
Abstract
Background
Physical, psychological, and/or social impairment can result after a stroke and can be exacerbated by pain. One type of pain after stroke, central poststroke pain, is believed to be due to primary central nervous system mechanisms. Estimated prevalence of central poststroke pain ranges widely from 8% to 55% of stroke patients, suggesting a difficulty in reliably, accurately, and consistently identifying central poststroke pain. This may be due to the absence of a generally accepted definition.
Aim
We aimed to clarify the role of thalamic strokes and damage to the spinothalamic pathway in central poststroke pain patients. Also, we aimed to gain a current understanding of anatomic substrates, brain imaging, and treatment of central poststroke pain.
Summary of review
Two independent reviewers identified 10,144 publications. Based on Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines, we extracted data from 23 papers and categorized the articles’ aims into four sections: somatosensory deficits, pathway stimulation, clinical trials, and brain imaging.
Conclusions
Our systematic review suggests that damage to the spinothalamic pathway is associated with central poststroke pain and this link could provide insights into mechanisms and treatment. Moreover, historical connection of strokes in the thalamic region of the brain and central poststroke pain should be reevaluated as many studies noted that strokes in other regions of the brain have high occurrence of central poststroke pain as well.
Keywords
Introduction
Stroke often leaves an individual with residual physical, psychological, and/or social impairment, which may compromise one’s capacity to carry out activities of daily living. 1 These impairments can result from pain after a stroke that is categorized as either poststroke pain (PSP) triggered by peripheral/mechanisms, or central poststroke pain (CPSP) due to primary central nervous system (CNS) mechanisms.2–4 Also, CPSP can have an effect on quality of life (QoL) without there being any disability or impairment from the stroke. Prevalence of CPSP among stroke patients has been found to range widely from 8% to 55%. 1 This variability suggests a difficulty in reliably identifying CPSP, in part due to the numerous types of pain that can be exhibited, including sensory deficits of thermal, tactile, and/or pinprick experiences of pain. 1 Further complicating its diagnosis, CPSP currently lacks a universal definition. 5 Clarifying the relationship between CPSP with strokes located in the thalamic region and damage to the spinothalamic pathway (STP) may help provide the groundwork for creating a universal definition and constructing an effective treatment plan.
Lesion location and affected neural pathways have been at the cornerstone of multiple theories concerning the underlying etiology of CPSP. The foundation of the disinhibition theory states that CPSP is only related to thalamic strokes.
6
Formally referred to by Dejerine and Roussy
6
as thalamic pain, more than 100 years ago, patients who had strokes affecting their thalamic region were the ones having pain after their stroke (Figure 1). Autopsies were performed on five patients who complained of pain after stroke in the thalamic region.6,7 Figure 1 illustrates the evolution of identifying CPSP and how in the late 1950s two new theories were developed. One theory following Dejerine and Roussy’s findings and another (central imbalance theory (CIT)) stating that the primary cause of CPSP is by damage to the STP. The CIT acknowledges that there could be alternative affected pathways that may cause CPSP (e.g. medial lemniscus pathway, posterior column-medial lemniscus pathway). Despite the introduction of this new theory, research has largely focused on the relationship between strokes in the thalamic region and CPSP.
