
Abstract
Dysfunctional interoception is increasingly being recognized as a risk factor for depression and anxiety. However, results remain mixed. Emerging research suggests that particular interoceptive phenotypes may be differentially pathogenic. The current studies aimed to evaluate the degree to which self-reported interoceptive accuracy and attention predict depression and anxiety symptoms, as well as to test the interaction between accuracy and attention. Participants (study 1: N = 170, M = 20.34 years, 69% female, 64% White; study 2: N = 826, M = 38.04 years, 49% female, 58% White) self-reported interoceptive accuracy and attention using the Interoceptive Accuracy Scale and Body Perception Questionnaire, respectively. Participants also reported depression and anxiety symptoms using the Hospital Anxiety and Depression Scale. In both studies, lower interoceptive accuracy and more interoceptive attention predicted higher depression and anxiety symptoms. In neither study did accuracy interact with attention to predict depression or anxiety symptoms. These results provide evidence that self-reported interoceptive accuracy and attention are independent predictors and do not interact to predict depression and anxiety symptoms.
Introduction
Depression is a negative affective state characterized by feelings of sadness, whereas anxiety is characterized by a high degree of apprehension and somatic symptoms of tension (VandenBos, 2007). Individuals with depression and anxiety have a lower quality of life and experience impaired functioning in work, social areas, and health (Brenes, 2007). Depression and anxiety disorders also create a societal burden in that they decrease work productivity and increase healthcare costs (Bandelow & Michaelis, 2015; Donohue & Pincus, 2007; Greenberg et al., 2023; Wittchen, 2002). With rates of depression and anxiety increasing (Terlizzi & Zablotsky, 2024), it is imperative to identify and understand risk factors.
Dysfunctional interoception is increasingly being recognized as a risk factor for depression and anxiety (Paulus & Stein, 2010). Interoception is defined as the perception of the internal state (Murphy et al., 2019). It is generally agreed upon that interoception is multidimensional (Garfinkel et al., 2015; Khalsa et al., 2018; Suksasilp & Garfinkel, 2022), with accuracy and attention being two independent interoceptive domains. Interoceptive accuracy is the precision with which internal signals are detected and is commonly quantified as objective performance on heartbeat detection tasks, whereas interoceptive attention refers to the degree to which people attend to internal signals (irrespective of accuracy). Recently, emphasis has been placed on the fact that interoceptive accuracy and interoceptive attention can be measured objectively or with self-report. Importantly, whereas objective measures provide performance-based assessments of accuracy, self-reported measures of interoceptive accuracy and attention represent one’s belief about how accurate they perceive or how often they attend to bodily signals, respectively (Murphy et al., 2019).
Despite the increasing recognition of a link between interoception and depression and anxiety, results describing these relationships remain inconsistent. Several small-scale studies (Dunn et al., 2007; Jenkinson et al., 2024) and a systematic review (Eggart et al., 2019) have indicated impaired interoceptive accuracy in those with depression. However, other studies (Blickle et al., 2024) as well as a formal meta-analysis have, in contrast, reported no relationship between objectively assessed interoceptive accuracy and depression (Desmedt et al., 2022). Compared to accuracy, fewer studies have examined the relationship between depression and interoceptive attention. Of these, some studies have indicated that higher levels of depression were associated with a lower self-reported ability to attend to interoceptive signals (Eggart & Valdés-Stauber, 2021; Dunne et al., 2021; Harshaw, 2015). Like depression, the relationship between anxiety and accuracy is also unclear. A positive correlation between anxiety and objectively-measured interoceptive accuracy has been reported, indicating that those with more severe anxiety are better at accurately perceiving their heartbeat (Pollatos et al., 2009). Multiple meta-analyses and reviews have found that there is no evidence of any positive, negative, or moderated relationship between cardiac objective interoceptive accuracy and anxiety (Adams et al., 2022; Desmedt et al., 2022; Jenkinson et al., 2024). A separate meta-analysis focusing on interoceptive attention and anxiety reported a positive relationship such that higher anxiety was associated with greater attention to negative body signals (Clemente et al., 2024).
