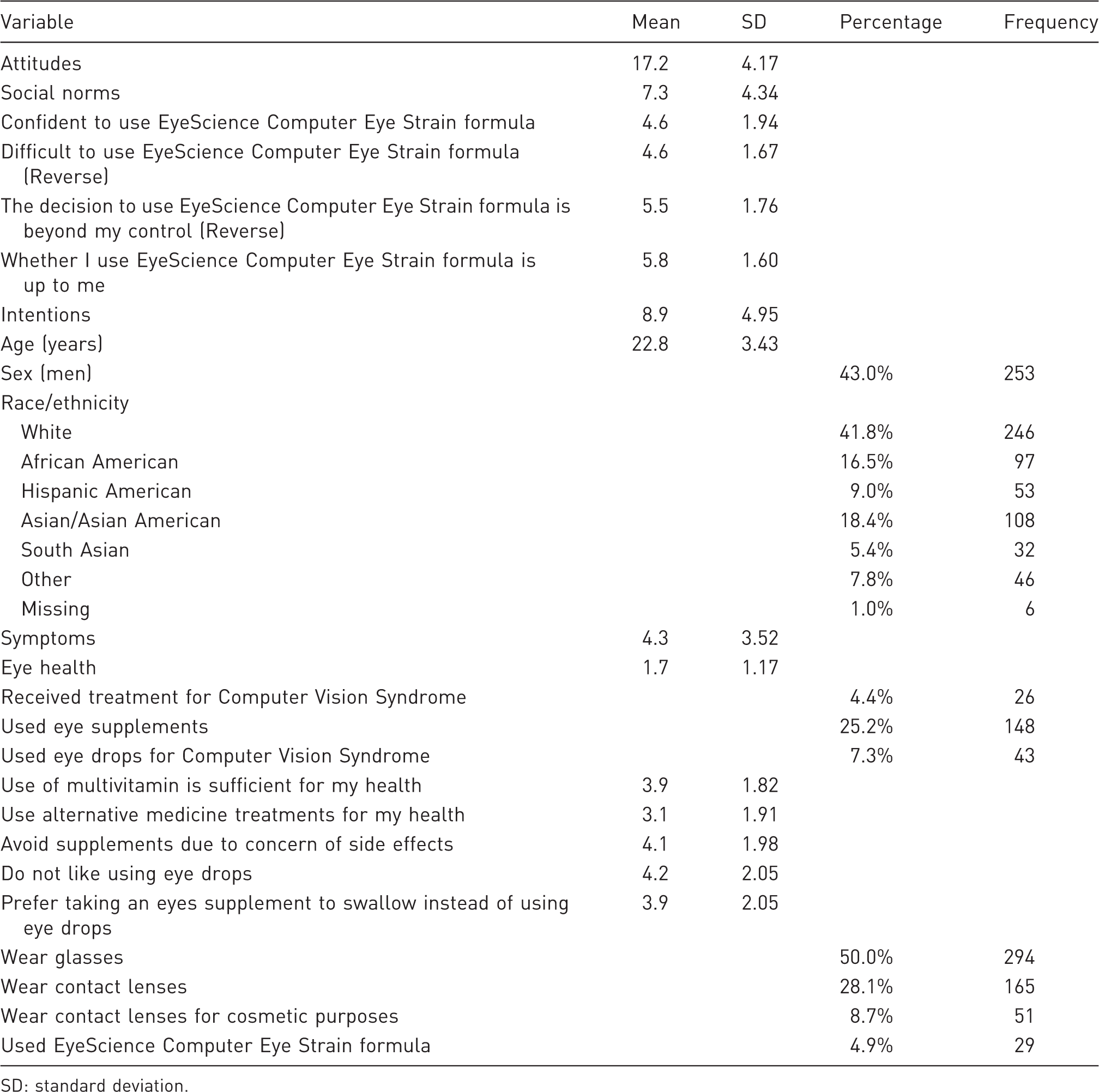
SD: standard deviation.
Linear regression analyses for intentions to use the EyeScience computer eye strain formula.