Evolution of classifying CPSP.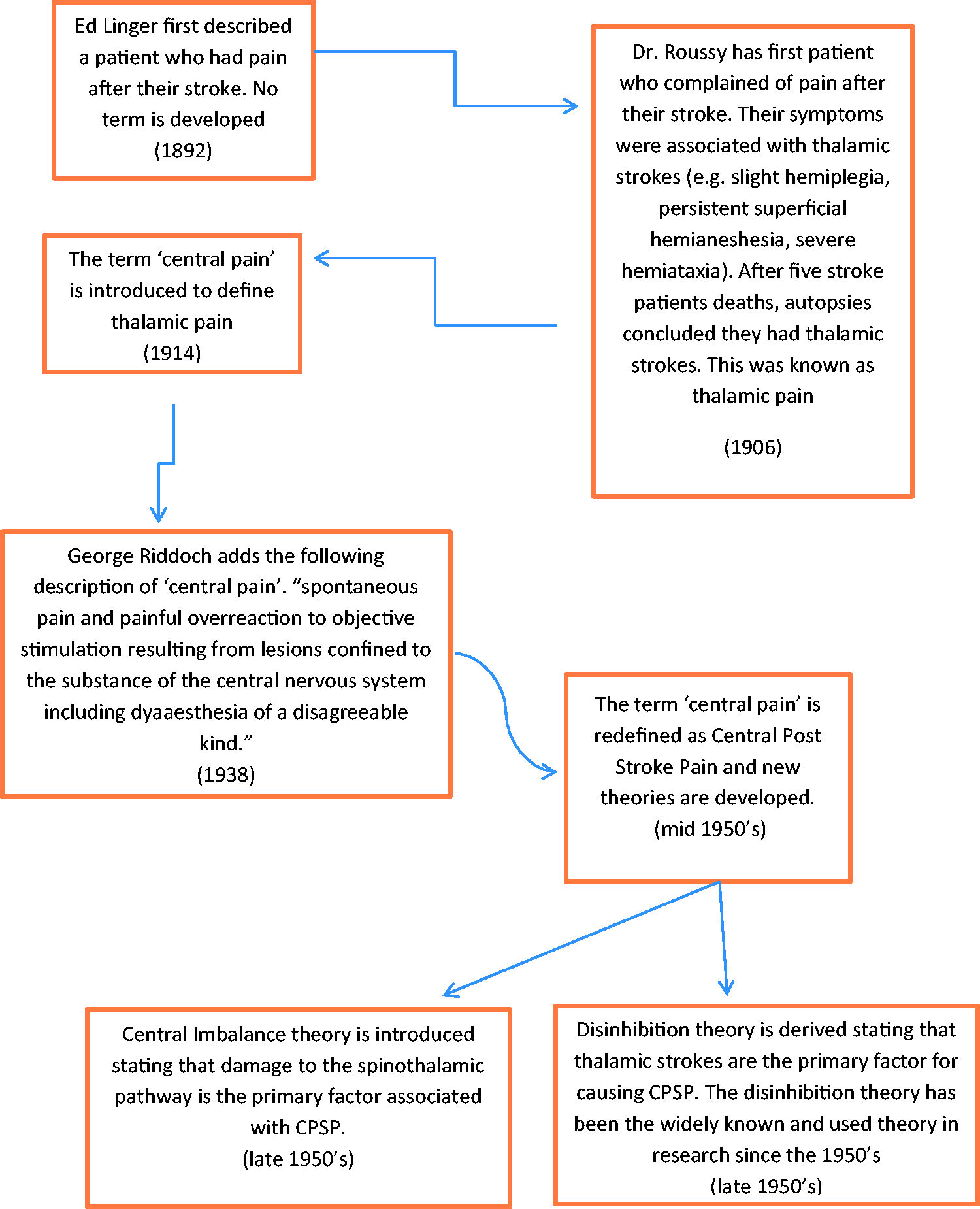
Differences in clinical presentation, brain imaging, and specific pathway lesions have made it challenging to treat patients with CPSP.5,9,10 To address the discrepancies in the literature, this systematic review will help the reader gain a great understanding of CPSP, while also constructing a more coherent understanding of the role of thalamic strokes and damage to the STP in patients with CPSP. Also, it builds upon the current understanding of anatomic substrates and brain imaging studies related to CPSP. Reviewing the current literature may also help to gain a greater understanding of why CPSP does not improve over time, but rather worsens. Also, this paper addresses evidence-based results of clinical trials, including randomized controlled trials (RCTs).
Methods
Search strategy
Eligibility assessment was performed independently and in a standardized manner by two reviewers (JS and ES) blinded to one another review. A third reviewer (AC) resolved any disagreements. When developing the search strategy, we consulted with a professional information scientist at SUNY Downstate library to generate the search terms and databases we should utilize. We searched the PubMed, CINAHL, and Web of Science databases starting on 11 January 2016 using keywords “pain,” “physical pain,” “psychological pain,” “mental pain,” or “poststroke pain” in combination with the medical subject headings, “brain stem infarction,” “infarction, anterior cerebral artery,” “infarction, middle cerebral artery,” “cerebral hemorrhages,” ‘intracranial hemorrhages,” “thalamic,” “putaminal hemorrhages,” “basal ganglia hemorrhages,” “cerebral vascular disorders,” “intracranial hemorrhage, hypertensive,” “infarction, basilar artery,” or “infarction brain stem.” We applied language limitations (English only).
