
Abstract
Background
Multiple acute cerebral infarcts in different arterial territories may be caused by several emboli concurrently or successively.
Aim and/or hypothesis
We hypothesized that the time from stroke onset to magnetic resonance imaging may shed light on underlying mechanisms of multiple acute cerebral infarcts.
Methods
This is a prospective observational cohort study involving 2697 ischemic stroke patients conducted at Haukeland University Hospital between February 2006 and October 2013. Only patients with diffusion-weighted imaging lesions in more than one arterial territory (left or right anterior circulation or posterior circulation) were included. The time from stroke onset to magnetic resonance imaging was registered and correlated with the etiology of multiple acute cerebral infarcts in each patient.
Results
We reviewed 2697 consecutive patients and 2220 (82%) underwent magnetic resonance imaging. Among these 2125 (96%) had diffusion-weighted imaging lesions. We found 187 multiple acute cerebral infarct patients who were then included in the study. There was positive correlation (0.20; p < .001) between time to magnetic resonance imaging and frequency of multiple acute cerebral infarcts caused by internal carotid stenosis. There was no correlation (−.02) between time to magnetic resonance imaging and frequency of multiple acute cerebral infarcts caused by cardiogenic embolism.
Conclusions
Multiple acute cerebral infarcts associated with cardiogenic embolism seem to happen concurrently as a shower of emboli whereas multiple acute cerebral infarcts associated with internal carotid artery stenosis seem to occur successively separated by hours or days.
Keywords
Introduction
Approximately 10% of stroke patients have multiple acute cerebral infarcts (MACI) in different arterial territories defined as left or right anterior circulation or posterior circulation.1–4 Cardiogenic embolism (CE) and large artery atherosclerosis (LAA) presenting as internal carotid artery stenosis (ICAS) are the main stroke subtypes in acute embolic cerebral infarcts. 5 Several pathological mechanisms may underlie MACI, but CE and both symptomatic and clinically asymptomatic ICAS are the most frequent causes.4,6 In patients with bilateral ICAS, the source of bilateral cerebral infarcts may be both hypoperfusion and embolism which may coexist and interfere with each other. 7
MACI may be caused by several emboli concurrently as a shower of emboli or successively as emboli separated by hours or days. 3 Diffusion-weighted magnetic resonance imaging (DWI) is the best way to assess MACI and distinguish acute and old ischemic lesions.8,9 Even though most patients with acute cerebral infarct are admitted within 24 h of onset, some patients are admitted several days after. In our department, magnetic resonance imaging (MRI) is performed in most patients normally within the first 24 h after admission, but sometimes delay occurs. These unavoidable time shifts in MRI may help to clarify the cause underlying MACI.
Aims and/or hypothesis
If MACI is caused by successive and independent emboli, the frequency of MACI would be expected to increase with time between stroke onset and MRI, in a stepwise time pattern. Contrarily, if MACI is caused by concurrent release of emboli, the frequency of MACI would be expected to be independent of MRI delay, in a simultaneous time pattern. The aim of our study was to determine whether the ICAS likely causes MACI successively and independently whereas CE occurs concurrently.
Methods
We retrospectively analyzed the data from a prospective observational study conducted at the Centre for Neurovascular Diseases, Department of Neurology, Haukeland University Hospital between February 2006 and October 2013. All consecutive patients with acute ischemic stroke (the index stroke) were prospectively registered in The Bergen NORSTROKE Registry.
Ischemic stroke was defined in accordance with the Baltimore–Washington Cooperative Young Stroke Study Criteria comprising neurological deficits lasting more than 24 h because of ischemic lesions or transient ischemic attacks where computer tomography (CT) or MRI showed infarctions related to the clinical findings. 10 National Institutes of Health Stroke Scale scores were registered at admission as an indicator of stroke severity.
Etiology was determined by the Trial of Org 10172 in Acute Stroke Treatment classification (TOAST) and classified as LAA, CE, small vessel disease, other cause, and undetermined source (US). 11 LAA was defined as symptomatic stenosis ≥50% in the proximal internal carotid artery, vertebral artery, or basilar artery due to atherosclerosis and no competing etiology including no cardiac disease.
MACIs in different arterial territories were defined as acute infarcts in at least two of the following arterial territories: left or right anterior circulation or posterior circulation based on DWI.
