
Abstract
If geroscience research delivers on its promise to increase healthy life years, societies around the globe will face profound moral questions. Unlike research addressing diseases such as cardiovascular disease, cancer, or diabetes, biological targeting of the process of senescence has a far wider, almost unprecedented sweep, potentially benefiting all people across the lifespan and future generations. This paper proposes that geroscience products must be allocated in a way that enhances global health equity, which requires setting an attainable, if difficult, goal of bringing everyone up to a minimal health span. After introducing the topic (in Section I), Section II responds to a range of ethical concerns geroscience research raises and argues that pursuing research in this area is a priority. Section III focuses on how to justly distribute possible future products of geroscience research and examines egalitarian, sufficientarian, and priority to the least well-off approaches. Section IV proposes a path forward that prioritizes ensuring people everywhere can attain health span sufficiency. Section V concludes that implementing the proposed approach will require large, collaborative efforts to be set in motion proactively, before inequities materialize. In this rapidly advancing field, there is an opportunity now to apply ethical forethought and planning.
Introduction
In an aging world, many individuals would welcome the prospect of living more years in good health and with greater physiological resilience (Farrelly, 2023). Many societies would be eager for a future where older people stay healthy and independent longer, saving governments trillions and making economies more productive. Geroscience aspires to deliver on these and other enticing possibilities. Rather than treating the symptoms of age-related chronic disease, geroscience targets underlying cellular changes associated with biological aging—senescence—that put people at risk of chronic conditions. According to its proponents, biological aging represents ‘the greatest modifiable risk factor for chronic diseases’ (Sierra et al., 2021: 2456).
In response to growing interest specifically in geroscience research, the National Institutes of Health (NIH) formed a Geroscience Interest Group in 2017 that brought together multiple institutes to explore the state of the science and potential challenges. Subsequently, the NIH hosted a series of scientific summits, the most recent in 2023 (Sierra and Kohanski, 2017).
Even supposing radical life extension is unlikely in the near term (Olshansky et al., 2024), and even if there is an upper limit to the human lifespan (Milholland and Vijg, 2022), many geroscientists consider the prospect of moderate improvements in health span (i.e., years of healthy life) plausible. Moderate progress might be accelerated by major investments in geroscience by venture capitalists, prominent investors, new foundations, large pharmaceutical and biotechnology companies, or by additional funding streams expected to open up if the U.S. Food and Drug Administration (FDA) classifies aging as a ‘medical indication’ that can be treated (Lederman, 2023). Geroscience breakthroughs might also be accelerated by applying artificial intelligence approaches to aging biology (Fuellen et al., 2025), making new discoveries in genomics, or finding new biomarkers predictive of rates of aging (Oh et al., 2025). In parallel, geroscience research might produce advances through the repurposing of already FDA-approved drugs, such as metformin (American Federation for Aging Research, 2025) or rapamycin (Lee et al., 2024).
Despite high hopes for geroscience, many geroscience studies once considered promising have yielded disappointing results (Brenner, 2023; Brown et al., 2024; El Maï et al., 2023). While it is difficult to say what the future holds, this still nascent field warrants the attention of bioethicists now. If geroscience eventually delivers on its promise to increase healthy life years, societies around the globe will face profound moral questions that have only begun to attract attention (Nuffield Council on Bioethics, 2023). Unlike research addressing diseases such as cardiovascular disease, cancer, or diabetes, biological targeting of the senescence process itself has a far wider sweep, potentially benefiting all people across the lifespan. Further, unlike research examining individual medical conditions, geroscience research targeting senescence has broader societal implications for how people understand and approach aging. This paper proposes that geroscience results and products must be allocated in a way that enhances global health equity, which requires setting an attainable, if difficult, goal of bringing everyone up to a minimal health span. Section II responds to a range of ethical concerns geroscience research raises and argues that pursuing research in this area is a priority. Section III focuses on how to justly distribute possible future products of geroscience research and examines egalitarian, sufficientarian, and priority to the least well-off approaches. Section IV propose a path forward that prioritizes ensuring people everywhere can attain health span sufficiency. Section V concludes that the practical application of our proposed approach will require large, collaborative efforts that need to be proactively set in motion before inequities materialize in this quickly advancing field.
Ethical concerns about conducting geroscience research
Despite its wide appeal, the prospect of extending healthy life years by modifying mechanisms of senescence has raised a range of ethical concerns.
