
Abstract
It is often assumed that empathy impairments are common in individuals with eating disorders (EDs), but empirical work has been limited and produced mixed results, making the clinical features and treatment needs of this population difficult to determine. Alexithymia, characterised by difficulties identifying and describing one’s own emotions, frequently co-occurs with EDs and is associated with atypical recognition of, and empathy for, others’ emotions. This study used an existing empathy for pain paradigm to determine whether atypical empathy in EDs stems from co-occurring alexithymia, rather than EDs per se. Empathy (specifically personal distress in response to others’ pain) was assessed in individuals with EDs (N = 21) and an alexithymia-matched control group (N = 22). Participants were simultaneously members of a high alexithymia (N = 16) or low alexithymia (N = 27) group, allowing the independent contributions of alexithymia and EDs to be determined. Participants judged the laterality of hands and feet in painful and non-painful situations, and the degree of empathic interference on response times was measured. Results indicated that observation of painful stimuli affected task performance in those with high levels of alexithymia more than those with low levels, but no effect of ED diagnosis was observed. These findings suggest that co-occurring alexithymia explains increased empathic personal distress in ED populations. Atypical empathy may therefore not be a core feature of EDs, and interventions aimed at improving empathy-related social functioning may only be necessary for patients who also have alexithymia. These findings emphasise the importance of determining the influence of co-occurring alexithymia when assessing empathy in clinical populations.
Feeding and eating disorders (hereafter EDs) are psychological disorders characterised by disturbed and inappropriate patterns of eating (American Psychiatric Association [APA], 2013). Three subtypes have been recognised: bulimia nervosa (BN) (associated with periods of bingeing, followed by inappropriate compensatory behaviour), anorexia nervosa (AN) (associated with emaciation, distorted body image, and an intense fear of gaining weight), and more recently, binge eating disorder (BED) (characterised by consumption of more food than most people would consume under similar circumstances and lack of control over eating behaviours). Although not defined as a core feature of EDs, deficits in social and emotional functioning, such as an atypical cognitive bias towards emotionally salient stimuli, impaired recognition and regulation of one’s own emotions, and a reduced ability to identify others’ emotions and other mental states, have often been reported in this population (Oldershaw et al., 2011). The ability to empathise is crucial for successful social and emotional functioning and has also been reported to be impaired in those with EDs (Gillberg, Råstam, & Gillberg, 1995; Morris, Bramham, Smith, & Tchanturia, 2014), though empirical evidence has been inconsistent (Courty et al., 2013; Hambrook, Tchanturia, Schmidt, Russell, & Treasure, 2008).
Although the concept of empathy encompasses multiple processes, it can be defined as comprising one’s affective response to one’s judgement of another’s emotional state (affect sharing) and the cognitive process of identifying another’s state (emotion identification; Coll, Grégoire, Eugène, & Jackson, 2017). The negative emotional state arising in the empathiser as a result of identification of the other’s negative state produces a state of personal distress in the empathiser, which is thought to be reduced when the aversive state is attributed to the other rather than the self. After this “self-other distinction” has occurred, the reduced personal distress may be accompanied by empathic concern for the other (Bird & Viding, 2014; Davis, 1980; Decety & Lamm, 2006; Moriguchi et al., 2007). Reduced empathic concern for others’ emotional states, through atypical affect sharing, emotion identification, or self-other distinction, is likely to impair social functioning more generally and place strain on relationships between individuals with ED and their support networks. As individuals with EDs are thought to use ED behaviours (such as restricting food intake, bingeing, and over-exercising) as a means of coping with emotional difficulties or distress (Wagener & Much, 2010), it is possible that atypical empathy and its consequences (such as reduced social support) may exacerbate ED symptoms. It has also been suggested that difficulties with empathy lead to poorer recovery from EDs (Gillberg, Rastam, & Gllberg, 1994), making increased understanding of these difficulties crucial. Determining whether empathy impairments are a genuine feature of EDs is therefore an urgent requirement, to optimise the design and implementation of suitable interventions, and to maximise successful treatment outcomes.
