
Abstract
Rationale
Endovascular therapy after acute ischemic stroke due to large vessel occlusion is now standard of care. There is equipoise as to what kind of anesthesia patients should receive during the procedure. Observational studies suggest that general anesthesia is associated with worse outcomes compared to conscious sedation. However, the findings may have been biased. Randomized clinical trials are needed to determine whether the choice of anesthesia may influence outcome.
Aim and hypothesis
The objective of GOLIATH (General or Local Anestesia in Intra Arterial Therapy) is to examine whether the choice of anesthetic regime during endovascular therapy for acute ischemic stroke influence patient outcome. Our hypothesis is that that conscious sedation is associated with less infarct growth and better functional outcome.
Methods
GOLIATH is an investigator-initiated, single-center, randomized study. Patients with acute ischemic stroke, scheduled for endovascular therapy, are randomized to receive either general anesthesia or conscious sedation.
Study outcomes
The primary outcome measure is infarct growth after 48–72 h (determined by serial diffusion-weighted magnetic resonance imaging). Secondary outcomes include 90-day modified Rankin Scale score, time parameters, blood pressure variables, use of vasopressors, procedural and anesthetic complications, success of revascularization, radiation dose, and amount of contrast media.
Discussion
Choice of anesthesia may influence outcome in acute ischemic stroke patients undergoing endovascular therapy. The results from this study may guide future decisions regarding the optimal anesthetic regime for endovascular therapy. In addition, this study may provide preliminary data for a multicenter randomized trial.
Keywords
Introduction and rationale
Endovascular therapy (EVT) is now evidence-based standard care for patients with acute ischemic stroke (AIS) caused by large vessel occlusion (LVO) presenting less than 6 h after symptom onset.1–5 However, several questions remain regarding optimal patient selection and treatment approach.
Controversy exists whether general anesthesia (GA) or conscious sedation (CS) should be used during EVT for AIS.6,7 No randomized trials address this question. Benefits of GA include airway protection, pain control, and patient immobility for potential improved radiographic imaging and intervention. Conversely, GA is time consuming and possibly associated with longer time to groin puncture and revascularization. Furthermore, hypotension with the risk of further ischemic injury can occur during GA. Advantages of CS might include shorter time to revascularization, fewer hemodynamic problems, and the possibility for better neurological assessment during the procedure. The main arguments against CS are that patient movement can result in procedural complications, higher radiation dose, the need of more contrast media, and the lack of airway control.8,9 In case of excessive patient movement, conversion to GA would subject the patient to an even longer procedure time.
Recent observational studies have suggested that GA may worsen neurological outcome and increase mortality.10–13 However, these results might be affected by confounding and selection bias. In these studies, National Institute of Health Stroke Score (NIHSS) was higher in the GA group, and GA was reserved for patients who could not cooperate and those with airway obstruction. None of the studies included a protocol for selecting either GA or CS. Furthermore, few observational studies reported detailed data on changes in blood pressure and type and dosage of administered anesthetics.14–16 Hypotension during EVT is a risk factor for poor neurological outcome. 17 Two studies have suggested that lower blood pressures associated with GA may explain the worse outcome.15,18 However, a recent study found no correlation between blood pressure and outcome, but a protective effect of volatile anesthetics. 16 Type and dosage of anesthetics and artificial ventilation with PaCO2 changes may also influence cerebral blood flow, oxygenation and outcome.
Hypothesis and objective
We hypothesize that patients receiving EVT under CS will have less tissue damage and better clinical outcomes, i.e. less growth of infarct and lower mRS than patients receiving EVT under GA.
