
Abstract
Perception of one’s own body in time and space is a fundamental aspect of self-consciousness. It scaffolds our subjective experience of being present, in the here and now, a vital condition for our survival and well-being. Depersonalisation (DP) is characterised by a distressing feeling of being “spaced out,” detached from one’s self, as well as atypical “flat” time perception. Using an audio-tactile paradigm, we conducted a study looking at the effect of DP experiences on peripersonal space (PPS)—the space close to the body—and time perception. Strikingly, we found no difference in PPS perception in people with higher DP experiences (High DPe) versus low occurrences of DP experiences (Low DPe). To assess time perception, we used the mental time travel (MTT) task measuring the individuals’ capacity to take one’s present as a reference point for situating personal versus general events in the past and the future. We found an overall poorer performance in locating events in time relative to their present reference point in High DPe. By contrast, Low DPe showed significant variation in performance when answering to relative past events, while High DPe did not. Our study sheds light on the close link between altered sense of self and egocentric spatiotemporal perception in individuals with DP experiences, the third most common psychological symptom in the general population.
Introduction
Adaptive bodily responses to constantly changing environments rely on accurate perception and representation of one’s body in time and space. Depersonalisation (DP) is a condition typically characterised by subjective feelings of detachment from one’s self, one’s body, or even reality itself (Sierra & Berrios, 1997). People experiencing DP report a qualitatively dramatic change in their sense of self (Sierra & David, 2011), and they may feel “unreal,” “spaced out,” not present, move through life like a robot or a machine (Sierra, 2009; Simeon & Abugel, 2006) or on “automatic pilot”: “I look in the mirror and it doesn’t feel like myself I’m looking at. It’s like I’m floating, not actually experiencing the world, and slowly fading away into nothing. It’s like I’m on autopilot in somebody’s else body” (Perkins, 2021, p. 198).
The condition was extensively studied in the late 19th and early 20th centuries, by both psychiatrists and philosophers (Dugas & Moutier, 1911; Ribot, 1885) before being relatively neglected until very recently, when several authors approached DP from different theoretical and empirical angles (Billon, 2017; Ciaunica, Seth, et al., 2022; Gerrans, 2019; Medford, 2012; Sierra, 2009; Simeon & Abugel, 2006; see Millman et al., 2021; Salami et al., 2020, for a recent review and discussion).
Transient DP experiences affect between 1% and 2% of the population (Hunter et al., 2004), often associated with everyday phenomena such as fatigue, sleep deprivation, or travelling to new places (Hunter et al., 2004; Salami et al., 2020; Tibubos et al., 2018; van Heugten-van der Kloet et al., 2015). When DP symptoms become chronic and debilitating, it may indicate the presence of a clinical Depersonalisation-Derealisation Disorder (DPD) (Diagnostic and Statistical Manual of Mental Disorders, 4th ed., text rev., DSM-IV-TR), 1 with between 0.95% and 2.4% of the general population suffering from DPD (Hunter et al., 2004; Lee et al., 2012).
Experiences of DP rank as the third most common psychological symptom reported (after anxiety and low mood; Simeon et al., 2003), often following severe stress, traumatic life events, or drug use, with onset most commonly occurring during adolescence (Baker et al., 2003, 2007). Remarkably, although symptoms of DP are increasingly being recognised in both clinical and non-clinical settings, their importance and the mechanisms that underlie them are only now being addressed and remain poorly understood.
A consistent feature of DP is the presence of anomalous body experiences, categorised by Sierra (2009) into four prominent types: (1) lack of body ownership, (2) feelings of loss of agency, (3) disembodiment feelings, and (4) somatosensory distortions. Previous theoretical and empirical work has demonstrated disrupted physiological responses in patients with DP, compared with healthy individuals (Dewe et al., 2018; Farmer et al., 2021; Owens et al., 2015; Sierra et al., 2002). DP has also been linked to disrupted activity in neuronal regions underlying somatic processing (Lemche, Brammer, et al., 2013; Lemche, Surguladze et al., 2013) and the vestibular system (Jáuregui Renaud, 2015), which is responsible for providing information about the body’s position in space (Ferrè & Haggard, 2016).
Several studies have found that people with DP experiences show atypical integration of multisensory body-related signals. For example, they are more likely to experience the rubber hand illusion (see also Braithwaite et al., 2017) and mirror-pain synaesthesia (Bowling et al., 2019). Previous quantitative and qualitative studies also report that DP is related to differences in self/other distinction at the level of body perception (Adler et al., 2016; Bowling et al., 2019; Ciaunica, McEllin, et al., 2022; Farmer et al., 2021; Woźniak et al., 2023). Crucially, previous works illustrate that multisensory integration of bodily signals plays a key role in structuring our basic sense of self, i.e., the subjective experience of an “I” or “self,” bound to my body and distinct from the world and others (Blanke & Metzinger, 2009; Gallagher, 2000; Gallese & Sinigaglia, 2010, 2011; Park & Blanke, 2019; Qin et al., 2020; Tsakiris, 2017). Importantly, multisensory signals relevant to the sense of self are not limited to the body itself, but they equally extend within one’s peripersonal space (PPS). PPS refers to the immediate zone surrounding the body where the self interacts with the environment (Rizzolatti et al., 1997), and it is typically represented by enhanced multisensory integration and faster reaction time (RT) to objects near the body. Thus, it has been suggested that PPS indexes the spatial self, i.e., the experience of being a bodily self in space, which contributes to the maintenance of a coherent representation of our basic sense of self in relation to the external world (Blanke et al., 2015).
DP is associated with anomalous self-location in space, whereby people report feelings of being “spaced-out” or “floating” above one’s body (Ciaunica et al., 2020; Perkins, 2021; Simeon & Abugel, 2006). Specific alterations to the perception of space are thus very common, including problems with the accurate perception of distances (objects seeming further away or closer than they really are) and feelings of disorientation (including getting lost in familiar places) (Ciaunica et al., 2023). People with DP also report feelings of space expanding or diminishing, perception of objects or space being flattened, and increased awareness of space itself (Simeon & Abugel, 2006). These alterations constrain people’s ability to feel fully present in their lives, to relate to others, and to participate in daily activities.
Notably, anomalous perception in the extension of PPS has been reported in other self-disorders (Di Cosmo et al., 2018; Ferroni, Ardizzi, et al., 2022; Ferroni & Gallese, 2022; Lee et al., 2021), not only in schizophrenia patients but also in healthy people with high schizotypal traits, often characterised by a high prevalence of dissociative states (for a comparative view, see Sass et al., 2013). However, the relationship between PPS representation and DP experiences remains an open question.
Along with this spatial dimension, time perception is another core aspect of human experiences, and a recurrent theme in psychopathology, for which there is increasing awareness in both neuroscientific and philosophical approaches (Bonnot et al., 2011; Dorato & Wittmann 2020; Gómez et al., 2014; Kent et al., 2022; Vogel, Falter-Wagner et al., 2020; Vogel, Jording et al., 2020). Indeed, numerous self-reports indicate that DP experiences involve altered sensations of the passing of time in terms of perceived duration and flowing, anomalous subjective recall, with a lack of “plot” or narrative in one’s life (Ciaunica & Charlton, 2018), suggesting a potential alteration of spatiotemporal processing in individuals suffering from the condition (Ciaunica, Roepstorff, et al., 2021; Perkins, 2021; Sierra, 2009; Simeon & Abugel, 2006). Alterations of subjective time and space perception in relation to one’s bodily self have been consistently reported in relation to DP (Perkins, 2021; Sierra, 2009; Simeon & Abugel, 2006). Yet, the question of how exactly DP affects PPS perception and temporal perspective remains to be addressed.