Multiple studies have observed difficulties in identification of others’ emotion in those with EDs (Harrison, Sullivan, Tchanturia, & Treasure, 2009; Kucharska-Pietura, Nikolaou, Masiak, & Treasure, 2004; Legenbauer, Vocks, & Ruddel, 2008; Pollatos, Herbert, Schandry, & Gramann, 2008), although findings have been mixed, and effect sizes are often small (Caglar-Nazali et al., 2014; Oldershaw et al., 2011). Previous investigation of the subsequent stages of empathy (beyond emotion identification, such as affect sharing and empathic concern) in EDs has relied almost exclusively, however, on self-report measures. Surprisingly, there is little evidence for reduced empathy in EDs using these measures, despite various anecdotal and clinical reports. Although some authors have found decreased levels of self-reported empathy in those with EDs (Morris et al., 2014), and in non-clinical samples with high levels of disordered eating (Costarelli, Demerzi, & Stamou, 2009), many studies have found no association between self-reported empathy and EDs (Courty et al., 2013; Guttman & Laporte, 2000; Hambrook et al., 2008; Lulé et al., 2014). When specific aspects of empathy are examined, in contrast to empathic concern, the personal distress facet of empathy is usually increased, rather than decreased, in ED samples in those studies where group differences are observed (Beadle, Paradiso, Salerno, & McCormick, 2013; Duchesne et al., 2012; Guttman & Laporte, 2002). To our knowledge, only one study has directly investigated online empathic responses of individuals with EDs to others’ emotional states (Cardi et al., 2015). In this study, participants viewed films of others in affective situations and were required to report their own emotional responses. No differences between the responses of those with and without EDs were observed.
Although assessing empathy objectively is challenging, tasks have been developed that are sensitive to the degree of personal distress evoked by another’s pain (Avenanti, Minio-Paluello, Bufalari, & Aglioti, 2009; Borgomaneri, Gazzola, & Avenanti, 2014; De Coster, Andres, & Brass, 2014). These tasks rely on objectively assessing responses to another’s pain, for example, by measuring muscle activity in response to another’s pain in the corresponding muscle (Avenanti, Bueti, Galati, & Aglioti, 2005; de Guzman, Bird, Banissy, & Catmur, 2016), neural activity while viewing others’ pain (Coll et al., 2017; Gu & Han, 2007; Jackson, Meltzoff, & Decety, 2005), or response times to stimuli depicting others in pain (Gu et al., 2012; Gu et al., 2010). Previous work has found, for example, that viewing others’ hands and feet in painful (relative to non-painful) situations leads to slower responses when performing a pain-irrelevant laterality judgement (indicating whether a right or left hand or foot was presented) (Gu et al., 2010). This task was therefore selected in this study to provide an objective assessment of empathy-related personal distress in those with, and without, a diagnosis of EDs.
In addition to providing an objective measure of empathy in EDs, this study also sought to test the impact of co-occurring alexithymia, a sub-clinical condition characterised by difficulties identifying and describing one’s own emotions (Nemiah, Freyberger, & Sifneos, 1976), on empathy in those with EDs. Alexithymia has consistently been associated with atypical empathy (Bernhardt & Singer, 2012; Bernhardt et al., 2013; Moriguchi et al., 2007; Silani et al., 2008), including increased self-reported personal distress (Guttman & Laporte, 2002; Moriguchi et al., 2006; Patil & Silani, 2014) in those with and without EDs (Beadle et al., 2013). Alexithymia is also associated with developmental dysfunction, or atypical structure, of the anterior insula (AI) and anterior cingulate cortex (ACC) (Bernhardt & Singer, 2012; Moriguchi et al., 2007; Singer, Critchley, & Preuschoff, 2009), which are some of the neural regions supporting empathy (Bernhardt & Singer, 2012; Decety, 2011; Lamm, Rütgen, & Wagner, 2017), and areas in which both function and structure are associated with individual differences in personal distress (Banissy, Kanai, Walsh, & Rees, 2012; Cheetham, 2009; Eres, Decety, Louis, & Molenberghs, 2015).
Importantly for this study, an elevated prevalence of alexithymia relative to the typical population has been observed in individuals with AN, BN, and BED (Bourke, Taylor, Parker, & Bagby, 1992; Cochrane, Brewerton, Wilson, & Hodges, 1993; Jimerson, Wolfe, Franko, Covino, & Sifneos, 1994; Pinaquy, Chabrol, Simon, Louvet, & Barbe, 2003; Rozenstein, Latzer, Stein, & Eviatar, 2011), meaning it could be alexithymia, rather than EDs themselves, that explains atypical empathy in those with EDs. Indeed, previously inconsistent findings relating to empathy in EDs suggest considerable heterogeneity in the ED population, with some individuals self-reporting increased personal distress and reduced empathic concern, and some not. Explaining this heterogeneity is clearly a valuable research aim as it will enable personalised interventions to be administered; those patients who experience increased personal distress can be taught strategies to engage in self-other distinction, reducing their levels of personal distress and increasing empathic concern (de Guzman et al., 2016; Santiesteban et al., 2012). Alexithymia is a plausible candidate to explain the empathy-related heterogeneity in those with EDs; the “alexithymia hypothesis” (Bird & Cook, 2013) posits that, where alexithymia co-occurs with clinical disorders, it may explain atypicalities in emotion processing and empathy, over and above the disorder itself (Bird, Press, & Richardson, 2011; Bird et al., 2010; Brewer, Cook, Cardi, Treasure, & Bird, 2015; Cook, Brewer, Shah, & Bird, 2013; Oakley, Brewer, Bird, & Catmur, 2016). Indeed, alexithymia has been found to explain the emotion identification stage of empathy in those with EDs (Brewer et al., 2015). It is therefore possible that the mixed findings concerning atypical empathy in EDs are due to previous samples differing according to alexithymia presence and severity; where deficits have been observed, alexithymia rates may have been elevated in the ED group, leading to observation of a group difference. As most previous studies have not measured alexithymia, or matched ED and control groups according to alexithymia severity, it has been impossible to determine the independent contribution of alexithymia and EDs to empathy. This study was therefore a preliminary investigation into the relative contributions of alexithymia and EDs to the increased personal distress seen in individuals diagnosed with EDs, using a self-report empathy measure and an objective test of responses to another’s pain.
