
Abstract
Background
Hairdresser-related ischemic cerebrovascular events (HICE) are attributed to compression of vertebral arteries or cervical artery dissections. We determined their frequency, mechanisms, localization and outcome in a pre-specified study.
Methods
We prospectively collected ischemic strokes and transient ischemic attacks occurring in relation to a hairdresser visit from 2002 to 2013, using consecutive data from an ischemic stroke registry (ASTRAL). HICE were compared to all other acute ischemic strokes in ASTRAL.
Results
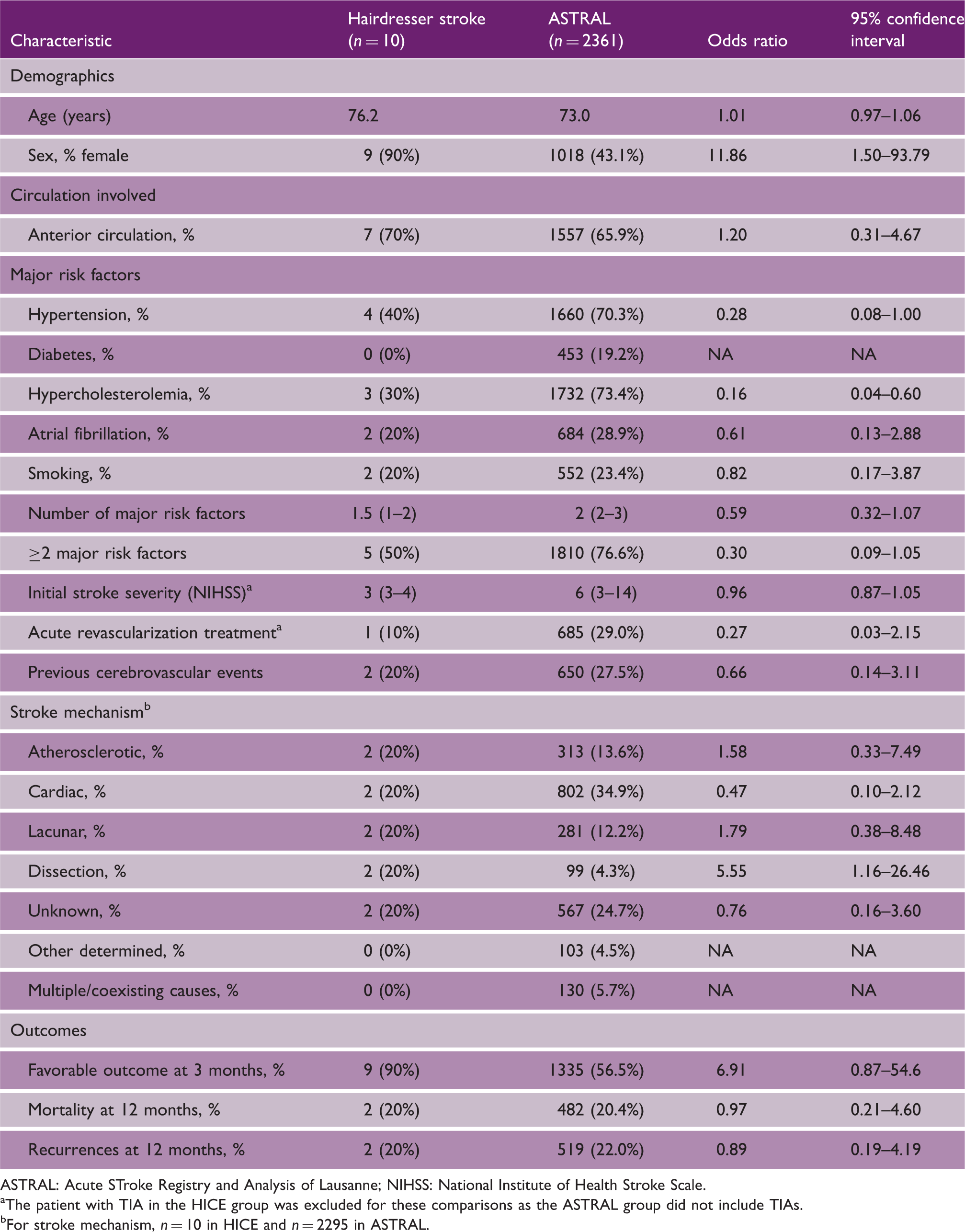
We identified 10 HICE (9 strokes and 1 transient ischemic attack). Age and anterior-posterior distribution were similar with a significantly higher rate of females (90% vs. 43%, p = 0.02) in the HICE group compared to ASTRAL. Patients with HICE had significantly lower incidence of hyperlipidemia (30% vs. 73%) and diabetes (0% vs. 19%). The mechanisms of HICE were diverse: carotid artery dissection (n = 2), cardiac (n = 2), lacunar (n = 2), other determined (n = 2) and unknown etiology (n = 2). Two HICE with atherosclerotic intracranial disease were possibly caused by acute hemodynamic changes related to systemic hypotension during hot air hair drying. Unadjusted favorable outcome at three months seemed to be better in HICE (90% vs. 57%), and 12-month mortality and recurrences were similar.