Prioritizing basic needs
Some question the fairness of investing in research to increase the number of years people can live in good health when many people cannot reach the current global average of a healthy lifespan (which was 61.9 years between 2000 and 2021; Pijnenburg and Leget, 2007; World Health Organization, 2021). Are research dollars not better spent on ensuring access to already known social determinants of health, such as food security, access to healthcare, education, and housing? Public health scientists have long urged a ‘war against disease’, waged by means of preventive measures that improve the social conditions in which people are born, grow, live, work, and age (Farrelly, 2024; World Health Organization, 2026).
In response, the same objection could be made against any biomedical research endeavor aiming to cure or treat disease. For example, it could be argued it is unethical to invest in research to treat or cure cancer, diabetes, or cardiovascular diseases because funding is better spent on feeding the hungry, housing the homeless, preventing disease, or increasing access to basic healthcare. Like all biomedical research, geroscience research has opportunity costs, that is, other social goods that might have been sought instead. Unless we want to say that everyone’s basic needs must be fully met before non-basic priorities are addressed, some fair and reasonable balance must be struck. The question (discussed in sections III and IV) thus becomes, ‘What is a fair and reasonable balance?’
Global health disparities
Others who raise concerns about geroscience research point to global disparities in the conduct of biomedical research and worry that geroscience research will exacerbate them (Addie et al., 2024). The so-called ‘10/90 split’ in international research funding—that is, the fact that 90% of research funding is spent on diseases affecting just 10% percent of the world’s population—epitomizes this concern (Yegros-Yegros et al., 2020). If geroscience research will be affordable primarily for the wealthiest people in the world, worsening the 10/90 split, can it be an ethically justified pursuit? Expressed differently, is it ethical for the governments of wealthy countries, private foundations, or philanthropists to devote large sums to research that will likely benefit people already fortunate enough to live into their later decades and beyond, while devoting so comparatively little to research on malaria, tuberculosis, diarrheal disease, malnutrition, and other conditions that prevent large numbers of people from reaching the global average of healthy life years? According to Pratt (2021: p. 1), ‘global health research should generate new knowledge to improve the health and well-being of those considered most disadvantaged and marginalized’.
Related to this is the question of how the possible products of geroscience research would be distributed and whether they would be broadly shared. With health span already far higher in high-income than in low- and middle-income countries (Garmany and Terzic, 2024), would access to future geroscience interventions worsen global health disparities? For example, across Africa, average healthy life expectancy at birth in 2021 was 55 years, well below Europe’s, which was 66 years during the same year. If geroscience interventions extended Europe’s average health span at birth by 5 years, while leaving Africa’s untouched, the health span gap between Europe and Africa would be 15 years, a 50% increase. Even if geroscience products eventually become more affordable, drug patents and other intellectual property protections will most likely keep prices high for many years (World Health Organization, 2021).
In partial reply, it might be argued that whether a distribution of benefits and burdens is fair depends on how the distribution came about. Perhaps, concerns over global health equity in geroscience research could be addressed by using allocation frameworks with built-in consideration of health disparities, such as Research for Health Justice, the Fair Benefits Framework (El Setouhy et al., 2021), Benchmarks for Ethical Research (Emanuel et al., 2004), or the framework of the Council for International Organizations of Medical Services (Council for International Organizations of Medical Sciences (CIOMS), 2016). In further reply, inequities are not yet inherent to geroscience research. Sponsors and funders could commit now to sharing the results of any future products with people in low- and middle-income countries by requiring this as a condition of funding (Hevolution Foundation, 2025). They could commit now to a diverse workforce in geroscience research by funding researchers in low-and middle-income countries (Teruel Camargo et al., 2024). These steps establish global partnerships that set the stage for a broader, more inclusive distribution of possible products of geroscience research.
Justice between young and old
A third concern relates to justice between young and old age groups. Will the net effect of increasing the well period of a person’s life be to undercut fair opportunity for younger people (Jecker, 2022a)? For example, will extending an older population’s ability to remain in the workforce and housing market reduce chances for younger people to get jobs and buy homes? Have older adults already had a ‘fair turn’ at life (Williams, 1997)?
A rejoinder to this objection is to consider an analogous case. Prescribing statins for people with cardiovascular disease prevents disease progression and saves lives. This may result in people on statins living longer and remaining in the workforce for more years than they otherwise would. Yet it hardly follows that treating older people with statins is unfair to younger people.