Method
Participants
A total of 21 females with an ED (18 AN, three BN; mean age = 25.9 years, SD = 6.0) and 22 females with no past or present psychological diagnosis (mean age = 23.0 years, SD = 6.3) participated in this study: 18 of the 21 ED participants were right handed (three left handed), and all 22 of the control participants were right handed. Participants were pre-screened using the Toronto Alexithymia Scale (TAS-20; Bagby, Parker, & Taylor, 1994) to ensure a broad range of alexithymia scores in each group. The ED and control groups were therefore matched according to alexithymia severity (t(41) = 1.35, p = .19). Seven participants in the control group and nine in the ED group met the criterion for severe alexithymia (TAS-20 score > 60). The 16 individuals reaching this criterion therefore comprised the high alexithymia group, and the 27 individuals not meeting this criterion comprised the low alexithymia group. These groups did not differ according to ED symptomatology, measured by the Eating Disorder Examination Questionnaire (EDE-Q; Mond, Hay, Rodgers, & Owen, 2006) (t(41) = 1.16, p = .25). The study therefore had a between-participants design, in which participants belonged to one of two ED groups and one of two alexithymia groups simultaneously.
All individuals with EDs were diagnosed by independent clinicians, according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) or Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V; APA, 2013) criteria. Fourteen of the 21 ED participants, who were diagnosed more than 1 year prior to study participation, also completed the EDs section of the research version of the SCID (Structured Clinical Interview for DSM-IV; First, Spitzer, Gibbon, & Williams, 2002) to assess current functioning. One member of the ED group had not previously been diagnosed by a clinician, but scored above the recommended cut-off for clinical significance on the EDE-Q, had a body mass index (BMI) below the healthy weight cut-off (16.5), and met criteria for “Anorexia, binge-purging type” according to the SCID. This participant was not an outlier in any analysis, and her exclusion did not alter the pattern of results. The ED group had significantly higher ED symptomatology (M = 4.28, SD = 1.57), assessed by the EDE-Q, than the control group (M = 1.39, SD = 1.36) (t(40) = 6.17, p < .01).
The two ED groups did not differ according to age (t(41) = 1.42, p = .16) or IQ (t(41) = 0.84, p = .41), measured by the Wechsler Abbreviated Scale of Intelligence (Wechsler, 2011). The high and low alexithymia groups were also matched according to age (t(41) = 0.45, p = .66) and IQ (t(41) = 1.80, p = .08). Depression levels were measured in all participants using the Depression, Anxiety and Stress Scale (DASS; Lovibond & Lovibond, 1995). Depression differed significantly between the ED (M = 24.0, SD = 9.89) and control (M = 5.29, SD = 6.73) groups (t(41) = 7.20, p < .01), but not between the high and low alexithymia groups. Anxiety was higher in the ED (M = 14.64, SD = 10.52) than in the control (M = 5.71, SD = 7.65) group (t(41) = 3.19, p = .003) and higher in the high alexithymia (M = 17.13, SD = 10.84) than in the low alexithymia (M = 6.22, SD = 7.29) group (t(41) = 3.56, p = .002). Stress was higher in the high alexithymia (M = 30.56, SD = 22.77) than in the low alexithymia (M = 14.93, SD = 10.56) group (t(41) = 3.07, p = .004). All participants also completed the Interpersonal Reactivity Index (IRI) (Davis, 1980), assessing four separate facets of empathy: perspective taking (the tendency to take another’s perspective), fantasy (the tendency to identify with fictional characters), empathic concern (the tendency to feel compassion and concern for others), and personal distress (the tendency to experience negative emotions in response to another’s negative state). All questionnaire measures were completed prior to the experiment.