To address these key questions, we have conducted a lab-based study examining the multisensory processing of self-centred spatiotemporal coordinates in healthy individuals with low and high occurrences of DP experiences. Two well-validated paradigms have been used. The first paradigm measures the extension and quality of PPS perception based on an audio–tactile interaction task with approaching sounds (Canzoneri et al., 2012; Ferroni et al., 2020). This approach, grounded in neurophysiology, offers a valid implicit method to quantify PPS perception and self–other boundary by estimating the parameters of PPS.
In addition, to examine time perception in relation to DP experiences, we implemented the mental time travel (MTT) task (Arzy et al., 2008). MTT assesses the capacity to construct one’s own temporal perspective towards the past and the future by referring to one’s personal experience. Specifically, MTT tasks require individuals to think about themselves at a specific position in time and to temporally locate the happening of events already passed and yet to happen. By assessing individuals’ ability to think about future and past events with respect to their own position in time, this method is able to detect emerging differences in time structuring in individuals with different subjective experiences, such as between younger and older people (Anelli et al., 2016) or between healthy individuals and patients with brain lesions (Anelli et al., 2018; Ciaramelli et al., 2021).
Given the well-established similarities between the schizophrenic spectrum and depersonalisation disorder, including their own subclinical manifestations (i.e., schizotypy and experiences of depersonalisation) (e.g., Millman et al., 2021; Sass et al., 2013, 2018), we expected to detect alterations in egocentric processing of PPS in people reporting a high level of depersonalisation experiences (i.e., the subclinical manifestation). Indeed, previous findings have highlighted an atypical representation and boundaries of PPS in other self-disorders such as schizophrenia (Ferroni, Ardizzi, et al., 2022; (Ferroni and Gallese, 2022)) and high schizotypy (Di Cosmo et al., 2018). Specifically, as one of the main characteristics of these subclinical manifestations is represented by a sense of self-detachment (a sense of separation from certain aspects of everyday experience, be it their body, their sense of self, or the external world), we hypothesised shallower PPS boundaries in people with high levels of DP experiences, indicating a weaker demarcation between the self and the world. In addition, considering previous evidence on altered time perception in psychosis (Berna et al., 2016; Brébion et al., 2020; d’Argembeau et al., 2008; Hazan et al., 2019), we expected high DP level participants to display a weaker ability to take themselves as a reference point for locating events in time.
Materials and methods
Participants
Recruitment was conducted via the University of Parma mailing channels, social media, and flyers distributed across the University campuses. All the tasks and questionnaires of our study were administered in Italian, and all participants were Italian nationals. Initial prescreen for DP was conducted on 240 participants via an online survey using the Cambridge Depersonalisation Scale (CDS-29: Sierra & Berrios, 2000). CDS-29 is a 29-item standard questionnaire used to evaluate the severity of occurrence of depersonalisation experiences by asking participants to estimate the frequency and duration of such experiences in the past 6 months. The total score (between 0 and 290 points) is calculated by summing every single item. CDS-29 has good statistical properties (Aponte-Soto et al., 2014; Fagioli et al., 2015; Migliorini et al., 2012; Sierra & Berrios, 2000; Sugiura et al., 2009), with internal reliability for different language versions reported between .89 and .94 (Cronbach’s alpha). Moreover, previous research has extracted four subscales from CDS-29 (Sierra et al., 2005): Anomalous Body Experience, Emotional Numbing, Anomalous Subjective Recall, and Alienation from Surroundings.
Three catch questions taken from Adler and colleagues (2016) were added: (1) “Are you taking antidepressants or antipsychotics?”; (2) “Are you suffering from a seizure disorder?”; (3) “Do you see colors when listening to music?” These additional questions allowed us to screen out participants under pharmacological treatment for depression and psychosis (to avoid studying dissociative episodes potentially induced by substances) and to control for anomalous sensory experiences possibly unrelated to disturbances of the self (in this case, from seizure-induced perceptual alterations or episodes of synaesthesia). Respondents who answered yes to any of these three questions were excluded regardless of their score on the CDS-29, leaving a sample of 214 participants. Other criteria for participants’ selection included (a) being between 18 and 40 years old, (b) being right-handed, and (c) not having a history of neurological illness.
To ensure that the DP scores were significantly distinct in their levels of DP experiences, we adopted two scoring thresholds, a high-group threshold (⩾50/290) and a low-group threshold (⩽20/290), previously employed by Kanayama et al. (2009), in turn based on a validated clinical cutoff for a DPD diagnosis. The high-group threshold is set relatively close to the score of 70 which previous studies have demonstrated to yield high sensitivity and specificity in differentiating DP patients from other conditions (Sierra et al., 2005). Previous studies adopting these cutoffs reported differences in neurophysiological activity (Kanayama et al. 2009) and behavioural measurements (Farmer et al., 2021) in tasks measuring self-perception in people without diagnosis of DP.
Out of our 214 eligible participants, 64 (~29%) resulted in the low group, 63 (~29%) resulted in the high group, and 87 (~40%) scored between the two thresholds. A t-test performed on the CDS scores from our two groups of interest (Low Group: M = 11, SD = 5.7; High Group: M = 77, SD = 26.2) showed that scores from the two groups were significantly distinct (p < .001), confirming that participants were successfully assigned to the two groups.
Following pre-screening, recruitment of participants proceeded on a voluntary basis, ultimately bringing 70 participants (23 males, M = 23.87 years, SE = 2.85) to take part in the study for the two groups: (1) 35 in the High DP experiences group (High DPe; 6 males and 29 females; M = 23.51 years, SE = 4.07) with their score ⩾ 50 on CDS-29 (M = 82.8; SD = 30.34; range = 50–185); and (2) 35 participants in the Low DP experiences group (Low DPe; 17 males and 18 females; M = 24.23 years, SE = 3.98) with their score ⩽ 20 on the CDS-29 (M = 12; SD = 6.10; range = 0–20). A matching procedure between participant pairs was not systematically conducted. Our two groups were adequately balanced concerning age, t(68) = −0.741; p = .461, and all participants were born and raised in Italy where they attended Italian school. We have subsequently post hoc controlled for their educational background (refer to section “Questionnaires”), demonstrating homogeneity among the groups, t(68) = 0.743; p = .459; mean education High DPe = 13.71, SE = 1.77; mean education Low DPe = 13.43, SE = 1.42. Furthermore, as mentioned above, the two groups differ in terms of the variable of gender. Indeed, while the Low DPe group is balanced for gender, the High DPe group is unbalanced due to the presence of more women than men. However, this finding is consistent with previous studies that have reported a higher incidence of women among people with high levels of DP experiences in the general population (Aderibigbe et al., 2001; Ciaunica, Mathew, et al., 2021; Yang et al., 2023) (see “Limitations and outlook” section).
The majority of High DPe participants were clustered in a range between 50 and 100 of the CDS score, with 17 participants (48.75%) within the 50–75 score range and 11 participants (31.42%) within the 75–100 score range. Five participants (14.28%) scored within the 100–125 range, while three participants (8.57%) scored within the 125–150 range. Only one participant (2.85%) showed a score above 150, resulting in an outlier within the High DPe group. Analysis on participants’ performances on tasks revealed no relevant outlier value as measured with Cook’s distance test. Thus, all participants were used in the analyses.
All participants signed informed consent forms and were fully debriefed after the study. The study was approved by the Research Ethics Board (REB) of the University of Parma under the reference number 0009104 and was carried out in accordance with the Declaration of Helsinki (1964 and subsequent amendments).
