
Abstract
Background
The accurate knowledge of secular trends in prevalence, characteristics and outcomes of patients with ischemic stroke and atrial fibrillation allows better projections into the future.
Aim
We aimed to report the overall, age- and sex-specific secular trends of characteristics and outcomes of patients with acute ischemic stroke (AIS) and atrial fibrillation between 1993 and 2012 in the Athens Stroke Registry.
Methods
We used Joinpoint regression analysis to calculate the average annual percent changes and 95% confidence intervals.
Results
Among 3314 stroke patients, 1044 (31.5%) had atrial fibrillation. Between 1993 and 2012, there was an average annual reduction of 0.8% (95% CI: −1.5%; 0.0%) in the proportion of atrial fibrillation patients among all AIS patients, whereas the proportion of newly diagnosed atrial fibrillation patients among all atrial fibrillation patients increased annually by an average of 7.1% (95% CI: 5.4%;8.9%). Among all atrial fibrillation patients, there was an average annual reduction of 2.9% (95% CI: −2.7; −3.2%) in the proportion of previously known atrial fibrillation patients, followed by an annual average reduction of 2.4% (95% CI: −1.2; −3.6%) in the proportion of previously known atrial fibrillation patients not receiving any antithrombotic treatment at admission. During that period, there was an increase in the average annual proportion of previously known atrial fibrillation patients treated with anticoagulants (6.4%, 95% CI: 1.2;11.9%) and aspirin (2.3%, 95% CI: −0.4;5.0%) at admission; an average annual increase in the proportion of atrial fibrillation patients who were prescribed anticoagulant was apparent both for patients with mRS<4 (3.5%) and mRS: 4–5 (7.2%), while the proportion of atrial fibrillation patients who were prescribed aspirin or no antithrombotic at discharge was annually reduced (5.8% for mRS<4; 1.6% for mRS: 4–5 and 7.1% for mRS<4;5.3% for mRS: 4–5 respectively). Stroke recurrences were annually reduced by an average of 5.8% (95% CI: −8.6; −3.0%), along with cardiovascular events (6.5%, 95% CI: −8.3; −4.7%) and deaths (7.9%, 95% CI: −9.2; −6.5%).
Conclusions
Between 1993 and 2012, the proportion of atrial fibrillation patients on proper antithrombotic treatment and the rate of newly diagnosed atrial fibrillation increased significantly. Rates of stroke recurrence, cardiovascular events, and mortality reduced significantly.
Introduction
Atrial fibrillation (AF) is the most frequent sustained cardiac arrhythmia with an estimated prevalence to be >7% in persons older than 65 years and >10% in those older than 75 years.1–4 The incidence of AF shows a steep rise of >12% during the recent decades, and it is expected that more than 15 million people will have AF in the U.S.A. by 2050.1,3 AF is a major risk factor for ischemic stroke (IS) as it increases stroke risk five-fold, and AF prevalence in patients with acute ischemic stroke or transient ischemic attack (TIA) is increasing.1,5 Strokes due to AF are frequently caused by emboli which occlude large vessels and may be retrieved by endovascular thrombectomy or dissolved by intravenous administration of alteplase;6,7 without effective treatment, AF strokes are usually severe and associated with high mortality, poor functional outcome, and higher recurrent risk compared to stroke of other etiologies.8–11 Timely detection of AF, before it leads to thromboembolic complications like ischemic stroke and systemic embolism, is of paramount importance for the primary prevention of stroke and related disability.
The accurate knowledge of secular trends in prevalence, characteristics, and outcomes of patients with IS and AF allows better projections into the future, which in turn may facilitate a more effective allocation of health-associated human and financial resources aiming to design more efficiently the organization of the acute stroke setting, the availability of rehabilitation facilities, and strategies for primary and secondary prevention.
We aimed to report the overall, age- and sex-specific secular trends of characteristics and outcomes of patients with acute ischemic stroke and AF during the two-decade period between 1993 and 2012 in the Athens Stroke Registry.
Methods
Study population and definitions
The study population was derived from the Athens Stroke Registry, which includes all consecutive patients with an acute first-ever IS admitted in Alexandra University Hospital, Athens, Greece between 1993 and 2012. 12 Patients with recurrent stroke have not been included in the registry. The scientific use of the data collected in the Athens Stroke Registry was approved by the local Ethics Committee.
