
Abstract
Background
Recombinant tissue plasminogen activator is the only FDA-approved thrombolytic agent for acute stroke treatment. However, there are concerns that recombinant tissue plasminogen activator may increase the risk of seizures (including early and late seizures).
Aims
We performed a systematic review to assess the incidence of seizures and the association of recombinant tissue plasminogen activator with seizure occurrence.
Summary of review
We searched major databases for articles published between 1995 and February 2016. The pooled incidence of post-stroke seizure, early seizure, late seizure, and seizures sub-types was estimated overall and by status for recombinant tissue plasminogen activator treatment, and unadjusted odds ratio used to quantify the effects of recombinant tissue plasminogen activator on post-stroke seizure occurrence. In all, 4362 stroke participants were included with 49–63% being male and median age ranging from 68 to 71 years. A total of 792 received recombinant tissue plasminogen activator. The incidence of post-stroke seizure per 1000 participants (95% CI) was 95 (31–196) overall, 113 (49–202) in recombinant tissue plasminogen activator and 169 (6–326) in non-recombinant tissue plasminogen activator-treated (all heterogeneity-p<0.0001). Incidence of early seizure per 1000 (95% CI) was 35 (27–45) overall; 34 (22–50) among recombinant tissue plasminogen activator-treated patients, and 36 (25–48) among recombinant tissue plasminogen activator naïve participants (all heterogeneity-p > 0.826). The pool incidence rate per 1000 (95% CI) of late seizure was 84 (4–263), 46 (2–145), and 212 (184–241), respectively, in the overall, the recombinant tissue plasminogen activator-treated group and non-recombinant tissue plasminogen activator-treated group (heterogeneity for overall and recombinant tissue plasminogen activator-treated group < 0.0001, non-recombinant tissue plasminogen activator naïve = 0.999). The pooled odds ratio for post-stroke seizure (recombinant tissue plasminogen activator vs. no recombinant tissue plasminogen activator) was 0.94 (95% CI: 0. 17–5.26, heterogeneity-p < 0.0001). The pooled incidence per 1000 participants (95% CI) was 30 (0–144), 17 (2–49), 16 (2–44), and 9 (0–50), respectively, for focal seizure without impairment of consciousness, focal seizure with impairment of consciousness, generalized convulsive seizure, and status epilepticus; all heterogeneity-p < 0.0003. Accompanying pooled odds ratio (recombinant tissue plasminogen activator vs. no recombinant tissue plasminogen activator) based on one study was always in favor of non-significantly lower risk in recombinant tissue plasminogen activator-treated patients (all heterogeneity-p = 1). There were insufficient data to compute pooled odds ratio for early and late seizure.
Conclusions
Seizures affect nearly 1 out of every 10 stroke patients with inconclusive suggestion that rates are similar in recombinant tissue plasminogen activator-treated and recombinant tissue plasminogen activator naïve patients. Large prospective studies are needed to better understand the relationship between recombinant tissue plasminogen activator and post-stroke seizure occurrence.
Keywords
Introduction
Stroke is a leading cause of seizure among adults. Between 3 and 30% of patients who have had a stroke develop post-stroke seizure,1–5 and contribute to approximately 11% of the population diagnosed with epilepsy. Post-stroke seizure is distinguished into ‘early onset seizure’ when occurring within one to two weeks of stroke onset, or ‘late onset seizure’ when occurring beyond one to two weeks after the index stroke event. Both are associated with increased mortality risk. In addition, early onset seizures are associated with increased disability rate, and late onset seizures with impaired quality of life. Since its first approval in 1995, recombinant tissue plasminogen activator (r-tPA) has been increasingly used for early revascularization in acute stroke, contributing to reducing related mortality and hence increasing the population of stroke survivors. In several observational studies, intracerebral hemorrhage, cerebral infarction with hemorrhagic transformation, stroke severity, and alcoholism have been associated with a greater probability of early seizure (ES) occurrence, while significant cortical involvement and stroke severity were associated with late onset seizure. 5 Endogenous tissue plasminogen activator (tPA) can sensitize the brain via up-regulation of N-methyl-d-aspartate receptors, leading to a lower threshold for a hyper-excitable state.6,7 This effect may be further exacerbated by the stress imposed on neurons, as well as short and long-term plasticity constraints induced by the vascular insult. Despite this theoretical background and the multiplicity of studies that have looked at seizure risk factors in stroke patients, to the best of our knowledge, the role of t-PA as a precursor of post-stroke seizure has not been systematically evaluated. Clarifying such a contribution has a potential to open avenues for new therapeutic approaches, by for instance specifically antagonizing the direct neuro-toxic effect of tPA or developing less epileptogenic pharmacological stroke therapies.