Design and experimental procedure
The study followed a mixed design. The participants’ Group, Low DPe and High DPe, was taken as between-subject factor. Each participant executed all the tasks according to a within-subject, repeated-measure design. The study consisted of two sessions: (1) the PPS task and (2) the MTT task, all carried out on the same day, with balanced order across participants (see Figure 1). Within-subject factors for the PPS and MTT tasks were modelled and analysed separately according to the dependent variable of interests of the two tasks (see sections “The PPS task” and “The MTT task”). Following these two sessions, participants completed two questionnaires: (1) the “Biographical and General knowledge questionnaire” and (2) the “Self, Space, and Time perception questionnaire” (see below).
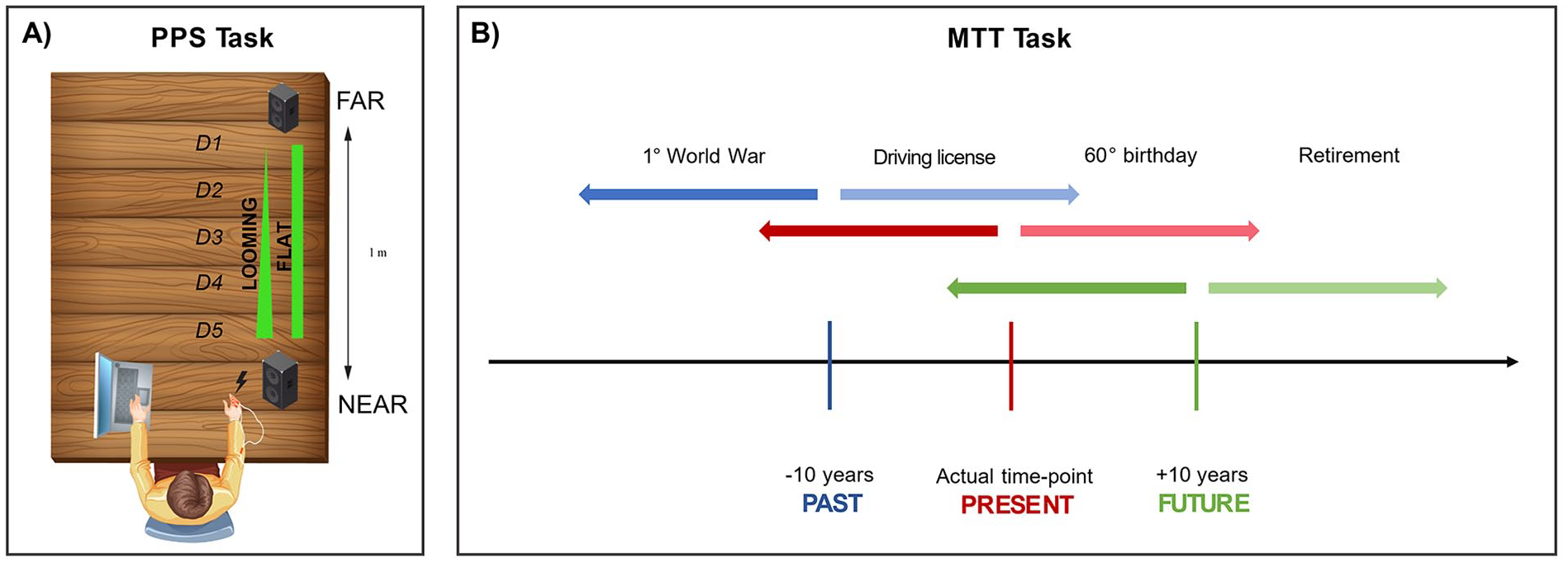
(a) The experimental setting of PPS (peripersonal space) task. The green shapes represent the two adopted sounds (rectangular shape = flat sound; triangular shape = looming sound). (b) The experimental stimuli and procedure of the MTT (mental travel task) task. Participants were required to project themselves in three different self-locations in time (past, present, or future) and determine whether the event being presented was in the past or the future relative to the current self-location.
The PPS task
Participants’ PPS perception was measured using an adapted version of the well-established PPS task procedure (Canzoneri et al., 2012; Ferroni, Ardizzi, et al., 2022; Ferroni et al., 2020; Ferroni, Gallese, et al., 2022). Participants were blindfolded and comfortably seated at a table with the palm of their right hand resting on it (Figure 1a). Participants were asked to respond as fast as possible with their left index finger on a keyboard (see Figure 1a) to a tactile target while an external auditory stimulus was presented either as a static (flat) sound or as a dynamic (looming) sound. The tactile stimulus consisted in a single, constant voltage, rectangular monophasic pulse delivered by means of electrical stimulators (DS3; Digitimer) via pairs of neurological electrodes placed on the hairy surface of the participant’s right index finger (see Supplementary materials for further details). The auditory stimuli were samples of pink noise (or 1/f noise) of 3,000 ms duration with flat or increasing (looming) intensity levels. The sounds were sampled at 44.1 kHz. Sound intensity was digitally manipulated so that “looming sounds” had exponentially rising acoustic intensity from 55 to 70 dB, whereas “flat sounds” had constant 62.5 dB acoustic intensity. Auditory stimuli were presented by two loudspeakers, one placed near (~10 cm) the participant’s right hand and one placed far from the participant (1 m from participant’s body). The looming sounds were emitted by both near and far loudspeakers, arranged so that the far loudspeaker activated at the maximum intensity and its intensity decreased up to silence along the trial, whereas the near loudspeaker activated at the minimum intensity and its intensity increased up to the maximum value along the trial. In this way, the looming sounds gave the impression of a sound approaching towards the participant’s body. Participants were instructed to focus on the tactile targets and to ignore the auditory stimulus. In 60% of the trials, participants were presented with both an auditory and a tactile stimulus. The tactile stimulus was delivered at varying temporal delays from the onset of the auditory stimulus. Five different temporal delays that resulted in five distances from participants’ body were used: 300 ms (D1); 800 ms (D2); 1,500 ms (D3); 2,200 ms (D4); and 2,700 ms (D5). The remaining trials (40% of total) were catch trials with auditory stimulation only (either looming or flat sounds), or unimodal tactile trials (with only vibration). Unimodal tactile stimuli served as baseline trials. In these trials, the tactile stimulation was delivered during silence periods, preceding sounds administration, namely at −700 ms (D0). These baseline trials were used to control for a potential confounding effect due to expectancy. Each trial was repeated if participants failed to answer to the tactile target.
The rationale behind this task refers to the PPS mapping itself, which is allowed through the integration of somatosensory information related to body part and visual or auditory information related to objects presented in the portion of space surrounding the same body part (for a review, see Macaluso & Maravita, 2010). Thus, the audio-tactile interaction task used here includes a bimodal stimulation (tactile and auditory stimulations), as it has been shown that stimuli from different sensory modalities interact more effectively when presented within the same portion of space (Stein & Meredith, 1993). The distance between the auditory stimulus and the participants’ body at which this multisensory effect occurs (e.g., tactile stimulation on the hand) is taken as a proxy of PPS representation.