Stimuli and materials
Stimuli were a subset of those used in a previous empathy for pain task (Gu et al., 2012; Gu et al., 2010). The stimulus set comprised 160 digital colour photographs of a hand or a foot, in either a painful or non-painful situation. Equal numbers of left and right, male and female hands and feet were viewed. Painful stimuli depicted the hand or foot being harmed in some way by an object encountered in everyday life, and a corresponding non-painful stimulus, showing the same (left or right) hand or foot with the object in an unthreatening position, existed for each painful stimulus (see Figure 1 for examples). All stimuli were presented from the first-person perspective. Stimuli were presented on a 15″ LCD screen and subtended 17° × 11° when viewed from a distance of 60 cm.
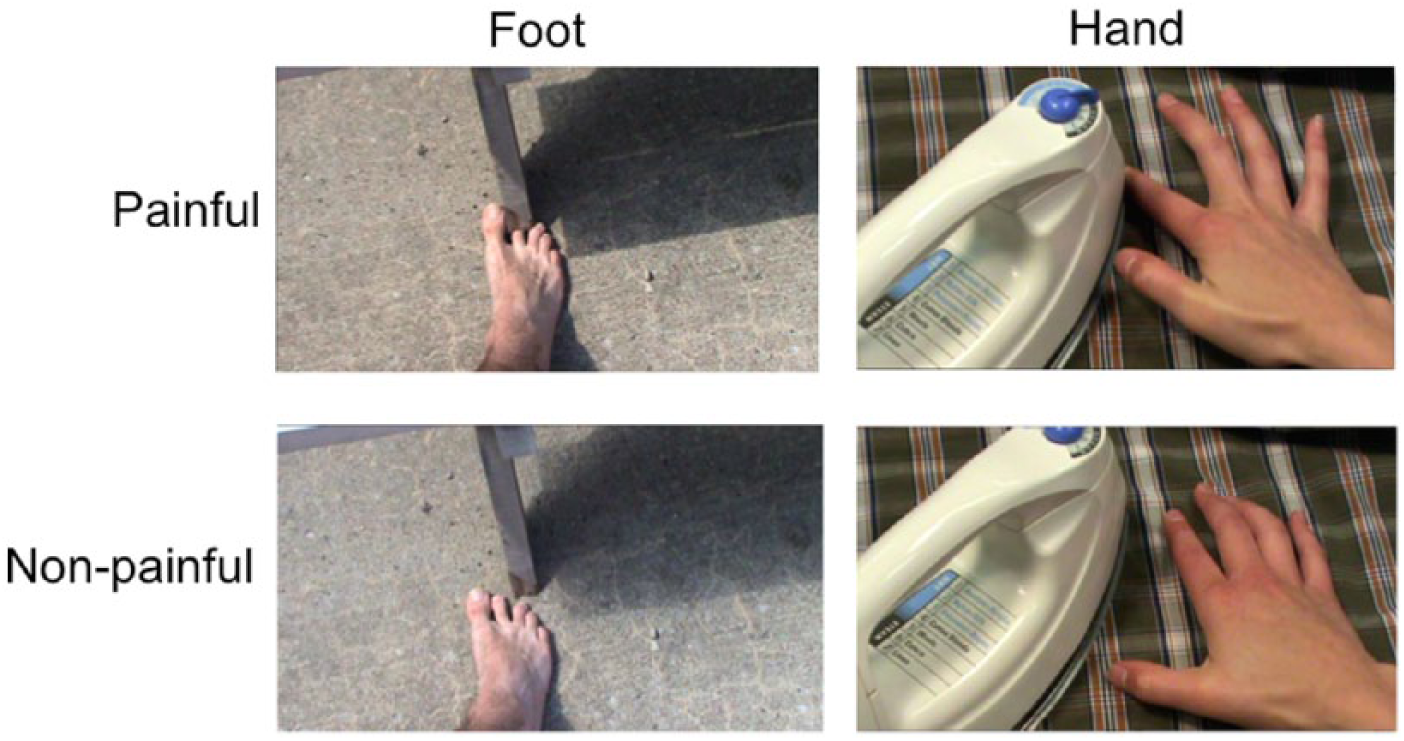
Examples of stimuli, depicting right and left hands and feet in painful and non-painful situations. Stimuli were a subset of those used by Gu et al. (2012).
Procedure
Stimuli were presented for 2,500 ms and followed by an inter-stimulus interval of 1,500 ms. Participants were required to perform a speeded laterality judgement (indicating whether the image depicted a right or left hand or foot) in the 4,000 ms following stimulus onset. Each stimulus was viewed once, yielding 160 trials. Participants responded by pressing the left or right arrow key on a laptop keyboard. All participants responded using their index and middle fingers of their right hand, to respond with “left” and “right,” respectively.