The current set of studies aimed to address the uncertainty surrounding the relationship between interoception and depression and anxiety. Oftentimes, interoceptive accuracy and attention are examined in isolation and are rarely analyzed together. So, it remains unknown if these separate interoceptive domains are independent predictors of mental health or interact to predict mental health (Brand et al., 2022; Gabriele et al., 2022). It is possible that an interaction exists between the two dimensions that could account for mixed results in the literature. For example, the positive relationship between health-related anxiety and interoceptive attention was found to be significantly stronger in individuals with low self-reported interoceptive accuracy (Trevisan et al., 2023). In another study, interoceptive accuracy, measured using the gastric loading task, was positively correlated with well-being in individuals exhibiting low interoceptive attention (Ferentzi et al., 2019). Therefore, the current studies aimed to test, in two independent cohorts, (a) the degree to which self-reported interoceptive accuracy and attention are indeed separate interoceptive domains, (b) the degree to which self-reported interoceptive accuracy and attention predict depression and anxiety symptoms individually, and (c) whether self-reported interoceptive accuracy and attention interact to predict depression and anxiety symptoms. It was hypothesized that accuracy and attention would not be significantly related to each other because they are independent domains of interoception. Also, it was hypothesized that both accuracy and attention would each be independent predictors of depression and anxiety symptoms, and that an interaction between the two interoceptive domains would be observed and uniquely predict variance in depression and anxiety symptoms. With successful interoception interventions emerging (Davies et al., 2019; Meuret & Ritz, 2010; Meuret et al., 2009; Quadt et al., 2021), understanding how each interoceptive dimension relates to depression and anxiety is crucial to effectively leveraging interoception to improve mental health.
Methods
Study 1
Participants and Power Analysis
Data were sourced from two cohorts tested under nearly identical conditions in the same laboratory. Participants (n = 202, female: n = 133) were at least 18 years of age at the time of testing and were recruited from the university community. For both studies, recruitment included flyers posted throughout university common areas as well as advertisements disbursed through university-wide email listservs. Participants comprised mostly undergraduate and graduate students. Participants were monetarily compensated for their participation. Participants were excluded due to missingness on the Body Perception Questionnaire (BPQ; n = 12), Hospital Anxiety and Depression Scale (HADS; n = 5), and Interoceptive Accuracy Scale (IAS; n = 15), leaving an analytical sample of (n = 170). Sample characteristics can be found in Table 1. Post hoc power analysis found that adequate power (⩾.80) was achieved to detect an effect size of f2 = 0.046 (or larger). Both studies were approved by the appropriate University Institutional Review Board, and all participants provided informed consent. Writing of this manuscript was guided by the STROBE cross-sectional checklist (von Elm et al., 2007).
Sample Characteristics.
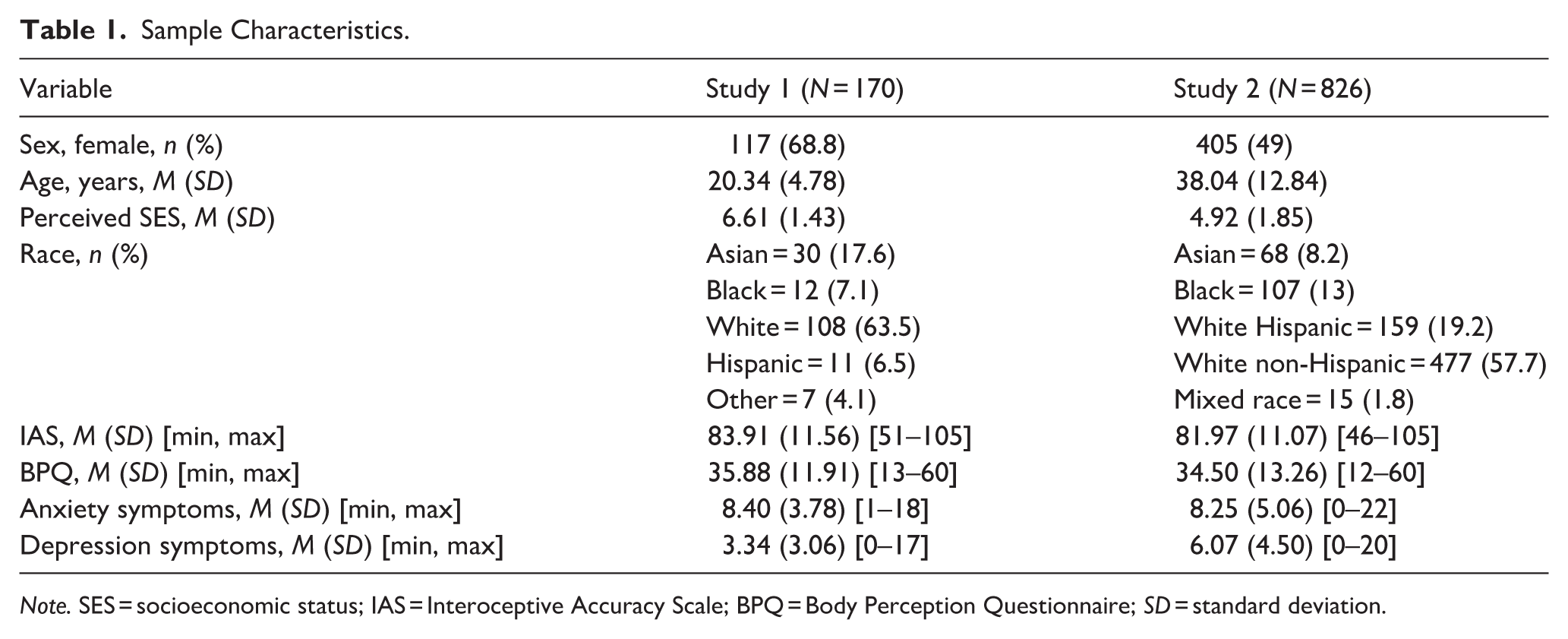
Note. SES = socioeconomic status; IAS = Interoceptive Accuracy Scale; BPQ = Body Perception Questionnaire; SD = standard deviation.