We conducted a systematic review to determine the incidence and the association of tissue plasminogen activator with post-stroke seizure.
Patients and methods
Data sources
We searched MEDLINE via PubMed, and SCOPUS using search strategies available in Additional file 1. Two evaluators (AL and AJJ) independently identified articles and sequentially (titles, abstracts, and then full texts) screened them for inclusion (Figure 1). We supplemented the electronic searches by scanning the references lists of relevant publications, and identifying their citations through the ISI Web of Sciences. Disagreements were solved by consensus or review by a third investigator (APK).
Flow chart of articles selection.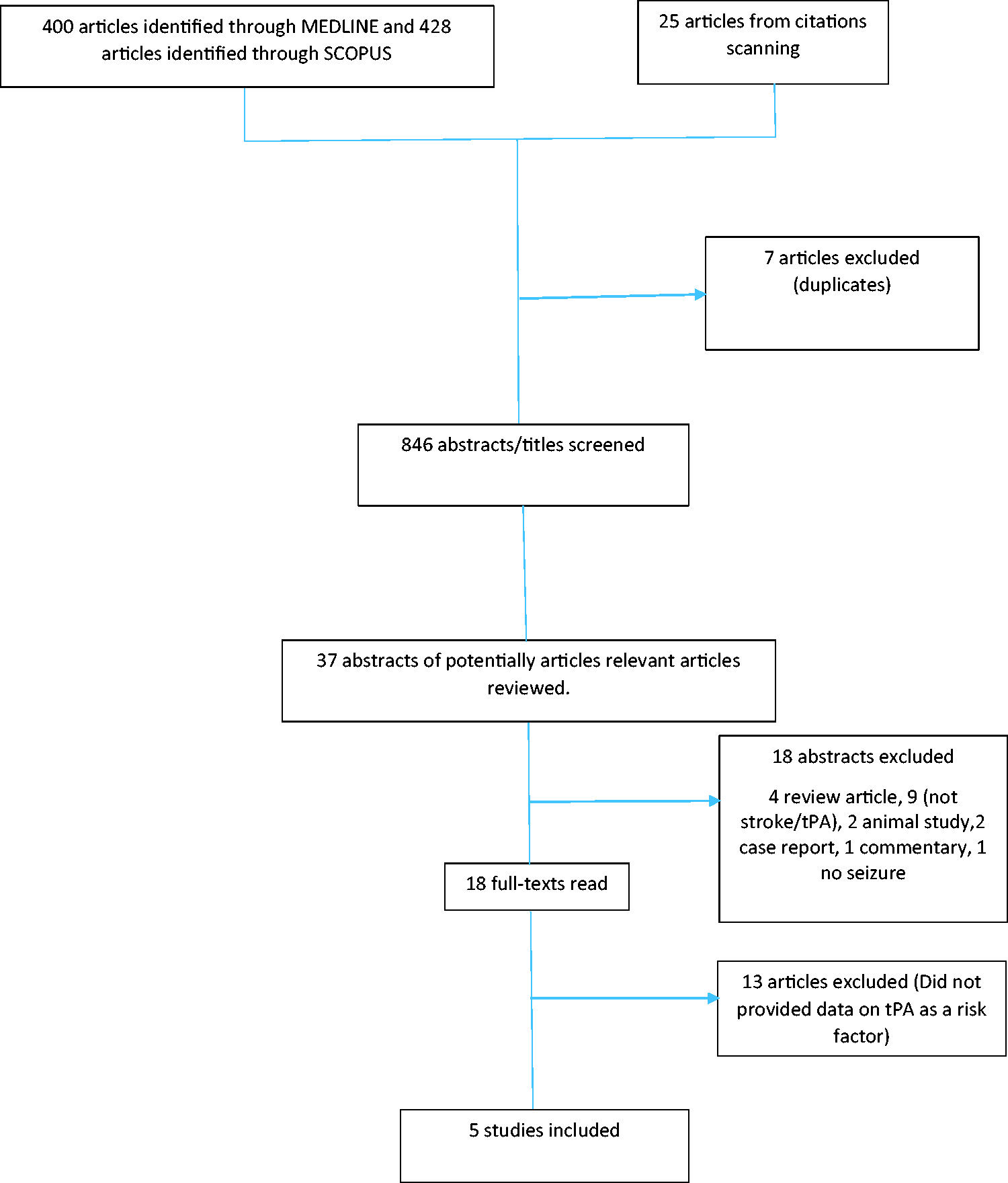
Study selection
We included studies that reported on post-stroke seizure. In 2014, the International League Against Epilepsy (ILAE) updated the definition of epilepsy as at least two unprovoked seizures occurring more than 24 h apart, one unprovoked seizure and a probability of further seizures similar to the general recurrence risk (approximately 60% or more) over the subsequent 10 years after two unprovoked seizures, or the diagnosis of an epileptic syndrome, 8 therefore in line with this definition, we included studies where the authors reported on post-stroke seizure. In addition, those studies had to include patients that had received r-tPA as part of the acute management of stroke. We excluded duplicate publications, review articles, studies conducted exclusively in pediatric populations, and case reports. Heterogeneity across studies was assessed with the use of the Cochran Q and I2 statistics, 9 while the Egger test of bias 10 was used to investigate the publication bias. Figure 1 shows the study selection process.
