
Abstract

Dear editor,
Beta-thalassemia is a genetic disorder that is due to a reduced or complete absence of synthesis of β-globin chain in a molecule of hemoglobin. Burden with about 200 mg of iron per unit of packed red blood cells and moderately increased gastrointestinal uptake of iron due to the suppression of hepcidin 1 leads to increased content of microelement in the body, which requires lifetime use of chelation therapy aimed to prevent or revers of related iron accumulation complications. In patients with thalassemia intermedia, there is a higher incidence of pulmonary hypertension and thrombosis.2,3 Iron overload is a result from repeated blood transfusions combined with increased gastrointestinal absorption in terms of ineffective erythropoiesis.
Hepcidin is a peptide of 25 amino acids, 4 whose main function is to inhibit the uptake of iron in plasma from three main sources: absorbed from food in the duodenum, recycled released by macrophages and released from landfills in hepatocytes. 5 The formation of hepcidin is regulated by the concentration of the iron – in elevated iron concentration a large amounts hepcidin are secreted, which inhibits further iron absorption. The opposite occurs with iron deficiency – separation of hepcidin is reduced or stopped in order to be able to absorb a sufficient amount of microelement. Except in iron overload, the concentration of hepcidin increases in inflammation; it decreases in hypoxia. In β-thalassemia occurs very low hepcidin despite the excessive iron burden.6,7 It is believed that the reason for this dominance is the need of iron in erythropoiesis activated and tissue hypoxia.
Samples were taken from 23 patients with thalassemia; 4 of them with stroke; average age 35.2 ± 2.9. Their results were compared to 19 ischemic stroke cases; average age 41.9 ± 3.5. We measure serum iron, hepcidin and ferritin levels. Pearson’s coefficient and Student’s t-test were used for evaluation of correlation and statistical significance. Patients were signing the informed consent according to the Declaration of Helsinki (Directive 2001/20/EC).
We found significant decreased hepcidin concentrations in thalassemia patients 0.95 ± 0.2 µg/L. Patients with acute ischemic stroke showed elevated hepcidin levels 87.8 ± 9.4 µg/L, (P < 0.001) (Figure 1).
Serum hepcidin levels (in µg/L).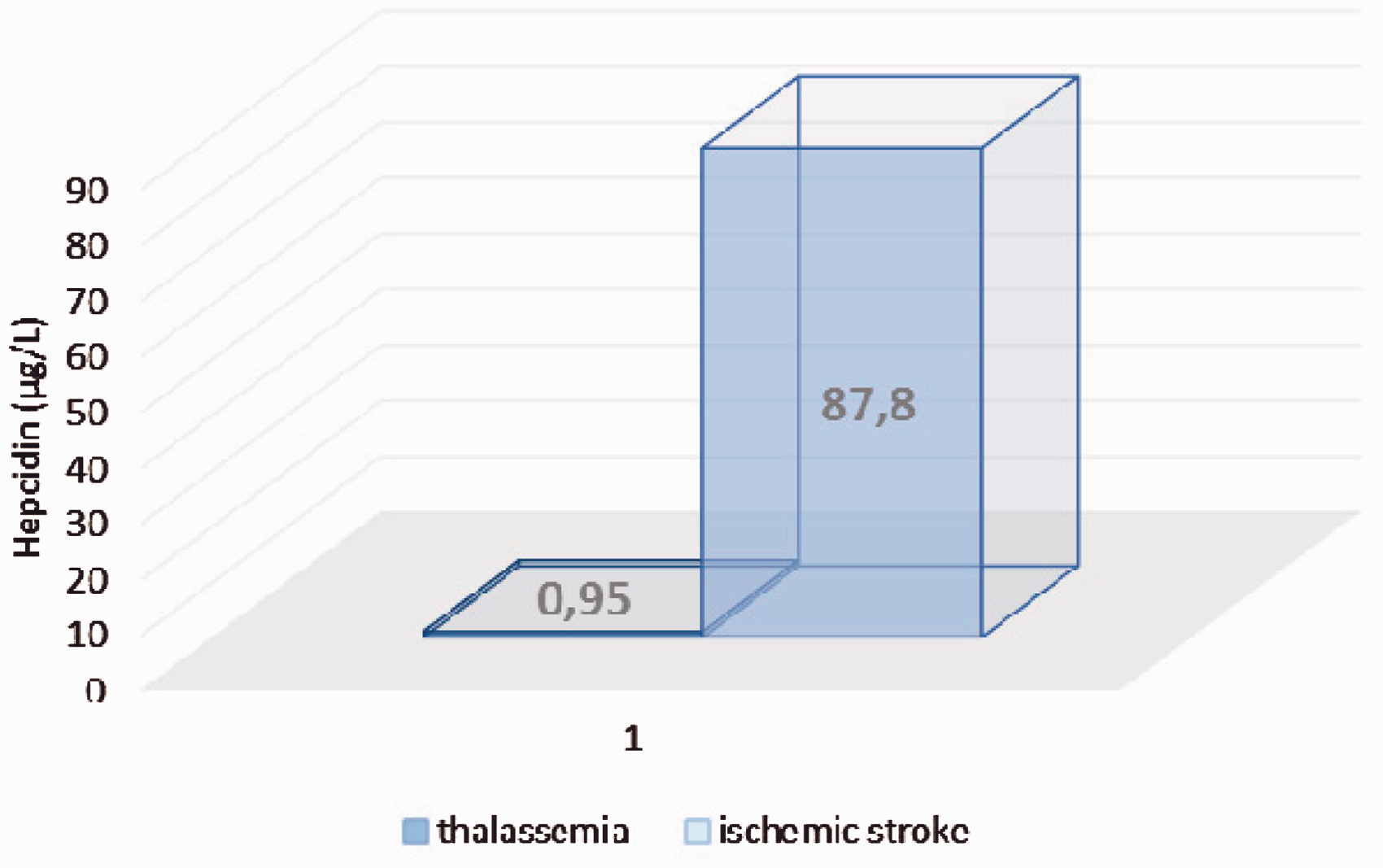
Serum iron levels were increased in both groups: 75.4 ± 12.1 µmol/L in thalassemia vs. 29.4 ± 2.8 µmol/L in ischemic stroke, P < 0.001 (Figure 2).