The MTT task
Participants sat in front of a 15-inch colour monitor, at about 60 cm. They were instructed to visually attend slide presentations reporting brief descriptions of BIOGRAPHICAL (e.g., bachelor’s degree, the first day of school) or GENERAL events (e.g., Trump’s election; the first man on the moon, etc.) (Figure 1b). All slides were presented on the computer screen (for a complete list of stimuli, see Supplementary Table 1). Different events were administered in three separate slide presentations corresponding to the three task conditions, one for each possible position in time: (1) PRESENT (current time) condition; (2) PAST (10 years in the past) condition; and (3) FUTURE (10 years in the future) condition. The order of conditions was balanced among participants. The time condition was indicated before each presentation, and participants were requested to thoroughly imagine themselves at the corresponding moment in time. Participants first performed a brief practice session, with eight stimuli randomly presented. Once familiarised with the task and ready to proceed, participants were invited to run the presentation with each slide presenting one event of either a GENERAL or BIOGRAPHICAL kind, as described above. They were instructed to indicate, as fast as possible, if the currently displayed event had already happened or had yet to happen relative to the moment in time, they were imagining themselves to be in. Thus, for each condition, some of the presented events happened in the past relative to the time condition considered, while others happened in the relative future. Given that responses pertaining to biographical events were contingent upon participants’ personal experiences and broader social contexts (e.g., employment, education, family), participants were explicitly instructed to identify as “events yet to happen” any biographical events they had not personally encountered. Such events were regarded as prospective, potential occurrences. Consequently, events like earning a bachelor’s degree or attending a child’s graduation could be classified as forthcoming events for individuals not presently enrolled in a university or without children.
Each time condition consisted of 24 trials, adding up to 72 trials overall. Twenty-four stimuli were used for each condition, half BIOGRAPHICAL (12 trials per time condition) and half GENERAL (12 trials per time condition). Furthermore, GENERAL and BIOGRAPHICAL trials within time conditions were equally distributed between (1) relative past and (2) relative future events, making up six trials of either BIOGRAPHICAL or GENERAL kinds for each relative time condition. Although this design was applied to every participant, it is important to note that the distribution of relative future and past events could vary slightly depending on each participant’s specific age and knowledge of general events. For instance, in the PRESENT condition, the 30th birthday is considered a future event for an 18-year-old but a past event for someone aged 40. Similarly, in the FUTURE condition (10 years in the future), while the 50th birthday remains a future event for an 18-year-old, it no longer holds the same status for a 40-year-old, now imagining herself as being 50 years old. Regarding GENERAL events, potential temporal misplacement of events (due to ignorance or incorrect knowledge of the event’s year) or subjective interpretations (e.g., “Brexit” could refer to the referendum vote in 2016 or the entry into force of the withdrawal agreement in 2020) could also influence the specific relative condition. Therefore, after the experiment, participants completed a “Biographical and General knowledge questionnaire” (see next section), enabling us to assess the consistency in the distribution of events (see Supplementary Materials, Section 3).
Each event appeared at the centre of the computer screen and remained visible until a response was given, with an interstimulus interval of 1,000 ms. Judgements were given using the index finger of the left or right hand if the event was past or future, respectively (counterbalanced). MATLAB (The MathWorks, version 2019b) software and the Psychophysics Toolbox Version 3 (PTB-3) interface were used for stimulus presentation and response collection. After the task, the “Biographical and General knowledge questionnaire” was administered to participants to determine correct responses in accordance with their temporal knowledge of the events presented (i.e., they were requested to indicate the year of happening of both biographical and general events). Accurate comprehension of the sentences used in the MTT task was monitored during the completion of the questionnaires at the study’s completion (see section “Questionnaires”).
The different conditions were used to analyse two processes: (1) SELF-REFERENCING skill, i.e., the general capacity of using one’s own position in time to estimate/situate events in time and (2) SELF-PROJECTING skill, i.e., the ability to mentally move back and forward in time, maintaining the competence of correctly situating events in time. For assessing SELF-REFERENCING, only the Present condition (i.e., imagining oneself in the present) was included in the analysis. This allowed us to use the Present condition as a baseline to evaluate the performance in SELF-PROJECTING, for which instead only the Future and Past conditions were used (see “Data analysis and results” section).
Questionnaires
“Biographical and general knowledge questionnaire.”
In this questionnaire, participants were requested to indicate the year of occurrence of each event previously presented to them in the MTT Task. Answers in this questionnaire were thus used to determine correct responses according to each participant’s anamnestic data (i.e., regarding autobiographical events) and personal knowledge. For questions regarding personal knowledge, participants were asked to report the precise year of happening of the general events presented in the task. As previously discussed, asking for personal knowledge about general events allowed us to correctly interpret participants’ responses according to their knowledge and personal perspectives about the events.
The “self, space, and time perception questionnaire.”
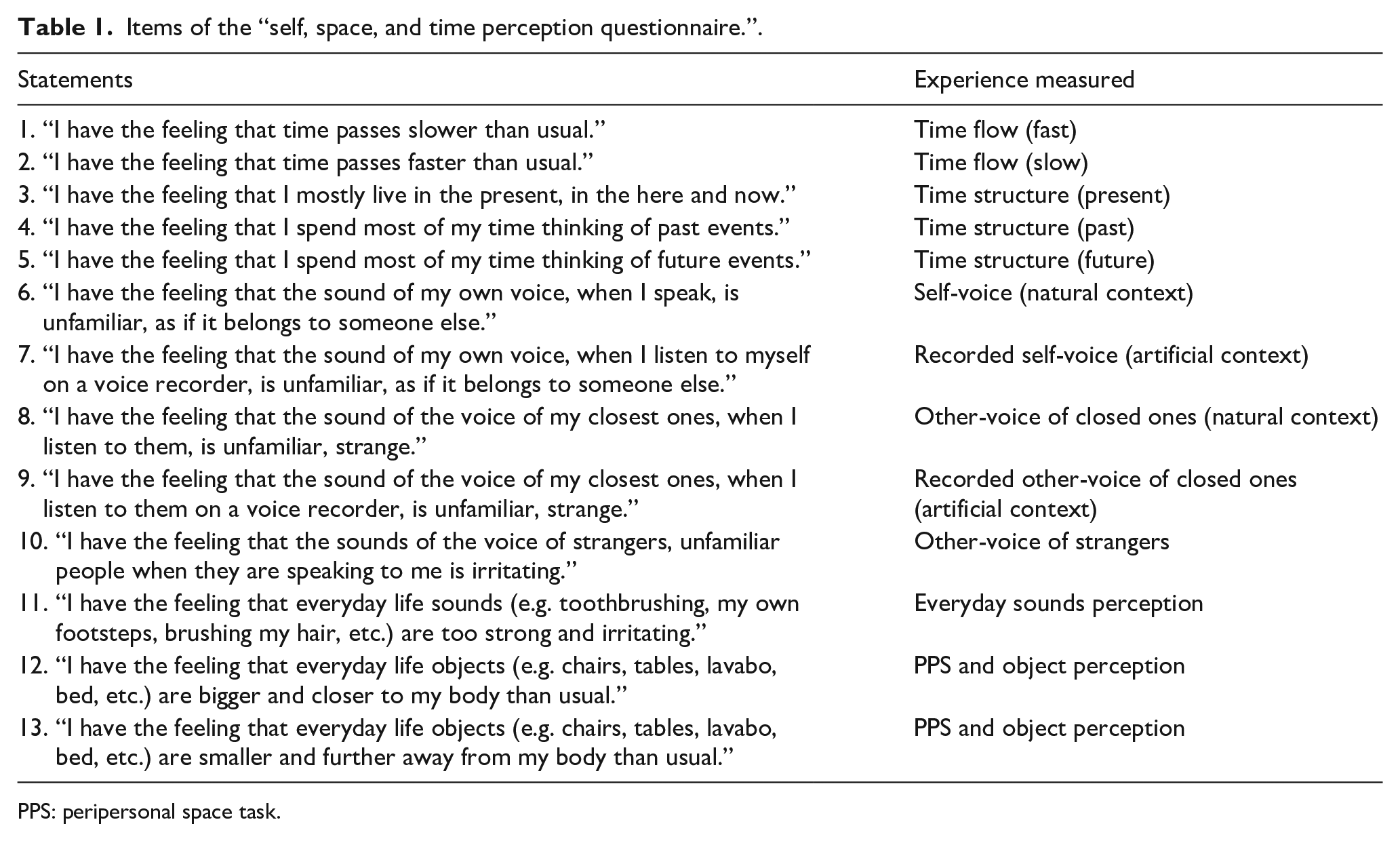
We designed a new questionnaire aimed at measuring specific facets of time and space perception to further assess participants’ relationship to DP experiences. The present questionnaire represents an exploratory tool, considering that it has not yet been statistically validated; it is nonetheless a tentative analysis of multiple phenomena related to self-perception in DP presently lacking a quantitative evaluation. It is well known that humans are embodied living biological organisms that are born, grow, decay, and ultimately die. Hence, how time is perceived in relation to one’s body and the objects perceived close to one’s body is a key aspect of human daily experiences. We have structured the new questionnaire to analyse self and body in time via two facets: (1) structure (past/present/ future) and (2) flow (fast/slow); and self and body in space via one facet, i.e., how close, or far objects are perceived to be to the body. Specifically, 13 statements (see Table 1) were crafted and presented to participants, who were asked to indicate on a scale from 1 (“Not at all”) to 5 (“Strong Yes”) whether each corresponded to their personal experiences within the past 6 months from the date of experiment. The questionnaire was organised as follows: (a) Questions from 1 to 5 measured the perception of time; (b) Questions from 6 to 11 measured the perception of Self-Voice versus Other-Voice; and (c) Questions 12 and 13 measured the perception of PPS. Scores were used to run correlational analyses with participants’ scores on the CDS and performances on tasks. The aim of this questionnaire was thus to further assess the relationship between our research questions and the symptomatic profile of DPD, albeit at an exploratory level being a newly designed method.