Results
Self-reported empathy
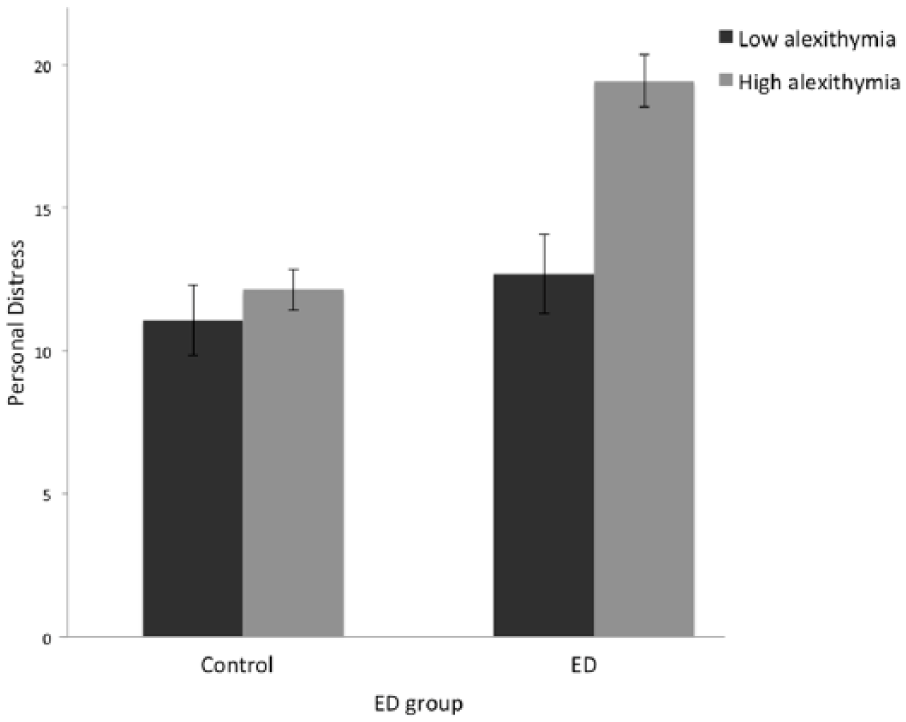
Analysis of self-reported empathy was conducted using alexithymia group (high or low) × ED group (ED or control) analyses of variance (ANOVAs) for each sub-scale of the IRI. Both the main effects of alexithymia (F(1, 39) = 9.06, p < .01, η = .19, 95% confidence interval [CI] for η [0.02, 0.38]) and ED diagnosis (F(1, 39) = 11.79, p < .01, η = .23, 95% CI for η [0.04, 0.42]) were significant with respect to personal distress scores (Figure 2) and were qualified by a significant interaction between these factors (F(1, 39) = 4.78, p = .035, η = .11, 95% CI for η [0, 0.30]). The high alexithymia group (M = 16.25, SD = 4.40) reported higher personal distress than the low alexithymia group (M = 11.85, SD = 4.77), and the ED group (M = 15.45, SD = 5.37) reported higher personal distress than the typical group (M = 11.43, SD = 3.85). Post hoc comparisons, however, indicated that the perception of personal distress in response to the pain of another was only elevated—in comparison with the low alexithymia control group—when an individual had both alexithymia and an ED. Those with high alexithymia and an ED (M = 19.44, SD = 2.74) reported significantly higher personal distress than those with low alexithymia and an ED (M = 12.69, SD = 5.02) (t(20) = 3.80, p = .003), those with high alexithymia and no ED (M = 12.14, SD = 1.86) (t(14) = 3.54, p = .006), and those with low alexithymia and no ED (M = 11.07, SD = 4.57) (t(21) = 4.78, p < .001). There was also a significant main effect of alexithymia on the fantasy scale (FS) of the IRI (F(1, 39) = 8.44, p < .01, η = .18, 95% CI for η [0.02, 0.37]), whereby the low alexithymia group (M = 18.30, SD = 8.47) reported increased fantasising relative to the high alexithymia group (M = 11.25, SD = 4.91). The low alexithymia group (M = 20.74, SD = 4.51) also reported higher empathic concern for others than the high alexithymia group (M = 17.75, SD = 5.03) (F(1, 39) = 4.16, p < .05, η = .10, 95% CI for η [0, 0.28]). No further significant main or interaction effects were observed.
Bar graphs showing significantly slower responses to painful than to non-painful stimuli (a) in both the ED and control groups and (b) in both the high and low alexithymia groups.
Empathy for pain task
Analysis of the accuracy of the laterality judgement, estimated by d′ (Green & Swets, 1966) using a two-way (ED group × alexithymia group) ANOVA produced no significant main or interaction effects for the painful–non-painful d′ difference. Accuracy, therefore, appears to be unaffected by either alexithymia or ED symptom severity in the current task.