The methodology followed to register data in the Athens Stroke Registry was described in detail elsewhere. 13 Stroke was defined according to the World Health Organization criteria. 14 Hypertension was defined as systolic blood pressure >140 mmHg and/or diastolic blood pressure >90 mmHg diagnosed at least twice before stroke or if patient was already on antihypertensives. 15 Diabetes mellitus was defined if patient was already on antidiabetic drugs and/or insulin, or if fasting blood glucose level was >6.0 mmol/l before stroke. 16 Dyslipidemia was defined as total cholesterol concentration >6.5 mmol/l the day after admission, or if patient had a previous diagnosis of dyslipidemia. 17 Coronary heart disease was assessed by questionnaire and relevant medical confirmation. Heart failure was defined according to the criteria recommended by the working group on heart failure of the European Society of Cardiology. 18 TIA was defined as complete disappearance of signs and symptoms within 24 h, regardless of infarction being shown on neuroimaging. 19 Stroke severity was assessed with the National Institutes of Health Stroke Scale score (NIHSS) at admission. 20 The CHADS2 score was calculated taking into account the following parameters: congestive heart failure, hypertension, age 75 years or older, diabetes mellitus (1 point each), and prior stroke or TIA (2 points).21,22 The CHA2DS2-VASc score was calculated incorporating the following parameters: congestive heart failure, hypertension, age (1 point if 65–74 years; 2 points if ≥ 75 years), diabetes mellitus, previous stroke/TIA (2 points), vascular disease, and sex category (1 point if female). 23 For the present analysis, the pre-stroke CHADS2 and CHA2DS2-VASc score were considered.
With regard to AF detection, all patients had a 12-lead electrocardiogram (ECG) at admission and serial ECGs during hospitalization. In patients on sinus rhythm, AF paroxysms were sought by (a) repeated ECGs during hospital stay, (b) continuous ECG monitoring for one week or until discharge for patients treated in the acute stroke unit (ECG was observed by trained nurse personnel and intermittently analysed by the treating physician), and (c) Holter ambulatory ECG monitoring in cases that a and b were negative, and AF was strongly suspected from the clinical presentation and/or brain imaging findings (e.g. multiterritorial infarcts, strokes presenting with maximum severity at onset, largely dilated left atrium). Stroke was considered as “AF-related” if AF was previously known or newly detected during hospitalization or diagnostic work-up, and no other apparent cause of stroke was identified.
Follow-up and outcomes
The time of initial stroke was the inception of follow-up. Patients were prospectively followed up at one, three, and six months after discharge and yearly thereafter. Follow-up was routinely performed at the outpatient clinic. In case of patients with severe handicap, clinical follow-up was assessed at patient's residence or by telephone interview. Lost to follow-up was defined as inability to reach the patient or the patient's proxies at a scheduled time point.
The outcomes assessed during follow-up included stroke recurrence, death, and a composite of major cardiovascular events comprising recurrent stroke, myocardial infarction, aortic aneurysm rupture, systemic embolism, or sudden cardiac death. Recurrent stroke was defined as a cerebrovascular event of sudden onset, lasting >24 h, subsequent to the initial stroke, which clearly resulted in a new neurological deficit, or an increase in an existing deficit. 24 Visualization of a new lesion on brain imaging, involving an anatomical site or vascular territory different from that of the index event, was mandatory to support the diagnosis of recurrent stroke during the first three weeks after stroke onset, in order to ensure that systemic causes of clinical deterioration after an initial stroke (e.g. hypoxia, hypotension, hyperglycaemia, infection) and worsening of symptoms because of progression of the initial stroke were not misclassified as a recurrent cerebrovascular event. Outcome events were evaluated by combining all available information obtained from death certificates, hospital records, physicians' notes in private practice, necropsy findings, and the patients' clinical presentation at the regular follow-up assessments.
Statistical analysis
Continuous variables are summarized as mean value and standard deviation (SD), discrete variables as median value and 95% confidence interval (CI) and categorical variables as absolute number and proportion. For patients lost during follow-up, survival data were censored at the last time known to be alive. Patients who experienced >1 composite vascular event during the follow-up period were censored at the time of the first event. Statistical analyses and graphs were performed/created with the R statistical package.