Questionnaires
Interoceptive Accuracy Scale
The IAS (Murphy et al., 2020) contains 21 self-reported items that measure beliefs regarding interoceptive accuracy. Questions ask about the degree to which participants believe they can accurately perceive various bodily functions (e.g., temperature, arousal, hunger). Participants respond on a 5-point scale, with 1 being “disagree strongly” to 5 being “strongly agree,” and final scores on the questionnaire range from 21 to 105. Higher scores indicate greater confidence in interoceptive accuracy. Previous studies show that the IAS is reliable (Murphy et al., 2020; Cronbach’s α = .88). The Cronbach’s alpha for the current study was excellent (α = .90).
Body Perception Questionnaire
The BPQ–very short form (BPQ-VSF; Porges, 1993) contains 12 questions that measure bodily awareness as an indicator of interoceptive attention. The questions include specific information about somatic symptoms (e.g., stomach pains and bloating), and participants’ responses indicate the degree to which they pay attention to these symptoms. Items are rated on a scale from 0 (“never”) to 5 (“always”), with higher scores indicating greater attention. The BPQ was chosen in the present study due to its wide use in interoceptive research (Garfinkel et al., 2015, 2016; Murphy et al., 2019, 2020; Palser et al., 2018), which aids in comparing results across studies. It also generalizes across interoceptive domains. However, some evidence does exist to show that a fraction of participants tends to interpret attention as accuracy, leading to small-magnitude spurious relationships between the BPQ and measures of interoceptive accuracy (Gabriele et al., 2022). The BPQ-VSF is found to be internally consistent (all categorical omegas >.83), strongly correlates with the 45-item BPQ (r = .94), and demonstrates excellent test–retest reliability (intraclass correlation coefficient = .97; Cabrera et al., 2018). The Cronbach’s alpha for the current study was excellent (α = .92).
Hospital Anxiety and Depression Scale
The HADS (Zigmond & Snaith, 1983) consists of 14 items—7 for depression and 7 for anxiety—that assess symptoms of depression and anxiety. Individual item scores range from 0 to 3, with higher scores indicating greater prevalence of symptoms. Across multiple studies, the HADS has been validated in both clinical and epidemiological samples (Johnston et al., 2000; Spinhoven et al., 1997). Importantly, the HADS has very few questions related to physical sensations, which might confound a potential relationship with interoception. Previously, it has been found that removing the sensation-related items from the Toronto Alexithymia Scale decreased the magnitude of its relationship with interoception measures (Ottley-Porter et al., 2025). The Cronbach’s alpha values for the current study were both acceptable for the anxiety (α = .79; HADS-A) and depression subscales (α = .78; HADS-D).
Procedure
In both studies, participants were asked to refrain from consuming caffeine for at least 2 hr and from exercising for 4 hr prior to testing. Upon arrival, participants provided informed consent, had physiological equipment fitted, and underwent an adaptation period. During the adaptation period, participants completed a battery of questionnaires, including the
HADS, IAS, BPQ, and sociodemographic questions, including the 10-rung perceived socioeconomic scale ladder (Adler et al., 2000). Participants were randomly presented with questionnaires for completion. In study 1, participants engaged in a 20-min adaptation period. Participants then conducted a 9-min formal baseline period in which they were instructed to sit still and relax, followed by a 9-min mental stress task. The 9-min baseline and stress tasks were then repeated, followed by a cycling exercise task (not reported here). In study 2, participants completed a 15-min adaptation period with the same questionnaires listed above, followed by a 5-min baseline phase. They then engaged in two reaction-time tasks, a 5-min break period, and a 9-min stress task (not reported here). The stress tasks (study 1 and 2) and exercise task (study 1) were part of a separate study aimed at testing the cardiometabolic appropriateness of the acute cardiovascular stress response, not interoception. Hence, data from these tasks are not presented here.