RT analyses were conducted having removed inaccurate trials and any trials in which RTs were more than 2 SDs from the participant’s mean RT. As in previous studies, RTs were significantly greater when judging laterality in painful than in non-painful situations, in both the ED group (painful mean RT = 929 ms, SD = 231 ms; non-painful RT = 909 ms, SD = 216 ms) (t(21) = 3.20, p < .01) and the typical group (painful mean RT = 949 ms, SD = 171 ms; non-painful RT = 919 ms, SD = 164 ms) (t(20) = 3.86, p < .01), as well as in the low alexithymia group (painful mean RT = 891 ms, SD = 183 ms; non-painful RT = 875 ms, SD = 172 ms) (t(26) = 2.61, p = .015) and the high alexithymia group (painful mean RT = 1019 ms, SD = 212 ms; non-painful RT = 981 ms, SD = 207 ms) (t(15) = 5.68, p < .01).
The difference in RT between painful and non-painful trials (“empathic interference effect”) was calculated for each participant. Group analyses, using a 2 (alexithymia group) × 2 (ED group) ANOVA indicated that empathic interference effect was significantly greater in the high alexithymia (M = 38 ms, SD = 27 ms) than in the low alexithymia group (M = 16 ms, SD = 32 ms) (F(1, 39) = 5.53, p = .024, η = .12, 95% CI for η [0, 0.32]). A non-significant main effect of ED group (F(1, 39) = 1.25, p = .27, η = .03, 95% CI for η [0.01, 0.06]) and non-significant interaction term (F(1, 39) = 0.09, p = .77, η < .002, 95% CI for η [0.001, 0.004]) indicated that ED diagnosis itself did not affect the empathic interference effect (Figure 3).
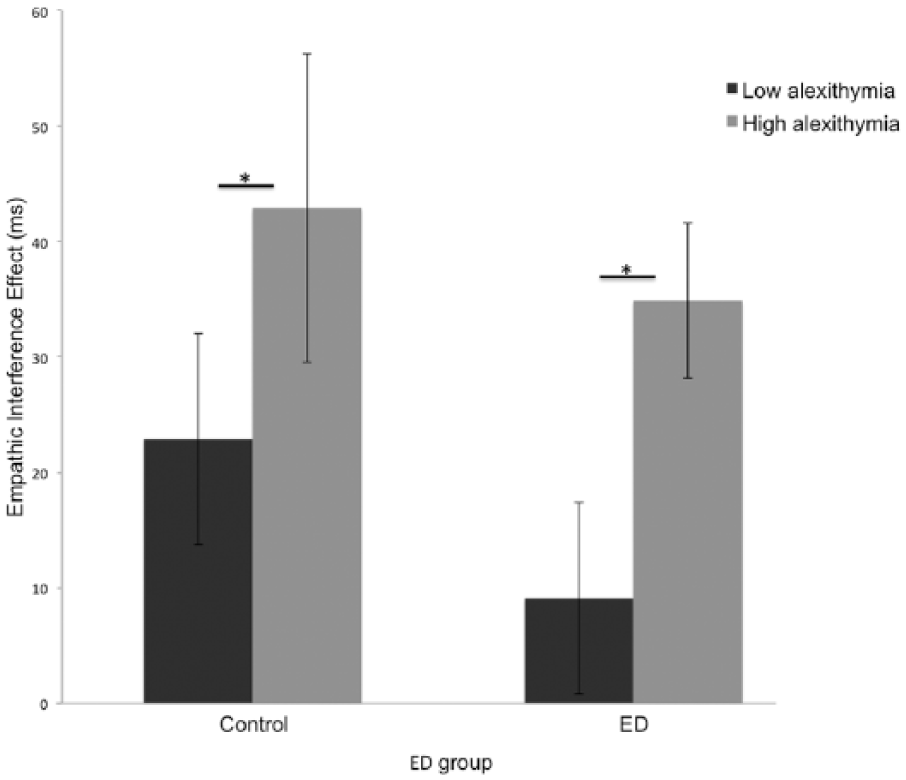
Bar graph showing the significant main effect of alexithymia group, but not ED group, on empathic interference effect, whereby high alexithymia was associated with greater empathic interference effect than low alexithymia.
It remained possible that the effect of alexithymia was due to co-linearity between alexithymia and ED diagnosis, ED symptom severity, or depression, anxiety, or stress symptom severity. To confirm that this was not the case, a series of six analyses of covariance (ANCOVA) was performed in which ED diagnosis or symptom severity (EDE-Q total score), along with depression, anxiety, or stress DASS scores, were included as covariates. In each case, a significant main effect of alexithymia group was observed (all Fs > 4.12, all ps < .05), except for the ANCOVA controlling for ED group and anxiety, where the main effect of alexithymia group fell to a trend level (F(1, 39) = 3.88, p = .056).