Eligibility criteria
We included only original, clinical studies, and RCTs. The studies had to assess CPSP, using a single question or pain scale. The studies needed a sample size of at least 10 patients with either hemorrhagic or ischemic strokes.
Studies were excluded if they (i) examined animals, (ii) lacked primary data (e.g. editorials, review articles, or protocol papers), (iii) investigated peripheral PSP (e.g. shoulder pain, arm pain), (iv) were not published in a peer reviewed journal, (v) were retrospective studies, and (iv) or examined individuals under 18 years old.
Results
The initial search yielded 1074 articles, removal of duplicates resulted in 731 selected articles. Two other articles were added from reference sections of other papers. All article titles and abstracts were screened resulting in 111 relevant studies. After reading the full articles, 88 articles were excluded (28 retrospective studies, and 60 that only measured PSP). Thus, 23 papers met our criteria and were included in the review (Figure 2, Preferred Reported Items for Systematic Reviews and Meta-Analyses (PRISMA)). We extracted data from 23 articles and categorized the articles’ aims into four sections: somatosensory deficits (five studies), pathway stimulation (three studies), clinical trials (eight studies) and brain imaging (seven studies). The selected articles were published between 1988 and 2014.
PRISMA 2009 flow diagram.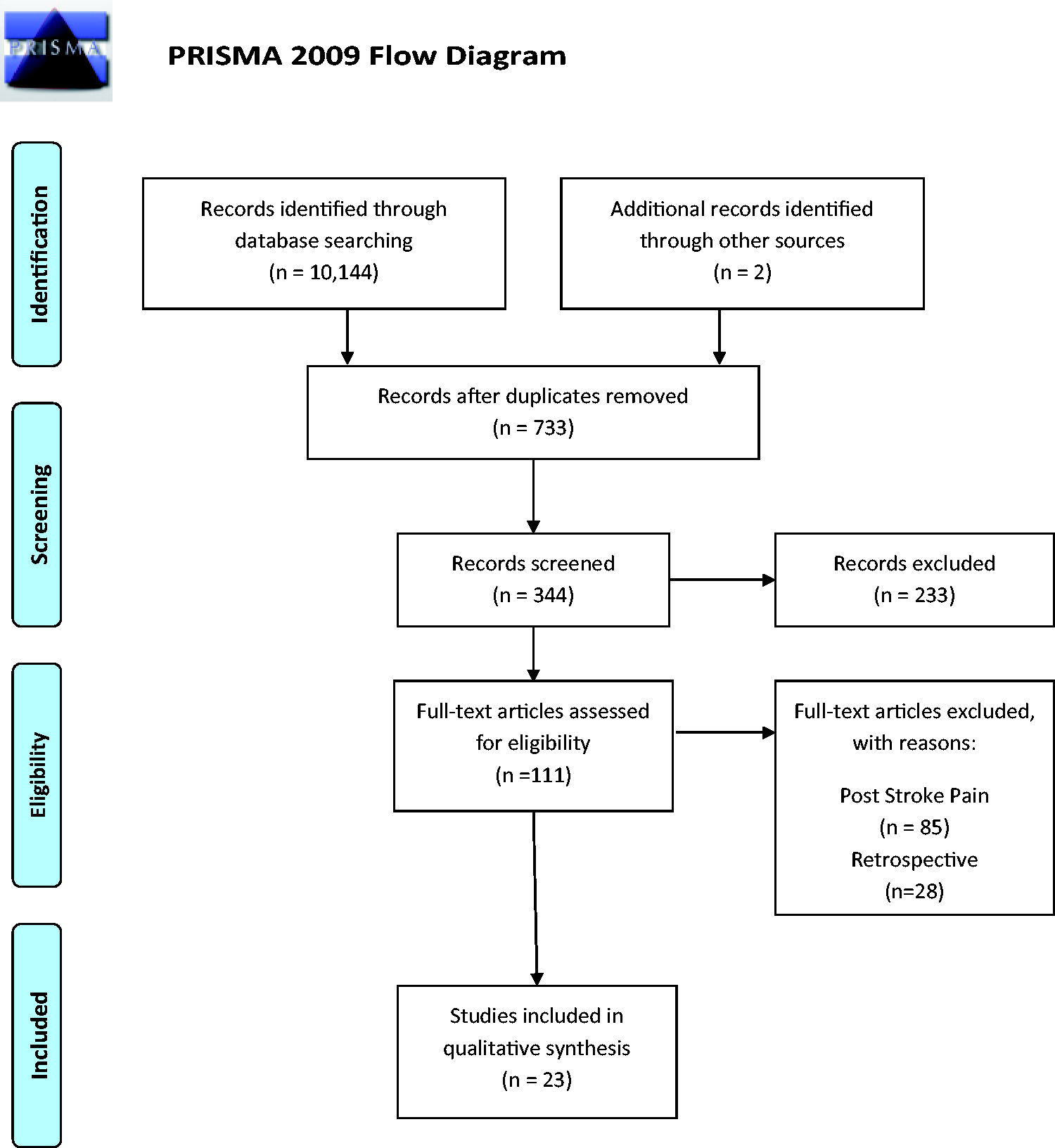
Somatosensory deficits
Studies accessing somatosensory deficits in CPSP (n = 5)
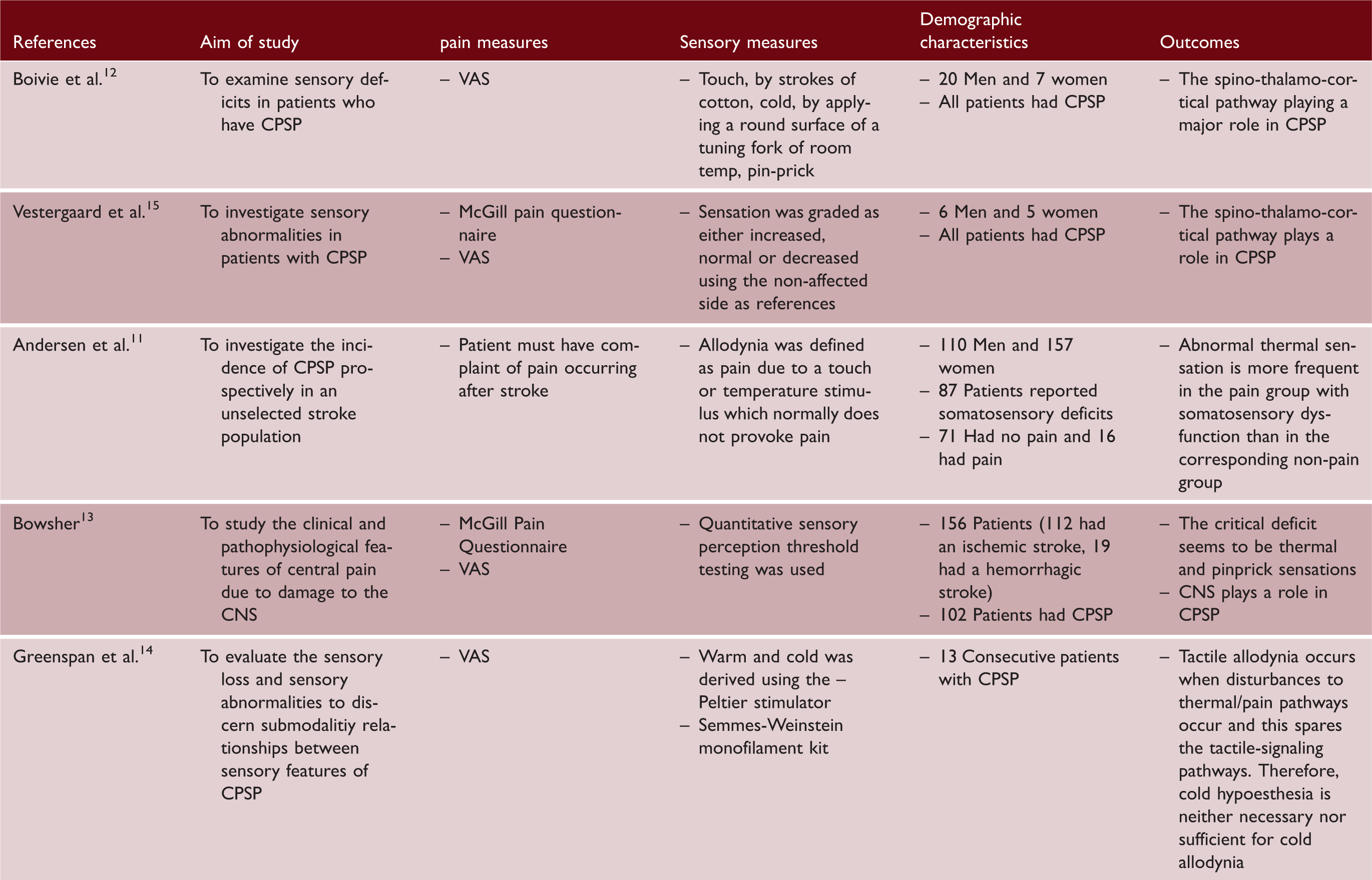
VAS: visual analogue scale; CPSP: central poststroke pain; CNS: central nervous system.
