
Abstract
Individuals with overweight and obesity represent the majority of U.S. adults, yet they are disproportionately excluded from clinical trials, particularly drug-development studies. Such exclusions raise serious ethical concerns related to justice and fair subject selection, while simultaneously compromising the generalizability of drug safety and efficacy. To better understand the scope of this issue, we conducted a systematic search of 251 active U.S.-based interventional drug-development trials registered on ClinicalTrials.gov. Among these, 186 (74.1%) studies used BMI-and/or-weight-based (BWB) eligibility criteria: 83 (44.4%) with BMI cutoffs only, 12 (6.4%) with weight cutoffs only, and 91 (49.2%) with both. BMI thresholds varied widely and frequently diverged from standard clinical categories. Only three (1.2%) studies offered an explicit justification for the criteria in publicly accessible documents. Meanwhile, 65 (25.9%) studies imposed no BWB limits, suggesting such exclusions are not universally believed to be necessary. We argue that BWB exclusions are not merely methodological deficits but expressions of structural injustice within research governance. Our descriptive analysis provides a foundation for future evaluation of whether such exclusions are scientifically or ethically justifiable. Inclusion of marginalized groups is a critical requirement for producing valid scientific knowledge and ethical clinical research. Oversight bodies, sponsors, institutions, and investigators must treat BWB criteria with careful discretion, requiring transparent justification and proactive inclusion to ensure justice, rigor, and equity in clinical research.
Introduction
A foundational principle of ethical clinical research is justice, which, in part, requires that the benefits and burdens of research be equitably distributed and that participant selection be fair (Emanuel et al., 2000; National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research, 1979). The Belmont Report and subsequent research guidelines (e.g. Common Rule) endorse the importance of ensuring that all populations are neither unequally burdened by, nor systematically excluded from, clinical research. Despite these longstanding ethical guidelines, research practices have historically excluded marginalized groups, including women, pregnant people, children, older adults, people with disabilities, and racial and ethnic minorities, from clinical trial participation (Bibbins-Domingo and Helman, 2022; Hussain-Gambles et al., 2004; van der Graaf et al., 2018). The most common justifications for the exclusion of these groups are founded upon concerns for liabilities, increased risk, analytic complexity, and vulnerability of the participants. However, as articulated in the Belmont Report, “an injustice occurs when some benefit to which a person is entitled is denied without good reason or when some burden is imposed unduly,” raising important questions about the ethical justification for excluding groups from research (National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research, 1979). The National Institutes of Health (NIH) Revitalization Act of 1993 mandates that women and minority groups be included in federally funded clinical research so long as their inclusion appropriately aligns with the health of the participants and purpose of the research (Mastroianni et al., 1994). Additional research policies have called for the inclusion of children and older adults, who have also historically been excluded from research (National Institutes of Health, 2017). Greater inclusivity in research has improved understanding of outcomes across different populations, and equitable representation in clinical trials has become an obligatory component of study design and approval (Chen et al., 2014; Mastroianni et al., 1994). Nonetheless, a pattern of unjustified exclusion of people with high BMIs 1 from clinical trials persists.
Although people with overweight and obesity comprise the statistical majority of the U.S. adult population, they are systematically excluded from clinical trials research—a practice that has received relatively little ethical scrutiny (Burckart and Greenblatt, 2023; Pagarkar et al., 2023; Pestine et al., 2018; Shen et al., 2024). This omission influences the generalizability of new interventional drugs and biologicals, as evidenced by the decreased efficacy and inadequate dosing standards of certain medications like the emergency contraceptive drug levonorgestrel and some antibiotics, like cefepime, in higher-weight populations (Jatlaoui and Curtis, 2016; Roe et al., 2012). In this article, we describe a systematic search of a relevant sample of ClinicalTrials.gov study records to assess the extent of BMI-and/or-weight-based (BWB) eligibility criteria in drug-development trials. We discuss our results in the context of justice, clinical research ethics, the generalizability and rigor of science, and recent literature promoting the inclusion of people with high BMIs in clinical trials. This study serves as a caution against the exclusion of individuals with overweight and obesity from clinical trials, which we argue researchers and oversight bodies like institutional review boards (IRBs) should be aware of and proactively seek to remedy.