We used Joinpoint regression analysis, using Kim's method 25 and Joinpoint Regression Program (Version 4.4.0.0-January 2017; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute) to assess changes according to sex and age in: the proportion of previously known AF among all patients with AF; the proportion of previously unknown AF among all patients with AF; the proportion of AF-related strokes among all ischaemic strokes; the type of antithrombotic treatment at admission in all patients with AF; the type of antithrombotic treatment at discharge in all patients with AF stratified by modified Rankin scale (mRS) score; the incidence of stroke recurrence in all patients with AF; the incidence of cardiovascular events in all patients with AF; the incidence of death in all patients with AF. We evaluated trends over time and calculated the average annual percent changes and 95% confidence intervals. Also, we assessed and depicted graphically the aforementioned trends during the study period at a two-year step.
Results
Between 1993 and 2012, 3314 patients were admitted with acute ischaemic stroke. Of these, in 1044 (31.5%), AF was previously known or newly diagnosed. Between 1993 and 2012, there was a slight average annual percentage reduction of 0.8% (95% CI: −1.5, 0.0%) in the proportion of patients with AF among all IS patients, which was similar for all age and sex groups with the exception of the >80 years group (Figure 1). The median age of AF patients was 76 years (IQR: 70–82 years) and 541 (51.8%) of them were women. The age- and sex-specific main characteristics of the AF patients, their comorbidities, their type of antithrombotic treatment at admission/discharge and their outcomes during the first and the last five-year period of the study (1993–1998 and 2007–2012, respectively) are summarized in the supplementary file.
