
Abstract
Background
Epilepsy is a common complication of pediatric stroke.
Aim
In this study, we aim to measure the association between epilepsy and neurologic outcome after childhood arterial ischemic stroke.
Methods
Prospective cohort study of children (29 days–19 years) enrolled after an acute arterial ischemic stroke at 21 international pediatric stroke centers and followed to identify epilepsy. One year post-stroke, outcomes were scored using the examination-based Pediatric Stroke Outcome Measure (range = 0–10); higher values reflect greater disability. Ordinal logistic regression was used to measure the association of Pediatric Stroke Outcome Measure scores (categorized as 0–1, 1.5–3, 3.5–6, 6.5–10) with epilepsy.
Results
Investigators enrolled 86 children (median age = 6.1 years, interquartile range (IQR) = 1.4–12.2 years) with acute stroke. At 1 year, 18/80 (23%) remained on an anticonvulsant including 8/80 (10%) with epilepsy. Among the 70 with Pediatric Stroke Outcome Measure scored, the median was 0.5 (IQR = 0–1.5) for children without epilepsy (n = 63), and 6 (IQR = 0.5–10) for children with epilepsy (n = 7). In univariable analyses, poorer 1-year outcome was associated with middle cerebral artery stroke, cortical infarcts, hemorrhagic transformation, hospital disposition not to home, and epilepsy. In multivariable analysis, middle cerebral artery stroke (odds ratio (OR) = 4.9, 95% confidence intervals (CI) = 1.1–21.3) and epilepsy (OR = 24.1, CI = 1.5–380) remained associated with poorer outcome.
Conclusions
Children who developed epilepsy during the first year post-stroke had poorer neurologic outcomes than those without epilepsy.
Introduction
Epilepsy is a common complication of pediatric stroke, with a 10-year cumulative incidence of approximately 30% among childhood stroke survivors. 1 Children with post-stroke epilepsy have worse parent-reported health status 2 and performance on cognitive testing compared to those without post-stroke epilepsy.3,4 However, the relationship of post-stroke epilepsy with children’s neurologic function is complex and poorly understood. Our hypothesis was that children with post-stroke epilepsy have worse neurologic outcomes than those without epilepsy. We aimed to prospectively measure the effects of infarct characteristics, anticonvulsants, and epilepsy on childhood arterial ischemic stroke (AIS) outcomes.
Methods
Seizures in Pediatric Stroke (SIPS) investigators enrolled children aged 29 days–19 years with acute AIS and identified seizures during the first year post-stroke as previously described. 5 At 1 year, neurologists examined children to score outcomes using the Pediatric Stroke Outcome Measure (PSOM). All sites obtained ethics approval from local institutional review boards. Guardians provided written consent.
Epilepsy was defined as at least one unprovoked seizure occurring > 1 month after stroke in accordance with the International League Against Epilepsy and the International Bureau for Epilepsy. 6 Total PSOM scores are the sum of five subscales (right and left sensorimotor, language production, language comprehension, cognitive/behavioral) scored after neurologic examination (0 no deficit, 0.5 minor exam abnormality detectable with no impact on function, 1 deficit impairs function, and 2 at least one function is missing). 7 A higher score indicates greater impairment. Investigators reported infarct characteristics from clinically obtained imaging.
Statistics
PSOM scores were categorized 0–1, 1.5–3, 3.5–6, 6.5–10 as in prior studies. 8 We used ordinal logistic regression to determine the association of predictor variables with outcome and reported common odds ratios (OR) as a measure of effect size (the odds of a worse PSOM category in one group of children compared to another). For multivariable analysis, we included variables associated with outcome at a level of P < 0.1.
Results
Investigators enrolled 86 children (Figure 1). Cohort characteristics (online Supplementary Table 1) were similar to the previously published SIPS cohort that included neonatal AIS.