Background
Obesity is a multifactorial chronic health condition broadly characterized by the presence of adiposity, or excess body fat. It can be influenced by a combination of biological, behavioral, sociocultural, genetic, environmental, and economic factors, and its classification has been a topic of public health discussions for decades (Kumanyika et al., 2002; Ross et al., 2020). Despite the condition’s complexity, obesity is commonly measured by the body mass index (BMI), an anthropometric calculation of weight in kilograms divided by height in meters squared (kg/m2), because this measure is non-invasive, simple, and useful in large-scale epidemiologic surveillance (Nguyen and El-Serag, 2010). However, BMI measurements fail to distinguish between fat and muscle, ignore fat distribution, vary across populations, misrepresent an individual’s health status, and reinforce weight stigma (Bays et al., 2013; Flegal, 2023; Nuttall, 2015). Recently, the American Medical Association has recommended moving away from BMI alone as a clinical measurement for diagnosing obesity and its comorbidities (Berg, 2023). The use of BMI outside of population-level assessments raises significant concerns, especially when it is used as a proxy for individual health or to determine eligibility for clinical research (Rubino et al., 2023). We distinguish between these uses and focus our ethical analysis on the use of BMI as an exclusionary criterion in clinical research.
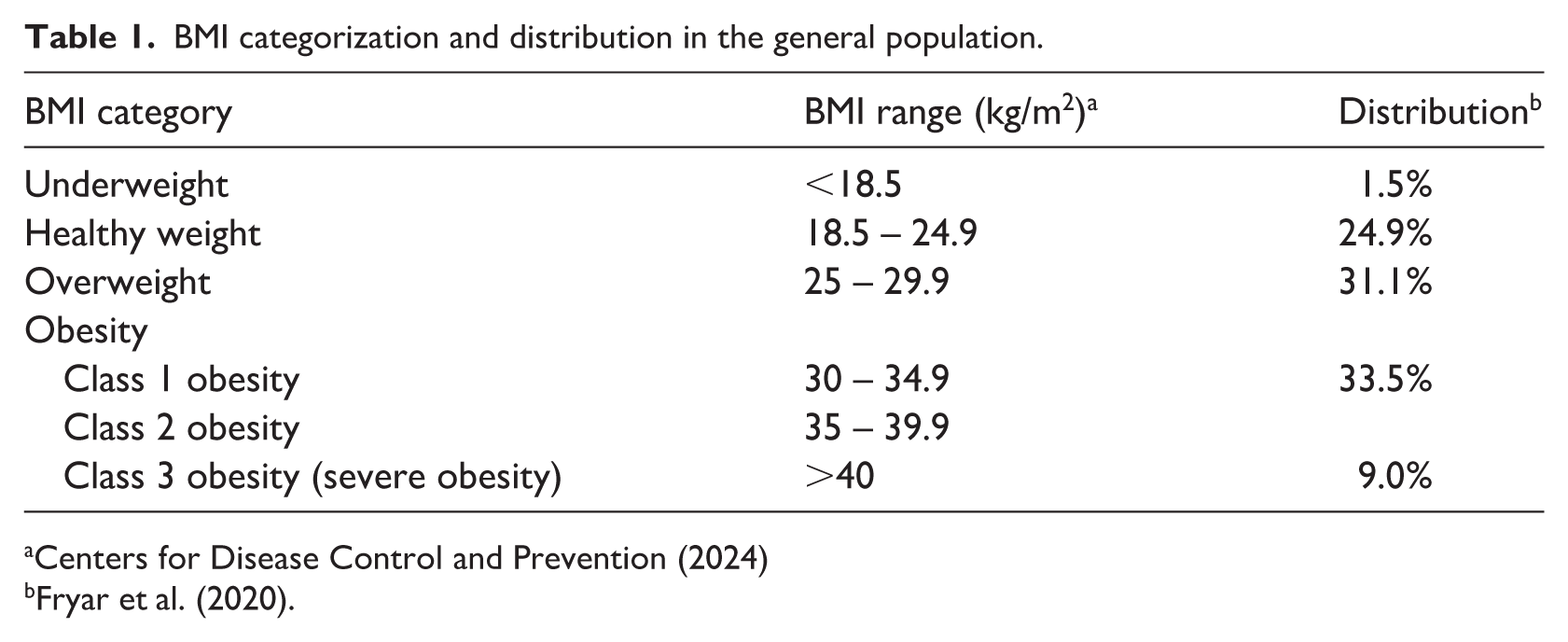
Assessments of the prevalence of overweight and obesity in the population vary slightly, but all concur that most of the U.S. adult population can be categorized as overweight or obese based on BMI data. Table 1 shows the current BMI classifications set forth by the U.S. Centers for Disease Control and Prevention (CDC) and the approximate distribution of each class across the U.S. adult population. According to the National Health and Nutrition Examination Survey (NHANES) 2017–2018 data, approximately 73% of U.S. adults aged 20 and over fall into the overweight or obesity BMI classifications, broken down further in Table 1 (Fryar et al., 2020). Using more recent data from NHANES 2021–2023, Emmerich et al. (2024) indicate that 40.3% of U.S. adults have obesity, including 9.4% with severe obesity, although that publication did not report underweight, healthy weight, and overweight statistics. A recent increase in the use of obesity management medications, including glucagon-like peptide-1 (GLP-1) receptor agonists, has moderately slowed the rate at which obesity prevalence continues to grow in the United States, but overall rates remain high (Witters and James, 2025).
BMI categorization and distribution in the general population.