Average annual percent change in the proportion of: previously known AF among all patients with AF; previously unknown AF among all patients with AF; AF-related strokes among all ischaemic strokes (upper left panel); the type of antithrombotic treatment at admission in all patients with AF (upper right panel); the type of antithrombotic treatment at discharge in all patients with AF stratified by mRS (middle panels); the incidence of stroke recurrence, cardiovascular event and death in all patients with AF (lower panel). Trends of CHADS2 (left panel) and CHA2DS2-VASc (right panel) scores during the study period (at a two-year step).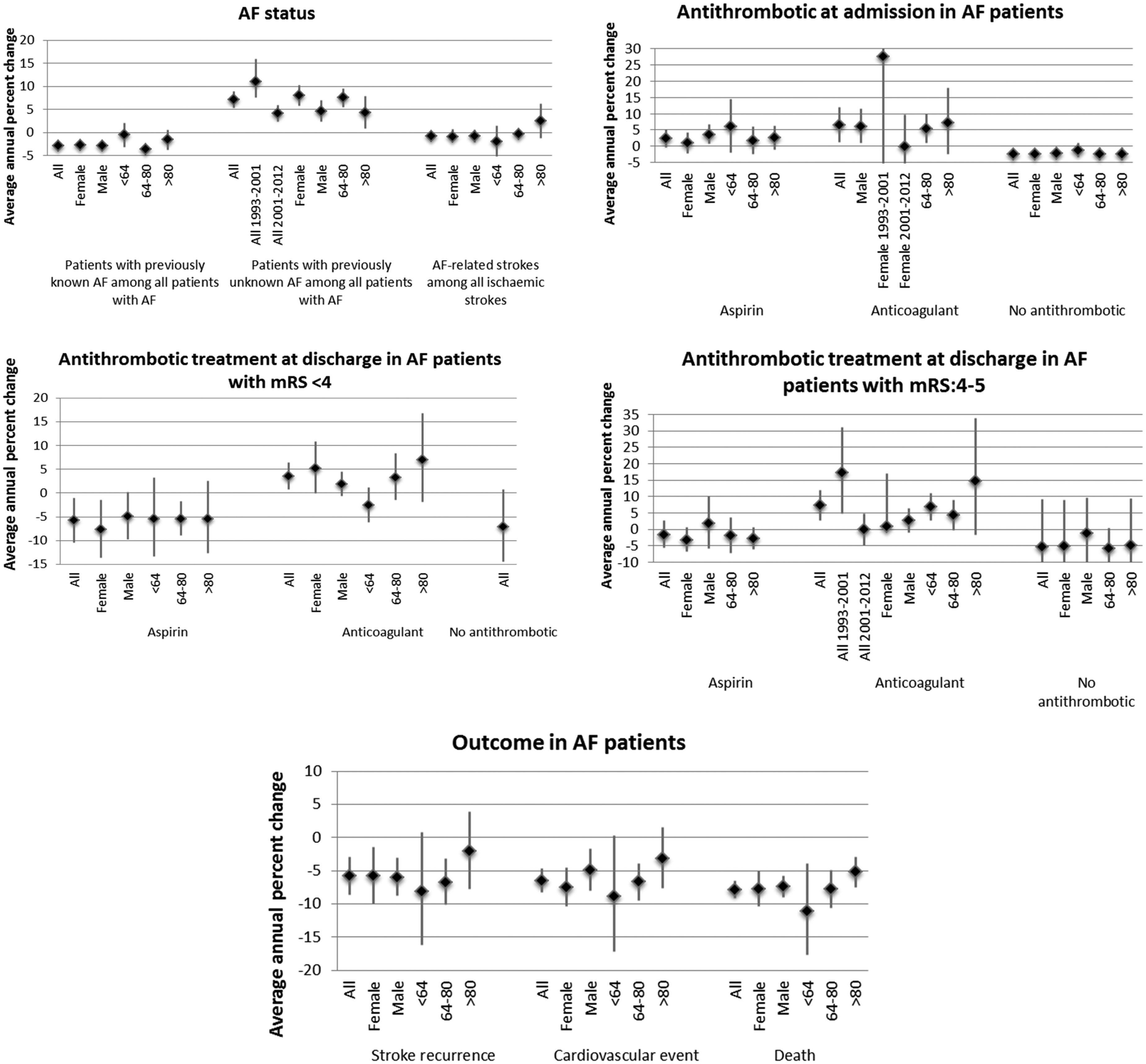

Trends of patient characteristics
There was a significant increase in the prevalence of arterial hypertension (from 66.6% in the 1993–1998 period to 85.1% in the 2007–2012 period in the overall AF population, relative increase of 27.8%) and dyslipidemia (from 18% in the 1993–1998 period to 29.2% in the 2007–2012 period in the overall AF population, relative increase of 62.2%) which was evident in all age and sex groups (supplementary file). On the contrary, there was no difference in the CHADS2 and CHA2DS2VASc scores of AF patients during the overall study period (supplementary table and Figure 2).
Trends of AF characteristics
Among all AF patients, AF was firstly diagnosed at admission in 110 patients (10.5%) and during follow-up in 197 patients (18.9%). Between 1993 and 2012, there was a significant average annual percentage increase of 7.1% (95% CI: 5.4, 8.9%) in the proportion of patients newly diagnosed with AF (either at admission or during diagnostic work-up) among all AF patients, a finding which was evident in all age and sex groups (Figure 1). During the same period, there was a significant average annual percentage reduction of 2.9% (95% CI: −2.7, −3.2%) in the proportion of patients with previously known AF among all AF patients, a finding which was evident in all age and sex groups with the exception of the <64 years group (Figure 1). Figure 3 summarizes these trends during the study period in a two-year pace.