Etiologic investigations encompassed routine blood tests, ECG, cerebral CT and MRI, carotid Duplex sonography, Holter monitoring, and transthoracic or transesophageal echocardiography.
All stroke patients underwent CT immediately after admission to the hospital. As a rule, MRI was performed in every patient with acute cerebral infarct unless there were contraindications such as pacemaker, claustrophobia, none consenting, or unstable patient. DWI was performed as part of a routine MRI protocol for stroke patients on a 1.5 Tesla Siemens Magnetom (Symphony). The DWI sequence used was ep2d_diff_3scan_trace, with the following specifications of parameters: field of view 230 mm, slice thickness 5 mm, repetition time (TR) 3200 ms, time to echo (TE) 94 ms. All CT and MRI scans were reviewed by a neurologist (HN) with long CT and MRI experience.
Angina pectoris, myocardial infarction, intermittent claudication, hypertension, diabetes mellitus on glucose lowering diet or medication, hypercholesterolemia, and smoking were considered as vascular risk factors.
We used Phillips software, integrated in Philips IU 22 ultrasound system to determine ICAS and its degree. Two-dimensional B-mode and color flow Doppler ultrasound were performed. The percentage of area reduction was assessed, and morphological features of stenosis and changes of hemodynamics were evaluated. ICAS was defined as proximal ICAS >50% or occlusion based on duplex sonography. ICAS >50% were considered asymptomatic if there were no related symptoms even if there were ipsilateral DWI lesions.