Outcome measures
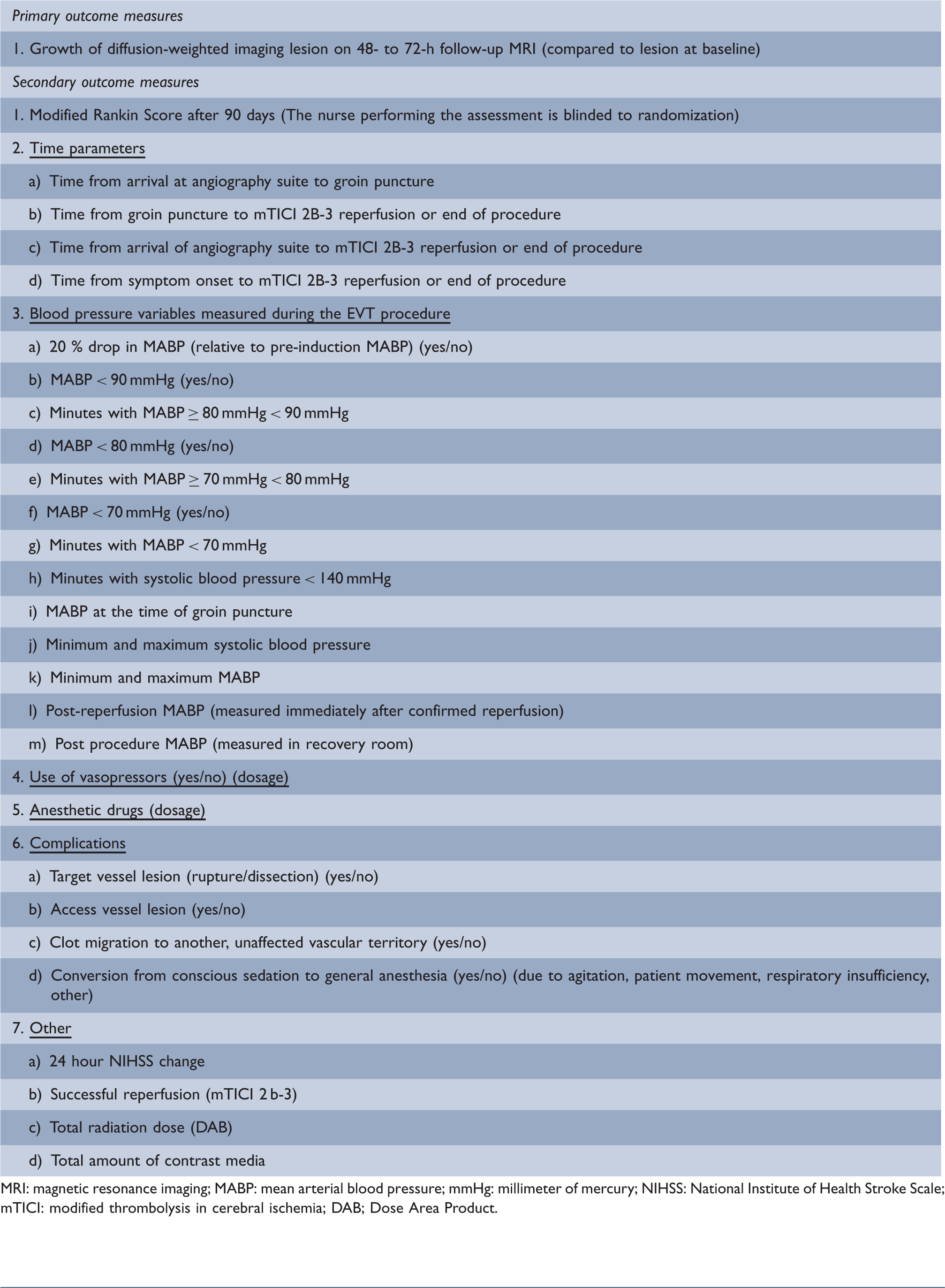
MRI: magnetic resonance imaging; MABP: mean arterial blood pressure; mmHg: millimeter of mercury; NIHSS: National Institute of Health Stroke Scale; mTICI: modified thrombolysis in cerebral ischemia; DAB; Dose Area Product.
As an exploratory objective, we also aim to examine the association between mean arterial blood pressure (MABP) and mRS after EVT.
Methods
Design
GOLIATH is an investigator-initiated trial with a PROBE (prospective, randomized, open-label with blinded end-point evaluation) design. Patients will be randomized 1:1 to either GA or CS.