And it is misleading to characterize geroscience as benefiting only older people. When today’s younger people are old, they too will benefit from more years of healthy life (Daniels, 1998). Aging is something that potentially affect all of us, if we are lucky enough to reach old age. Intervening in aging is in thus highly egalitarian. What’s more, if geroscience research slows or reverses the effects of aging, this could potentially free up resources that benefit younger people.
Geroscience is ageist
A further worry is that efforts to eradicate age-related disease and disability might appear to be ageist, making those older people who do not benefit from geroscience feel put down, harshly judged, or even abandoned. Thus, proponents of ‘healthy aging’ (also promoted as, ‘successful’, ‘active’, ‘productive’ and ‘vital’ aging, or ‘aging well’) urge older adults to do what they can to stay young, and to attain good health by making the ‘right’ lifestyle choices (Havighurst, 1961). Yet critics argue that healthy aging discourse embeds ageist and ableist biases (Langmann and Weßel, 2023) and that ‘talking about “successful aging”—meaning robust and active old age—implies that old people who are not robust and active are “unsuccessful” (Gillick, 2010: 648).
In reply, if the fruits of geroscience research slow or reverse age-related disease and disability, geroscience advances could reduce the stigma associated with growing old by decoupling chronological from biological aging (García-Barranquero et al., 2024). Thus, a utilitarian who holds that ‘other things being equal, it is better if very happy people live rather than less happy people’ (Tānsjo, 2010: 103) might regard aging as a net negative utility, because it raises risk of age-related disease and disability, reducing subjective happiness (whether due to societal discrimination or features of a disability; García-Barranquero et al., 2024). If geroscience reduced age-related disease and disability, allowing people to enjoy more years in good health, utilitarians would presumably regard chronologically aging more positively.
To further combat ageism, investors in geroscience research might encourage investment in services and environments tied to increasing opportunities for all. Moreover, it is important to combine health span extension with comprehensive end of life planning, including plans for treatment limitation, advance directives, and assisted dying/euthanasia.
Other concerns
Geroscience has raised many other ethical concerns (Ringel et al., 2025). First, the field has a history of quackery and hucksterism that has bred distrust (de Gray et al., 2002). Discoveries in the field have been exploited by those looking to quickly capitalize by selling services (tests, treatments, supplements etc.) that are not evidence-based. Related to this is the perception that biological aging is immutable, making geroscience a ‘tough sell’ (Lederman, 2023). To address this, legitimate scientific efforts must be distinguished from antiaging quackery (Perls, 2004). The scientific community, and geroscience researchers especially, must acknowledge that there are currently no scientifically proven antiaging medicines.
Second, the prospect that older people will simply grow tired of living, or feel that their ‘life is completed and no longer worth living’ (van Wijngaarden et al., 2015: 257) might lead some to ask, what is the point of geroscience. In the Netherlands, over 100,000 healthy people signed a petition in 2010 to extend euthanasia legislation to permit physician-assisted dying for older people who regarded their lives to be complete (Van der Geest and Satalkar, 2021). In 2015, a cross-sectional survey of the Dutch general public showed that 21% agreed with the statement, ‘In my opinion, euthanasia should be allowed for persons who are tired of living without having a serious disease’ (Raijmakers et al., 2015: 147). Some bioethicists argue that after a certain age, people have pursued whatever life projects they are going to pursue and made whatever contributions they will make (Callahan, 2003; Emanuel, 2014). Yet the point of geroscience research is not to extend life, but to make the life we have healthier. The majority of people might welcome this possibility.
Third, the impact of mixed success scenarios raises concerns. These are cases in which geroscience breakthroughs come in some areas, for example, cardiovascular disease, but not others, for example, dementia (Jecker, 2022b). Suppose a person with Alzheimer’s disease lived 5 or 10 years longer than they otherwise would have due to geroscience interventions that resulted in a healthier heart. In addition to general quality-of-life concerns for that person, what impact would this scenario have on caregivers? Importantly, men are more likely than women to favor lifespan extension, at least in the United States (PEW Research Center, 2013); at the same time, they are less likely than women to serve as caregivers for dependent older people (Ophir and Polos, 2022).