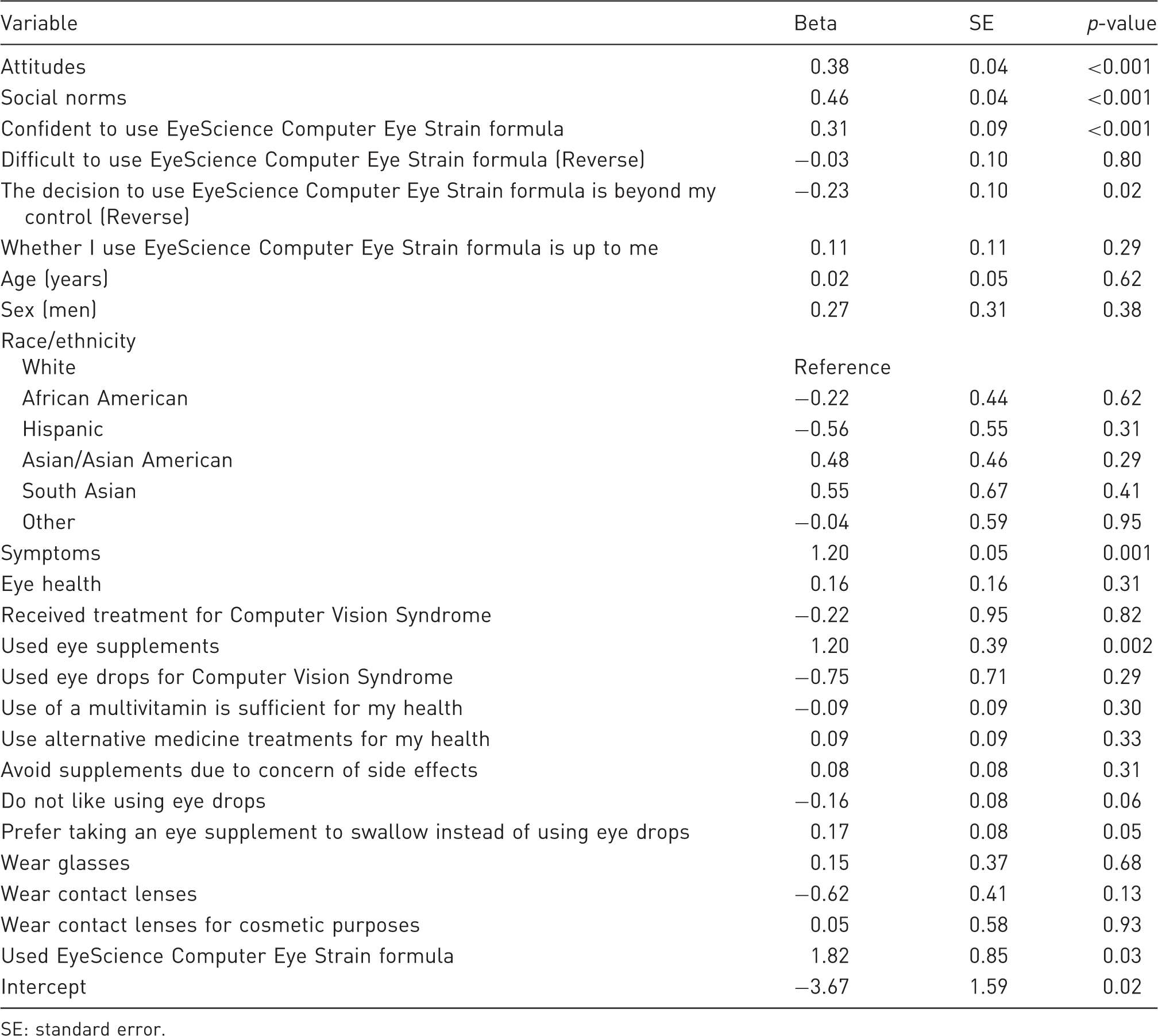
SE: standard error.
Logistic regression analyses for use of the EyeScience computer eye strain formula.