Statistical Analyses
To test that interoceptive accuracy and attention were indeed independent interoceptive domains, a Pearson’s bivariate correlation between interoceptive accuracy and interoceptive attention was conducted. To determine whether accuracy and attention independently predict anxiety or depression symptoms, four initial bivariate regressions were run with interoceptive accuracy and attention individually predicting either depression or anxiety scores. Next, multiple regressions were run with both accuracy and attention as predictors to determine if they each remained independent predictors of depression or anxiety. Finally, a formal moderation analysis was conducted to analyze the interaction of attention and accuracy in predicting anxiety and depression symptoms. All analyses controlled for study cohort and participant sex. Since data were aggregated from two independent studies, the study cohort was controlled for to account for any between-cohort differences that might exist. Participant sex was chosen as a control variable since meta-analytic evidence suggests that interoception may differ by sex (Prentice & Murphy, 2022). All linear regression assumptions were checked and satisfied. All hypotheses and analyses were pre-registered prior to analysis using SPSS (v29) (https://doi.org/10.17605/OSF.IO/WRVF9).
Results: Study 1
Sample Characteristics
Sample (N = 170) characteristics can be found in Table 1. The sample was young, majority female, and White.
Relationship Between Self-Reported Accuracy/Attention
Self-reported interoceptive accuracy and attention were significantly related, r = .168, p = .029. Higher interoceptive accuracy scores were related to higher attention scores.
Depressive Symptomology
Lower self-reported accuracy significantly predicted more depression symptoms, β = −.302, p < .001, whereas interoceptive attention was found not to be a significant predictor, β = .131, p = .086, in bivariate regressions. When entered into a simultaneous regression, lower accuracy, β = −.333, p < .001, and more attention, β = .187, p = .011, both significantly predicted more depression symptoms. A moderation analysis failed to reveal any statistically significant interaction between accuracy and attention, p = .71 (Table 2).
Regression Analyses of Interoception Predicting Depression Symptoms.
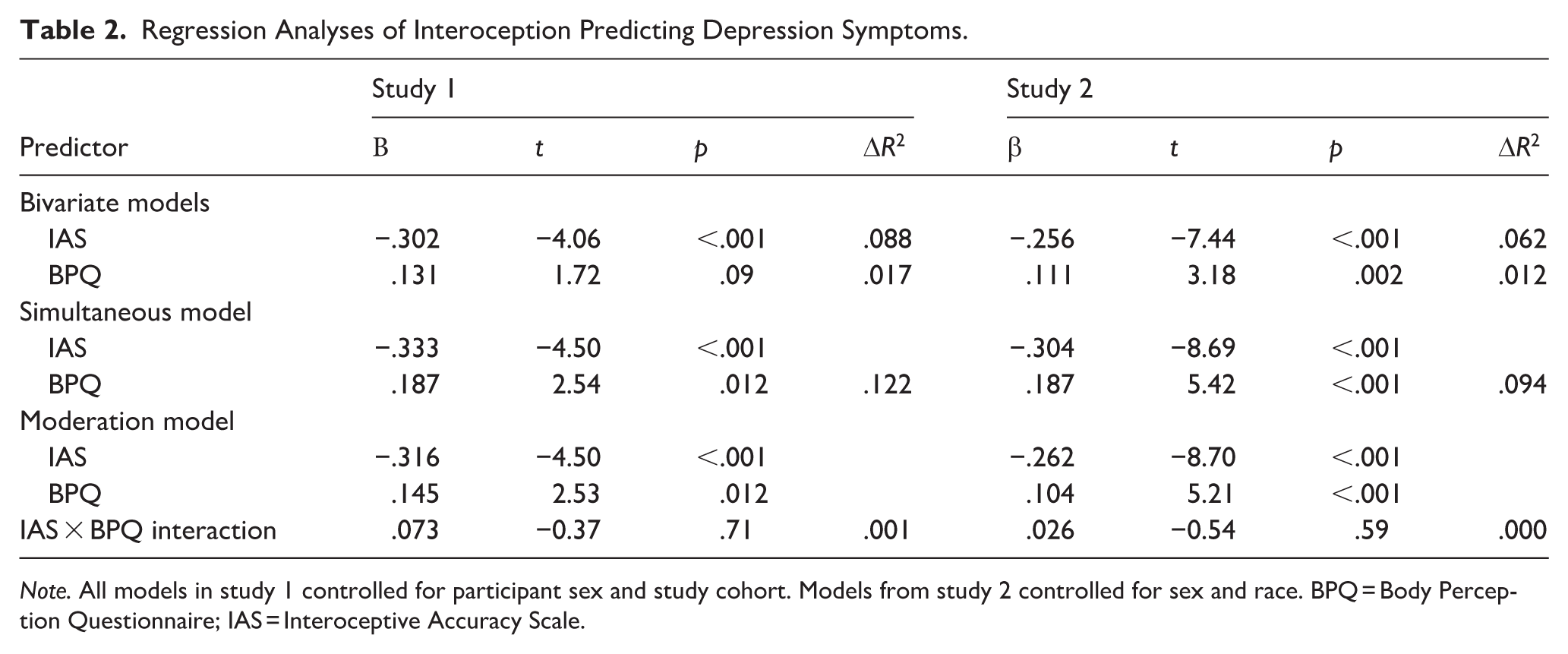
Note. All models in study 1 controlled for participant sex and study cohort. Models from study 2 controlled for sex and race. BPQ = Body Perception Questionnaire; IAS = Interoceptive Accuracy Scale.