Patient population
Inclusion and exclusion criteria
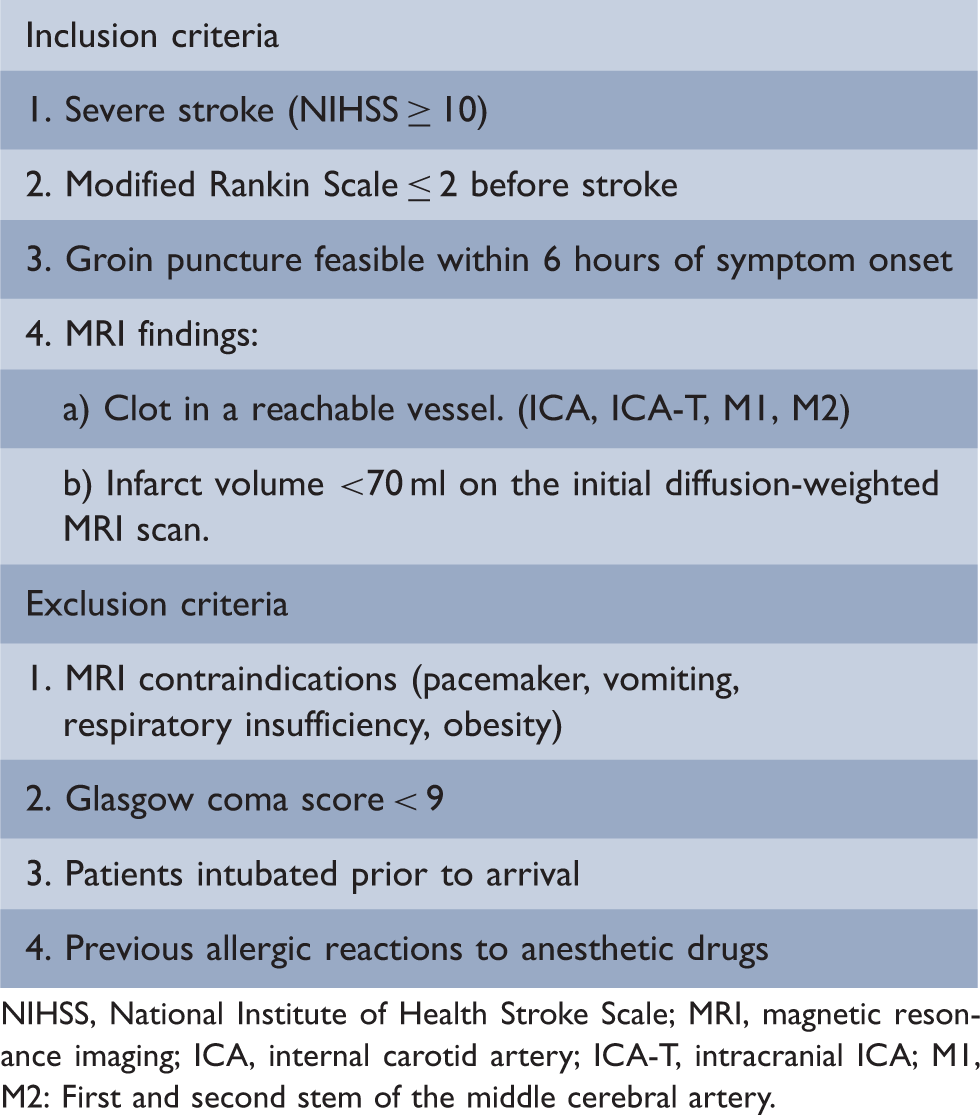
NIHSS, National Institute of Health Stroke Scale; MRI, magnetic resonance imaging; ICA, internal carotid artery; ICA-T, intracranial ICA; M1, M2: First and second stem of the middle cerebral artery.
Randomization
Randomization is performed by the investigator on-call via a web-based randomization program (Opus Consult ApS, Egaa, Denmark). Patient randomization is stratified for NIHSS (10–16 or ≥17) and age (18–65 or ≥66). Block randomization (with the sizes 4, 6 and 8) is performed after stratification. Allocation of block size is also random.
The study is acknowledged by the Ethical Committee as an acute study and consent is waived in the acute phase (record no. 1-10-72-356-14.)
Treatment and intervention
In the absence of contraindications, intravenous thrombolysis is started before EVT in all patients. Patients referred from a primary stroke center are typically admitted as “drip-and-ship” patients and MRI is done before EVT to delineate initial infarct volume. Patients fulfilling inclusion criteria are randomized and transferred directly to the neurointerventional suite. The study workflow is illustrated in Figure 1.