Tactile and thermal allodynia were investigated in all five studies using a sensory measure (see Table 1). When examining patients who have been diagnosed with CPSP, allodynia as a whole was found to range from 23% to 85% across studies. Tactile allodynia, including sensitivity to light or touch, was found to range from 5% to 55% in CPSP patients, with a mean of 40% across studies. Thermal allodynia was found to range from 15% to 56% with the mean of the five studies being 33%. The impact of allodynia on stroke patients has been addressed, 5 and the results from these studies show a wide range of prevalence of allodynia within CPSP. A number of factors may have contributed to the large variability in prevalence rates for reported throughout these studies, including the lack of a universal definition of CPSP and wide variations in sample sizes utilized across studies.
Table 1 outlines the prevalence of hyperalagesia (excessive pinprick, cold, and touch sensitivity) in all five studies.11–15 Four of the studies reported data on pinprick sensitivity. Three of these four studies found rates of pinprick sensitivity to be between 69% and 72% of CPSP patients. However, the remaining study found that only 6% of CPSP patients reported pinprick sensitivity. 13 Cold sensitivity was reported in all five of the studies and was found to range from 38% to 100%.11–15 Similar to allodynia, there was a large variability of hyperalagesia in CPSP patients. The same aforementioned reasoning for the large variability may apply to hyperalegesia, but hyperalgesia was found at a much higher rate than allodynia.
In an earlier review, 5 patients with CPSP were found to report allodynia more often, but from the results of the present review, there is compelling evidence that hyperesthesia is as likely and could possibly be more prevalent than allodynia. All five of these studies show high rates of some form of somatosensory deficit with CPSP patients; however, the underlying causes of these deficits are unclear. Most of the studies do not refer to location of the stroke as playing a role of these deficits, but the theme of the study’s findings were that pathways may play a role and future research is needed11,12,14,15 (Table 1).
STP