Obesity status is a well-documented source of stigma and discrimination in clinical settings, contributing to mistrust, delays in care, and poor health outcomes for people in larger bodies (Humbyrd, 2018; Keller et al., 2024; Puhl and Heuer, 2009; Rubino et al., 2020). Furthermore, the prevalence of overweight and obesity is frequently higher among some marginalized populations, like those with a lower socioeconomic status or belonging to certain racial or ethnic groups, demonstrating the impact that the social determinants of health have on obesity and other related health conditions (Datar et al., 2023; Williams et al., 2024). Considering this, the exclusion of people with high BMIs from clinical research is, by extension, the exclusion of individuals from various minority populations.
Individuals with high BMIs who may wish to enroll in clinical research face exclusionary practices justified by uncertain and inconsistent evidence, such as concerns for pharmacokinetic and pharmacodynamic variability, safety, and undesirable protocol complexity (Cheymol, 2000; Gouju and Legeay, 2023; Moore et al., 2023). Robust empirical research to support these justifications is lacking both in volume and consensus. As with other historically excluded groups, these practices instead reflect structural biases that conflate physical difference with scientific inconvenience. Only recently have regulators begun to recognize that the exclusion of participants with overweight and obesity constitutes a form of structural discrimination. Guidance documents from the Food and Drug Administration (FDA) and publications by the American College of Clinical Pharmacology and the Obesity Action Coalition have drawn attention to the need for inclusive research practices that better reflect the demographics and attributes of the population, including those affected by obesity, to bolster safety, efficacy, and generalizability (Burckart and Greenblatt, 2023; Food and Drug Administration, 2018; Obesity Action Coalition, 2023; Shen et al., 2024).
However, people with high BMIs remain markedly underrepresented in clinical trials (Nayak, 2023). Unlike other prohibitive eligibility criteria, BWB criteria have no reporting mandate nor justification standard. Excluding those with high BMIs from clinical trials limits access to potentially beneficial interventions and contributes to a cycle in which data gaps justify further exclusions (Keller et al., 2024; Puhl and Heuer, 2009; Rubino et al., 2020). This not only compromises scientific advancement but also exacerbates social and health inequities. Notably, a review of 137 new molecular entity (NME) products that were approved between 2004 and 2010 revealed that only 2 included safety and efficacy information for patients with obesity on the label (Jain et al., 2011). Mitigating this deficit requires more than improved methodology; it demands re-examining how ethical oversight, scientific validity, and justice are intertwined in the design and governance of biomedical research.