Data extraction
Two reviewers (AL and AJJ) independently conducted the data extraction from included studies. We extracted data on study settings, designs, population characteristics, measures of disease occurrence (incidence and/or prevalence), and risk factors for ES and late seizure (LS). We included studies that reported enough data to estimate the crude incidence of PSS.
Data assessment
Whenever prospective or retrospective studies had been conducted, we relied more on the conclusions of the prospective studies to address relevant questions, and appropriately reported the results.
Data synthesis
We conducted a narrative synthesis of the number of studies, study settings, and diagnoses criteria for ischemic stroke and seizure. To derive the overall incidence rate of PSS, and when possible ES, and LS across available studies, risk of r-tPA-related PSS, ES, and LS and the incidence of each type of seizure, we applied the random-effects model meta-analyses and restricted maximum-likelihood estimator to combine the estimates of the incidence and risk estimates from those studies and assessed the between-study heterogeneity, with the use of the ‘metaphor’ package of the R statistical software version 3.2.2 (15 August 2015), The R Foundation for Statistical Computing, Vienna, Austria. The incidence rates follow a Poisson distribution. Therefore, the square-root transformation was applied to stabilize the variance of the incidence rates prior to meta-analyses, and the estimates back-transformed for reporting.
This systematic review is reported according to the Preferred Reporting Items for Systematic Review and Meta-Analyses; please see checklist in the online appendix. No funding was received for the current study.
Results
