
Abstract
Cerebral amyloid angiopathy is a common hemorrhagic small vessel disease of the brain, often associated with high risk of spontaneous lobar intracerebral hemorrhage. When the suspicion of cerebral amyloid angiopathy is raised, clinicians are hesitant in prescribing oral anticoagulation in patients in whom it is otherwise indicated, including the case of non-valvular atrial fibrillation. This is one of the thorniest clinical dilemmas in the field currently. In this short Leading Opinion piece by an international panel of clinicians-researchers active in the field, we present our consistent approach and future outlook on oral anticoagulation post intracerebral hemorrhage and in the setting of clinical-radiologic evidence of cerebral amyloid angiopathy. We discuss recent advances and support a more balanced approach with implications for the wider neurological clinical community in regards to successful recruiting this patient population in ongoing and future randomized trials.
Keywords
Cerebral amyloid angiopathy (CAA) is a common small vessel disease characterized by amyloid deposition in small cortical and leptomeningeal arteries. 1 CAA commonly accompanies stroke due to spontaneous lobar intracerebral hemorrhage (ICH) in elderly people, often associated with high risk of recurrence, in the range of 7% (95% CI: 3–12%) per year in well-phenotyped patients. 2 For this reason, when there is suspicion of CAA, clinicians might remain hesitant in prescribing oral anticoagulation in patients in whom it is otherwise indicated, including the case of non-valvular atrial fibrillation. This point is well illustrated in a recent comment piece by DeSimone et al., 3 as well as various review articles and opinion pieces on the topic. Though we agree with the general approach that clinicians should consider the possibility of CAA in weighing the risks and benefits of anticoagulation in elderly patients, 3 the clinical setting and context are key in these “tightrope balancing acts.”
While CAA is estimated to have prevalence of 20–40% in non-demented, and 50–60% in demented elderly subjects based on population-based autopsy studies, 4 only a small proportion of these individuals go on to develop CAA-related clinical events including symptomatic ICH. 1 Hence, the majority of individuals with CAA won’t be clinically affected by the disease and are never diagnosed during life, even through the use of the validated clinical-neuroimaging Boston criteria. 5 The most devastating clinical presentation of CAA is spontaneous lobar ICH. 1 Indeed, given the high recurrence rates after CAA-related ICH, a common approach has been to avoid anticoagulation when possible, to mitigate recurrence risk. 6 The role of oral anticoagulation for atrial fibrillation in CAA patients with a history of ICH thus remains hotly debated, despite the absence of real-world data on the effect of CAA on risk of anticoagulation-related ICH. 7 CAA is associated with a high risk of ICH recurrence, but in recent years, it has been better appreciated that this risk is not uniform, with the potential for different CAA phenotypes with varying propensities towards bleeding. Particularly, it seems that cortical superficial siderosis 8 – a recently discovered hemorrhagic MRI signature of CAA – is a potent marker of individuals at highest risk for recurrent ICH. This has implications in balancing ischemic versus hemorrhagic stroke risk, in that even after a CAA-related ICH, the presence of atrial fibrillation might confer enough risk for ischemic stroke, to offset the presumed risk of ICH recurrence in many patients (especially in the absence of siderosis and a CHA2DS2 score >1–2).