The STP’s importance to the development of CPSP has been highly debated and its role in the syndrome’s development is still poorly understood. 13 As mentioned above, the CIT states that impairment to STP is associated with pathogenesis of CPSP.12,13 Previous studies have shown that patients who have CPSP can have lesions outside the thalamic region.12–17 Moreover, the theory states that the development of CPSP is not determined by the location of the lesion within the brain; rather it is dependent on the impairment of the STP. Furthermore, even partial lesions affecting the STP lead to a higher risk of developing CPSP. 18
Studies accessing pathways in the brain (n = 3)
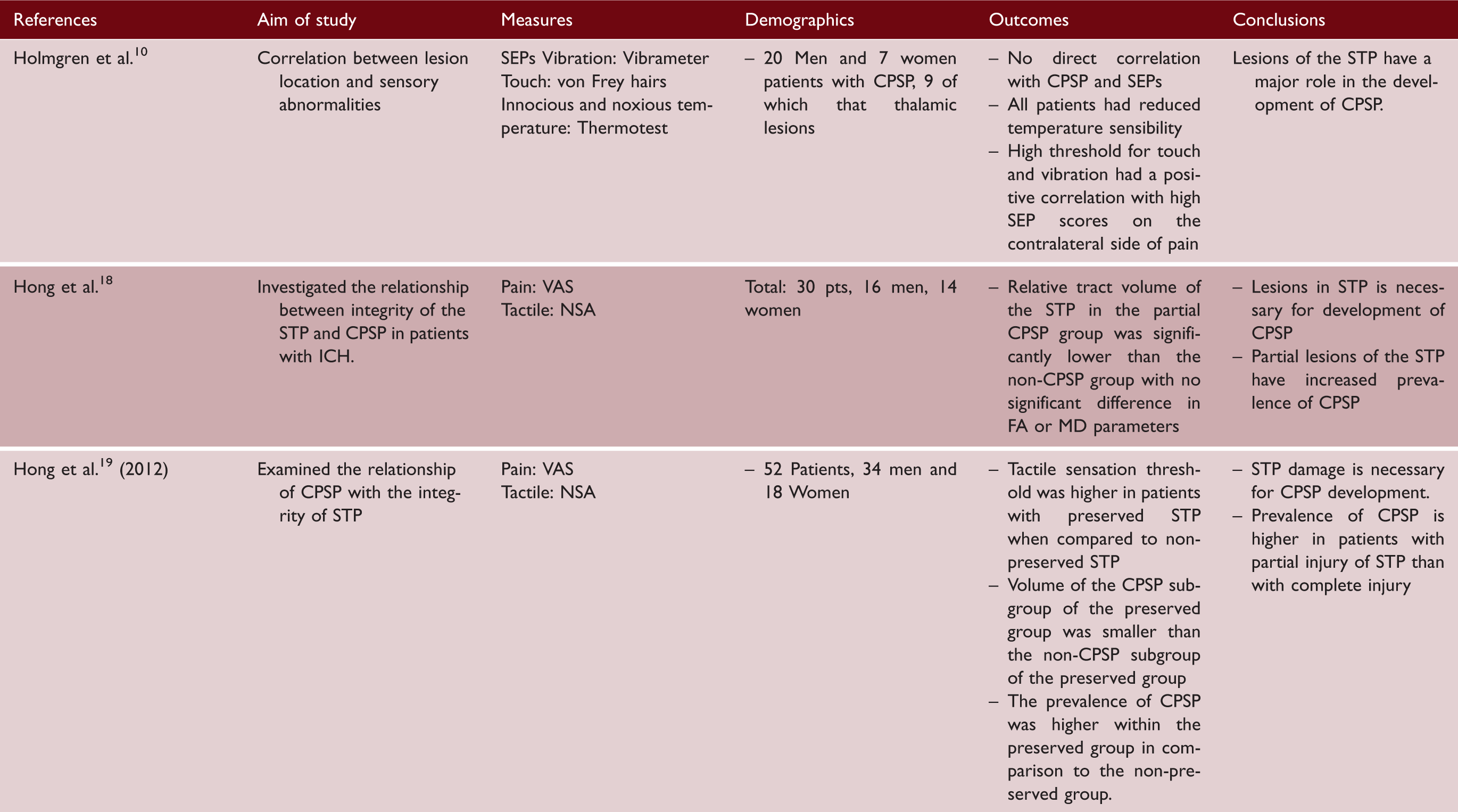
SEP: somatosensory-evoked potential; STP: spinothalamic pathway; ICH: intracranial hemorrhage; CPSP: central poststroke pain; VAS: visual analogue scale; FA: fractional anisotropy; MD: mean diffusivity
The second study 20 used diffusion tensor tractography (DTT) to visualize the STP and measure its integrity in 30 participants. 18 Patients were placed into one of two groups, CPSP (n = 16) or non-CPSP (n = 14). A significant decrease in STP volume was reported in the CPSP group when compared to the non-CPSP group. The authors reported no significant correlations between both CPSP and non-CPSP groups with the two other DTT parameters, fractional anisotropy (FA) and mean diffusivity (MD), representing the degree of microstructure directionality and water diffusion, respectively. They concluded that lack of significant correlations with FA and MD could be due to partial integrity of the STP, and that injury of the STP is a requirement for development of CPSP.
The integrity of the STP using DTT was also investigated in the third study, 19 but it incorporated patients with complete lesions of STP. A total of 52 patients were split into two groups, preserved (n = 34) and disrupted (n = 18) STP and subgroups of CPSP (preserved n = 16, disrupted n = 3) and non-CPSP (preserved n = 18, disrupted n = 15). The preserved group had a higher incidence of CPSP and despite the subgroup, tactile sensation was decreased in the preserved group, which may represent a dysfunctional regulation system. Spinothalamic tract volume in the CPSP preserved group was significantly less than the volume of the non-CPSP preserved group and the control group. Overall, they concluded that the STP plays a role in the development of CPSP and that patients with partial injury of the STP might have an increased risk of CPSP.