Tempering these concerns is the fact that geroscience seeks to delay the onset and progression of multiple chronic conditions simultaneously by targeting their shared biological mechanisms (aging; Sierra et al., 2021). Yet it remains to be seen whether geroscience will deliver on its promise or instead yield mixed success outcomes, with variable degrees of improvement (or no improvement) among different age-related diseases. If mixed successes occur, justice frameworks will be needed to help determine funding priorities between diseases. We return to this topic briefly later in the paper (Section IV).
Lastly, it is worth considering how immensely pharmaceutical companies stand to benefit from breakthrough geroscience drugs, especially if aging were classified as a medical indication for treatment. This concern underscores the need to establish clear ethical guardrails. Doing so now, before geroscience products become available, can more profoundly shape the field’s future trajectory (Berkley, 2025). Table 1 summarizes ethical objections to conducting geroscience research and our replies.
Ethical concerns about conducting geroscience research.
Justly distributing products of geroscience research
Given the above concerns, if geroscience research continues to advance and eventually yields interventions that slow, stop, or reverse aging processes, what would be an ethically fair distribution of geroscience products? Although each country has its own process for distributing healthcare products, it is worth considering the ‘north star’ or best-case scenario for the purpose of setting ethical guidelines. Since the just distribution of healthcare is contested, we give a broad overview before setting forth and defending our preferred approach.
Egalitarian justice
Egalitarian justice might recommend setting as a goal reducing years of unhealthy life to the same degree for everyone, regardless of baseline (Figure 1).
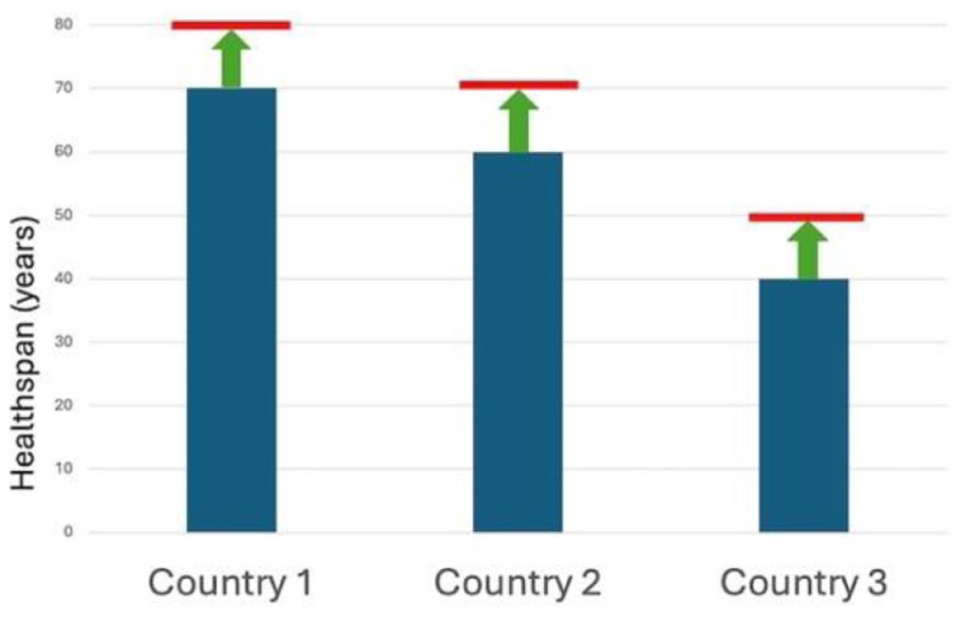
Egalitarian justice.
For example, people in Niger, where healthy life expectancy is 55 years, and people in Switzerland, where it is 71 years, should each have access to the means to increase health span by 2 years.
Other possible interpretations of egalitarian justice include establishing and maintaining the same baseline of healthy life expectancy for all people. For example, considering again the example of Niger and Switzerland, access to geroscience interventions should be allotted first to people in Niger; no one in Switzerland should have access until the health span of people in Niger ‘catches up’ to the health span of people in Switzerland.
The justification for either interpretation of egalitarianism might be that people should have an equal opportunity to pursue goods such as life liberty and happiness; or that physical pains of a sufficient degree ought to be treated the same, regardless of who experiences them; or that showing equal respect to persons requires ensuring equal access to tools that slow or reverse disease and disability (Gutmann, 1983).
Sufficientarian justice
A second possible answer to the question of how future geroscience products ought to be distributed holds that inequality per se is not a bad thing, provided everyone has enough of the good in question, which in this case is healthy life years (Figure 2).