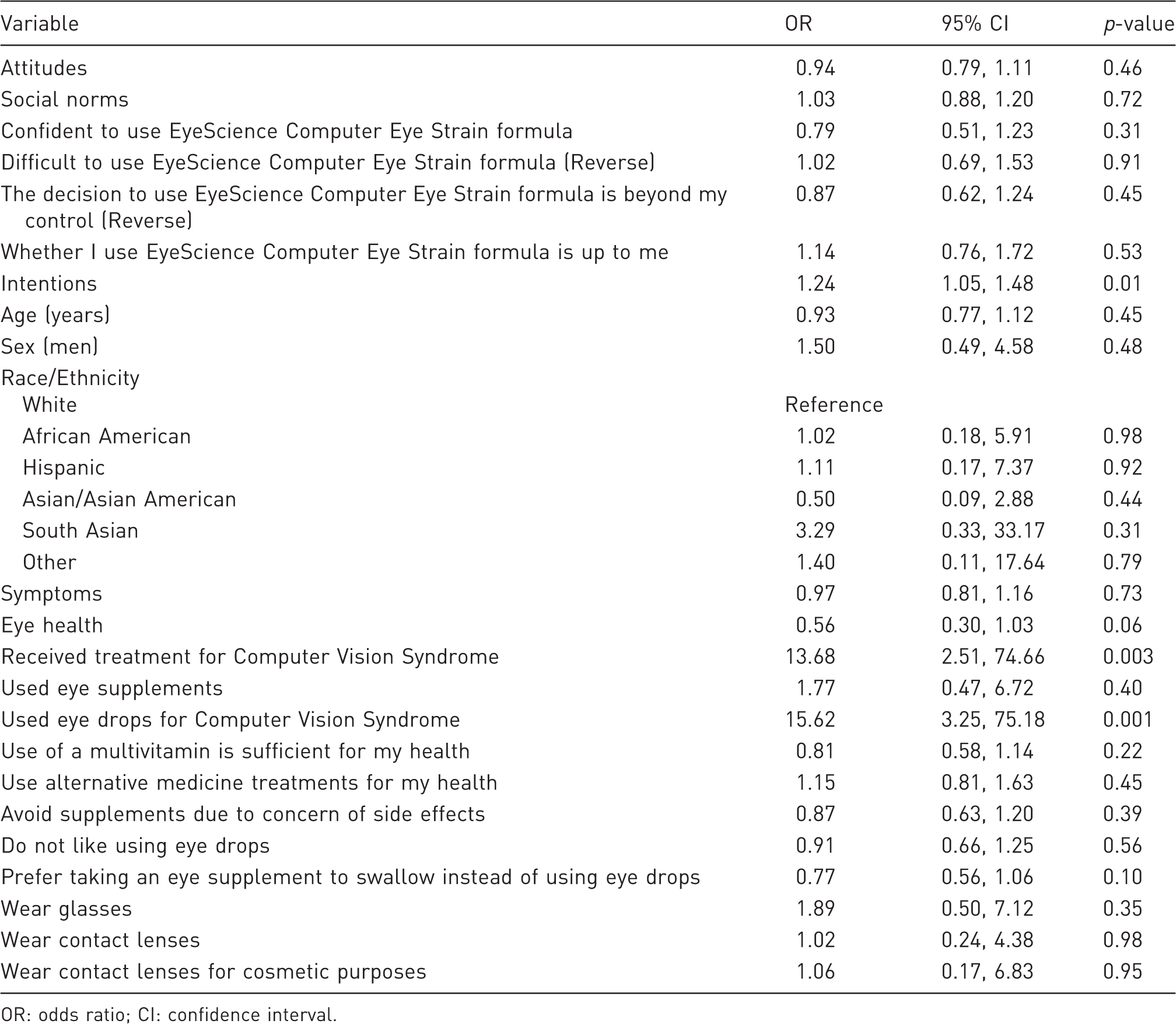
OR: odds ratio; CI: confidence interval.
Discussion
We found that 4.9% used the EyeScience Computer Eye Strain formula. With regard to the Theory of Planned Behavior variables, increased attitudes, increased social norms, increased confidence to use the Eye Science Computer Eye Strain formula, and decreased decision to use the Eye Science Computer Eye Strain formula is beyond my control (reverse coded) were all significantly associated with increased intentions to use the product. We found that an increase in symptoms and previously using eye supplements were significantly associated with increased intentions to use the product. Additionally, the preference to swallow an eye supplement instead of using eye drops and having previously used the Eye Science Computer Eye Strain formula were significantly associated with increased intentions to use the product. The pattern for variables associated with use of the Eye Science Computer Eye Strain formula was different from intentions to use. We found that increased intentions, those who received treatment for computer vision syndrome, and those who previously used eye drops for computer vision syndrome had significantly increased odds for use.
We found that the Theory of Planned Behavior variables of attitudes, social norms, and behavioral control were significantly associated with increased intentions to use the EyeScience Computer Eye Strain formula. The Theory of Planned Behavior has been previously used for eye-related topics. One study of purchasing eye glasses found that attitudes, social norms, and behavioral control were all important for understanding intentions to purchase eye glasses. 16 Our study is similar in finding that the Theory of Planned Behavior is important for understanding intentions to use the EyeScience Computer Eye Strain formula. However, with regard to use, we found that only intentions but not attitudes, social norms, and behavioral control were significantly associated with use. This is not consistent with the Theory of Planned Behavior. It is challenging to understand why many of the variables used as part of the Theory of Planned Behavior were not associated with use. Future research needs to replicate this study to determine if the Theory of Planned Behavior is not applicable to use of the EyeScience Computer Eye Strain formula.
