
Abstract
Background and Purpose
Vorapaxar, a novel platelet thrombin protease-activated receptor 1 blocker, is currently approved for post-myocardial infarction and peripheral artery disease indications on top of clopidogrel or/and aspirin. We sought to summarize the conflicting stroke data after vorapaxar for justifying a secondary stroke prevention trial.
Methods
Analyses of the stroke data after vorapaxar yielded from thrombin-receptor antagonist vorapaxar in acute coronary syndromes (TRACER) and TRA2P clinical trials, and affiliated Food and Drug Administration (FDA) reviews.
Results
The stroke data are mixed, with catastrophic 2.5 excess of intracranial bleeding risks (HR = 2.52; 95% CI = 1.46–4.36, p < 0.0001); trend to worsened second stroke rates (13.0% vs. 11.7%; HR = 1.03; 95% CI = 0.85–1.25, p = NS), but a hint towards less primary ischemic strokes in vorapaxar indicated population (HR = 0.57; 95% CI = 0.43 to 0.75; p < 0.001). These conflicting data are not solely attributed to vorapaxar, but rather reflect unreasonably aggressive triple antiplatelet strategies utilized frequently in TRA2P and dominant in TRACER. Overall, the FDA-confirmed evidence advocates future vorapaxar secondary stroke prevention trial due to being first-in-class agent, unique pharmakynetics, and exhibiting very mild “comfort zone” antiplatelet profile. The three arm trial testing head-to-head monotherapy with vorapaxar (Zontivity®), versus clopidogrel (Plavix®), and versus extended-released dipyridamole with very low dose aspirin (Aggrenox®) is warranted.
Conclusions
Vorapaxar may be superior to currently recommended antiplatelet strategies and should be tested as a monotherapy in a randomized outcome-driven secondary stroke prevention trial.
Introduction
Development of novel antiplatelet agents has been generally established for the management of patients with clinically evident coronary atherothrombosis. In contrast, these agents have shown limited (if any) efficacy in the prevention of cerebrovascular occlusions, and consistent harm in patients with a history of stroke or transient ischemic attack with regard to elevated bleeding risk including excess of deadly intracranial hemorrhages.1,2 Vorapaxar is a selective, orally active, potent, and competitive protease-activated receptor 1 (PAR-1) antagonist that potently inhibits thrombin-induced platelet activation. 3 The drug Phase III program included two large outcome trials in patients with acute and chronic coronary atherothrombosis, namely thrombin-receptor antagonist vorapaxar in acute coronary syndromes (TRACER), 4 and trial to assess the effects of SCH 530348 in preventing heart attack and stroke in patients with arteriosclerosis (TRA 2P-TIMI 50). 5
Methods
Herein, the efficacy and safety of vorapaxar related to stroke are briefly reviewed with a focus on the perspectives and obstacles for an outcome-driven stroke prevention trial. We critically assessed the stroke data from vorapaxar trials, and affiliated Food and Drug Administration (FDA) reviews.