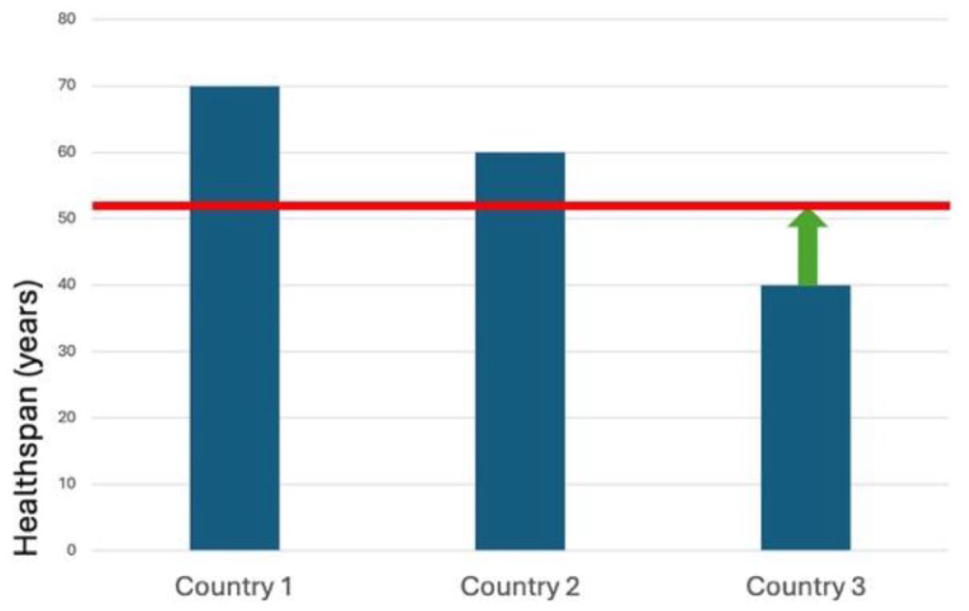
Sufficientarian justice.
A sufficientarian approach to geroscience would focus first on regions where health span falls below the threshold of healthy years considered minimal (National Academy of Medicine, 2024). Another formulation of this is the ‘fair innings’ argument, which holds that what everyone is entitled to is a fair innings (a life of sufficient length; Harris, 1985) or a ‘fair go’ (Savulescu, 2022).
What counts as ‘good enough’, a ‘fair innings’, or a ‘fair go’? Typically, the threshold for sufficiency is set above mere survival. It arguably can be set at a minimally good life: ‘Everyone must obtain what helps them secure the relationships, pleasures, knowledge, appreciation, worthwhile activities, and other life-improving good they need to live minimally good lives’ (Hassoun, 2024). Others interpret ‘good enough’ vis-a-vis central human capabilities required to lead a dignified human life, including having the ability to live to the end of a human life of normal length, be healthy, have bodily integrity, deliberate about plans and goals, affiliate with others and nature, express a range of human emotions, play and recreate (Jecker, 2020; Nussbaum, 2011; Ringel et al., 2025).
Priority to the least well-off
A third response to the question of how to fairly share possible fruits of geroscience research recommends priority to people who are the least well-off. One way to translate this would be to say that years of unhealthy life should be reduced in a way that benefits groups with the least health longevity, regardless of how many years of healthy life they are expected to live (Figure 3).