Overview
Figure 1 describes the study selection process. Of the 846 articles identified, 37 abstracts were selected for in-depth evaluation (with most articles being excluded for not reporting on tPA administration) and 18 full texts were reviewed, of which 5 were included in the final selection.
Population characteristics and diagnosis criteria of selected studies
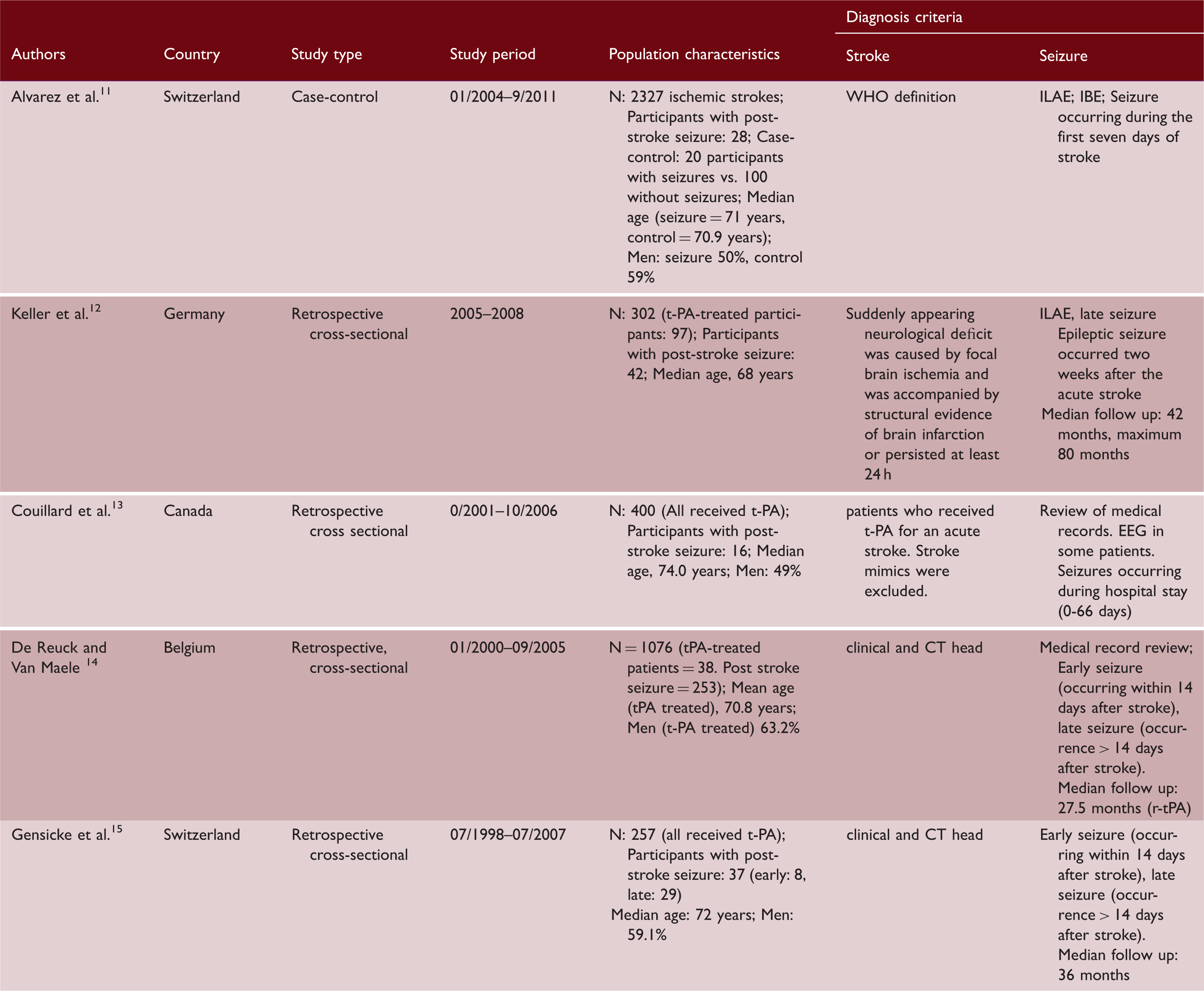
Note: WHO definition: new syndrome of rapidly developing clinical symptoms and/or signs of focal disturbance of cerebral function lasting longer than 24 h with no apparent cause other than vascular origin, regardless of whether infarction was evident on cerebral radio-imaging.
ILAE: international league against epilepsy; BE: international bureau of epilepsy.
Diagnosis criteria and measure of association between post-stroke seizure and exposure to r-tPA.
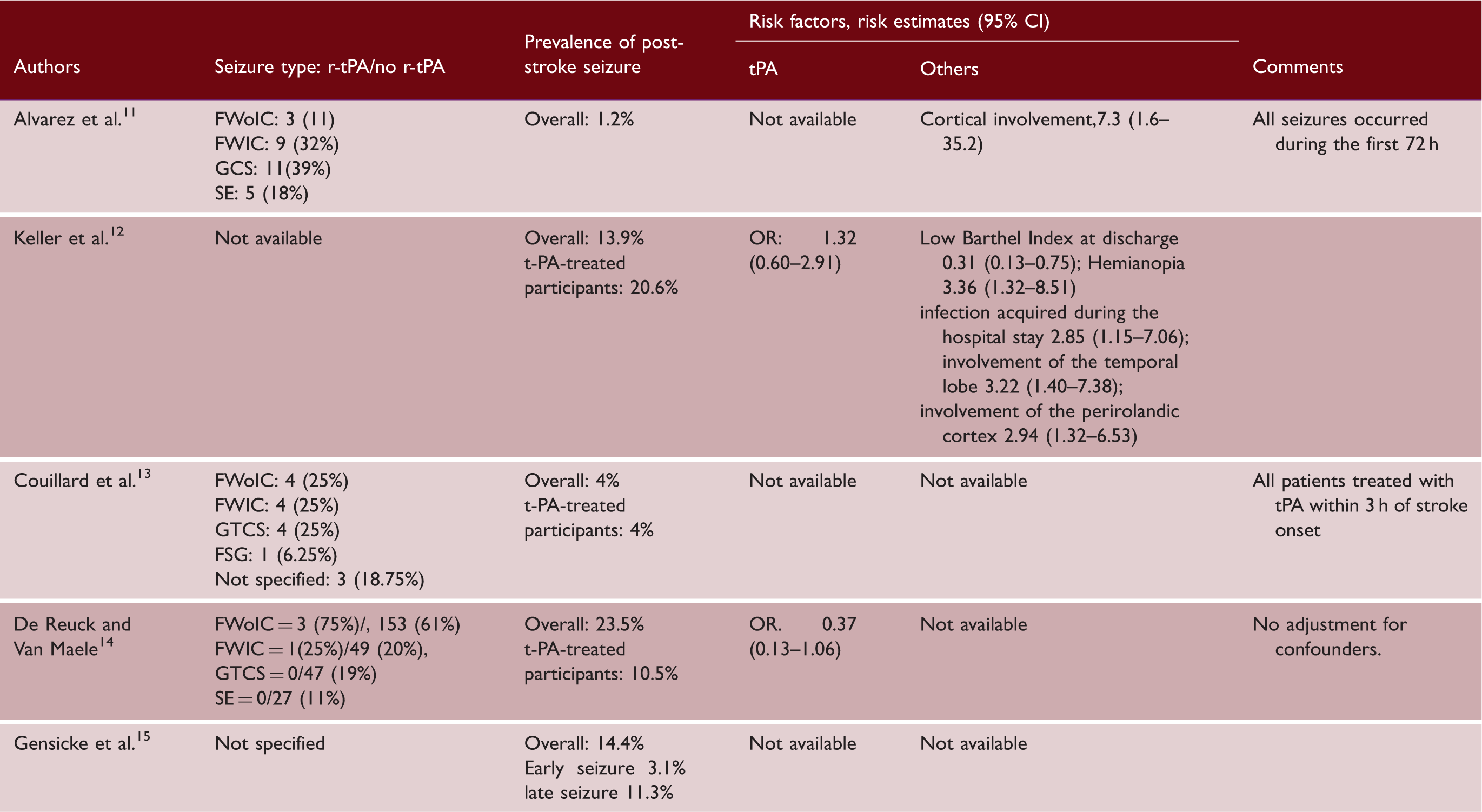
Note: Figure in brackets represents percentages within each subgroup.
t-PA: tissue plasminogen activator; FWoIC: focal seizure without impairment of consciousness; FWIC: focal seizure with impairment of consciousness; GTCS: generalized tonic and clonic seizure; SE: status epilepticus; FSG: focal seizure with secondary generalization; CI: confidence interval; OR: odds ratio.¶
Diagnosis of stroke was based on the onset of a focal or global persistent neurological deficit and supported by neuro-imaging. Only ischemic strokes were included. Intracranial hemorrhage and transient ischemic attacks were excluded. All seizure diagnoses were based on retrospective data obtained from medical records (five studies) and/or telephone encounter/letters to the patient or general practitioner (one study). Two studies used the International League Against Epilepsy definition. In other studies, no definition of seizure was provided. All studies provided a time-frame for the occurrence of seizure which ranged from a median of < 7 days to 42 months.