This is a flow chart of the patients’ way through the study.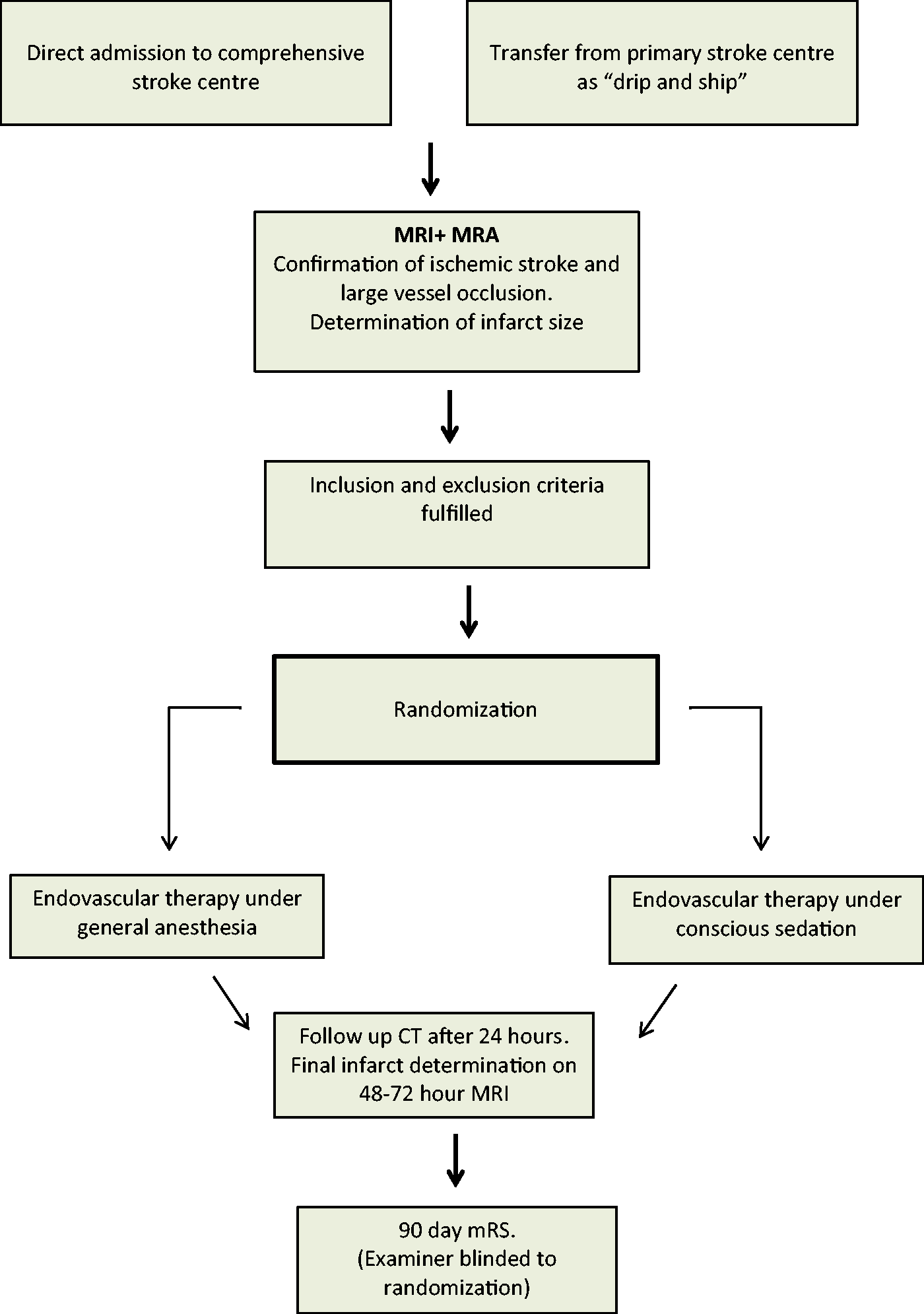
Monitoring
Electrocardiography, heart rate, pulse oximetry, end-tidal carbon dioxide and continuous invasive blood pressure measurements are performed during the procedure. In patients randomized to CS, oxygen is administered at a rate of 3–5 L/min and end-tidal carbon dioxide is monitored simultaneously via a combined nasal catheter. We aim to maintain MABP ≥ 70 mmHg 20 and systolic blood pressure ≥140 mmHg 15 during the procedure, in accordance with published guidelines. 21 A reduction in MABP and systolic blood pressure below the above-mentioned thresholds is immediately treated with vasopressors (ephedrine/phenylephrine). Blood pressure and dose of vasopressors are recorded.