Methods
We conducted a systematic search of ClinicalTrials.gov, a publicly accessible database containing information about clinical research studies. Our goal was to undertake a descriptive analysis, characterizing how BWB criteria are applied across U.S. drug-development trials and generating an empirical foundation for ethical analysis. The following search terms and filters were applied: (1) Other terms: “Pharmacokinetics OR pharmacodynamics”; (2) Study status: “Recruiting” or “Not yet recruiting”; (3) Accepts healthy volunteers; (4) Study type: “Interventional.”
Our search yielded 849 results, which underwent screening and review. All studies were active as of May 2025. We screened the 849 studies for additional criteria that could not be selected on ClinicalTrials.gov, particularly to identify studies that targeted drug or biological interventions and those with study locations in the United States. Studies that did not have sites in the U.S. were excluded to ensure comparability with national obesity prevalence, regulatory frameworks (NIH, FDA), and the predominant ethical discourse shaping inclusion practices and policy. At this stage, 42 studies were excluded for intervention type, 482 for lacking U.S. study sites, and 74 for incomplete recruitment data, yielding 251 studies for full-text review.
For the final 251 studies, the Participant Criteria section of each study was screened to document the appearance of the terms “body mass index,” “BMI,” “weigh,” “weight,” “kg/m2,” “kg,” “lb,” “overweight,” or “obese.” Whether one of these terms appeared as inclusion or exclusion criteria was recorded, along with the corresponding numerical values of the criterion. Specifically, we recorded the BMI range, BMI lower bound, BMI upper bound, weight range, weight lower bound, and/or weight upper bound for each study when applicable. If weight was listed in pounds, we converted to kilograms and rounded to the nearest whole number for consistency in analysis. Data were analyzed descriptively to identify prevalence, variability, and justifications for BWB restrictions.
Results
Of the 251 studies that underwent full review, 186 (74.1%) had BMI-and/or-weight-based (BWB) eligibility criteria, and 65 (25.9%) did not. Among the 186 studies that had BWB eligibility criteria, 12 (6.5%) had weight criteria only, 83 (44.6%) had BMI criteria only, and 91 (48.9%) had both weight and BMI criteria. Of the 174 studies with BMI criteria, some included multiple BMI ranges for different study arms, totaling 185 BMI ranges calculated in our results. Of these 185 ranges, 8 (4.3%) excluded people with overweight (BMI 25–29.9); 118 (63.8%) excluded people with class I obesity using the CDC’s BMI categories (BMI 30–34.9); 142 (76.8%) excluded people with class II obesity (BMI 35–39.9); and 181 (97.8%) excluded people with class III obesity (BMI 40+). The remaining four (2.2%) ranges that did not exclude people with class III obesity only had a lower bound (e.g. BMI over 16), meaning these studies were not exclusionary of people with high BMIs. Seven (3.8%) studies assessed drug efficacy specifically in populations with overweight and obesity, and their BWB criteria were therefore set to only include participants with BMIs in those categories, although some of these studies still excluded potential participants with the highest level of obesity.
BMI ranges across the 186 studies with BWB eligibility criteria varied considerably and did not typically align with the BMI classifications in Table 1 (e.g. an upper-bound cut-off of a BMI of 32 falls in the middle of Class II obesity). We searched the entire study record available on ClinicalTrials.gov for any rationale given to support inclusion or exclusion based on BWB criteria. Only three (1.6%) studies listed explicit reasons for their criteria, which included: (1) lack of data regarding appropriate dosing of the interventional drug being studied; (2) weight limit for MRI and CT tables; and (3) amount of intervention given as part of study must be capped based on weight of individuals.
Of the 186 studies that listed BWB eligibility criteria, almost all (n = 182; 97.8%) were early phase trials (Phase 1 or 2). Among the 65 studies that did not list BWB participation criteria, a similar proportion (n = 59; 90.8%) were early phase trials.
Across all 251 studies, many listed eligibility criteria that set restrictions on the health conditions a participant may have or used language like “deemed healthy as determined by the investigator.” Two studies allowed the investigator or funder to allow people outside the BMI range into the study if they determined their BMI to be “irrelevant.”
We looked further at the details of the 65 studies without BWB eligibility criteria to better understand why they did not list such information. These studies were diverse in design and scope, reflecting a range of scientific objectives, with no significant differences in aim or format from studies with BWB criteria, other than this eligibility difference.