Items of the “self, space, and time perception questionnaire.”.
PPS: peripersonal space task.
Data analysis and results
Peripersonal space and slopes estimation results
To estimate the individual boundary of PPS, PSE (point of subjective equality) of the psychometric function describing audio-tactile RT as a function of audio-tactile distance was measured via the Spearman–Karber (SK) method (Bausenhart et al., 2018; Miller & Ulrich, 2001) in line with recent studies on PPS (Ferroni, Ardizzi, et al., 2022; Ferroni, Gallese, et al., 2022; Masson et al., 2021; Noel et al., 2021). This allowed us to estimate these parameters without any specific assumptions about the functional family of the underlying psychometric functions. Specifically, the 10% trimmed means of participants’ RTs obtained in response to the tactile stimulus administered at the five distances (D1, D2, D3, D4, D5) were used to estimate the PSE. PSE was estimated as a measure of location, and difference limen (DL) as a measure of steepness, of the psychometric function underlying the data (e.g., Miller & Ulrich, 2001).
PSE values were entered into a two-sample t-test with Group (High DPe, Low DPe) as between-subjects factor. Results revealed the absence of a significant difference between the two groups, Low DPe: M = 1,421.56, SE = 281.70; High DPe: M = 1,453.09, SE = 309.28; t(68) = −0.44, p = .66. The slope’s values (DL values) were entered into a two-sample t-test with Group (High DPe, Low DPe) as between-subjects factor. Results revealed the absence of a significant difference between the two groups, Low DPe: M = 691.52, SE = 150.47; High DPe: M = 684.36, SE = 149.03; t(68) = 0.2, p = .84. Our results indicate the absence of significant differences between the High versus Low DPe groups, suggesting that people with higher occurrences of DP experiences have a similar representation of the extension and sharpness of PPS than those with low occurrences of DP experiences.
MTT results
Error rates (ERs) and RTs were collected during the task. Importantly, participants were instructed to answer as fast as they could and that resulted in a trade-off between the two parameters. For this reason, a speed-accuracy trade-off was expected. To deal with this aspect and to have a more precise measure of participants’ performance, ERs and RTs were used to compute Inverse Efficiency Scores (IESs, Townsend & Ashby, 1983). The IES is a weighted index of RT which is calculated as a ratio between mean RT value and the accuracy of response (i.e., % of correct responses) on a certain condition. For example, higher ERs penalise the corresponding RT by increasing their value (i.e. the higher the IES, the poorer the performance on that condition). To assess SELF-REFERENCING and SELF-PROJECTING participants’ scores, the obtained IESs were then submitted to two analyses of variance (ANOVAs). Only correct responses were considered for analysis.
First, for SELF-REFERENCING condition, data were entered into a 2 × 2 × 2 mixed design repeated-measures ANOVA with Group (Low DPe, High DPe) as between-subjects factor and Type of Event (General, Biographical), Relative Time of Event (i.e., Future Relative vs Past Relative to the moment in time the participants were imagining themselves in) as within-subjects factor. The analyses on the IESs revealed a significant main effect of the factor Group (Figure 2a), with the High DPe group showing an overall poorer performance in locating events in time relative to their present situation, Low DPe: M = 1,389.29, SE = 75.36; High DPe: M = 1,632.58, SE = 75.36; F(1,68)= 5.21; p = .025; η2p = .071. Moreover, a significant interaction between the Relative Time of Event and Group was found (Figure 2c), with the Low DPe group performing better in answering to past events. Notably, this facilitation was absent in the High DPe group which performed similarly regardless of relative time, Low DPe: M = 1,253.21, SE = 76; High DPe: M = 1,597.33, SE = 76; F(1,68) = 6.98; p = .01; η2p = .09. No other interaction with the factor Group showed significant results (all ps > .67).