Conclusions
HICE may occur frequently in females without a predilection for the posterior circulation. Although some HICE may occur by chance (pseudo-HICE), hairdresser visits may have a causal role in some cases, including cervical artery dissection or hemodynamic compromise related to pre-existing arterial disease (true HICE). Available data are insufficient for specific preventive recommendations.
Introduction
Ischemic strokes (ISs) temporally related to a hairdresser visit have been first described by Weintraub et al.,1,2 who coined the term “Beauty Parlor Stroke Syndrome.” Further publications on the topic have been scarce and limited to small case series.3,4 We aimed at determining the frequency, mechanisms, localization and outcome of a prospectively collected sample of hairdresser-related ischemic cerebrovascular events (HICE).
Methods
We defined HICE as an ischemic stroke or transient ischemic attack (TIA) during or shortly after a hairdresser visit. We prospectively collected patients fulfilling these criteria from 2002 to 2013. The medical charts and neuroimaging were retrospectively reviewed, and the Acute STroke Registry and Analysis of Lausanne (ASTRAL) 5 was used to complete missing data and identify the non-HICE group. ASTRAL is a prospective consecutive cohort initiated in 2003 of acute ischemic stroke patients admitted to our stroke unit within 24 h of symptom onset. All patients underwent metabolic and cerebrovascular imaging. Each group was compared for demographics, risk factors (hypertension, hyperlipidemia, atrial fibrillation, diabetes and smoking), vascular territory, National Institute of Health Stroke Scale (NIHSS) score and revascularization treatment. The stroke mechanisms were classified as per Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria, with dissections and multiple causes added. Acute neuroimaging was reviewed for ischemic lesions and arterial pathology. Modified Rankin scale was considered favorable if the score was ≤2 at three months. At 12 months, mortality was assessed by telephonic interview. The data of the TIA patient in the HICE group were excluded when admission NIHSS and outcomes were compared with the IS control group. Statistical analyses were conducted with STATA 13.1 (StataCorp, College Station, TX).
ASTRAL is approved for prospective data collection and retrospective analysis by the Ethics Committee for Research on Humans of the Canton de Vaud, Switzerland.
Results
HICE and non-HICE ASTRAL patients
ASTRAL: Acute STroke Registry and Analysis of Lausanne; NIHSS: National Institute of Health Stroke Scale.
The patient with TIA in the HICE group was excluded for these comparisons as the ASTRAL group did not include TIAs.
For stroke mechanism, n = 10 in HICE and n = 2295 in ASTRAL.
Age distribution was similar between groups, but there were significantly more women in the HICE group. The median admission NIHSS was non-significantly lower (3 vs. 6). Both patients with carotid dissections (Figure 1) had acute unilateral head and neck pain immediately after the hairdresser visit, followed by an ipsilateral TIA and IS on the same day (#5) and by an IS 10 days later (#6). The patient presenting with a TIA (#9) had paraparesis at the end of the hairdresser visit. Her symptoms resolved after 6 h, magnetic resonance imaging was negative, and a hemodynamic pontine TIA related to atherosclerotic vertebral artery stenosis was diagnosed (Supplementary Table, which can be found online with this article, http://wso.sagepub.com).