Discussion
This study demonstrates that BMI- and/or-weight-based (BWB) eligibility criteria are pervasive in U.S.-based drug-development trials and are rarely justified in publicly accessible study records. While we are critical of the appropriateness of BMI as a proxy for individual health and as an exclusionary tool in clinical research, we recognize that it remains widely used in population-level and epidemiologic contexts; it is therefore additionally problematic that the studies we reviewed largely did not use BMI ranges aligned with CDC classification categories of overweight and obesity. Ignoring recognized BMI categories further limits the ability to make comparisons between studies across health care contexts. Together, these findings highlight the widespread and inconsistently applied nature of BWB eligibility criteria in drug-development research and raise concern about scientific rigor, as well as justice concerns relating to stigma and bias. This study calls for increased ethical oversight and reforms to the norms of clinical research.
Scientific validity, generalizability, and knowledge gaps
Exclusion of participants with overweight and obesity at early stages of drug development may perpetuate downstream uncertainty, as later-phase trials and post-market surveillance must rely on incomplete evidence. As adiposity is known to affect drug metabolism, preventing individuals on either end of the spectrum of body sizes from participating in clinical trials may limit the development of accurate dosing guidelines, safety profiles, and efficacy measures. The lack of transparency about the representation of a range of body sizes in clinical research, including drug-development trials, also prevents patients, providers, and policymakers from making fully informed decisions about the applicability of interventions. Regulations promoting more inclusive study design and reducing unjustified exclusion based on BMI—or at least requiring subgroup analysis and more transparent reporting on the size of people included in trials—would help fill this knowledge gap and more equitably distribute the benefits and burdens of research. Absent such measures, drug-development research risks continuing to generate evidence that is incomplete or insufficiently generalizable to the populations most likely to use these interventions.
Justice and fair subject selection
This exclusion pattern raises a deeper question: when, if ever, are such exclusions ethically justifiable? Without concerted education efforts and normative shifts in research ethics, the status quo will continue to marginalize individuals with overweight and obesity and compromise the representativeness and validity of clinical research. The exclusion of people with high BMIs from clinical research perpetuates epistemic injustice, systematically excluding and devaluing certain bodies in the production of knowledge. It also violates the principle of fair subject selection, which is the dual idea that no population should be excluded without proportionate justification, and that all affected populations should have equitable access to both the burdens and benefits of research (Emanuel et al., 2000). Exclusion therefore perpetuates health inequities by producing medications and interventions that are not designed for the full range of body sizes across the population. From this perspective, BWB exclusions are not merely methodological choices but are ethically consequential decisions about who is permitted to contribute to—and benefit from—the knowledge generated from biomedical research.
Beyond explicit BMI-based exclusion, our results also reveal several indirect mechanisms through which people with overweight and obesity remain underrepresented in practice. Though some studies we identified allow for participants with a higher BMI to enroll or do not have BWB eligibility criteria to begin with, this does not guarantee that individuals with overweight and obesity will be proportionally represented when studies are implemented. We recognize that early phase drug-development trials are not designed to achieve proportional representation across population subgroups, as their primary aims are to assess safety, tolerability, and pharmacokinetics. Nonetheless, many studies we reviewed included eligibility criteria that participants be “overtly healthy,” have no “clinically significant” conditions, or be free from “any major illness” as determined by the investigator. These vague requirements reproduce exclusion indirectly, as they may function as proxies for body-size discrimination. Conversely, body size may be incorrectly assumed to be an indication of health status, despite the fact that health or illness may exist in people of any body size (Burgard, 2009).
Importantly, these indirect mechanisms of exclusion are unlikely to operate uniformly across populations. Given the well-documented intersections between BMI, race, ethnicity, gender, and socioeconomic status, such discretionary criteria may disproportionately exclude individuals from racial and ethnic minority groups, women, and gender-diverse populations who already experience higher burdens of chronic disease and structural barriers to health care access (Williams et al., 2024). Exclusion of individuals with common comorbidities of obesity like type 2 diabetes, high cholesterol, and hypertension may be more medically justifiable, particularly in drug development studies in which the intervention may interact with corresponding treatments for these conditions. However, these eligibility criteria may also be used to exclude people with overweight and obesity even if there is no explicit justification for exclusion based on those health conditions.