Trends of the proportion of patients with previously known and newly diagnosed AF during the study period (at a two-year step). (a): overall AF population; (b): sex-specific trends; (c): age-specific trends.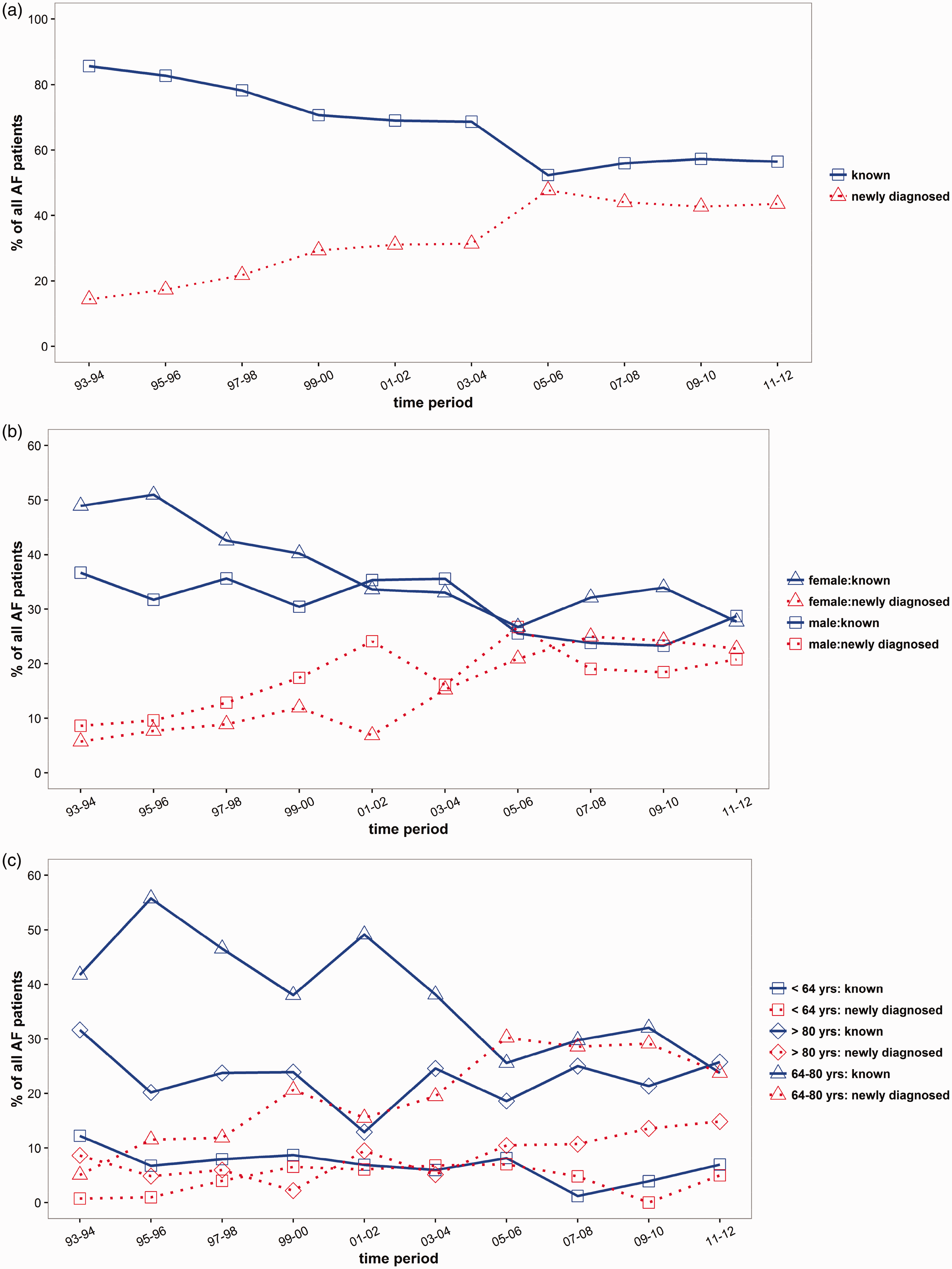
Trends of antithrombotic strategies at admission
Among all AF patients, AF was previously known in 718 patients (68.8%), of whom 186 (25.9%) were previously treated with aspirin, 184 (25.6%) with anticoagulants, and 354 (49.3%) were not treated with any antithrombotic. Between 1993 and 2012, there was a significant average annual percentage reduction of 2.4 (95% CI: −1.2, −3.6%) in the proportion of patients with previously known AF who were not receiving any antithrombotic treatment which was evident in all age and sex groups (Figure 1). During the same period, there was a significant average annual percentage increase of 6.4% (95% CI: 1.2–11.9%) in the proportion of patients with previously known AF who were on anticoagulants at admission, which was evident in all age and sex groups with the exception of the female group for the 2001–2012 period where no further increase was noticed (Figure 1). Also, during the 1993 and 2012 period, there was a marginal average annual percentage increase of 2.3% (95% CI: −0.4, 5.0%) in the proportion of patients with previously known AF who were on aspirin at admission which was evident in all age and sex groups (Figure 1).
Trends of antithrombotic strategies at discharge
Among the 883 AF patients alive at discharge (84.6% of all admitted AF patients), 282 (31.9%) were prescribed aspirin, 435 (49.3%) an anticoagulant, 49 (5.5%) a combination of antiplatelet and anticoagulant, and 117 (13.2%) were not prescribed any antithrombotic.