Anesthesia protocol
General anesthesia: Rapid sequence intubation with suxamethonium (bolus: 0.5–1 mg/kg), alfentanil (bolus: 0.02–0.03 mg/kg), and propofol (bolus: 1–5 mg/kg followed by infusion of 2–10 mg/kg/h). Endotracheal intubation is followed by mechanical ventilation with attempted normoventilation. Anesthesia is maintained with propofol and remifentanil according to institutional guidelines. Dosage and infusion rate of anesthetic drugs are under the discretion of the anesthesiologist with consideration of age, the general condition of the patient, co-morbidity, blood pressure and requirements from the neurointerventionalist. In the rare case of a contraindication to propofol, sevoflurane will be used.
Conscious sedation: The overall goal is to reduce agitation, anxiety, and movements and still be able to communicate with the patient. Also, it is a goal to avoid that the patient converts to GA. All patients allocated to CS will receive the institutional sedation regime consisting of:
Fentanyl bolus 25–50 µg. This dose may be repeated. Propofol infusion. 1–2 mg/kg/h. If deemed necessary by the anesthesiologist, the infusion rate can be increased or reduced.
A nurse anesthetist and consultant anesthetist continually monitor the patient during the EVT procedure. Reasons for conversion from CS to GA may include patient movement, respiratory failure (due to hypoxia or inadequate ventilation), vomiting or seizures. Intra-procedural documentation is performed in the study case-report form by the consultant anesthetist attending the patient.
After the EVT procedure, the patient is monitored in the neurointensive care unit. The duration of stay is dependent on ABC criteria and neurological performance.
Data collection
The following data are collected on all enrolled patients:
Demographical data: Age, sex, hypertension, diabetes mellitus, smoking, ischemic heart disease, known congestive heart failure, and atrial fibrillation.
Stroke data: NIHSS, clot location (internal carotid at the neck, intracranial carotid, first or second branch of the middle cerebral artery) and side (left, right). Infarct volume before procedure (DWI), volume of perfusion lesion, microbleeds, leukoaraiosis (Fazekas Scale), reperfusion (modified Thrombolysis in Cerebral Infarction (mTICI)), infarct volume after 48–72 hours, hemorrhagic transformation (by ECASS definition), 24-h NIHSS and 90 day mRS. Evaluation of mRS at 90 days will be performed by a study nurse not involved in the trial and blinded to the anesthesia used.
Time-related data: Symptom onset/last seen well, time of admission, time of MRI scan, time to intravenous thrombolysis, time to arrival at angio-suite, time to groin puncture, time to endovascular reperfusion (mTICI ≥2B), time to end of procedure.
Anesthetic and physiological data are recorded on a case report form and subsequently entered into the study database.
Imaging data: The MRI scans acquired before treatment and 48–72 h after treatment will be analyzed by an independent neuroradiologist (AJY) unaware of the anesthesia the patients received. Infarct volume will be delineated on the DWI scans. “Growth” is defined as DWI volume after the procedure minus DWI volume prior to the procedure. In case of deterioration before the 48- to 72-h scan, we will use the last available scan, including CT. Hemorrhage will be included in the final infarct.
Data monitoring body
The study is not monitored by an external monitoring body. Permissions prior to initialization of the study are obtained from the Danish Data Protection Agency (record no. 1-16-02-647-14) and the Regional Ethical Committee.
Data management
All study data are entered into a study-specific database by the investigators.
Sample size estimates
A power analysis yielded a sample size of n = 98 in order to detect a 10 ml mean difference (standard deviation 25 ml, alpha 0.05 and power of 0.8) in the growth of infarcted tissue between the GA and the LA group, respectively. To account for scans with possible bad quality, missing scans or withdrawal of consent, we will include an additional 30% leading to a total sample size of 128 patients.