Structural injustice and stigma
For study participants, perceptions of stigma, prior experiences with weight-based discrimination, and mistrust in medicine or research may pose considerable barriers to participation for those with overweight and obesity (Puhl and Heuer, 2009). Even when eligibility is not explicitly prohibitive, individuals with overweight and obesity often encounter criticism regarding lifestyle decisions, competence, or adherence to health-promoting behaviors in clinical settings. Weight-based stigma therefore does not merely influence an individual’s willingness to participate in clinical research; it shapes who feels welcome, safe, and valued in both research and clinical environments. Over time, these experiences may contribute to lower health care utilization among people with overweight and obesity, reducing the likelihood that potential participants are reached through health system-based recruitment efforts (Washington et al., 2023).
These individual-level barriers are reinforced by institutional and infrastructural constraints within health care systems. The exclusion of people with high BMIs due to weight restrictions on medical equipment, such as MRI and CT machines, reflects broader patterns of weight discrimination, as many facilities lack bariatric devices and resources necessary to accommodate all patients. As a result, the underrepresentation of people with high BMIs in clinical research is both a cause and a consequence of inequitable medical care. Taken together, these dynamics contribute to a form of structural injustice in which large body size becomes synonymous with undesirability in science. Such practices undermine not only the integrity of the research enterprise but also the moral obligation to include diverse and representative populations in the co-production of medical knowledge. They further conflict with the tenets of the Health at Every Size movement by relying on BMI and weight as proxies for health rather than centering health metrics themselves (Burgard, 2009).
Normative implications and the need for reform
While there were a few studies in our sample that were specifically targeting pharmacokinetics and pharmacodynamics in populations with higher BMIs, these studies were few and far between. Ethical concerns related to representativeness in research become especially salient considering the growing prevalence of obesity and the increasing demand for medications targeted at mitigating obesity itself, like GLP-1s, known colloquially as anti-obesity medications. These drugs have contributed to the increasing medicalization of obesity and to the growing emphasis on pharmacological management, prioritizing biomedical intervention over attention to the broader social and structural determinants of health. Participants with high BMIs were, reasonably so, overrepresented in the clinical trials for GLP-1s, yet are frequently unable to participate in other drug-development trials for other medications. This equates to the historical use of female participants only in studies on reproduction, while they were excluded from other types of clinical trials (Bennett, 1993).
This pattern of selective inclusion raises concerns about the instrumentalization of fat bodies, whereby individuals with high BMIs are included only when their body size is the primary clinical concern but excluded when their involvement presents complexity or variability that could pose challenges for the study team or regulatory entity. These studies alone are unlikely to fill the knowledge gaps sufficiently to make the studies in lower-BMI populations more generalizable. They are also a less efficient use of limited research funding and resources than including all populations in drug-development trials would be.
Ethical principles such as justice and fair subject selection demand active efforts to dismantle participation barriers and build trust with populations that have historically been marginalized, stigmatized, and excluded. Consistent with how clinical research regulations have evolved to include other historically excluded populations, ethical research governance should treat the inclusion of individuals with overweight and obesity as the default, with exclusion permitted only in cases where clear scientific justification for their exclusion exists. Within this framework, it is not sufficient for study teams merely to apply BWB eligibility criteria; they must be prepared to articulate a compelling scientific and ethical rationale when exclusion is proposed. Transparent justification, which we did not frequently encounter in our search, is therefore a necessary but not sufficient condition for ethical permissibility, helping ensure that exclusion does not continue to function as an unexamined default. Without acknowledging and addressing these nuanced ethical dimensions, the biomedical research system risks perpetuating a cycle of exclusion that ultimately harms both individual and population-level health outcomes.
Limitations
Several limitations impacted our systematic search of ClinicalTrials.gov and its results. Although our search and inclusion criteria were selected to capture the studies most relevant to our aims, the final sample represents only a small fraction of all ongoing clinical research. As described in the Results, the sample was skewed toward early-phase studies, with relatively fewer Phase 3 and Phase 4 studies, which typically require more representative populations to assess broader clinical applications. Increased representation of these later phase studies may change the observed prevalence of BWB eligibility criteria, but we assert that inclusion of people of all sizes is ethically salient in all phases of clinical research.