Anxiety Symptomology
Separate bivariate regressions showed that lower interoceptive accuracy, β = −.238, p = .002, and more interoceptive attention, β = .204, p = .007, each predicted more anxiety symptoms. When considered together, both accuracy, β = −.280, p < .001, and attention, β = .251, p < .001, remained significant predictors of anxiety. A moderation analysis failed to reveal any statistically significant interaction between accuracy and attention, p = .19 (Table 3).
Regression Analyses of Interoception Predicting Anxiety Symptoms.
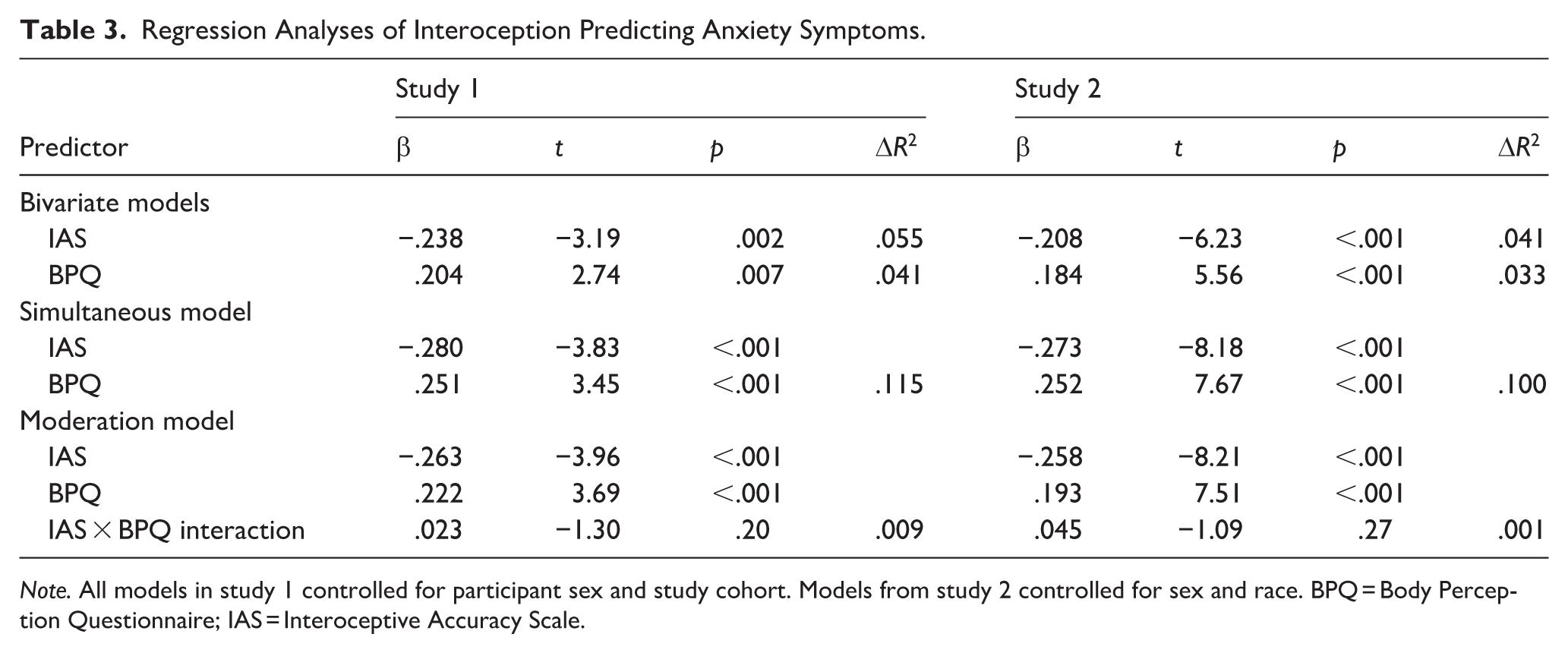
Note. All models in study 1 controlled for participant sex and study cohort. Models from study 2 controlled for sex and race. BPQ = Body Perception Questionnaire; IAS = Interoceptive Accuracy Scale.