When RTs on painful and non-painful trials were analysed separately, a two-way (ED group × alexithymia group) ANOVA for painful trials suggested that individuals with high alexithymia (M = 1019 ms, SD = 212 ms) made slower responses to painful stimuli than did those with low alexithymia (M = 891 ms, SD = 183 ms) (F(1, 38) = 4.13, p = .049, η = .11, 95% CI for η [0.06, 0.20]). A non-significant main effect of ED group and non-significant ED group × alexithymia group interaction suggested that ED diagnosis was unrelated to RTs to painful stimuli. An equivalent ANOVA for non-painful RTs revealed no significant effects. Taken together, these results indicate that the association between alexithymia and painful-non-painful RT difference is driven by increased RTs to painful stimuli, rather than decreased RTs to non-painful stimuli.
Discussion
This study was a preliminary investigation into empathy for others’ pain, and its relationship with alexithymia, in individuals with and without EDs. Findings suggested that increased alexithymia was associated with increased empathic personal distress as indexed by the empathic interference effect in an empathy for pain task (the difference between individuals’ RTs to discriminate hand or foot laterality in painful and non-painful situations). This effect remained once ED diagnosis and depression were controlled for, and ED diagnosis itself was unrelated to the empathic interference effect. Similarly, self-reported personal distress was higher in the high than in the low alexithymia group, and in the ED than in the control group, meaning that high alexithymia had a particularly strong impact in the ED group. This is consistent with previous findings of high self-reported personal distress in those with alexithymia (Guttman & Laporte, 2002; Moriguchi et al., 2006; Patil & Silani, 2014) and EDs (Beadle et al., 2013; Duchesne et al., 2012; Guttman & Laporte, 2002), and a relationship between increased personal distress and alexithymia in those with EDs. Conversely, self-reported empathy data indicated that those with low alexithymia were more likely to fantasise and had increased empathic concern for others than those with high alexithymia. ED diagnosis itself, however, was unrelated to fantasising and empathic concern, likely due to the fact that the two groups were matched according to alexithymia.
The higher empathic interference effect (painful RT – non-painful RT) observed in the high alexithymia group parallels Gu et al.’s (2012) observation of an increased empathic interference effect in individuals with AI lesions in a similar task and appears to be driven by slower responses to painful stimuli, as opposed to faster responses to non-painful stimuli, in those with high alexithymia. Alexithymia has consistently been shown to be associated with atypicalities in AI functioning (Bernhardt & Singer, 2012; Moriguchi et al., 2007; Singer et al., 2009), meaning similarities between individuals with high alexithymia and those with AI lesions are unsurprising. It is worth noting that where previous studies have observed reduced empathy in those with alexithymia (e.g., Grynberg, Luminet, Corneille, Grèzes, & Berthoz, 2010; Guttman & Laporte, 2002; Moriguchi et al., 2007; Moriguchi et al., 2006; Patil & Silani, 2014), this is usually when the empathic concern or perspective-taking facets of empathy are analysed. In the same studies, however, alexithymia was associated with increased levels of personal distress. Self-report data in this study showed the same pattern of results. As the current behavioural paradigm is best characterised as assessing personal distress (rather than empathic concern), an increased empathic interference effect in those with alexithymia is to be expected.
There are at least two plausible explanations for the increased levels of personal distress in those with alexithymia. The first is that increased personal distress occurs due to reduced emotion regulation in those with alexithymia. Individuals with alexithymia report reduced emotion regulation (Stasiewicz et al., 2012; Venta, Hart, & Sharp, 2013), and atypical regulation strategies, with a greater reliance on maladaptive emotion suppression, rather than reappraisal techniques, when attempting to regulate their own emotions (Swart, Kortekaas, & Aleman, 2009). Furthermore, it has been suggested that simply identifying and naming one’s own emotional state serves to reduce the intensity of that state (Foland-Ross et al., 2010; Lieberman et al., 2007; Mazefsky & White, 2014), and impaired ability to identify and describe one’s emotions (which is the defining feature of alexithymia) would result in reduced opportunity to utilise this system for emotion regulation. As AI and ACC are known to play a role in emotional regulation (Goldin, McRae, Ramel, & Gross, 2008), it is likely that atypical function of these areas in those with alexithymia prevents these individuals from regulating their emotional state, leading to increased personal distress, and in turn, delayed responses to painful stimuli.