Serum iron concentrations (in µmol/L).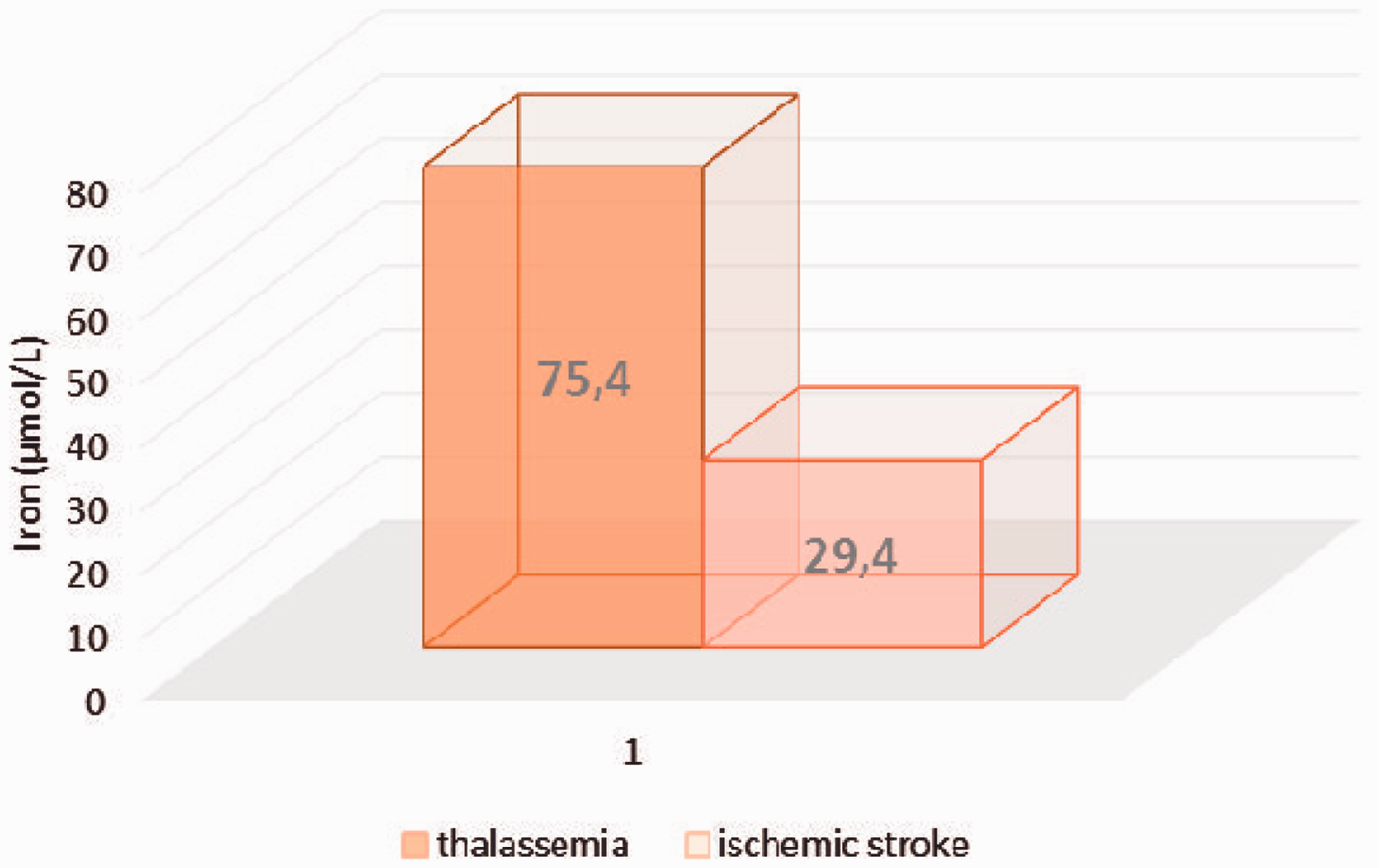
It is known that free iron increases significantly during ischemia and is responsible for oxidative damage in the brain. Increased hypoxia inducible factors leads to an oxidative stress, which plays an important role in neuronal injuries caused by cerebral ischemia.
The burden of iron overload in beta-thalassemia was unaffected by treatment with chelators, which can have severe side effects. There are a few studies about micro-hepcidin as an alternative of chelation therapy, especially in patients without transfusion therapy. 8 Treatment with hepcidin may have a beneficial effect and ineffective erythropoiesis.
Hepcidin measurement in cases of beta-thalassemia is important to determine whether transfusion treatment is effective in terms of ineffective erythropoiesis. It will avoid any further iron supplementation therapy in cases of microelement overload.
Footnotes
Acknowledgments
We kindly appreciate support for clinical laboratory evaluations from “Marvena” (“Siemens Healthcare”distributor in Bulgaria), and especially to Mr. Velizar Dragoev and Mrs. Silvia Kirova.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is implemented with the support of the Medical University – Sofia, as part of “Grant 2015”.