Atrial fibrillation (AF) was categorized as paroxysmal or chronical. Newly diagnosed AF or AF diagnosed before admission was noted or confirmed by ECG or Holter monitoring during hospital stay.
MACIs were defined as at least two noncontiguous high intense DWI lesions in at least two different arterial territories (left or right anterior circulation or posterior circulation). Ischemic strokes were classified as lacunar when the diameter was less than 15 mm and in the distribution of deep penetrating arteries located subcortically or in the brainstem. Ischemic strokes were classified as nonlacunar if the size was more than 15 mm in diameter. T2-weighted hypointense signals in the periventricular white matter were considered as leukoaraiosis.
The exact time from stroke onset to MRI was registered. Lesions were considered as acute if we found hyperintense signals on DWI, hypointense signals on ADC, and normal or slightly increased signals on corresponding T2 series. 12
The study was approved by the local ethics committee (REK Vest).
Statistics
We used chi-square test for categorical variables and Student’s t-test for the continuous variables when appropriate. Linear prediction was used for estimation of future frequencies of MACI in relation to time to MRI. STATA 14.0 (StataCorp, College Station, Texas, USA) was used for analyses.
Results
In total, 2697 patients had acute stroke. MRI was performed in 2220 (82%) and among these 2125 (96%) had DWI lesions. MACIs were detected in 187 (8.8%) patients.
Frequency of multiple acute cerebral infarcts, shown by diffusion-weighted magnetic resonance imaging within different etiologic groups according to the TOAST criteria and internal carotid artery stenosis (ICAS)
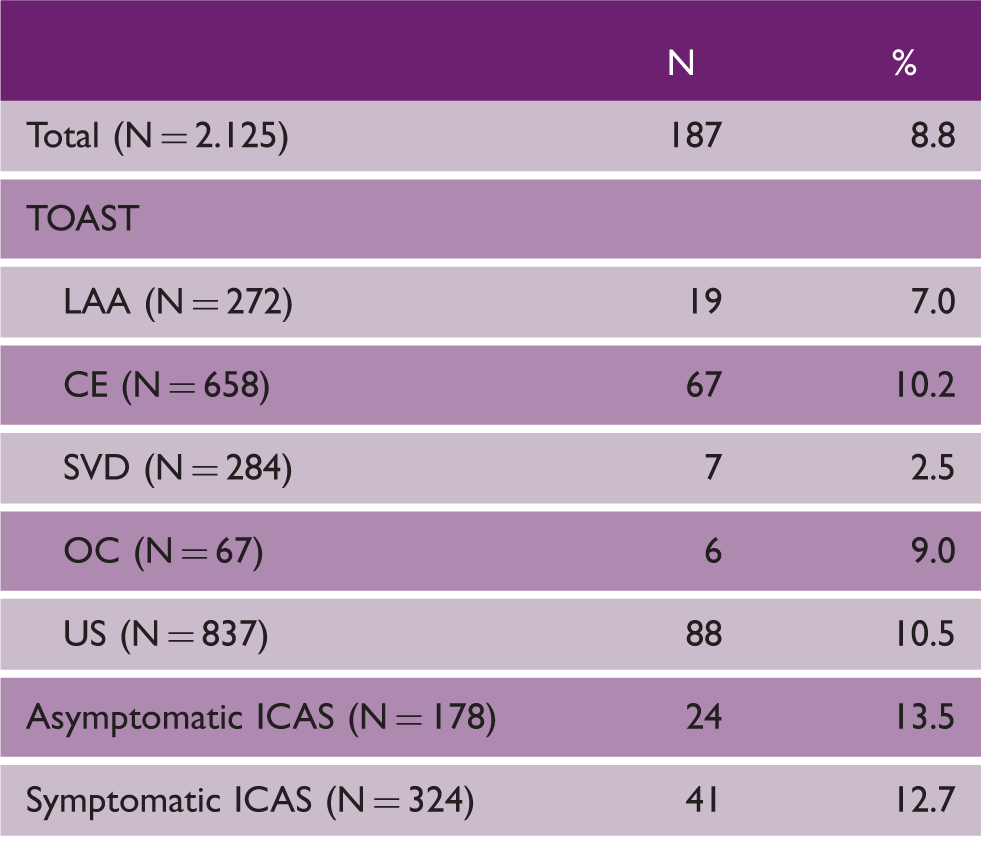
CE: cardiogenic embolism; LAA: large artery atherosclerosis; OC: other cause; SVD: small vessel disease; US: undetermined cause.
MRI investigations were mostly performed within the first 48 h after stroke onset (Figure 1). The average mean time from stroke onset to MRI was 2.3 days (SD = 2.6 days) in the whole DWI group (N = 2125), 2.5 days (SD = 2.6 days) in the MACI group, and 2.3 days (SD = 2.6 days) in the non-MACI group.
Distribution of time to magnetic resonance imaging in relation to stroke onset for 2125 patients with acute ischemic stroke.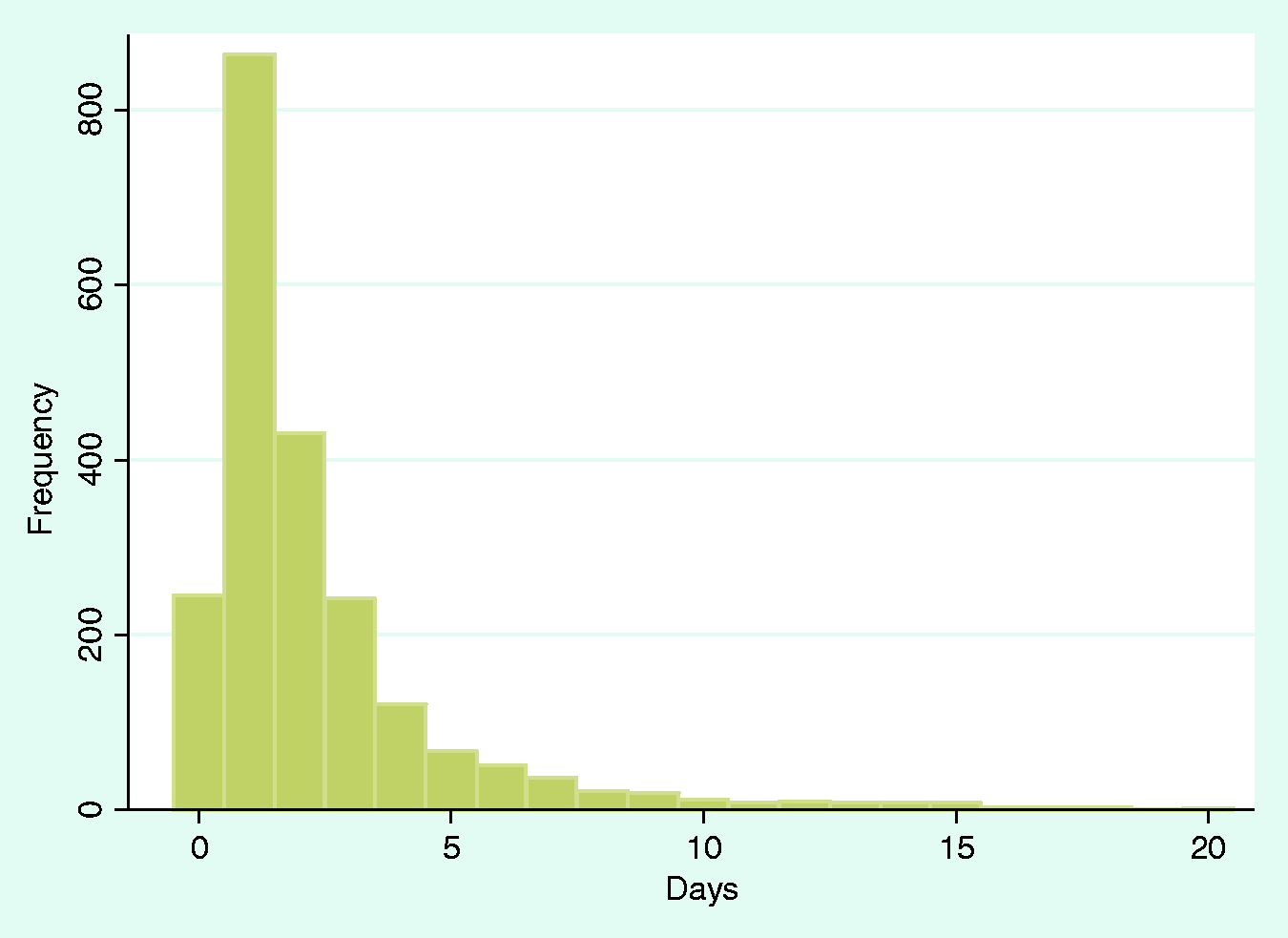
Correlation between time to magnetic resonance imaging and multiple acute cerebral infarcts in different circulations
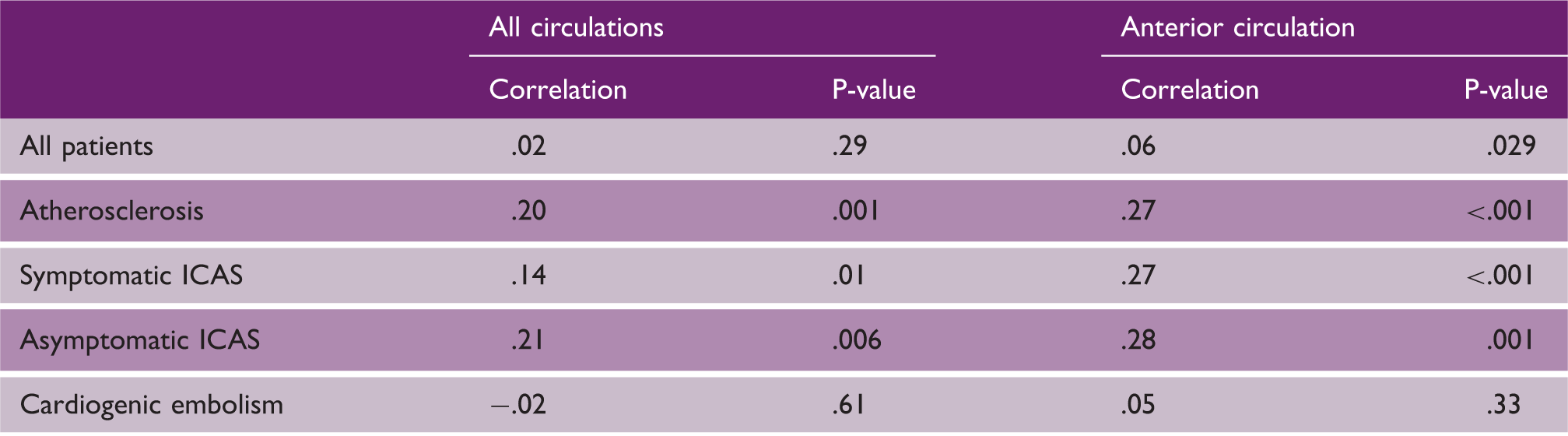
ICAS: internal carotid artery stenosis.