These three studies display consistent evidence that the STP plays a major role in CPSP. They also delineate that CPSP can occur even when the stroke is not in the thalamic region10,12,17,18 and when damage to the STP occurs. Therefore, it may be important to focus on the CIT when attempting to identify the etiology and treatment of CPSP. The CIT supports the findings that any disturbance to the pathway will result in pain after a stroke. However, the reason damage to these pathways cause CPSP is still unknown.
Brain imaging
Brain imaging studies (n = 7)

CPSP: central poststroke pain; VAS: visual analogue scale; MRI: magnetic resonance imaging; SPECT: single-photon emission computed tomography; LCH: lenticulocapsular hemorrhage; VPL: ventral posterior lateral; CT: computed tomography.
One reason for these differing results could be due to limitations in the studies (see Table 3). The four studies that17,21–23 found that strokes outside of the thalamic region had a high prevalence of CPSP did not have a control group. Also, two of these studies examined only patients who had a stroke in their thalamus, one examined patients who had strokes only in their ventroposterior thalamic nucleus and one examined patients who only had medial medullary infarction. In the three studies24–26 that concluded that CPSP is related to thalamic infarcts, two only examined thalamic strokes and one examined only patients with diagnosed CPSP. All seven studies had wide variability from time of diagnoses of stroke (imaging) and diagnoses of CPSP (see Table 3). CPSP often arises after initial stroke imaging and issues of selection bias due to major time variability (from time of imaging and diagnoses of CPSP) could cause both type I and type II errors. If imaging was done after CPSP was diagnosed, it may rule out other confounding variables (e.g. new infarct) and reduce the risk of a type I or type II errors. However, these studies only reported baseline imaging even when CPSP was diagnosed three years later. The results of the present systematic review indicate that the major limitations have impeded reliable and consistent findings about CPSP (Table 3). Future studies with larger sample sizes, a control group, and no selection bias are warranted to examine the role of CPSP with lesion location.
Clinical trials
Clinical studies and RCT for CPSP (n = 8)

VAS: visual analogue scale; RCT: randomized controlled trial.
The following trials include invasive as well as non-invasive methods. To date, effective clinical trials for CPSP are limited.29,30 Presently, tricyclic antidepressant amitriptyline is the only oral medication with a beneficial effect on CPSP. However, a number of studies have reported high rates of patient non-responders and intolerable side effects, which often result in medication cessation.15,31,32
Spinal cord and motor cortex stimulation
One clinical study (n = 30) addressed CPSP with percutaneous spinal cord stimulation (SCS) during a continuous treatment phase of two to seven days for CPSP patients. 31 Global pain relief measured at follow-up indicated that 30% (n = 9) reported good relief, 20% (n = 6) reported fair relief, and 50% (n = 15) reported poor relief. VAS score decreased from 8 to 6 (p = 0.001) from baseline to post-treatment. 31 Although the results of this study offer compelling preliminary evidence that SCS may provide improved pain relief for individuals with CPSP, there are notable limitations including small sample size, high percentages of individuals reporting poor to no relief, and lack of a control arm. As a result, findings from this study must be interpreted with caution until they can be replicated with larger samples sizes with a more stringent research design.
Only one study was identified that examined motor cortex stimulation as a potential treatment for CPSP. In this study, 11 patients with CPSP were treated at the pre-central gyrus. 32 Effective treatment (see Table 4) was observed in 73% of patients with pre-central stimulation, while 100% reported no pain reduction with post-central stimulation. Additionally, 45% continued to achieve pain relief with pre-central stimulation at their two-year follow-up. The authors 32 proposed that the mechanism of action is likely due to deafferented (partially or totally interrupted afferent signals) nociceptive neurons using motor provocation, which was more readily activated in the STP. Along with STPs, coexisting tracts were also stimulated, suggesting the need for further investigation on anatomical delineations to narrow down the therapeutic focus.
Tricyclic antidepressants
A double-blind RCT (n = 15) to evaluate amitriptyline (75 mg/d), cabamazepine (800 mg/d), and placebo’s effect on pain intensity was completed over a four-week treatment period. Table 4 shows mean pain intensity scores during the fourth week were identical for amitriptyline and cabamazepine. Global assessment of pain at the end of each treatment phase demonstrated a difference in effect for amitriptyline vs. placebo (p = 0.05) with improvement reported for 10 patients from the amitriptyline group and one from placebo.