Study 1: Discussion
Results of study 1 showed that both interoceptive accuracy and attention were related to mental health. Higher self-reported interoceptive accuracy scores were significantly correlated with lower depression and anxiety symptoms, whereas higher interoceptive attention scores predicted greater depression and anxiety symptoms. Self-reported interoceptive accuracy and attention were marginally correlated, suggesting that they are indeed independent interoceptive domains. No evidence of an interaction between accuracy and attention was observed in the context of depression or anxiety symptoms. As such, these results provide preliminary evidence that self-reported interoceptive accuracy and attention are independent predictors of depression and anxiety symptoms.
The results of this study should be interpreted with caution, given a number of limitations within the study. First, the sample in this study was small and homogenous in terms of race and sex. Second, the small sample size precluded detecting small effects. Third, the questionnaires were completed by participants who were informed that after questionnaire completion, they would engage in a mental stress task. The questionnaires were completed in a random order to guard against order effects; however, it is unclear if the impending tasks affected participant responses. To address these limitations, a follow-up online survey study was conducted, using similar methods, to determine if these relationships persisted in a larger, more representative sample with greater statistical power. Study 2 had the same aims as study 1.
Methods: Study 2
Participants
This study was pre-registered (https://doi.org/10.17605/OSF.IO/WRVF9). A total of 911 (Table 1: 48.6% female, mean age 37.98 years) participants were recruited through the Prolific online research platform. Inclusion criteria included being aged 18 years or older at the time of testing and being a current resident in the United States. This latter criterion was applied because the present study aimed to recruit a representative sample of the United States based on 2023 census data. In all, 85 participants were removed (16 for failing attention checks, 27 for missing BPQ, 11 for missing HADS, 39 for missing IAS, and 1 for stereotyped responding). The final sample consisted of 826 participants due to overlapping missingness. An a priori power analysis found that adequate power (⩾.80) to detect a small effect size of f2 = 0.01 (or larger) with five total predictors (sex, race, main effects, and interaction) required 787. We oversampled to ensure this number of participants was achieved after exclusions from missing data and failed attention checks. The present study was approved by the appropriate University Institutional Review Board, and all participants provided informed consent.
Study Measures
All measures used in study 2 were identical to those in study 1: HADS (Depression α = .84; Anxiety α = .88, both good); IAS (α = .89, good); BPQ (α = .95, excellent).
Procedure
The study was conducted online using the survey platform Prolific (Douglas et al., 2023). Questionnaires were presented in random order to participants and included matrix-type questions, fill-in-the-blank questions, and free-response questions. To ensure participant attentiveness throughout the survey, attention-check questions were interspersed throughout the survey. Once an a priori total sample size was calculated based on power analysis, the sample was divided proportionally to ensure sample representation in line with 2023 government population estimates of major racial/ethnic groups (U.S. Census Bureau, 2023). To do this, surveys were administered to target certain racial/ethnic groups and were released around the clock to collect data from unemployed and employed individuals within the United States. All samples were balanced for sex.
Statistical Analyses
An identical statistical approach was used as described in study 1, with the exception that analyses controlled for only participant sex and race. Race was additionally controlled for in study 2 since the sample was heterogeneous with regard to race (in contrast to study 1), and previous reports suggest that both interoceptive accuracy and attention can vary across racial and ethnic groups (Chentsova-Dutton & Dzokoto, 2014; Ma-Kellams, 2014; Ma-Kellams et al., 2024).
Results: Study 2
Sample Characteristics
Sample (N = 826) sociodemographic factors can be found in Table 1. Participants were roughly half male and female, and racial/ethnic composition successfully reflected 2023 U.S. census data.
Relationship Between Self-Perceived Attention and Accuracy
Self-reported interoceptive accuracy and attention were significantly and positively related, r = .241, p < .001. Higher interoceptive accuracy scores were related to higher attention scores.
Depression Symptoms
Separate bivariate regressions showed that lower interoceptive accuracy, β = −.256, p < .001, and more interoceptive attention, β = .111, p = .002, each predicted more depression symptoms. When considered together, lower accuracy, β = −.304, p < .001, and more attention, β = .187, p = <.001, both remained significant predictors of greater depression symptoms. A moderation analysis failed to reveal any statistically significant interaction between accuracy and attention, p = .59 (Table 2).
Anxiety Symptoms
Separate bivariate regressions revealed that lower self-reported accuracy, β = −.208, p < .001, and more attention, β = .184, p < .001, each predicted anxiety symptoms. In a simultaneous regression, lower accuracy, β = −.273, p < .001, and more attention, β = .252, p < .001, both remained predictors of greater anxiety symptoms. A moderation analysis revealed no significant interaction between interoceptive accuracy and attention, p = .27 (Table 3).