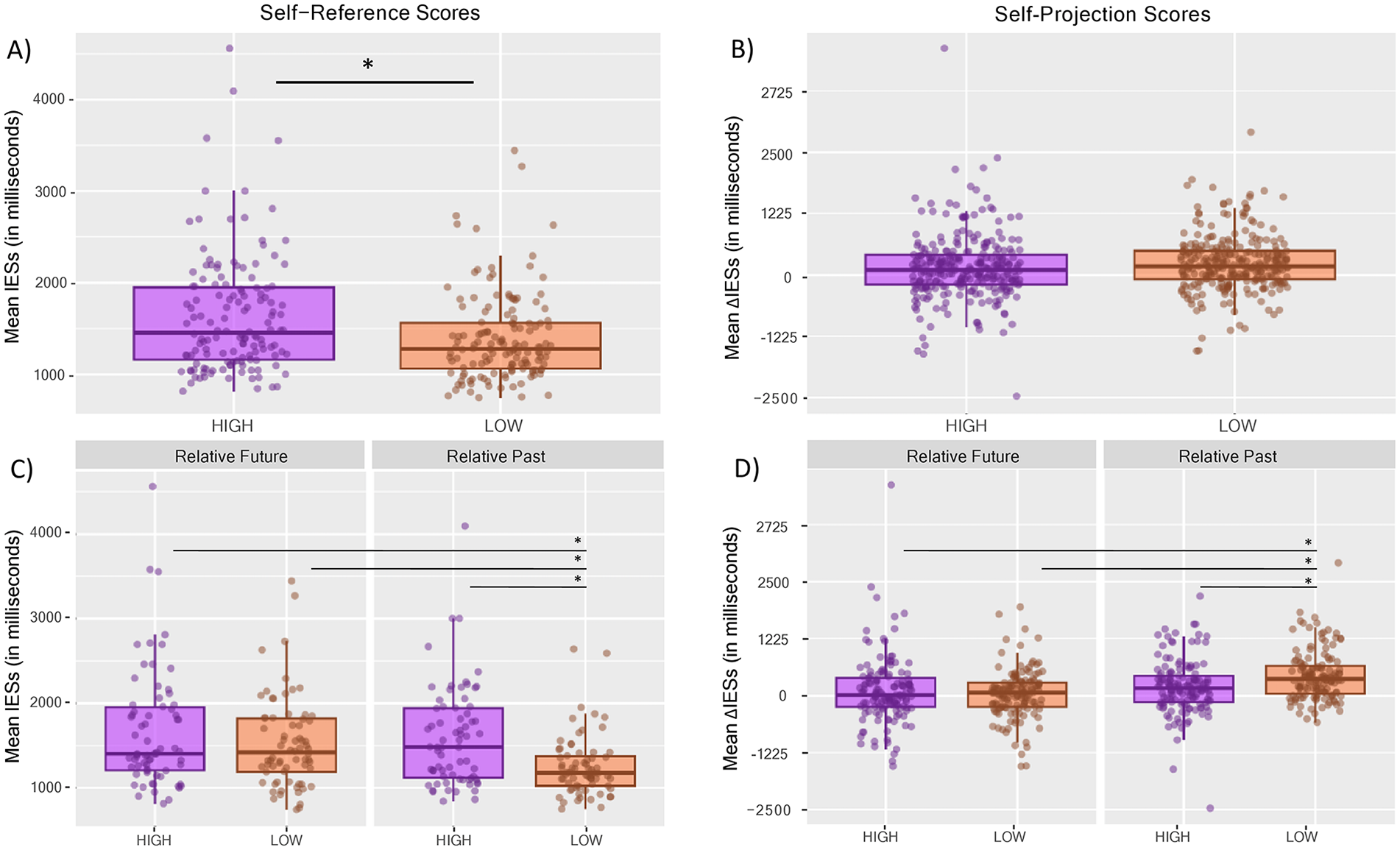
Distribution of IES in the Mental Travel Task for the High DPe Group (purple) and the Low DPe Group (orange). “*” indicates significant differences (p < .05). (a) Group difference in executing the Self-Reference Task. (b) Group difference in executing the Self-Projection Task. (c) Group difference in answering to events in the relative past versus the relative future in the Self-Reference condition. (d) Group difference in answering to events in the relative past versus the relative future in the Self-Projection condition. IES: Inverse Efficiency Scores; HIGH: people with high depersonalisation experiences; LOW: people with low depersonalisation experiences.
Regarding the SELF-PROJECTION condition, data obtained were preprocessed by subtracting participants’ values recorded in the Present condition (i.e., IESs scores in SELF-REFERENCE) from the other two time conditions, namely the PAST condition and FUTURE condition. Thus, values recorded in the Future and Past conditions were transformed into Δ values (i.e., ΔIES). The rationale of this process was to isolate the specific effects exerted by “moving” on the temporal timeline in the past or in the future on participants’ performance, removing the baseline skill of locating events in time. A positive Δ value thus indexes that the related time condition hinders participants’ performance, while a negative one indexes advantage. Δ values were entered into a 2 × 2 × 2 × 2 mixed design repeated-measures ANOVA with Group (Low DPe, High DPe) as between-subjects factor and Type of Event (General, Biographical), Relative Time of Event (i.e., Future Relative vs Past Relative to the moment in time the participants were imagining themselves in), and Time (Future, Past) as within-subjects factors.
By contrast with the SELF-REFERENCING condition, the main effect of Group on the task disappeared in the SELF-PROJECTION condition (Figure 2b). No significant differences in performance between the two groups due to projecting into different time conditions (p = .25) were found. Again, a significant interaction was found between Relative Time of Event and Group, F(1,68) = 8.97; p = .003; η2p = .12 (Figure 2d), this time showing that the Low DPe Group is more penalised than the High DPe Group in answering to past events when moving through time conditions (Low DPe: M = 432.89, SE = 62.42; High DPe: M = 197.12, SE = 61.52; p = .04).
Correlational analysis between questionnaires scores and mental travel and peripersonal space tasks—results
Pearson’s correlation analyses were performed on mean scores from performances on both tasks and on scores from all the questionnaires submitted to participants to determine potential correlations between:
Participants’ performance on the PPS and MTT tasks for each measured parameter (i.e., size and sharpness from the PPS task; IESs for SELF-REFERENCING and SELF-PROJECTING abilities from the MTT task).
Participants’ performance on both tasks and scores on the CDS main score and subscales.
Specific elements of the Self, Space and Time Perception questionnaire (SSTq) and participants’ scores in the two tasks, again for each measured parameter.
Finally, we evaluated whether elements from the SSTq held a significant relation with scores on the CDS main scores and subscales.
Our results indicate (see Table 2):
No significant correlation between participants’ performances in the MTT and PPS tasks.
Results of correlational analyses performed between all questionnaires scores and all measured parameters on the PPS and MTT tasks.
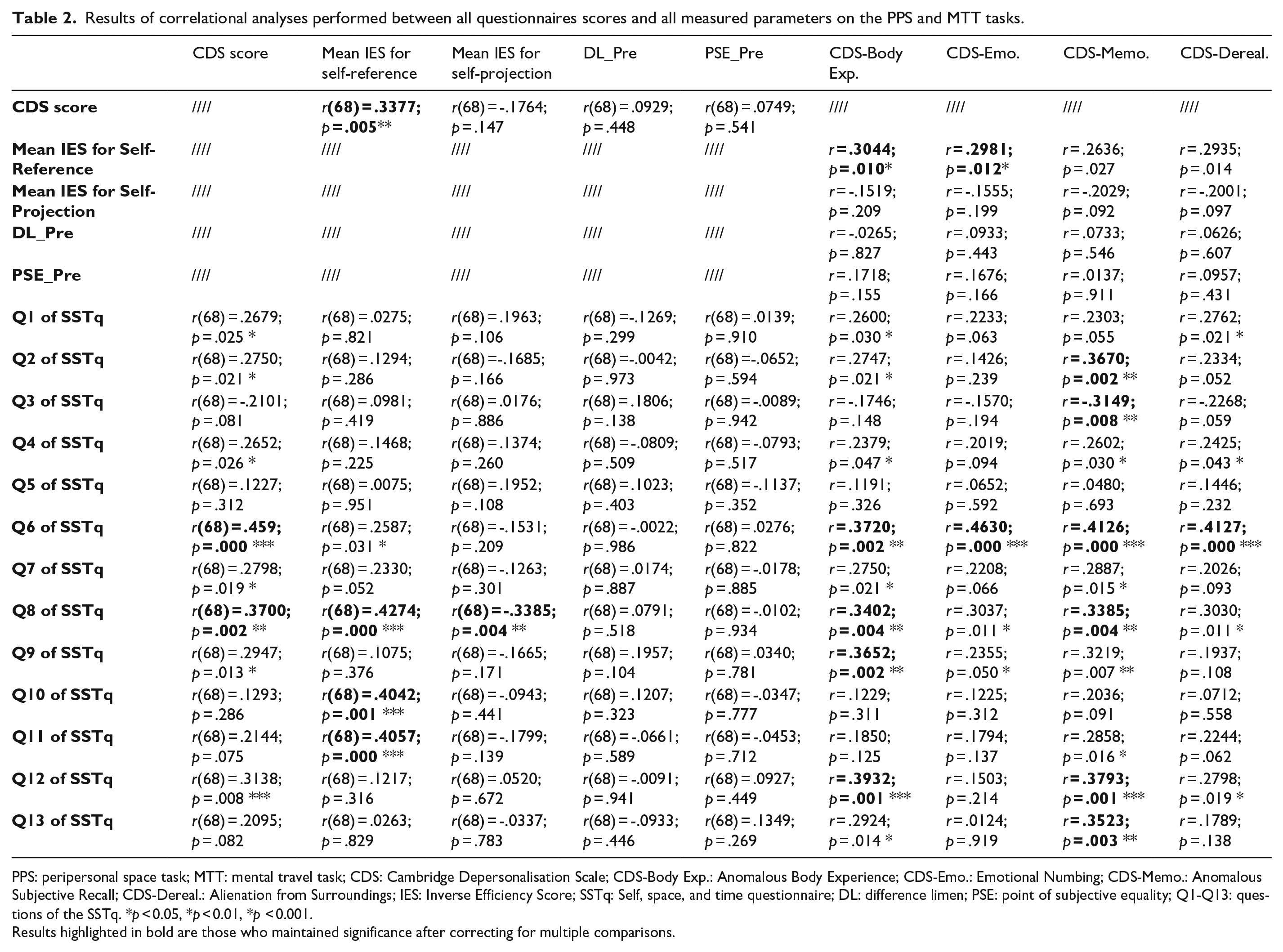
PPS: peripersonal space task; MTT: mental travel task; CDS: Cambridge Depersonalisation Scale; CDS-Body Exp.: Anomalous Body Experience; CDS-Emo.: Emotional Numbing; CDS-Memo.: Anomalous Subjective Recall; CDS-Dereal.: Alienation from Surroundings; IES: Inverse Efficiency Score; SSTq: Self, space, and time questionnaire; DL: difference limen; PSE: point of subjective equality; Q1-Q13: questions of the SSTq. *p < 0.05, *p < 0.01, *p < 0.001.