Time patterns in all studied etiology groups are displayed in Figure 2(a) to (d) as a linear model of prediction with confidence intervals.
(a) Linear prediction model of multiple acute cerebral infarcts frequency due to cardiogenic embolism in relation to time to magnetic resonance imaging; (b) linear prediction model of multiple acute cerebral infarcts frequency due to large artery atherosclerosis in relation to time to magnetic resonance imaging; (c) linear prediction model of multiple acute cerebral infarcts frequency in patients with symptomatic internal carotid artery stenosis; (d) linear prediction model of multiple acute cerebral infarcts frequency in patients with asymptomatic internal carotid artery stenosis. axis X: number of days to magnetic resonance imaging from symptom onset; axis Y: fraction of patients with reccurent cerebral infarcts; CI: confidence interval.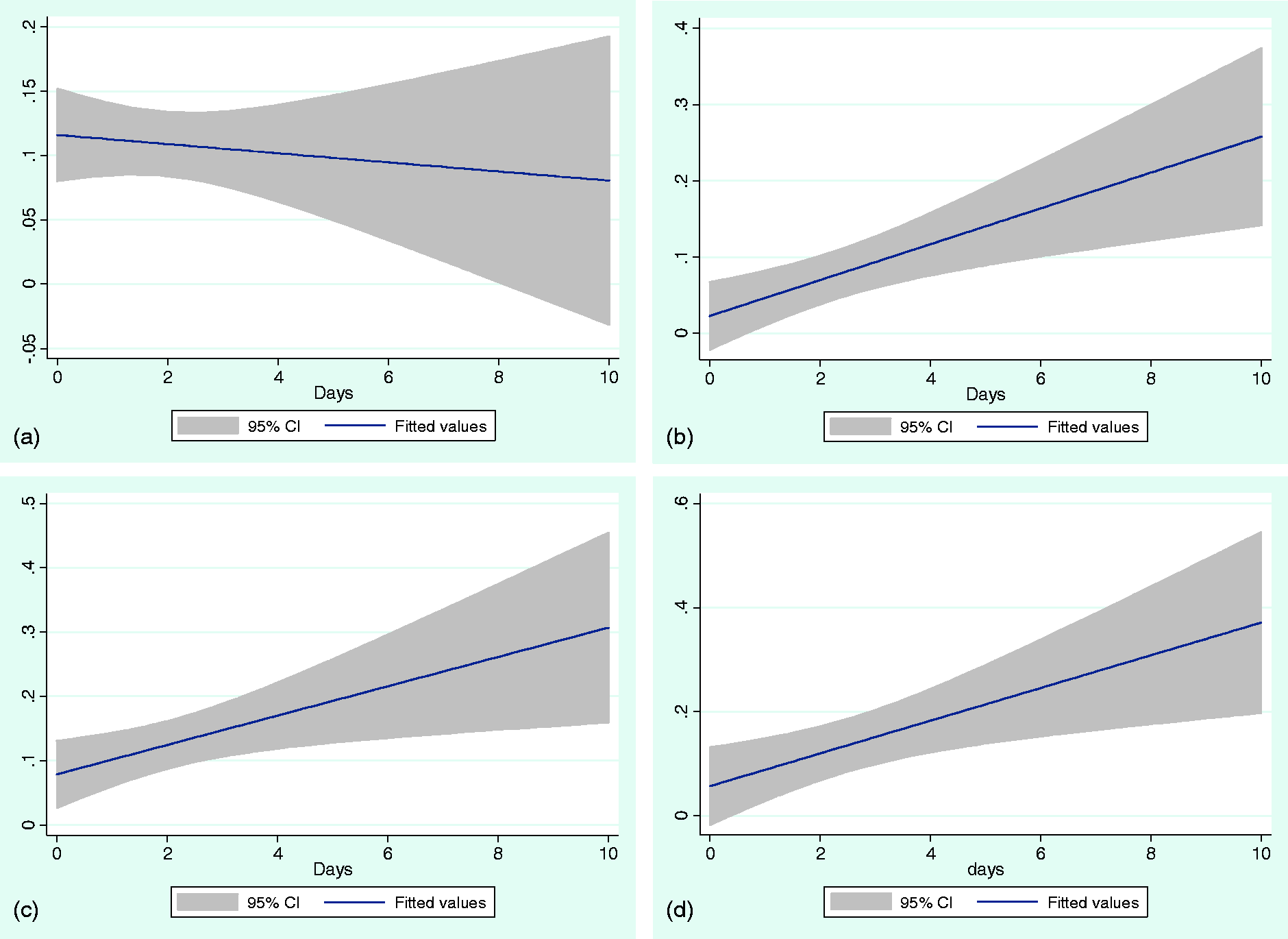
Acute cerebral infarcts in both anterior circulations associated with internal carotid stenosis (P < .001); N = 93. Frequencies of symptomatic and asymptomatic internal carotid stenoses in patients with infarcts in both anterior circulations
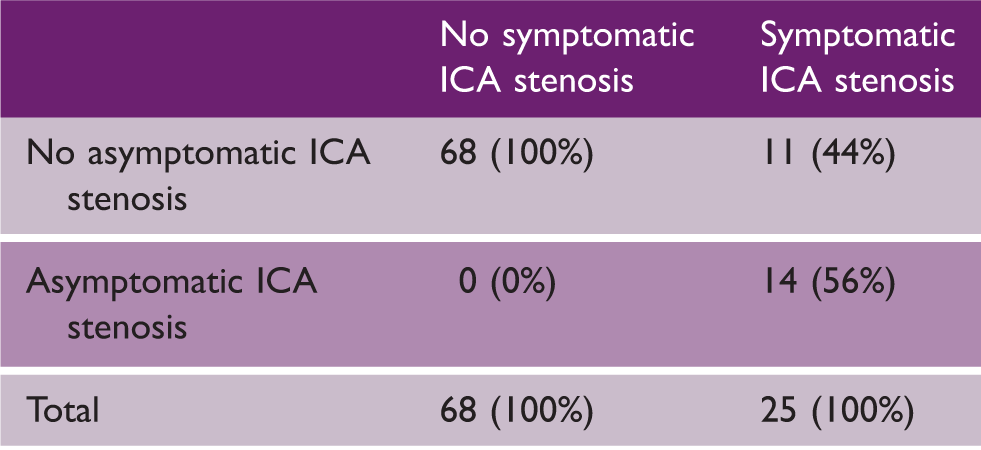
ICAS: internal carotid artery stenosis.
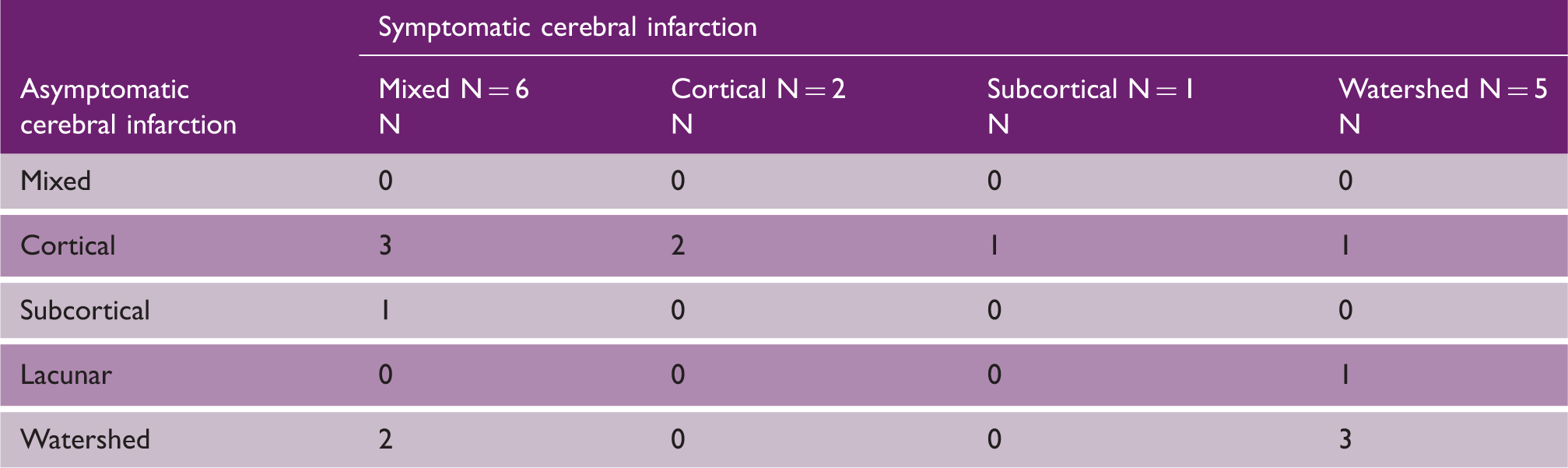
Patients with acute cerebral infarctions in both middle cerebral artery territories and bilateral internal carotid artery stenosis >50% (N = 14)
Discussion
We found no correlation between time to MRI and the frequency of MACI in different arterial territories (left or right anterior circulations or posterior circulation) when the etiology was identified as CE (Figure 2(a)). This indicates that patients with CE usually suffer from two or more emboli released concurrently or nearly concurrently. It seems likely that in these patients, a thrombus is released from the atrium, fragmentizes and causes infarcts in different arterial territories. Our findings suggest that the risk of subsequent emboli from the heart is low, at least within the first 10 days of stroke onset. This would be in line with negative findings concerning effects of early anticoagulation (HAEST study, other Heparin-/Fragmin-/other anticoagulation studies). 13