Overall post-stroke seizure incidence, clinical semiology, and risk of post-stroke seizure and r-tPA use
Out of a total of 4362 stroke participants included, 376 had PSS. Therefore, the incidence of PSS per 1000 participants (95% CI) from random effect models was 95 (31–196). Among the 792 participants who received treatment with r-tPA, 77 developed PSS yielding an incidence per 1000 (95% CI) of PSS of 113 (49–202) among r-tPA recipients. A total of 1243 participants did not receive r-tPA. In this group, 271 had PSS. Therefore, the incidence per 1000 (95% CI) of PSS in r-tPA naïve patients was 169 (6–326). Overall and in both sub-groups, there was evidence of heterogeneity (all p < 0.0001 for heterogeneity), Figure 2. Incidence of ES per 1000 (95% CI) was 35 (27–45) overall; 34 (22–50) among r-tPA-treated patients, and 36 (25–48) among non-rtPA-treated participants from a single study; with always no evidence of heterogeneity (all p > 826) Supplemental Figure I. The pool incidence rate per 1000 (95% CI) of LS in the three studies that provided data on late onset seizure was 84 (4–263), 46 (2–145), and 212 (184–241), respectively, in the overall, the r-tPA-treated group and non-r-tPA-treated group, with evidence of heterogeneity in the overall and r-tPA-treated group (both p < 0.0001), but not in non r-tPA-treated group which was based on a single study; Supplemental Figure II. The pooled odds ratio (OR) comparing r-tPA-treated vs. r-tPA naïve for PSS occurrence across two relevant studies was 0.94 (95% CI: 0. 17–5.26), Figure 3.