Opioid antagonists
One double-blind trial (n = 20) assessed the effects of 8 mg intravenous naloxone in a 20 ml manufacturer’s vehicle and saline on CPSP on two occasions separated by two to three weeks 33 (Table 4). The results indicated no immediate effect of naloxone on pain. Analyses of before/after differences between naloxone and saline for all patients showed no significance (p = 0.86). The authors also noted that none of the subjects who experienced immediate pain relief were able to maintain improvement when long-term analyses concluded at two weeks. This further suggests that naloxone is ineffective for the treatment of CPSP pain. 33
Acupuncture
A single-blind RCT of apipuncture (see Table 4) and saline acupuncture on pain over a three-week treatment period found a significant reduction in the median VAS score (36.5 vs. 11.50; p = 0.009). 29 These results suggest that apipuncture might have an effect on reducing CPSP. Further studies including larger sample sizes, long-term follow-up, and double-blind trials would be beneficial in determining the efficacy of apipuncture for this population.
Anticonvulsants
An RCT to evaluate the effect Lamotrigine’s (200 mg/d) effect over two eight-week treatment periods (n = 30). 34 Both the treatment and control group indicated a baseline ongoing daily pain score of 6 (11-point scale) and post-treatment scores of 5 and 7, respectively. At the end of treatment, global pain scores were measured as 3 (moderate pain) for Lamotrigine and 4 (strong pain, p = 0.02) for placebo. 34 The study also implemented a global assessment of pain on daily activities, which did not indicate significant differences between Lamotrigine and placebo (p = 0.11). The results suggest that Lamotrigine is not effective monotherapy for CPSP.
One double-blind RCT evaluated Pregabalin’s (n = 220) effect on pain intensity, was assessed in a 12-week trial. 35 Results indicated that although the weekly pain score decreased for both treatment groups (pregabalin: 6.3–4.9, placebo: 6.3–5.0), there were no significant differences (p = 0.578).The authors delineate that the majority of patients treated with pregabalin did not achieve a 30% or 50% reduction in pain at endpoint compared to baseline as hypothesized. Additionally, 70% of pregabalin and 55% in placebo patients experienced adverse events. 35 Serious adverse events were experienced in six patients receiving pregabalin and two patients in the placebo arm.
A double-blind RCT examined the effect of levetiracetam (n = 42) on pain intensity over 24 weeks. 36 Side effects including, tiredness, increased pain, dizziness, pruritus, and headache were substantially more common in the treatment group than the control group, during the first treatment period. The authors reported that levetiracetam did not improve spontaneous or evoked pain and median pain scores did not differ between groups. They concluded that levetiracetam was not effective in reducing pain for CPSP patients.
Interpretation
Although a number of the above clinical trials29,30 reported reduction in CPSP symptoms, a substantial number of limitations (e.g. not multi-centered; no replication studies with diverse populations; small sample sizes; small effect sizes) were noted across studies, resulting in decreased generalizability of results. We are unable at this time to report any gender, race, or age differences in the trials, as they were not reported in the analysis and would likely have been underpowered. The brain stem and motor cortex stimulation studies show promise, but they were preliminary studies with small samples, and no significant values were reported. This systematic review of clinical trials did not identify any study that gave a clear picture of how to treat or identify CPSP.
Conclusions and limitations
There were three limitations in this systematic review. The first is that we examined papers in English and the second is we only used three major databases. However, more than 10,000 articles were identified during the screening process. The third is publication bias, as negative studies about CPSP were not published and could create bias with the findings in this systematic review. Even though CPSP has been linked to the thalamic region of the brain since the early 1900s, the literature showed equivocal results when examining location of stroke and CPSP. Overall, our review, which used the highest protocol for systematic reviews (PRISMA Guidelines), of the relevant literature indicates that there is a salient relationship between damage to the STP and CPSP.
Future investigation is pivotal in creating a universal definition of CPSP. Further investigating brain imaging and CPSP with studies that have stronger methodology may give way to the development of clinical trials that can address treatment options for CPSP. Also, we were unable to identify any research that addresses why CPSP worsens over time, but hypothesize and hope that future research will examine the role of damage to the STP networks as the primary reason for this progression. The results summarized in this systematic review support the CIT, suggesting that there are alternative affected pathways that may cause CPSP. Moreover, the link between strokes in the thalamic region of the brain and CPSP should be reevaluated as many studies indicated variability and/or a lack of association.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.