Because detailed study protocols and internal documents (such as IRB materials) were not publicly available, we could not assess the full justification for size-based eligibility criteria if they exist in these resources. We did not contact study teams for enrollment information, but that approach has yielded valuable insights in prior work (Pestine et al., 2018). Additionally, ClinicalTrials.gov records may not be consistently updated, and registries do not require investigators to publicly report scientific or ethical justifications for inclusion or exclusion criteria, meaning that nuanced eligibility decisions may not have been captured. Taken together, these limitations highlight the need for greater transparency and accountability in clinical research regulations, especially for eligibility criteria that exclude a large proportion of the population.
Conclusion
Oversight bodies, sponsors, institutions, and investigators may consider the following questions for evaluating the ethical justifiability of BWB exclusions moving forward: (1) Is the exclusion scientifically necessary for the research question at hand? (2) If so, does the exclusion apply the principle of least restrictive means? (3) Is the justification for the exclusion both transparent and accountable to the population the research is intended to benefit? When these conditions are unmet, BWB exclusions become ethically indefensible and constitute discriminatory design rather than precautionary science. Policies that call for the inclusion of participants with a wide range of body sizes in drug-development trials are critical, and IRBs, researchers, and community members can partner to ensure their implementation (Pagarkar et al., 2023). Considering the well-documented marginalization of people with overweight and obesity in clinical and research settings, collaboration across design, education, and enforcement efforts is critical.
As stewards of justice in research governance, IRBs and other research governing bodies play a critical role in ensuring that research protocols meet and uphold ethical standards, including fair and equitable inclusion of participants. Given this obligation, reviewers and regulators should scrutinize study protocols that include BWB eligibility criteria. While these committees currently lack universal standards for how to evaluate such criteria, they are well-positioned to demand a clear, scientifically justified rationale for such limitations. IRBs and research ethics educators can work to ensure that researchers are not only aware of the potential for unjust participant exclusions but are also guided toward recruitment strategies and protocol designs that are inclusive to the furthest extent possible. Furthermore, IRBs can advocate for institutions and study sponsors to provide adequate accommodations to expand recruitment potential, like securing access to bariatric equipment. Without such oversight, BWB exclusions will persist as default eligibility criteria, perpetuating structural injustice and scientific blind spots.
The routine exclusion of people with high BMIs from drug-development trials, especially without clear scientific justification, is an ethically concerning practice that undermines the principle of justice in biomedical research. Body size, weight, or BMI should not themselves determine access to participation in clinical research for the reasons discussed above, yet our findings reveal that these factors are frequently listed as eligibility criteria with little rationale offered for their use on ClinicalTrials.gov. This practice is partially informed by biased assumptions about body size and health, not only restricting an individual’s access to the benefits of research participation but also compromising the validity and generalizability of safety and efficacy results. Subtle forms of exclusion, including infrastructural limitations and reductive definitions of health, further prevent people with high BMIs from participating in research. To generate research that is both scientifically robust and ethically appropriate, the clinical research enterprise must reject outdated metrics like BMI, confront weight stigma in research settings, and adopt inclusive study design practices that include diverse members of the population. While efforts to broaden eligibility criteria may slightly improve representation in the short term, the use of BMI measures to include or exclude participants perpetuates harmful assumptions about body size and health and wrongfully reinforces a flawed metric. Eliminating BWB eligibility criteria for drug-development trials is not only a matter of justice, but a requirement for producing relevant, trustworthy, and equitable scientific knowledge moving forward.
Footnotes
Acknowledgements
Thank you to colleagues at the National Institutes of Health’s Clinical Center Department of Bioethics, Johns Hopkins Bloomberg School of Public Health, and the Berman Institute of Bioethics for their thoughtful reviews of this manuscript.
Author note
The contributions conducted by both authors while at NIH are considered Works of the United States Government. The findings and conclusions presented in this paper are those of the authors and do not necessarily reflect the views of the NIH or the U.S. Department of Health and Human Services.
Ethical considerations
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the Intramural Research Program of the National Institutes of Health (NIH).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.