Summary of the ongoing randomized trials of anticoagulation for atrial fibrillation after intracranial hemorrhage
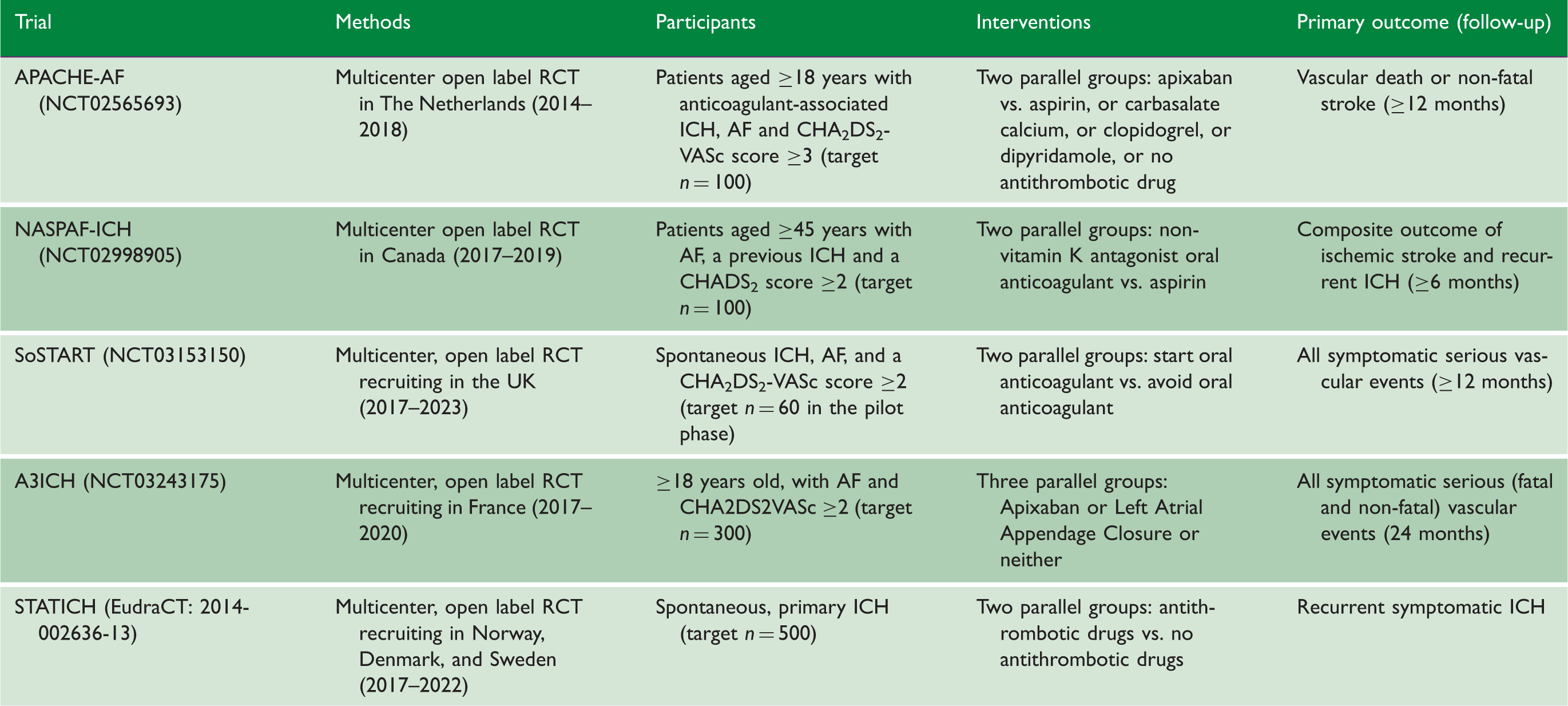
ICH: intracerebral hemorrhage.
The risk/benefit of anticoagulation therapy seems most reassuring for individuals with other CAA manifestations, including asymptomatic lobar microbleeds, particularly in the context of secondary ischemic stroke prevention. In this setting, clinicians should carefully weight risk-benefit for recurrent ischemic stroke vs. hemorrhagic complications, while keeping in mind that cerebral microbleeds are not only a marker of ICH, but also of ischemic stroke. A meta-analysis of ischemic stroke/TIA cohorts showed that in the presence of strictly lobar microbleeds, the pooled absolute event rate was 9.3% for future ischemic stroke versus 3.6% for ICH. 13 Moreover, it is important to keep in mind that there exists strong evidence from large randomized trials for the benefits of oral anticoagulation for people with atrial fibrillation, while data on ICH risk in relation to CAA and cerebral microbleeds mainly come from relatively small (and likely prone to selection bias) observational studies.2,13 In light of these, a scientific statement from the American Heart Association/American Stroke Association on prevention of stroke in patients with silent cerebrovascular disease, recommends that MRI screening for microbleeds is not needed before the initiation of antithrombotic therapies. 14
We suggest that a clinical approach based on the absolute risks of ischemic stroke vs. intracerebral hemorrhage, and considering the specific clinical context (symptomatic CAA presenting with ICH vs. other presentations or incidentally found, etc.) might be helpful in guiding anticoagulation decisions in the setting of CAA and atrial fibrillation. Randomized trials are clearly required to settle these important questions in survivors of CAA-ICH. A major barrier to overcome in future randomized trials of different oral anticoagulation strategies after ICH, is the threat of low recruitment rates, due to the reluctance of investigators to enroll patients with lobar ICH or CAA out of fear of bleeding complications based on small observational studies alone. 15 In patients with non-ICH CAA manifestations, no trials are underway, but the weight of evidence in this setting might favor oral anticoagulation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ contributions
Andreas Charidimou: Write-up. Ashkan Shoamanesh: Critical revisions, Table. Rustam Al-Shahi Salman: Critical revisions. Charlotte Cordonnier: Critical revisions. Luke A Perry: Critical revisions, Table design. Kevin N Sheth: Critical revisions. Alessandro Biffi: Critical revisions. Jonathan Rosand: Critical revisions. Anand Viswanathan: Critical revisions.