Results highlighted in bold are those who maintained significance after correcting for multiple comparisons.
Discussion
This study examined the relationship between PPS, time perception, and depersonalisation (DP) experiences in the healthy population (Sierra & Berrios, 1997). Our study yields several significant results regarding egocentric spatial processing in self-related disorders and points to the crucial role of time misperception in dissociative experiences.
First, and strikingly, we found no difference in PPS perception in healthy people with High versus Low DP experiences. Based on previous findings, reporting a narrow PPS extent in schizophrenia patients and high schizotypal individuals (Di Cosmo et al., 2018; Ferroni, Ardizzi, et al., 2022), and considering the similarities between these two clinical and subclinical disorders, we hypothesised that people with higher occurrences of DP experiences would show an altered PPS representation.
Indeed, previous studies (Ciaunica et al., 2023; Sass et al., 2013; Værnes et al., 2018) noted a substantial overlap in the anomalous self-experience lived by schizophrenic patients and people with high levels of depersonalisation experiences. However, these clinical and subclinical conditions remain distinct, and these discrepancies can account for our results. For example, Vaernes and colleagues (2018) found that early disturbances in self-experience and sociality with no obvious triggers, as well as the presence of delusion-like ideas of control and external influence, were present in a patient with schizotypal personality disorder but not in depersonalisation disorder.
Furthermore, people experiencing psychosis and schizophrenia often describe profound confusion between reality and fantasy or imagination and may come to doubt many aspects of existence that most people take for granted (Sass et al., 2013). By contrast, numerous subjective reports and empirical studies illustrate that people experiencing DP episodes are very much aware that their perceptual alterations are subjective phenomena and do not reflect reality itself (Guralnik et al., 2000; Sierra, 2009; Simeon & Abugel, 2006; see Yang et al., 2023, for a recent discussion). Considering this difference in intact versus altered reality testing, it has been suggested that self-disturbances in schizophrenia may depend on some unique additional processes (such as diminished self-presence) which allow them to be distinguished from those in depersonalisation experiences (Hunter et al., 2014; Sass et al., 2013; Sierra & David, 2011).
In this regard, the results from our PPS measurements might hint at potential differences in multisensory integration of bodily stimuli in relation to action in people with high occurrences of DP experiences versus schizophrenia spectrum. Previous works outlined the crucial role that processes related to motor control play in regulating multisensory integration around bodily effectors (Bufacchi & Iannetti, 2018; Ferroni & Gallese, 2022). Indeed, the importance of the ability to control one’s actions in grounding our sense of self as agent has been extensively illustrated in typical populations (Gallese & Sinigaglia, 2010; Haggard, 2017). However, here we speculate that a careful comparison between motor processes (Fogassi et al., 1992, 1996) in DP versus psychosis may reveal important differences, as demonstrated by previous studies on schizophrenia patients (see Ardizzi et al., 2020). Thus, although there is substantial symptom overlap between depersonalisation in clinical depersonalisation/derealisation disorder (DPDR) and schizophrenia (see Sass et al., 2018), there might be bodily and self-related mechanisms/processes specifically altered in psychosis which are unaffected in DPDR, and vice versa.
The examination of time perception in relation to DP has revealed differences in the way people with High versus Low occurrences of DP experiences process past events. Specifically, the Low DPe Group performed better when answering to past event as opposed to future events, possibly indicating that in typical conditions memory recall of events that have already happened results in faster responses than the processing of hypothetical or counterfactual future events yet to happen.
Crucially, this performance was negatively affected by moving through time conditions, a process which shifted participants’ temporal frame of reference, making it more difficult to quickly locate events that had already happened. In contrast, the same modulation was not found for the High DPe group, which performed similarly with both kinds of events (i.e., relative future and relative past events) among tasks.
Their performance was thus not negatively affected by self-projecting through time, possibly indicating that they did not leverage memory for past events to foster faster RT as the Low DP Group did. This is consistent with subjective reports of anomalous subjective recall and feelings of detachment from one’s own memories in DP (Ciaunica & Charlton, 2018; Perkins, 2021; Sierra & David, 2011). One may speculate that the temporal “flatness” found in High DPe individuals’ performance most likely mirrors their phenomenological experience of “being stuck” in time, further highlighting a potential connection between detachment from bodily sensations and detachment from life experiences overall (Sierra, 2009; Simeon & Abugel, 2006).
Existing studies outline a strong link between body, memory, and emotions. For example, several studies showed that affective states (Apgáua & Jaeger, 2019; Auguste et al., 2023), visual feedback from one’s own body (Bréchet et al., 2020; Penaud et al., 2023), and shifts among ego and allocentric spatial perspectives (King et al., 2022) affect memory retrieval (and possibly memory formation, see Gauthier et al., 2020), resulting in changes in informational content and access to both the semantic and perceptual details of memory. Moreover, experiencing temporal blunting or stuck perception of time has been consistently linked to major depression (Thönes & Oberfeld, 2015; Vogel et al., 2018, 2019). Subjective reports of time dilation and stagnation (Stanghellini et al., 2017) together with an altered experience of the current passing of time (Kent, Van Doorn, & Klein, 2019) are common in conditions of depressive mood. While it has been suggested that some more autonoetic (i.e., reflective) features like negative self-narration (Vogel, Jording, et al., 2020) and feeling of hopelessness (Kent, van Doorn, Hohwy, & Klein, 2019) are likely to be in play, abnormal time experience in depression is also characterised by altered relation to “conative” (i.e., appetitive) processes (Stanghellini et al., 2017) and loss of general propensity for goal-directed behaviour (Vogel et al., 2018).