Results
Vorapaxar and stroke
The most evidence with regard to stroke has been driven from the overall successful TRA2P secondary pre-specified analyses. Indeed, among patients who qualified with stroke (N = 4883) had a history of ischemic stroke in the prior 2 weeks to 12 months. The qualifying stroke was classified as large vessel in 35%, small vessel in 47%, and other/unknown in 18%. In the stroke cohort, cardiovascular death, myocardial infarction, or stroke through three years were not reduced with vorapaxar versus placebo (13.0% vs. 11.7%; hazard ratio, 1.03; 95% confidence interval, 0.85–1.25), including recurrent ischemic stroke (hazard ratio, 0.99; 95% confidence interval, 0.78–1.25). 6 There were no significant differences in the effect of vorapaxar based on the type or timing of the qualifying stroke. Intracranial hemorrhage at three years was increased with vorapaxar (2.5% vs. 1.0%; hazard ratio, 2.52; 95% confidence interval, 1.46–4.36). The study concluded that in patients with prior ischemic stroke who receive standard antiplatelet therapy, adding vorapaxar increased the risk of intracranial hemorrhage without an improvement in major vascular events, including ischemic stroke. 6 Moreover, the elegant quality meta-analyses of 9 PAR-1 antagonist trials including 42,000 patients with a history of thrombotic vascular disease or acute coronary syndrome, PAR-1 antagonist treatment was associated with a highly significantly increased risk of intracranial hemorrhage (0.59% vs. 0.30%; relative risk, 1.98; 95% CI = 1.46–2.68; p < 0.00001; number needed to harm = 345). There was no heterogeneity across trials (p = 0.84; I2 = 0%), PAR-1 antagonist agent (p = 0.52), treatment duration (p = 0.38), or trial-qualifying event (p = 0.59). Risk of death from any cause or a cardiovascular cause did not differ between active treatment and control groups. In a large pooled analysis, PAR-1 antagonist therapy was associated with an increased risk for intracranial hemorrhage. 7 The encouraging news, however, were yielded from another TRA2P indicated population analyses. That study triaged and looked at the myocardial infarction or peripheral disease patients with no prior stroke or transient ischemic attack. Importantly, vorapaxar reduced first ischemic stroke (HR = 0.57, 95% CI = 0.43 to 0.75; p < 0.001). The risk of hemorrhagic conversion after stroke (HR: 1.19, 95% CI = 0.49 to 2.91; p = 0.70) or death (HR: 1.09, 95% CI = 0.57 to 2.07; p = 0.79) during follow-up trended to be higher, but not significantly increased with vorapaxar in patients who had a new (n = 204) ischemic stroke (12). 8 Although hemorrhagic stroke was borderline increased (HR: 2.79, 95% CI = 1.00 to 7.73; p = 0.049), overall stroke was significantly reduced (HR: 0.67, 95% CI = 0.52 to 0.87; p = 0.002) (12). 8 So, importantly, vorapaxar reduces first ischemic stroke in TRA2P indicated population cohort.
The FDA reviews