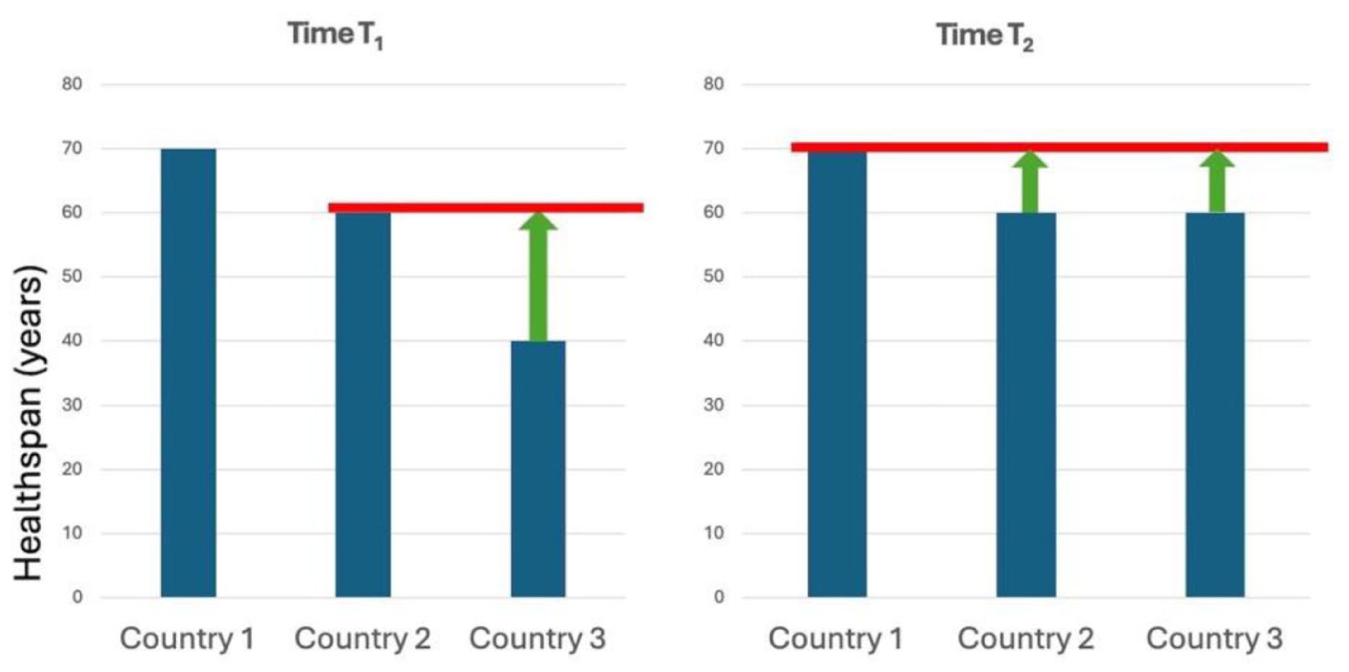
Priority to the least well off.
In contrast to a sufficientarian approach, priority to the least well-off prioritizes access to geroscience for people in low- and middle-income countries where health span is generally lowest, irrespective of what level of health span exists in those countries.
The justification for helping the least well-off might be utilitarian: helping the least well-off creates the greatest improvement in aggregate well-being. Alternatively, priority to the least well-off might be warranted because it reduces inequality. Finally, the justification for assigning priority to the least well-off might be based on Rawlsian justice. A Rawlsian approach holds that the just distribution of any future geroscience products should be determined behind a hypothetical veil of ignorance, where we imagine ourselves to be ignorant of important facts about ourselves like our health, wealth, or country of origin. From this perspective, we would might prioritize distributing geroscience products to those expected to live the fewest years of healthy life, because when the veil is lifted we might be among them.
A path forward
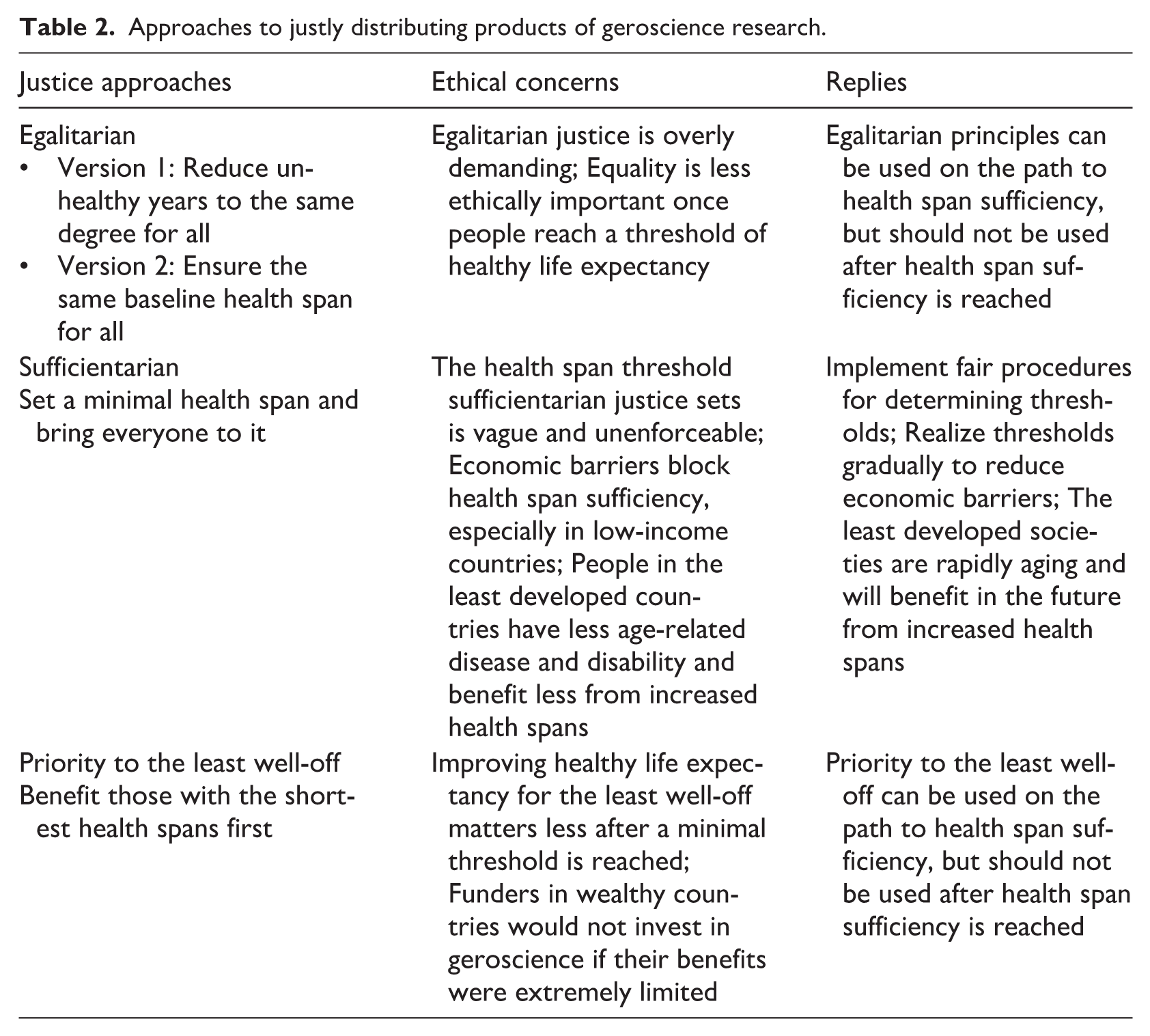
All these approaches agree that geroscience ought to be pursued fairly, and in ways that enhance global health equity. We submit that the best way to realize fairness is sufficientarian justice: commit to bringing everyone up to a minimal health span. This approach has both ethical and pragmatic advantages over the alternatives of egalitarian justice and priority to the least well-off.
Both egalitarian justice and priority to the least well-off are less attractive than sufficientarian justice because these alterantives demand too much. Egalitarian approaches require equal increases in health span for everyone, even for those who are already objectively well-off. Yet equality of distribution seems to matter far more if those at the bottom fare extremely poorly than if they fare extremely well (or good enough). Priority to the least well-off raises a parallel concern, because it privileges the claims of the least well-off even if they exceed the level of sufficiency. By demanding too much, both views fall short not only on ethical, but pragmatic, grounds. Funders of geroscience, most of them situated in wealthy regions, may have little incentive to invest in geroscience research if they themselves were precluded from benefiting from future geroscience