Between 1993 and 2012, there was a significant average annual percentage increase of 3.5% (95% CI: 0.7–6.4%) in the proportion of patients with mRS<4 who were prescribed an anticoagulant for stroke prevention which was evident in all age and sex groups with the exception of the <64 age group (Figure 1). Similar were the results for the patients with mRS: 4–5, where there was a significant average annual percentage increase of 7.2% (95% CI: 2.6, 11.9%) in the proportion of patients who were prescribed an anticoagulant for stroke prevention (Figure 1).
Between 1993 and 2012, there was a significant average annual percentage reduction of 5.8% (95% CI: −10.4%, −1.1%) in the proportion of patients with mRS<4 who were prescribed aspirin for stroke prevention which was evident in all age and sex groups (Figure 1). Similar were the results for the patients with mRS: 4–5, where there was a marginal average annual percentage reduction of 1.6% (95% CI: −5.7%, 2.7%) in the proportion of patients who were prescribed aspirin for stroke prevention which was evident in all age and sex groups with the exception of men (Figure 1). Also, during the study period, there was a significant average annual percentage reduction in the number of AF patients who were not prescribed any antithrombotic at discharge (7.1% in patients with mRS <4 and 5.3% in patients with mRS: 4–5, Figure 1).
Trends of outcomes
The 883 AF patients alive at discharge (85% of all admitted AF patients) were followed up for a median of 29.4 months, which corresponds to 2162 patient-years. During the follow-up period, we recorded 6.7 stroke recurrences, 9.6 major cardiovascular events, and 16 deaths per 100 patient-years.
Between 1993 and 2012, there were there was a significant average annual percentage reduction in stroke recurrences (5.8%, 95% CI: −8.6, −3.0%), cardiovascular events (6.5%, 95% CI: −8.3, −4.7%), and deaths (7.9%, 95% CI: −9.2, −6.5%), which were evident in all age and sex groups (Figure 1). In particular, there was a significant reduction in the rate of stroke recurrence (from 8.1 events per 100 patient-years in the 1993–1998 period to 3.1 events per 100 patient-years in the 2007–2012 period, relative reduction of 62.3%), major cardiovascular events (from 12.3 events per 100 patient-years in the 1993–1998 period to 8.0 events per 100 patient-years in the 2007–2012 period, relative reduction of 35.0%), and death (from 21.3 events per 100 patient-years in the 1993–1998 period to 12.3 events per 100 patient-years in the 2007–2012 period, relative reduction of 42.4%). These trends were evident in all age and sex groups (supplementary table and Figure 4).
Overall, age- and sex-specific trends of outcome events (per 100 patient-years) according to the admission year (at a two-year step). (a): stroke recurrence; (b): major cardiovascular events; (c): death.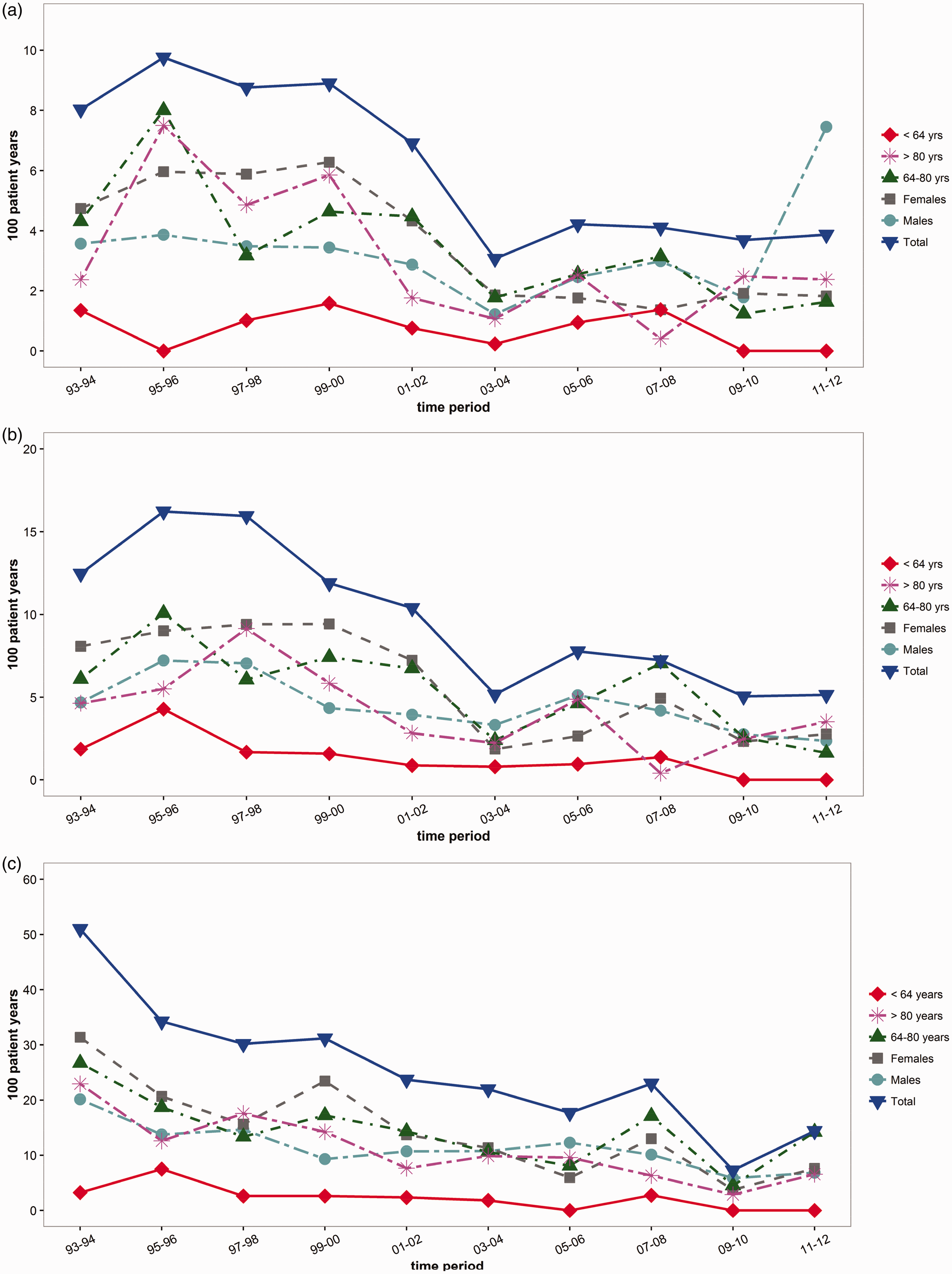
Discussion
In this analysis of 1044 acute ischemic stroke patients with AF who were prospectively registered within a 20-year period between 1993 and 2012, we found that during this period the antithrombotic strategy at discharge improved with time as more patients were anticoagulated and fewer patients were on antiplatelets or no antithrombotic treatment; the outcomes improved with time as the rate of stroke recurrence, major cardiovascular events and death decreased; the rate of AF detection improved with time as the proportion of patients with newly diagnosed AF increased; there were no major differences among age and sex groups.