Forrest plot summarizing the frequency of post-stroke seizure. Forrest plot summarizing the odds of seizure in r-tPA vs non-tPA patients.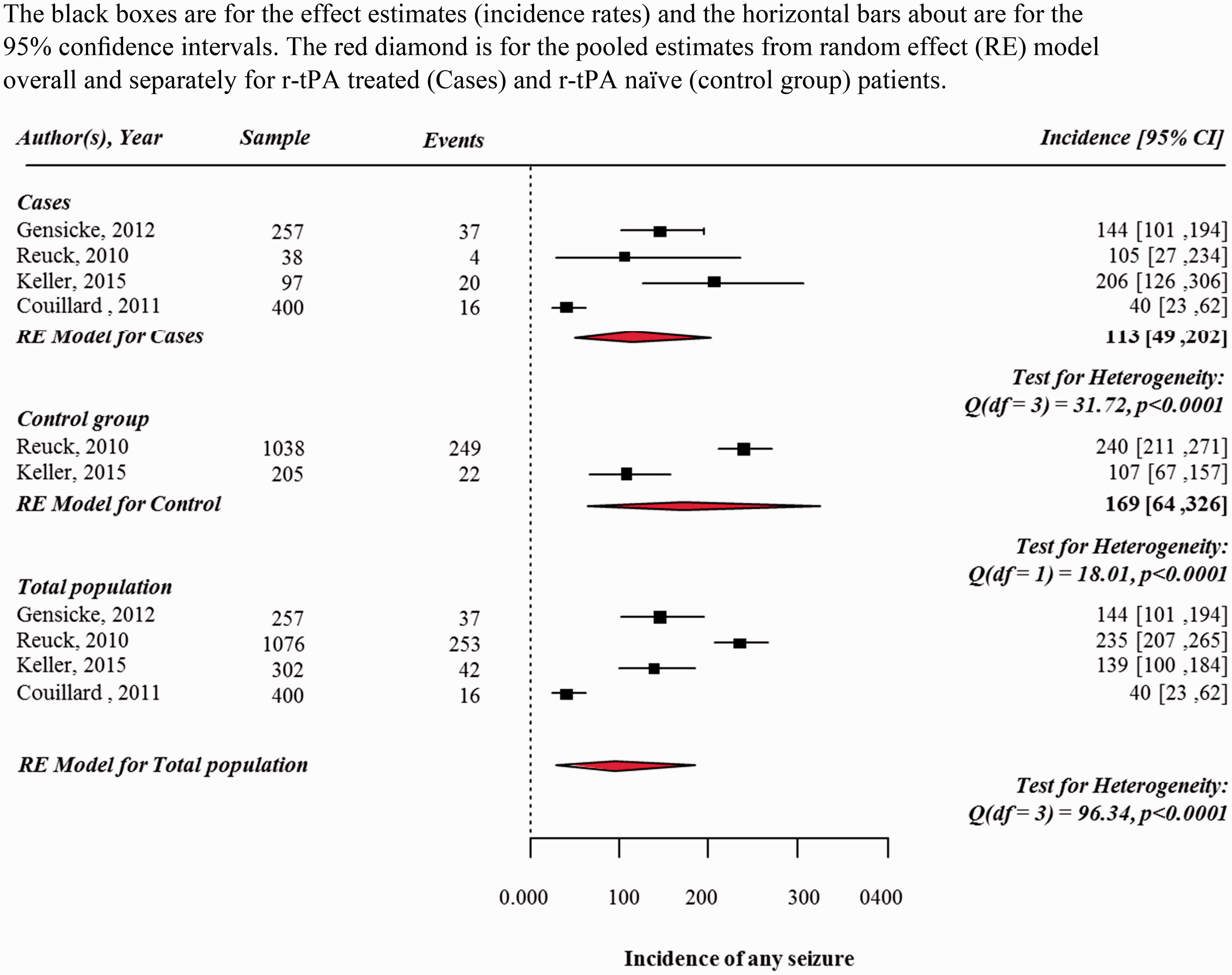
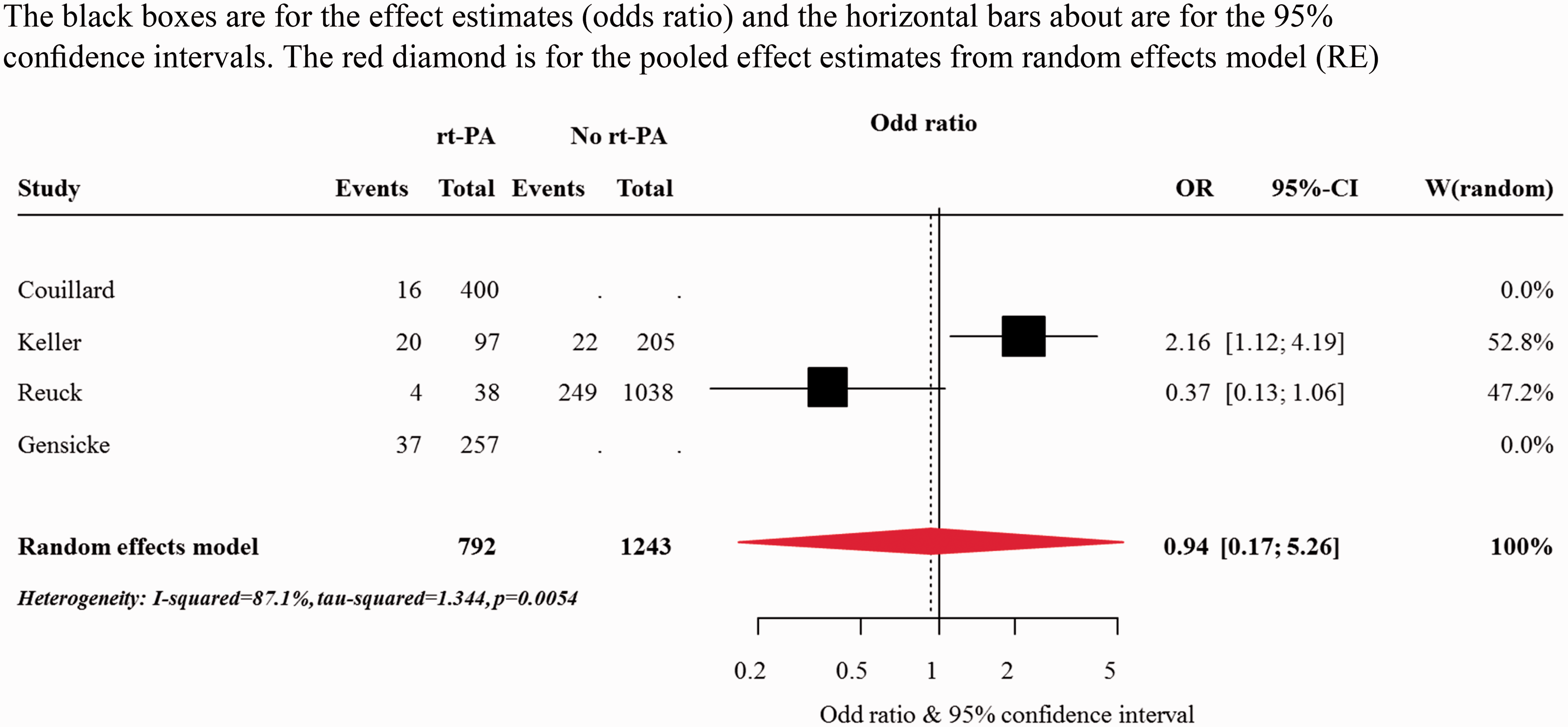
The type of clinical seizure was available in three studies totalizing 3083 participants including 458 who received r-tPA. Two studies provided incidence of seizure subtypes for r-tPA recipient separately and one study for r-tPA naïve participants separately. The incidence per 1000 participants (95% CI) of focal seizure without impairment of consciousness was 30 (0–144) overall, 30 (0–121) among r-tPA-treated participants and 146 (124–171) among r-tPA naïve participants with evidence of heterogeneity in the overall and r-tPA-treated group (both p < 0.0001), but not in non r-tPA-treated group which was based on a single study (p > 0.999) Supplemental Figure III. Equivalent figures for focal seizure with impairment of consciousness were 17 (2–49), 13 (5–27) and 48 (36–62), with evidence of heterogeneity in the overall (p = 0.0003), but not in the r-tPA (p = 0.5525) and non r-tPA-treated group which was based on a single study (p > 0.999) Supplemental Figure IV. Those for generalized convulsive seizures were 16 (2–44), 10 (3–22), and 45 (33–59), with evidence of heterogeneity in the overall (p = 0.0002), but not in the r-tPA (p = 0.8624) and non r-tPA-treated group (p > 0.999) which was based on a single study Supplemental Figure V. Finally, equivalent figures for status epilepticus were 7 (0–25), 21 (0–91), and 9 (0–50), with evidence of heterogeneity in the overall (p = 0.0002), but not in the r-tPA (p = 0.4458) and non r-tPA-treated group (p > 0.999) which was based on a single study Supplemental Figure VI. Only one study had sufficient information to allow computation of OR for the association between r-tPA and the occurrence of specific seizure types. In that study, the OR for focal onset seizure without impairment of consciousness comparing r-tPA vs. those who did not receive t-PA was 0.5 (0.15–1.64), Supplemental Figure VII. Equivalent figures for focal seizure with impairment of consciousness, generalized seizure, and status epilepticus were 0.53 (0.07–3.97), 0.27 (0.02–4.48), and (0.48 (0.03–7.98) respectively, Supplemental Figures VII, VIII, IX, and X.