products (because priority was given to the least well-off) or if the benefits they could expect were extremely limited (because benefits were equally distributed). To avoid being overly demanding, both approaches should be limited. For example, an egalitarian principle could be applied on the path to health span sufficiency, but end after a society attains health span sufficiency. Likewise, priority to those with the least health span sufficiency might apply until health span sufficiency is realized, but end after a society reaches health span sufficiency.
Jecker (2020) and Venkatapuram (2011) translate health span sufficiency in terms of having all or a subset of central human capabilities at a minimum level required to lead a dignified human life. A provisional list of central human capabilities includes life stage-related capacities for life (being able to have a narrative of one’s life i.e. still unfolding); health (being able to have all or a subset of the other capabilities at a threshold level); bodily integrity (being able to use one’s body to realize one’s desires and goals); senses, imagination, and thought (being able to engage in meaningful ways in sensing, imagining, and thinking); emotions (being able to feel and express a range of emotions); practical reason (being able to form and reflect on goals and life plans); affiliation (being able to live for and in relation to others); nature (being able to live in relation to nature and other species); play (being able to play and recreate); and environment (being able to regulate one’s immediate physical and social environments (Jecker, 2020), adapted from Nussbaum (2011)). A capabilities framework can aid with complex decisions about setting priorities based on the relative capabilities of target populations. Various capability metrics have been developed to assess capability thresholds, most prominently the United Nations Human Development Index, which assesses the human development of countries (United Nations, n.d.; Robeyns, 2006). In domains of health and social care, a standard of achieving ‘basic capabilities’ or ‘a minimum level of capability attainment’ has also been incorporated into capability metrics (Mitchell et al., 2017). Applied to geroscience, these metrics can aid with difficult decisions about the relative priority of improving health spans in rich and poor nations, or funding research into different diseases in ‘mixed success scenarios’ (discussed in Section II, subsection 5).