(a and b) Patient #8: (a) right lenticulostriate stroke with (b) tight right proximal middle cerebral artery stenosis. (c and d) Patient #5: (c) right deep and superficial middle cerebral artery stroke with (d) high right internal carotid dissection.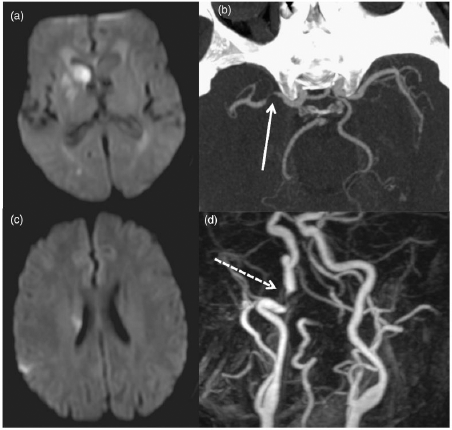
HICE patients had less major risk factors than the control group (Table 1). They had multiple different stroke mechanisms, with dissections being more frequent. Two patients who also had hot air hair drying possibly had hemodynamic decompensation of their intracranial atherosclerotic M1 (#8, Figure 1(a) and (b)) and V4 stenosis (#9).
The posterior circulation was not more often involved in HICE. Vertebral artery hypoplasia was seen in one patient with clinically acute right pontine lacunar stroke (#8). One HICE patient (#10) with right middle cerebral artery occlusion due to new onset atrial fibrillation received intravenous thrombolysis and thrombectomy.
Over 12 months, two HICE patients had recurrences: patient #6 with an occlusive carotid dissection had recurrent minor anterior cerebral artery and middle cerebral artery strokes at 6 and 11 days, respectively. Patient #8 had a TIA at 15 days related to atheromatous M1 stenosis. The recurrence rate of 20% for ISs and TIAs over 12 months was similar to the control group (Table 1). Unadjusted favorable outcome at three months was somewhat better in HICE than in controls, whereas 12-month mortality was similar.
Discussion
In a pre-specified analysis of HICE patients over 11 years, we found higher rate of females, and non-significantly lower burden of cerebrovascular risk factors and admission NIHSS. Posterior circulation involvement was similar, and the rate of dissections was higher. Previous series have shown a higher proportion of women in HICE.1,2
Posterior circulation has been hypothesized to be more often involved in HICE.1,2 Shimura et al. 4 reported that 12 of 500 consecutive posterior circulation strokes were likely related to a hairdresser visit. These authors proposed an impingement of the vertebral artery during neck rotation and hyperextension while shampooing as a mechanism, with possible additive effects from hypoplasia, atherosclerosis, intimal injury and stasis. Patients with symptoms of brainstem ischemia showed vertebral artery hypoperfusion with neck angulation during dynamic magnetic resonance angiography. 6 However, patients with dizziness during shampooing showed no changes in vertebrobasilar hemodynamics during neck extension with vascular ultrasound. 7 In our series, we did not confirm an increased frequency of posterior circulation stroke and therefore find no support for previous recommendations about a flexed shampooing posture. 2
Dissection seems to be one likely cause of HICE in our series. This observation was previously made for anterior 3 and posterior circulation strokes 8 and may be explained by the stretching of the artery during unusual neck positions. In addition, two of our patients probably had HICE related to hemodynamic decompensation of atherosclerotic disease, possibly from vasovagal activation during hot air hair drying. We considered both these patients (#8 and #9), as well as two patients with arterial dissections (#5 and #6) to be “true HICE” with a possible direct causal link to the hairdresser visit, whereas the cerebrovascular event in other patients may have been a chance occurrence (“pseudo-HICE”).
Three-month functional outcome was somewhat better after HICE compared to control patients, which may be related to a lower initial NIHSS, but the small number of HICE patients limits the relevance of this observation.
Strengths of our study are the pre-specified analysis, the long observation period, thorough cerebrovascular work-up and a large comparison sample from the same population. Limitations are the retrospective, non-randomized analysis of the study, the small number of identified HICE and the absence of detailed recording of type and duration of head positioning and other pathophysiological parameters during the hairdresser visit.
In conclusion, HICE are seen more commonly in females but do not seem to have a predilection for the posterior circulation. These strokes may be due to chance occurrence in some patients (“pseudo-HICE”). Still, a lower rate of cerebrovascular risk factors in HICE suggest possible mechanisms that are causally related to the hairdresser visit (true HICE), such as cervical artery dissections and hemodynamic decompensation of pre-existing arterial disease. It was recently recommended that practitioners should inform patients of a possible risk between cervical manipulation therapy and vertebral artery dissection stroke. 9 Our data are insufficient to suggest specific preventive recommendations to persons visiting the hairdresser.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Pamela Correia received a Swiss Government Excellence Scholarship to work at the Centre Hospitalier Universitaire Vaudois, Switzerland.