Statistical analyses
The primary analysis will be performed unadjusted and according to the intention-to-treat principle. This means that a cross-over patient from CS to GA will stay in the CS group for analysis. Data will be analyzed using conventional appropriate test statistics stratified according to NIHSS and age depending on the distribution of the individual outcome parameters (including paired t-test or Wilcoxon signed rank test for infarct volume and Mann–Whitney for mRS). Supplementary analyses using multivariable regression will be done in order to account for any imbalances in the distribution of prognostic factors between the two treatment arms. A generalized linear mixed model will be used for comparing infarct growth in the two treatment arms. Ordinal and logistic regression will be used for comparing 90 days mRS. Univariate (p < 0.10) predictors of infarct growth and 90 days mRS, respectively, will be included in the supplementary multivariable analyses.
The association between MABP and mRS will be examined using multivariable polynomial regression.
Statistical significance is defined as a two-tailed p < 0.05.
Study organization and funding
The study is investigator-initiated and investigator led. The study is financed by departmental sources of funding from Aarhus University Hospital.
Ethics
Since there are no national or international guidelines as to whether GA or CS should be offered in this situation and since the focus of the study is to test two different anesthesia procedures that are currently used in clinical practice and not investigational drugs, we do not find it necessary to obtain consent from patient or relatives prior to EVT. We are randomizing without consent, which is permitted under Danish law if the patient as a rule is unable to give consent and the treatment is time sensitive. Since the majority of the patients are incapacitated at admission and since the treatment effect is severely time dependent, 22 we found that the conditions for exemption from informed consent are fulfilled. The study is approved by the Ethical Committee of Central Denmark Region.
After the procedure, we are required to obtain consent for keeping the data in the database. The patient will be presented with a consent form with information about the study. If the patient is in a state where we cannot obtain consent, consent will be obtained from next of kin and the primary care physician. (Obligation in Danish law.)
Discussion
The choice of anesthetic regime for EVT in patients with AIS varies among endovascular centers. Current practice is largely based on local protocols and preferences of the neurointerventionalists and anesthesiologists. In our institution, we use CS for co-operative patients and GA for severely agitated or unresponsive patients. Retrospective studies all suggest that CS is associated with a better outcome.10–13 Despite the lack of prospective data, the Society for Neuroscience in Anesthesiology and Critical Care has published a consensus paper on anesthetic management of patients undergoing EVT for AIS. 21 Based on analysis of retrospective studies, they recommend that “the choice of anesthetic technique and pharmacological agents should be individualized based on clinical characteristics of each patient, in close communication with the neurointerventionalist.” Thus, randomized data are needed to determine the optimal anesthetic regime during EVT. GOLIATH is a randomized trial with the aim to determine whether anesthetic management during EVT for AIS may influence outcome. Outcome measures include infarct growth, clinical outcome, and several important physiological and anesthetic parameters.
This area is of clinical importance as highlighted by other prospective studies which are on the way. In a recent paper, Schönenberger et al. presented the SIESTA (Sedation vs. Intubation for Endovascular Stroke TreAtment.) protocol with a similar prospective, randomized design. 23 The primary endpoint in SIESTA is 24-h neurological improvement determined by a change in NIHSS. By looking at infarct growth as a surrogate outcome, we hope to have a more sensitive marker of outcome. We also determine 90-day mRS as secondary outcome measure. We are aware, however, that many factors may influence the 90-day functional outcome, most of which we are able to adjust for. The final outcome after AIS is determined by the combination of optimal pre-hospital, in-hospital, and rehabilitation management.
GOLIATH aims to present data concerning type and dosage of anesthetics in addition to peri-procedural blood pressure data and whether changes in blood pressure may be related to outcome. One previous study has reported type and dosage of anesthetics used during the EVT procedure. 16 In addition, a limited number of studies have reported data concerning peri-procedural changes in blood pressure.15,18 Anesthetics influence hemodynamics and periods with low blood pressure may be associated with worse outcome, as previously reported in patients subjected to GA.15–18
Time to groin puncture could differ in the two groups, giving GA patients a disadvantage. On the other hand, treatment time could be longer in the CS group. If a difference in infarct size is found between the two groups, we will examine if this can be explained by factors such as differences in time parameters or blood pressure, or it has to be attributed to anesthesia itself.
Summary and conclusion
Observational studies indicate that GA is associated with worse outcome in patients undergoing EVT for AIS. GOLIATH is a randomized trial with the aim to examine whether the choice of GA or CS during EVT influences infarct growth and patient outcome.
Footnotes
Authors’ contribution
All authors contributed to the writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Albert J Yoo received research grant from Penumbra Inc. and Neuravi Inc.