This study shows that the antithrombotic strategy in AF patients during the two last decades has considerably improved not only in the secondary prevention setting (as it is evident by our finding that the proportion of our stroke patients who were discharged on anticoagulants increased with time) but also in the primary setting (as it is evident by the finding that the proportion of patients with previously diagnosed AF who were on anticoagulants increased with time). Apparently, this reflects upon the amount of scientific evidence which came available during these years which clearly concluded that anticoagulation is the optimal antithrombotic strategy in the vast majority of AF patients, the more effective medical education, and the increased awareness of patients and families about the importance of adherence to anticoagulant treatment.26,27
Apparently, the improvement in the antithrombotic strategy in AF patients during these years as recorded in the present study is the major cause of the important reduction of outcome events in these patients. This is further potentiated by the fact that AF is more frequently detected nowadays as it was evident by our finding that newly diagnosed AF was increasingly detected in our IS patients during this 20-year period. Apparently, the availability of modern techniques of prolonged continuous ECG recording and the emerged evidence that these techniques can efficiently detect covert AF enhanced the ability and alertness of physicians to detect previously undiagnosed AF and, ultimately, prevented AF-related strokes.28,29 These facts may counteract, at least partly, the current steep increase of the prevalence of the AF epidemic and may have obvious important implications for the patients, the families, and the allocation of human and financial resources of the health system. 1
Although encouraging, these results show a reality which is still far from ideal: during the 2007–2012 period one out of five patients with previously known AF were not on any antithrombotic at admission, although it should be taken into consideration that this may partly represent AF patients who have had some contraindication for antithrombotic treatment. This finding is similar to a recent report by the phase 1 GLORIA-AF (Global Registry on Long-Term Oral Antithrombotic Treatment in Patients with Atrial Fibrillation) where approximately 20% of AF patients were not on any antithrombotic. 30 The availability of the non-vitamin-K antagonist oral anticoagulants (NOACs) which have a superior safety profile than vitamin-K antagonists may have led to some improvement during the recent years.31–34 Other advances that may improve further the outcomes of AF patients include the increasing awareness of physicians about the importance of anticoagulation; the enhanced adherence of patients to NOAC compared to warfarin; 35 the development of NOAC reversal agents which may rapidly remove the anticoagulant effect of the NOACs in case of an acute ischemic stroke and make the patient eligible for intravenous thrombolysis; 36 the strong evidence that endovascular thrombectomy improves outcomes of stroke patients with large-vessel occlusion as it is very frequently the case for AF patients; 6 the availability of modern techniques of prolonged continuous ECG recording which can efficiently detect covert AF and increase the rate of anticoagulation in these patients.26,27 All these advances allow us to be optimistic that the consequences of the current AF epidemic can be counterbalanced, at least up to a certain degree.