We found that increased symptoms were associated with increased intentions to use the EyeScience Computer Eye Strain formula, but increased symptoms were not associated with actual use. There is limited literature on symptom level and behavior as part of the theoretical framework of the Theory of Planned Behavior. One study using the Theory of Planned Behavior framework with undergraduate college men found that symptom severity was not significantly associated with intentions for performing a testicular examination, while intentions were significantly associated with performing a testicular examination. 17 Our study has similar findings of intentions being associated with behavior. However, our study differs from the testicular examination study and does find an association of symptoms with intentions. A possible reason for this difference may be related to how invasive a supplement is determined to be. For example, by HIV testing, there is literature showing that people who would decline a serum HIV test would agree to take a less invasive salivary test. 18 Swallowing an eye supplement may be interpreted as less invasive or less involved than having to perform a testicular examination and therefore those experiencing eye symptoms are willing to consider using a perceived non-invasive oral eye supplement.
We found that general use of eye supplements and also those who used the Eye Science Computer Eye Strain formula were significantly associated with intentions to use the Eye Science Computer Eye Strain formula. It is logical to expect that those who used eye supplements and had positive experiences with eye supplements will be interested in continuing to use eye supplements in the future. Similarly, it is logical to expect that those who used the Eye Science Computer Eye Strain formula and had positive experiences with the Eye Science Computer Eye Strain formula will be interested in continuing to use the Eye Science Computer Eye Strain formula.
We found that the preference to swallow an oral eye supplement instead of using eye drops was significantly associated with increased intentions to use the EyeScience Computer Eye Strain formula but not with the behavior of actual use of the EyeScience Computer Eye Strain formula product. We also found that those who previously used eye drops for computer vision syndrome had high odds to use the EyeScience Computer Eye Strain formula product. This preference can be understood from both a preventive medicine approach and also from an experiencing symptoms approach. From a preventive medicine approach, a study of HIV prevention with a choice for preference of using either a vaginal gel or an oral tablet found that among those with no previous experience of either treatment, there was a preference to use the oral tablet. 19 It is possible that such a preference exists for intentions to use an oral supplement of the EyeScience Computer Eye Strain formula. The lack of such a preference for actual behavior for use of the EyeScience Computer Eye Strain formula may depend on past experience of eye treatments in addition to other factors. However, as we found that those who previously used eye drops for computer vision syndrome had high odds to use the EyeScience Computer Eye Strain formula, although they may not have had a particular preference, their behavior showed that they were willing to consider an oral supplement of the EyeScience Computer Eye Strain formula too. From an experiencing symptoms approach, a study about preference for either topical or oral use of a non-steroidal anti-inflammatory drug for knee pain found a preference for use of an oral drug rather than a topical cream. Reasons for preference for oral drug over a topical cream included that the oral drug provided a quicker way for treatment and also was less messy than a topical cream. 20 It is possible that such a preference exists with similar reasons for intentions to use an oral supplement of the EyeScience Computer Eye Strain formula rather than eye drops. The lack of such a preference for actual behavior for use of the EyeScience Computer Eye Strain formula may depend upon what a healthcare practitioner recommends to those experiencing adverse eye symptoms.
We found that those who received treatment for computer vision syndrome had high odds to use the EyeScience Computer Eye Strain formula. It is logical to assume that those who received treatment for a particular health condition such as computer vision syndrome have greater odds to engage in behavior to obtain treatments associated with their health condition of computer vision syndrome. Reasons for use can range from a belief that it can enhance their treatment to that their current treatment plan did not work and this new treatment is worth using.
This study has several limitations. First, the sample was from one college and the findings may not generalize to other colleges. Second, we found that the behavior of using the Eye Science Computer Eye Strain formula was less than 5% which may indicate that many did not know about this product until our survey introduced them to this product. Future research may be useful to study known users of Eye Science Computer Eye Strain formula and to determine their experience with the product and their likelihood of continued use of the product.
In conclusion, we found that those who previously used eye supplements and also those with computer vision syndrome related symptoms were associated with increased intentions to use the oral supplement for computer vision syndrome of the Eye Science Computer Eye Strain formula. Also, those who received treatment for computer vision syndrome and those who used eye drops for computer vision syndrome had increased odds to use the Eye Science Computer Eye Strain formula. We recommend that when relevant, healthcare practitioners recommend oral treatments such as the Eye Science Computer Eye Strain formula for computer vision syndrome. Marketers of oral treatments such as the Eye Science Computer Eye Strain formula should consider as part of their advertising campaign including content about computer vision syndrome related symptoms and also that those who previously used eye drops are very receptive to considering use of an oral treatment for computer vision syndrome.
Footnotes
Conflict of interest
The authors declare that there are no conflicts of interest.
Funding
No funding was received to conduct this study.