Advantages and obstacles for vorapaxar stroke prevention trial
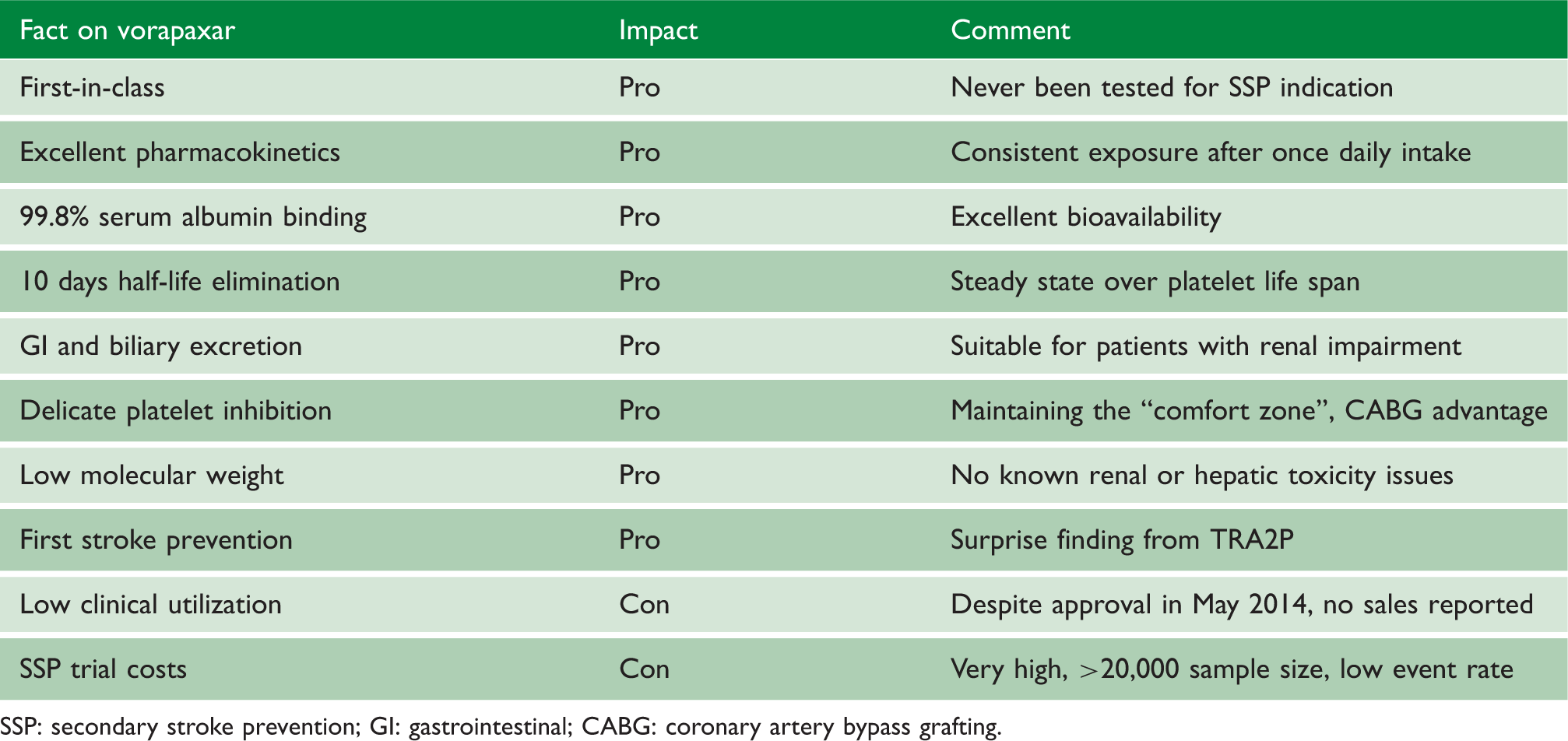
SSP: secondary stroke prevention; GI: gastrointestinal; CABG: coronary artery bypass grafting.
Discussion
In addition, to the facts outlined in Table 1, negative findings in TRACER and TRA2P with regard to stroke are predominantly related to overtreatment and are not applicable to per se vorapaxar antiplatelet properties. Applying the proposed vorapaxar monotherapy will ultimately yield much milder platelet inhibition, and most likely be superior to clopidogrel and dipyridamole with regard to bleeding risks in general, and hopefully intracranial hemorrhages in particular in stroke victims. On the other hand, borderline efficacy results of the latest SSP trials, high failure rates, and limited commercial success for the sponsors may represent the array of substantial obstacles for the new trial implementation. Indeed, the impact of event incidence miscalculations, heterogeneous population, different level of general health, concomitant comorbidities or/and medications in violation of protocol, and unwillingness to perform and accept subgroup analysis based on geographic regions somewhat clouded recent worldwide SSP mega trials.11–13 By initially aggressive unreasonable design, TRA2P and TRACER were prone to fail for stroke prevention and cause more intracranial bleedings. The “good news” is that vorapaxar per se can be most definitely exonerated from the harm observed for stroke prevention, and especially from alarming ICH numbers. 14 The bad news is that vorapaxar has been approved in May 2014, but it’s clinical utilization is still very low, or even not existing in many remote from US markets. It seems that despite the heavy expense of investing in two mega trials, it is challenging to test vorapaxar as a monotherapy in another head-to-head stroke prevention study against clopidogrel and extended-released dipyridamole. Hopefully, future development of PAR1/PAR4 agents will learn from the pitfalls from the initial experience with vorapaxar, and will apply way more delicate strategies, especially relevant for stroke victims.
Footnotes
Acknowledgments
We wish to thank Dr. Wolfganf Eisert for constructive comments.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: VLS is listed as an inventor for the issued US patent “Treating vascular events with statins by inhibiting PAR-1 and PAR-4” (7,842,716) assigned to HeartDrug™ Research; and “Method for treatment of platelet activity with E5555” (USN 61/080,791); assigned to Eisai and HeartDrug™. He received compensation for the issued U.S. Patent 11/996,380 “Use of PAR-1/PAR-4 inhibitors for treating and preventing vascular diseases” on prasugrel assigned to Lilly. MHK and DFH have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Part of this work was supported by the “Brain Pool” program funded by the Korean Ministry of Science and Technology to VLS.