The main strengths of this study is its long period, the prospective registration of a wide set of clinical, laboratory and imaging data using pre-specified definitions, the long follow-up and the assessment of several hard outcomes including stroke recurrence and death. Also of importance, we assessed not only AF detected during hospitalization but also AF detected during outpatient monitoring performed after hospital discharge. Nonetheless, this analysis is limited by its retrospective and single-centre design which may have introduced selection bias. Moreover, continuous ECG monitoring was not automated and it is possible that some AF diagnoses may have been missed. Also, the diagnosis of paroxysmal AF may have been missed in patients who died early after admission or in patients with very severe stroke and extreme disability for whom the family may have considered any further diagnostic examinations as futile. In addition, other potential confounders were not systematically assessed such as crossover treatment allocations, adherence, persistence to treatment strategies, and confounding by indication.
In conclusion, the trends of the characteristics and outcomes of acute ischemic stroke patients with AF during the 1993–2012 period have been promising but still far from ideal. This highlights the need to continue investing on stroke education and management as a means to address the unmet needs associated with AF and stroke. Recent developments in anticoagulant treatment, AF detection techniques, and recanalization strategies may lead to further improvement of outcomes in acute ischemic stroke patients with AF.
Supplemental Material
Supplementary Table -Supplemental material for 20-year trends of characteristics and outcomes of stroke patients with atrial fibrillation
Supplemental material, Supplementary Table for 20-year trends of characteristics and outcomes of stroke patients with atrial fibrillation by George Ntaios, Dimitrios Sagris, Fotios Gioulekas, Petros Galanis, Christianna Pardali, Anastasia Vemmou, Eleni Koroboki, Vasileios Papavasileiou, Sofia Vassilopoulou, Efstathios Manios, Konstantinos Makaritsis, Konstantinos Spengos, Dimos-Dimitrios Mitsikostas, Haralambos Milionis and Konstantinos Vemmos in International Journal of Stroke
Footnotes
Author contributions
George Ntaios: study concept, statistical analysis and interpretation, preparation of manuscript, study supervision. Dimitrios Sagris: statistical analysis and interpretation, preparation of manuscript, critical revision of the manuscript. Fotios Gioulekas: statistical analysis, preparation of manuscript, critical revision of the manuscript. Petros Galanis: statistical analysis. Christianna Pardali: data collection, critical revision of the manuscript. Anastasia Vemmou: data collection, critical revision of the manuscript. Eleni Koroboki: data collection, critical revision of the manuscript. Vasileios Papavasileiou: statistical analysis and interpretation, critical revision of the manuscript. Sofia Vassilopoulou: data collection, critical revision of the manuscript. Efstathios Manios: data collection, critical revision of the manuscript. Konstantinos Makaritsis: data collection, critical revision of the manuscript. Konstantinos Spengos: data collection, critical revision of the manuscript. Dimos-Dimitrios Mitsikostas: critical revision of the manuscript. Haralambos Milionis: critical revision of the manuscript. Konstantinos Vemmos: data collection, statistical analysis and interpretation, preparation of manuscript, study supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.