The second potential explanation for increased personal distress in alexithymia is that self-other distinction is reduced in these individuals. When viewing another’s pain, one must distinguish between the emotional state of the self and the other, to correctly attribute the painful state to the other. As the AI is known to play a role in distinguishing between representations of the self and other (Denny, Kober, Wager, & Ochsner, 2012; Qin et al., 2012; Qin & Northoff, 2011), atypical function of this area in alexithymia (and those with AI lesions) may cause difficulties making this distinction. Indeed, recent evidence suggests that the ability to automatically inhibit imitation of others’ actions (a process known to rely on self-other distinction) varies as a function of alexithymia (Sowden, Brewer, Catmur, & Bird, 2016). Individuals with alexithymia may, therefore, experience increased personal distress in response to another’s pain due to less well-defined boundaries between the self and other. This explanation remains consistent with the high self-reported personal distress observed in individuals with alexithymia (Guttman & Laporte, 2002; Moriguchi et al., 2006; Patil & Silani, 2014); others’ pain is more personally distressing when representations of the self and other are less separable, as the state is not attributed to the other rather than the self. Interestingly, this explanation is consistent with recent evidence suggesting that those with alexithymia exhibit poor interoception (the ability to detect the internal state of the body) (Brewer, Cook, & Bird, 2016; Herbert, Herbert, & Pollatos, 2011; Murphy, Brewer, & Bird, 2017; Murphy, Catmur, & Bird, 2018; Shah, Hall, Catmur, & Bird, 2016), and that effective interoception is crucial for representing the self as distinct from others (Quattrocki & Friston, 2014; Seth, 2013). It is worth noting that, as the images viewed in the current paradigm were presented from the first-person perspective, self-other distinction may be particularly difficult. Whether the increased personal distress observed in those with alexithymia in the current paradigm arises due to poor emotion regulation or reduced self-other distinction remains to be seen, but as previous evidence suggests that both processes are compromised in alexithymia, it is likely that both contribute to the increased empathic interference effects in the current task. The extent to which each process contributes remains a question for future research.
In contrast to the impact of alexithymia, ED symptomatology was unrelated to the empathic interference effect. In line with the alexithymia hypothesis, it seems that alexithymia, rather than ED presence or severity per se, contributes to atypicalities in empathic personal distress in these individuals. Where atypical personal distress has previously been observed in those with EDs, this is likely explained by co-occurring alexithymia. It should be noted, however, that although EDs did not affect the empathic interference effect, individuals with EDs did self-report increased personal distress. The effect of EDs on self-reported personal distress was particularly pronounced, however, in those with co-occurring high alexithymia, suggesting that the effect of alexithymia is especially pronounced in this population. As alexithymia has been found to predict a number of emotional abilities in clinical groups, such as emotion recognition (Cook et al., 2013; Oakley et al., 2016), empathic response of the insula to others’ pain (Bird et al., 2010), and emotion expression (Trevisan, Bowering, & Birmingham, 2016) in autism spectrum disorder (ASD), and emotion recognition in EDs (Brewer et al., 2015), it is possible that alexithymia also explains atypicalities in other facets of empathy in those with EDs, such as empathic concern. Whether this is the case remains an outstanding question. The current finding allows the literature on atypical empathy in EDs to be disambiguated, suggesting that individuals with EDs only exhibit increased empathic personal distress if they have co-occurring alexithymia. Atypical empathy is therefore unlikely to be a core feature of EDs, although examination of additional empathy facets (empathic concern in particular) in alexithymia-matched ED and control groups is also necessary to draw this conclusion. The current findings suggest that clinical treatment outcomes may vary considerably in those with high and low alexithymia, and that interventions aiming to improve emotional understanding, empathy, and social interactions should be tailored according to patients’ alexithymia severity.
Overall, the current findings suggest that, as in individuals with ASD (Bird et al., 2010), atypical performance on an empathy for pain task in individuals with EDs depends on co-occurring alexithymia, rather than ED presence or severity per se. In line with the alexithymia hypothesis (Bird & Cook, 2013), alexithymia may account for atypical empathy, where observed, in those with EDs. Specifically, the current task implicates alexithymia in increased empathic personal distress, likely due to a reduced ability to regulate the emotional contagion experienced when viewing others’ pain, or to reduced ability to distinguish between the self and others. Although further work is required to determine the relative contribution of each these factors to increased personal distress in those with alexithymia, these findings have implications for both ED research and intervention. They suggest that research concerning empathy, and other emotional processes, in ED populations should measure and control for alexithymia severity, to independently investigate alexithymia and ED symptomatology. The findings also suggest that emotion- and empathy-based clinical interventions should be tailored to individual ED patients according to alexithymia severity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent
All participants gave informed consent prior to taking part in this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Health and safety
All mandatory laboratory health and safety guidelines were complied with during data collection for this study.