As opposed to CE, an increased frequency of MACI due to LAA was associated with time to MRI (Figure 2(b)). A similar time pattern was found among patients with symptomatic and asymptomatic ICAS (Figure 2(c) and (d)). Interestingly, all patients with acute cerebral infarcts in both anterior circulations and one asymptomatic ICAS also had symptomatic ICAS (Table 3). A plausible interpretation is that MACIs in patients with bilateral ICAS are caused by successive emboli. Likely, both ICAS are unstable. Increased shear stress in the stenotic part of ICAS forms platelet-rich clots which are small in size and relatively fragile. 14 Shear stress likely contributes to repetitive detachment of these thrombi and subsequent MACI in a stepwise time pattern. Moreover, increasing degree of ICAS is associated with a higher number of DWI lesions. MACIs are more common in patients with high-degree ICAS. 15 Therefore, microemboli detection by transcranial Doppler ultrasound most likely is an appropriate examination for consideration of more aggressive antiplatelet therapy in these patients. 16 If simultaneous acute cerebral infarcts in both anterior circulations are caused by ICAS, anatomical variations like unpaired ACA or cross-flow mechanism should be considered. 17 Hypoperfusion, suggesting no association between MACI and time to MRI, seems to be a less likely mechanism.
MACI patients have generally worse clinical outcome and functional recovery. 18 Therefore, proper DWI evaluation is important as a part of initial investigation and improves accuracy in diagnostics of MACI. Both lacunar and cortical MACI may present with a clinical picture of a single lesion. MACI may then be easily overlooked and classified as a single lesion infarct if a systematic DWI analysis is not done.19,20 The knowledge of time patterns in the development of MACI may help to determine etiologies of MACI and prevent recurrent infarcts which subsequently improve health outcome and reduce treatment costs in future. 21
Our study has some limitations. We did not conduct long-term ECG monitoring for more than 24 h which may have underdiagnosed the final number of AF. Serial implantations of loop recorders should be considered in selected patients. 22 It is possible that different cardiac disorders are associated with different risks of MACI. This should be addressed in future studies. In addition, diagnostic algorithm for embolic strokes of undetermined source recently published by Hart et al. 23 should be applied in all stroke patients.
In conclusion, the time pattern between two major groups of MACI sources differs. CE is not associated with time to MRI and occurs in most cases simultaneously, whereas LAA is associated with time to MRI fitting a stepwise time pattern. Correct and proper determination of MACI origin is crucial. As a result, tailored therapeutic strategies will prevent recurrent ischemic stroke in patients with MACI.
Footnotes
Acknowledgement
We gratefully acknowledge study nurse Maren Inselseth for study administration.
Authors’ contributions
VN interpreted the data, performed DWI analysis, substantially contributed on the study conception, and drafted the manuscript. ANK performed DWI analysis and contributed on the study conception. UW-A contributed on data collection and provided critical revisions of the manuscript. LT provided critical revisions of the manuscript. HN performed the statistical analysis, substantially contributed on the study conception, data collection, and did final revision of the manuscript. All authors read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.