Study 2: Discussion
In study 2, both interoceptive accuracy and attention significantly predicted mental health. Higher self-reported interoceptive accuracy scores were significantly correlated with lower depression and anxiety symptoms, whereas more interoceptive attention scores predicted greater depression and anxiety symptoms. The interaction between accuracy and attention did not predict depression or anxiety symptoms. Given that study 2 was statistically powered to detect even a small interaction between accuracy and attention, these results replicate those found in study 1 and provide further evidence that self-reported interoceptive accuracy and attention are independent predictors of depression and anxiety symptoms.
General Discussion
Dysfunctional interoception is increasingly being recognized as a risk factor for anxiety and depression (Paulus & Stein, 2010). However, prior findings relating interoception to mental health remain mixed. The current studies aimed to reexamine the relationship between self-reported interoceptive attention and accuracy and depression and anxiety symptoms, as well as test whether an interaction between accuracy and attention predicts mental health. In both samples, lower interoceptive accuracy and more interoceptive attention predicted higher depression and anxiety symptoms. In neither sample was evidence found to suggest that accuracy and attention interact to predict depression or anxiety symptoms. As such, in two independent samples differing in sociodemographic composition, convergent results suggest that interoceptive accuracy and attention are independent predictors of depression and anxiety symptoms.
The first aim of the current set of studies was to assess the relationship between interoceptive accuracy and attention, as they are believed to be independent interoceptive domains (Khalsa et al., 2018). If attention and accuracy are indeed independent interoceptive domains, it can be expected that they should not relate to each other, as has been found previously using the BPQ and Interoceptive Attention Scale (Murphy et al., 2020; Tünte et al., 2024). However, in both studies, interoceptive accuracy and interoceptive attention were found to be weakly correlated with one another, such that more attention was related to higher accuracy. This result has been reported previously (Gabriele et al., 2022) and found to derive from some participants conflating accuracy and attention; specifically, interpreting attention-related items on the BPQ as measuring accuracy. It may be that in the current set of studies, a similar misunderstanding occurred in a small fraction of participants, leading to the observed small-magnitude relationship.
Simultaneous regressions showed that both self-reported interoceptive accuracy and attention were strong and independent predictors of depression and anxiety. In both cases, lower belief in interoceptive accuracy and more interoceptive attention predicted greater symptomology. With regard to accuracy, such strong results stand in contrast to the mixed results reported in the literature (Adams et al., 2022; Desmedt et al., 2022; Jenkinson et al., 2024). This should not be totally unexpected since objectively measured interoceptive accuracy only weakly correlates with self-reported accuracy (Murphy et al., 2020); whereas objective measures of accuracy measure performance, subjective measures capture belief in accuracy. However, the directionality of the current results appears to be consistent with studies using objectively measured interoceptive accuracy. Lower objectively measured interoceptive accuracy was related to depression and anxiety, whereas in the current study, a belief in lower accuracy (i.e., subjective accuracy) predicted greater symptoms. The current results regarding interoceptive attention also add to a comparatively smaller literature examining interoceptive attention. For both depression and anxiety symptoms, more attention was related to more symptoms, even after controlling for accuracy. Unexpectedly, in the context of depression in both samples, attention appeared to be qualitatively weaker (albeit statistically significant) than accuracy in predicting symptoms, whereas both accuracy and attention were relatively equal in their ability to predict anxiety symptoms. These results partially accord with a previous study showing that attention, despite being a significant predictor itself, is a weaker predictor than accuracy when predicting depression and anxiety symptoms (Benau, 2023). Although these results should be further replicated, they suggest that although both interoceptive attention and accuracy are significant predictors of mental health, their relative importance may differ as a function of outcome.
Emerging research suggests that attention and accuracy may interact to form specific interoceptive phenotypes that could be differentially pathogenic. Findings indicate that for individuals with lower interoceptive accuracy, the positive relationship between interoceptive attention and health anxiety is stronger (Trevisan et al., 2023). Previous work (Garfinkel et al., 2016) has also demonstrated that high BPQ scores and low cardioperceptive accuracy predict anxiety in participants with autism. Finally, interoceptive accuracy, measured using the gastric loading task, was positively correlated with well-being in individuals exhibiting low interoceptive attention (Ferentzi et al., 2019). Since interoceptive accuracy and attention are often studied in isolation and are rarely examined together, the current study aimed to test the interaction of interoceptive accuracy and interoceptive attention in predicting depression and anxiety symptoms. Contrary to previous literature, no evidence of an interaction between accuracy and attention was found in either study. Importantly, study 2 was statistically powered to detect even a small interaction (f2 = 0.01), suggesting that no meaningful interaction exists between interoceptive accuracy and attention in the context of depression and anxiety. More research is needed to verify potential interactions between interoceptive domains. Reasons for such discrepant results may stem from the use of different objective (Ferentzi et al., 2019; Garfinkel et al., 2016) and subjective (Trevisan et al., 2023) methods to assess interoceptive accuracy. Also, it may be that interoceptive domains only interact in the context of certain populations (i.e., individuals with autism; Garfinkel et al., 2016) or facets of anxiety (i.e., health-related anxiety; Trevisan et al., 2023).