Given that Emotional Numbing and Anomalous Bodily Experiences are among the major traits of DP experiences (Sierra & Berrios, 1997), altered bodily perception might lead to a differential quality in memory recall processes (for proposals about possible mechanisms, see Fuchs, 2015; Palombo et al., 2018; Riva, 2018). Future studies should further assess memory recall abilities on different kinds of memories’ content and different memory systems (e.g., episodic vs semantic memory, see Fragueiro et al., 2021), or by contrasting DP with other mental health conditions known to affect memory processing such as anxiety and depression.
Indeed, previous studies reported depersonalisation symptomatology in severe cases of depression (Zikić et al., 2009). Given this relevant co-occurrence of altered self-narration and altered bodily feelings in dilated time experience, future research is needed to clarify what developmental trajectories the two aspects follow in diverse conditions presenting a common “flattening” of time experience.
Another important finding from the MTT task is that people with higher occurrences of DP experiences display an overall impairment in locating time events relative to position in time. This specific deficit in Self-Referencing is coherent with the symptomatic profile of depersonalisation where people report losing connection with their sense of self and personal stories (Sierra, 2009; Simeon & Abugel, 2006).
Participants’ scores on the Anomalous Body Experience subscale and Emotional Numbing subscale proved to be predictive of their performance on the Self-Reference Task, confirming a close relationship between time experiences and bodily and emotional experiences. Further works tackling this specific relationship may shed new light on how altered self-experiences affect the situatedness in time and space, as well as the potential relationship between the “flatness” of time perception in DP experiences and emotional “flatness” or numbing.
Our correlational analyses further highlighted a positive correlation between participants’ scores on questions of the SSTq measuring auditory perception of surroundings (questions 8, 10, and 11) and performance in self-referencing. This result fits with the idea that a chronically altered processing of environmental stimuli might affect the quality of memory recall (as previously suggested). It also aligns with the hypothesis that people with High DPe might be more detached from exogenous stimuli, resulting in a deteriorated effectiveness of self-referencing processes in locating temporal events. Indeed, a wide body of research on DP notes that individuals tend to focus on inner experiences and thoughts rather than attending and engaging with the external world, projecting into the future, or relating to the past (Hunter et al., 2003). This is also consistent with persistent feelings of existential concerns, hyper-reflexivity, or “over-thinking” in people experiencing DP (Ciaunica, Seth, et al., 2022; Hunter et al., 2003).
Interestingly, the two items of the SSTq measuring, namely self and other voice perception (i.e., questions 6 and 8), showed a positive correlation with participants’ scores on CDS, which might be a further index of altered processing of auditory stimuli, in this case, self-produced (i.e., feedbacked) and perceived speech. Indeed, voice perception is an important communication tool, allowing individuals to successfully engage with others socially. Scores on these questions measuring voice perception in natural context and performance in SELF-REFERENCING held a significant positive correlation with the Anomalous Body Experience subscale and the Memory Retrieval subscale of the CDS, confirming a link between anomalous somatic sensations, self-referencing, and time processing. Finally, a negative correlation was found between scores on the other-voice perception item (i.e., question 8) and performance in SELF-PROJECTING. Notably, the detected directions of these correlations for items measuring self and other voice perception reflect the trends that emerged from our main results in the MTT task. Specifically, people with High DPe levels showed an overall poorer performance in SELF-REFERENCING, while people with Low DPe levels showed a greater drawback in SELF-PROJECTING.
Limitations and outlook
Our study has several important limitations. First, our sample tested non-clinical experiences of depersonalisation in the general population. These experiences are transient and highly variable between individuals, hence a systematic investigation of PPS and time perception in relation to clinically diagnosed DP may present a different picture. Further work needs to test PPS and spatiotemporal integration in clinical DPDR.
Second, the gender sample is not balanced for the group with high levels of DP experiences. This could, however, be due to the inherent nature of this phenomenon as previous studies have reported a higher incidence of women among those with high-level DP experiences (Aderibigbe et al., 2001; Ciaunica, Mathew, et al., 2021, Yang et al., 2023).
Third, while ruling out people under pharmacological treatments for depression or psychosis, our pre-screening procedure did not allow us to categorically exclude recruitment of individuals with other subclinical traits or with actual diagnosis (for which we did not explicitly ask) without ongoing pharmacological treatments. Studies on the level of correlation and comorbidity with other conditions are thus necessary to corroborate our results.
Moreover, our study used an audio-tactile multisensory integration paradigm. It would be interesting and important to test PPS perception in relation to other sensory modalities, e.g., visuo-tactile. Future work could be done to examine more thoroughly the sensitivity to distinct sensory inputs (visual, auditory, tactile, olfactory, vestibular, proprioceptive), their multisensory integration, and their impact on time and space perception in people with DP experiences. Specifically, it would be key to investigate to what extent feelings of (un)realness are triggered by atypical sensorimotor integration of self- and world-related information. For example, it has been recently suggested that different senses and modes of perception (e.g., vision vs touch) may provide a different basis for self- and world-experiences (Ciaunica, Roepstorff, et al., 2021).
Finally, given that PPS task measures an implicit processing of space, our study is not informative regarding participants’ performance in the explicit evaluation of spatial relationships such as those measured by reaching distance tasks (e.g., Ambrosini & Costantini, 2013; Costantini et al., 2011).
Conclusion
Space and time perception constitute a fundamental axis of self-experiences, allowing the individual to situate themselves in the world and to keep track of their life milestones. This study examined the relationship between Depersonalisation experiences (i.e., the experience of feeling detached from one’s self and body) and PPS and time perception.
The present study found no significant differences in space perception in people with high versus low occurrences of depersonalisation experiences. This suggests that DP experiences may constitute a cluster of distinct phenomena, partially overlapping but fundamentally distinct from other self-disturbances such as those of the schizophrenic spectrum. Further work needs to address this comparison in more detail, to disentangle various facets of the link between spatiotemporal perception and self-processing in typical and atypical population.
Furthermore, high frequency of depersonalisation experiences is correlated with atypical time processing. We believe that our results, while limited by possible confounds previously highlighted, suggest that the ability to flexibly orient through time and project oneself into the future could be linked to an intact core sense of the self. Alterations of the subjective experiences of feeling unreal and disconnected from one’s self and body may lead a subject to experience the passing of time as being “flat,” with no discrimination between past, present, and future, and inability to project oneself in the future (Figure 3).

Graphical abstract.
Supplemental Material
sj-docx-1-qjp-10.1177_17470218241261645 – Supplemental material for Lost in time and space? Multisensory processing of peripersonal space and time perception in people with frequent experiences of depersonalisation
Supplemental material, sj-docx-1-qjp-10.1177_17470218241261645 for Lost in time and space? Multisensory processing of peripersonal space and time perception in people with frequent experiences of depersonalisation by Francesca Ferroni, Edoardo Arcuri, Martina Ardizzi, Nicola Chinchella, Vittorio Gallese and Anna Ciaunica in Quarterly Journal of Experimental Psychology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by #NEXTGENERATIONEU (NGEU) and funded by the Ministry of University and Research (MUR) of Italy, National Recovery and Resilience Plan (NRRP), project MNESYS (PE0000006)—A Multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022) to V.G. F.F. and M.A. were also supported by HORIZON EUROPE Research Programme (Excellent Science). A.C. was supported by a Fundaçao para a Ciencias e Tecnologia (FCT) grant PTDC/FER-FIL/4802/2020 and 2020-02773 CEECIND FCT, and a Templeton World Charity Foundation and SSNAP Duke University award n° TWCF0384. These funding agencies had no further role in the study, in the analyses, or in the decision to submit the article for publication.
Supplementary material
The supplementary material is available at qjep.sagepub.com.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.