Discussion
This systematic review has revealed that PSS overall, ES and LS affect nearly 1 out of every 10, 1 out of 30 and 1 out of 20 stroke patients treated with r-tPA, respectively. Except for a lower incidence of LS among non r-tPA recipient, incidence rates of post-stroke seizure were not different across r-tPA treatment status. However, these findings have to be interpreted in the context of the small number of eligible studies included, the likely low statistical power of individual studies and substantial heterogeneities across included studies.
The relationship between r-tPA and PSS was likely masked in the current systematic review by the heterogeneity across included studies. One possible source of heterogeneities is the varying definition of post-stroke seizure used across the few existing studies. For instance, two studies used the ILAE definition,11,12 while in other studies, the diagnosis of PSS relied on review of medical records.13–15 In one study, EEG was used to support the diagnosis of seizure in some participants. 10 Furthermore, the duration of follow-up studies ranged from as low as 7 days in one studies to up to 80 months in another. This variation could explain the difference in the incidence of PSS across studies. It is of note that studies did not provide enough data to allow us to account for the time of follow-up in the analysis. In the absence of such data in the form of person-time of follow-up for instance, we computed the incidence relative to the total number of participants at baseline, and compared r-tPA-treated versus r-tPA naïve participants for outcome occurrence using OR and not relative risk. The likely high incidence of PSS and seizures sub-types suggests that these cannot be treated as rare events, and as such OR is likely a biased estimator of the risk in this context. When analyzed separately, incidence of ES was comparable in r-tPA treated and r-tPA naïve participants, while non r-tPA participants seem to have a higher incidence rate of LS. Data on non-rtPA participants were, however, obtained from a single study, therefore limiting our ability to make any meaningful conclusion. If this later observation was real, this would signify that any association between r-tPA and seizure would wear off with time from r-tPA administration. In addition, the interpretation of the results of this study should account for the fact that r-tPA-treated patients represent only a small proportion of ischemic stroke patients which may not be representative of ischemic stroke in the general population.
With regard to the types of seizure observed in r-tPA-treated individuals, the incidence of focal seizure with impairment of consciousness was among the highest and was consistent across studies. A logical explanation to the focal onset is the presence of an epileptogenic brain lesion (i.e. cerebral infarct), while the impairment of consciousness may be related to large infarct size and/or severity of stroke. While none of the studies included in this systematic review has identified the size of the infarct or stroke severity as an independent predictor of PSS, previous studies have consistently found that those who have a large infarct or severe strokes are at increased risk of PSS.
Despite the absence of evidence for of the association between r-tPA in PSS in the current study, biological models and animal studies have suggested that tPA has an epileptogenic potential. Brain cells (neurons, oligodendrocytes, astrocytes, and microglia) are capable of secreting tPA which can be localized in pre-synaptic vesicles and dendrites. Endogenous tPA has been shown to exert an excitotoxic effect mediated by N-methyl D-Aspartate receptors through plasmin dependent and plasmin independent mechanisms. 16 Moreover, Tsirka et al. 17 have demonstrated that tPA-deficient mice are more resistant to pharmacologically induced seizures than wild types both with respect to the dose of Kainic acid (a glutamate receptor agonist) and Metrazol (a Gamma amino-butyric acid inhibitor) and the time from injection of pharmacological agent to seizure onset suggesting an epileptogenic property of tPA. The observation that grey matter is more vulnerable to ischemia and that tPA prevents white matter damage more than grey mater damage after stroke further add to the epileptogenic role of tPA.18,19
In conclusion, PSS affects 1 out of 10 stroke patients who receive r-tPA. High quality data from prospective large cohort are needed to better define the association of r-tPA and PSS. If such an association is clearly demonstrated, this might pave the way to the development of seizure-safe thrombolytic therapy or co-administration of seizure-prophylactic therapies.
Key points
Post-stroke seizure affects 1 out of 10 patients who received r-tPA. There is significant heterogeneity across study designs of PSS. There is a paucity of high quality data on the association between r-tPA and PSS
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.