Results of the current study indicate that both accuracy and attention relate to anxiety and depression symptoms. These results reinforce the notion that, in general, interoception might be a potential treatment target for these conditions and further suggest that both accuracy and attention should be considered, preferably together. Already, interoceptive treatments are gaining a foothold in the clinic, particularly in regard to the treatment of anxiety and related panic disorders. For example, capnometry-assisted respiratory training, in which PCO2 (the partial pressure of CO2 in the blood) is increased, and numeric feedback is provided, which patients can then correlate with their breathing patterns to “calibrate” sensations of respiration to gas content in the bloodstream. This method has been shown to help alleviate symptoms of panic and anxiety related to breathing (Davies et al., 2019; Meuret et al., 2009, 2010). Similarly, in a randomized controlled trial among individuals with autism, it was found that heartbeat detection with feedback significantly decreased anxiety at 1-week and 3-month follow-ups (Quadt et al., 2021). Although both examples are interventions targeted at improving interoceptive accuracy, it remains unclear whether targeting interoceptive attention could augment treatment results or if interoceptive attention could act as a modifying factor.
The studies described above must be interpreted in the context of several limitations. First, interoceptive accuracy and attention were measured using self-report survey methods. Although this is a standard and common practice for measuring interoceptive attention, objective measures of interoception, especially accuracy, do exist (e.g., heart rate tracking). However, the IAS has been previously shown to weakly correlate with objective measures from the heartbeat counting task (Murphy et al., 2020). Second, both studies were cross-sectional, so no causality or directionality can be inferred. In fact, contrary to the directionality in the current set of studies, others have reported that depression and anxiety symptoms interact to predict interoceptive accuracy (Dunn et al., 2010; Pollatos et al., 2009). However, altered interoception is increasingly being considered an underlying risk factor of depression and anxiety, and preliminary causal links are emerging from clinical trials whereby clinically induced changes in interoception appear to cause improvement in depression and anxiety (Heim et al., 2023). Finally, in both studies, a small, yet statistically significant, positive relationship was observed between measures of interoceptive attention and accuracy. It may be that participants misinterpreted items, conflating both accuracy and attention. However, it is not believed that this relationship confounded the reported results because, in fact, measures of attention and accuracy are differentially related to depression and anxiety symptoms; future studies should include items to disentangle participant understanding (e.g., Gabriele et al., 2022).
In conclusion, the current studies addressed the relationships between interoceptive accuracy and attention, anxiety, and depression symptoms. Collectively, the results of both studies, from independent cohorts, revealed that anxiety and depression symptoms were related to lower self-perceived accuracy as well as higher attention. In neither study was evidence found to suggest that accuracy and attention interact to predict anxiety or depression symptoms. These findings inform basic research on the link between anxiety and depression and interoception, as well as further characterize the extent to which interoception may be involved in mental health.
Supplemental Material
sj-docx-1-qjp-10.1177_17470218261446824 – Supplemental material for Self-Reported Interoceptive Accuracy and Attention Do Not Interact to Predict Depression and Anxiety Symptoms: A Conceptual Replication Across Two Independent Samples
Supplemental material, sj-docx-1-qjp-10.1177_17470218261446824 for Self-Reported Interoceptive Accuracy and Attention Do Not Interact to Predict Depression and Anxiety Symptoms: A Conceptual Replication Across Two Independent Samples by Paige Gray, Bailey Hedgemon, Ann Carlton Keller, Hollins Pierpoint, Maria Johanna Vargas and Ryan C. Brindle in Quarterly Journal of Experimental Psychology
Footnotes
Acknowledgements
The authors would like to thank all of the participants and research assistants who contributed to these studies.
Ethical Considerations
Both studies in this manuscript received approval from the appropriate Institutional Review Board.
Consent to Participate
All participants provided written informed consent prior to participating in these studies.
Author Contributions
PG, BH, ACK, HP, and MJV: Conceptualization, Formal analysis, Investigation, Writing – original draft, Writing – review and editing. RCB: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Project administration, Supervision, Writing – original draft, Writing – review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research came from the Washington and Lee University Lenfest Fund and Summer Research Scholars Program, the Thomas F. and Kate Miller Jeffress Memorial Trust, Bank of America, Trustee and specified donor Hazel Thorpe Carman and George Gay Carman Trust, and Virginia Foundation for Independent Colleges. The funding sources had no involvement in the study design or in the collecting, analyzing, or reporting of data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, RCB, upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.