Stroke is the leading cause of disability, the second cause of dementia and one of the most prevalent causes of death in high- to middle-income countries.1 Nevertheless, geographical barriers and limited resources impose differing levels of access to health services and prevent adequate care for acute stroke patients.2 In two decades, telemedicine applied to cerebrovascular disease has facilitated the administration of thrombolytic therapy successfully to a larger number of patients with ischemic stroke and increased the efficacy of stroke units.3 The rapid expansion and practice of telemedicine networks has allowed the development of evidences for use and the implementation of guidelines.4
Our hub stroke research center partnered with two stroke community hospitals, and a five-year prospective cohort study of stroke patients was conducted. Consultations were held to make shared decisions on treatment with recombinant tissue plasminogen activator (rtPA). A total of 1189 patients with acute ischemic stroke were diagnosed by the referring centers, 81 (6.81%) were evaluated using telestroke and 56.8% were treated with intravenous rtPA. Mean baseline National Institutes of Health Stroke Scale score was 14.3 (vs. 13.7 in tertiary center, p = 0.48). Door-to-needle time was 15 min longer in telestroke patients than in the tertiary center (p < 0.001), due to teleconsultation (p < 0.001 in CT-needle time). However, there were similar rates of symptomatic cerebral hemorrhage (2.2% vs. 3.6%, p = 0.8) and long-term mortality (17% vs. 21%, p = 0.72) with a trend towards higher disability (39.6% had a modified Rankin scale score of ≤2 vs. 55.6%, p = 0.07) (Table 1).
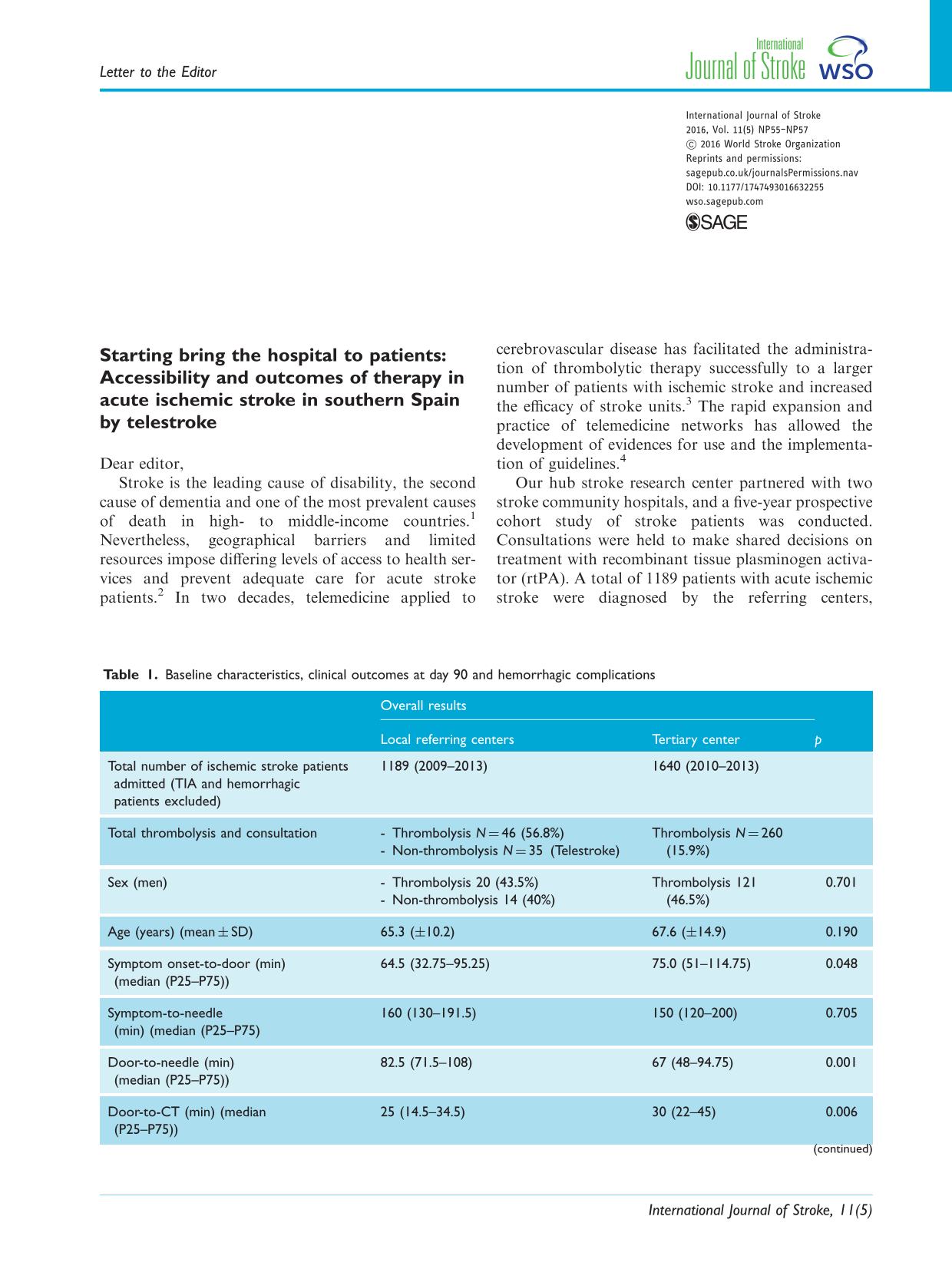
Baseline characteristics, clinical outcomes at day 90 and hemorrhagic complications
Overall results
Local referring centers
Tertiary center
p
Total number of ischemic stroke patients admitted (TIA and hemorrhagic patients excluded)
1189 (2009–2013)
1640 (2010–2013)
Total thrombolysis and consultation
- Thrombolysis N = 46 (56.8%) - Non-thrombolysis N = 35 (Telestroke)
Door-to-CT: time between the emergency department admission service or first emergency medical care and cranial CT; CT-to-needle: time from cranial CT and the beginning of treatment; NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin scale.
Classification of The European Cooperative Acute Stroke Study III.
Telestroke safely select a large number of patients requiring intravenous rtPA. The results are similar in terms of efficacy and safety in experienced centers, and unnecessary transfers of patients are avoided. Telestroke is now considered key to clinical practice in academic and community environments. So, it has been demonstrated that high-quality telestroke consultations can be performed with mobile enhancing the portability of the service and to progress in the prehospital setting.5 This field appears to be advancing via creative postimplementation studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by a grant from the Spanish Ministry of Health and Consumer Affairs (Instituto de Salud Carlos III)” and “FIS (Fondo de Investigación Sanitaria)/Reference.
EvensonKRForakerREMorrisDLRosamondWD. A comprehensive review of prehospital and in-hospital delay times in acute stroke-care. Int J Stroke2009; 4: 187–199.
3.
SchwabSVatankhahBKuklaCet al.TEMPiS Group. Long-term outcome after thrombolysis in telemedical stroke care. Neurology2007; 69: 898–903.
4.
SchwammLHAudebertHJAmarencoPet al.Recommendations for the implementation of telemedicine within stroke systems of care: a policy statement from the American Heart Association. Stroke2009; 40: 2635–2660.
5.
WeberJEEbingerMRozanskiMet al.Prehospital thrombolysis in acute stroke: results of the PHANTOM-S pilot study. Neurology2013; 80: 163–168.