While these considerations argue in favor of a sufficientarian approach, objections to sufficientarian justice can be raised. First, increasing health spans would do little to help people in the least developed countries (LDCs) reach health span sufficiency, because age-related disease and disability are not the major drivers of death in these countries. In reply, LDCs are currently undergoing a rapid demographic transition that is forecast to result in the number of persons aged 65 tripling between 2023 and 2050 (United Nations, Department of Economic and Social Affairs, 2023). If geroscience research increases health span, this could help LDCs as their populations age.
Second, the key concept of a ‘minimal threshold’ is vague and difficult to translate, and societies lack consensus about what constitutes a minimally good life (Casal, 2007). Yet, when societies lack consensus, fair processes, such as accountability for reasonableness, might be implemented (Daniels, 2008). Accountability for reasonableness engages relevant stakeholders (e.g. scientists, policymakers, and the public) and requires that criteria for choosing distributive criteria be publicly available, relevant to stakeholder goals, revisable, measurable, and enforceable.
Third, even if societies agree to a threshold health span, sufficientarian justice is difficult to measure and enforce (Masny, 2023). How could anyone stop wealthy individuals or high-income nations from prioritizing or hoarding effective products yielded by geroscience? In response, every ethical guidance faces headwinds. The value of establishing ethical standards for geroscience is to point societies and wealthy investors to goals they should aspire to realize. For societies that fall well below health span sufficiency, policies can deliver progress gradually, with longer time horizons to achieve sufficiency. Our recommendations could be impactful if endorsed partially or stepwise. For example, if private funders of geroscience research endorsed them, or professional medical groups incorporated them, this could touch the lives of many people. Alternatives, such as banning geroscience research, would be difficult to enforce, and entail drawbacks, such as failing to offer aid to those who fall below health span sufficiency (Wareham, 2016).
Our ethical analysis lends strong support to a sufficientarian approach to distributing products of geroscience research. Table 2 summarizes the analysis.
Approaches to justly distributing products of geroscience research.
The practical application of this approach will require large, collaborative efforts. Such efforts should be proactively set in motion before inequities materialize and become entrenched in this quickly advancing field.
Conclusion
In closing, this paper (1) addressed ethical concerns geroscience research raises; (2) argued that if geroscience delivers on its promise to extend healthy lifespan, its products should be allocated to ensure everyone can reach health span sufficiency; and (3) proposed a path forward, including steps that research funders can take now to promote global justice in geroscience research. The challenge of translating our proposed sufficientarian approach into practice is formidable. While all humanity stands to benefit from future products of geroscience research, the just distribution of geroscience products is hardly a given. It demands ethical forethought and planning now.
Footnotes
Acknowledgements
This paper was informed by the work of the International Bioethics Advisory Committee to the Hevolution Foundation based at New York University’s Grossman School of Medicine. Special thanks are due to the following Advisory Committee members: Colin Farrelly, Bartha Knoppers, and Vina Vaswani. All views expressed in the paper are solely the authors’ own and do not represent the views of any institutions, associations, or organizations the authors may be affiliated with. A version of this paper was presented at the National Academy of Medicine workshop, ‘Societal Implications of Geroscience’ (by Nancy S. Jecker, December 2024, Washington, D.C.). The authors are grateful to workshop participants for helpful comments that improved the paper.
Ethical considerations
Not applicable.
Author contributions
Each author contributed substantially to the conception and analysis of the work; drafting or revising it critically; final approval of the version to be published; and is accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the National Research Foundation, Singapore under its AI Singapore Program (AISG Award No: AISG3-GV-2023-012). This work was supported by the Wellcome Trust (Grant number: 226801) for Discovery Research Platform for Transformative Inclusivity in Ethics and Humanities Research (ANTITHESES). For the purpose of open access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.