5
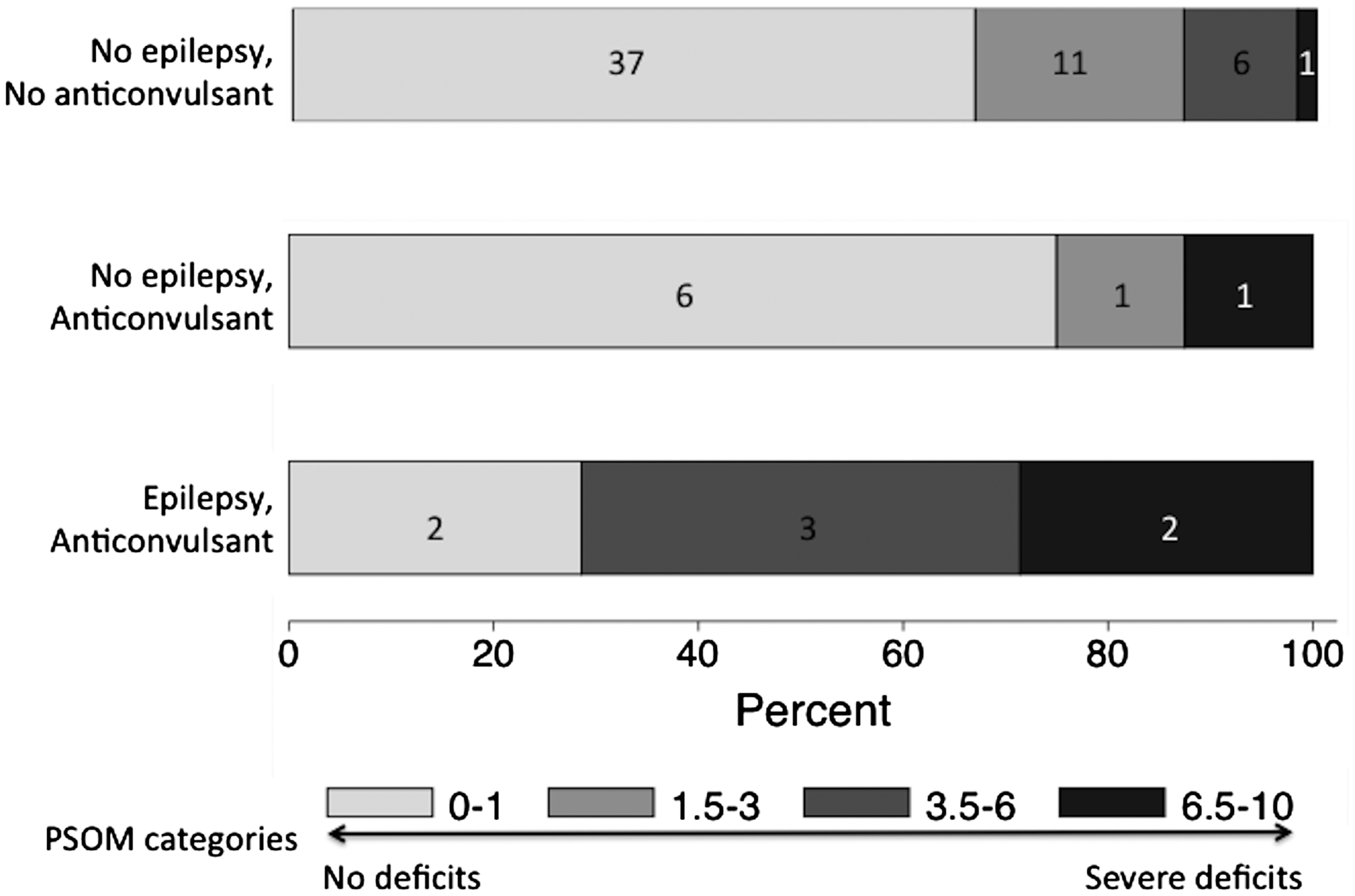
Follow-up data were available for 80 children (4 deceased, 2 lost to follow-up) at a median of 12.1 months (interquartile range (IQR) = 11.4–12.9) post-stroke. At 1 year, 18/80 (23%) were taking a maintenance anticonvulsant including 8/80 (10%) who met our definition of epilepsy. No child discharged from the stroke hospitalization without anticonvulsant treatment developed epilepsy during the first year. Among 70 with PSOM scored, the median was 0.5 (IQR = 0–1.5) for children without epilepsy (n = 63), and 6 (IQR = 0.5–10) for the children with epilepsy (n = 7). The distribution of PSOM scores among children with epilepsy, children without epilepsy but treated with anticonvulsant, and those without epilepsy or anticonvulsant treatment are shown in Figure 2.
Flow diagram of the childhood stroke cohort followed 1 year. Distribution of PSOM scores stratified by the presence of epilepsy and ongoing treatment with an anticonvulsant 1 year post-stroke. Percent is shown on the y-axis, with frequency counts in boxes representing each category.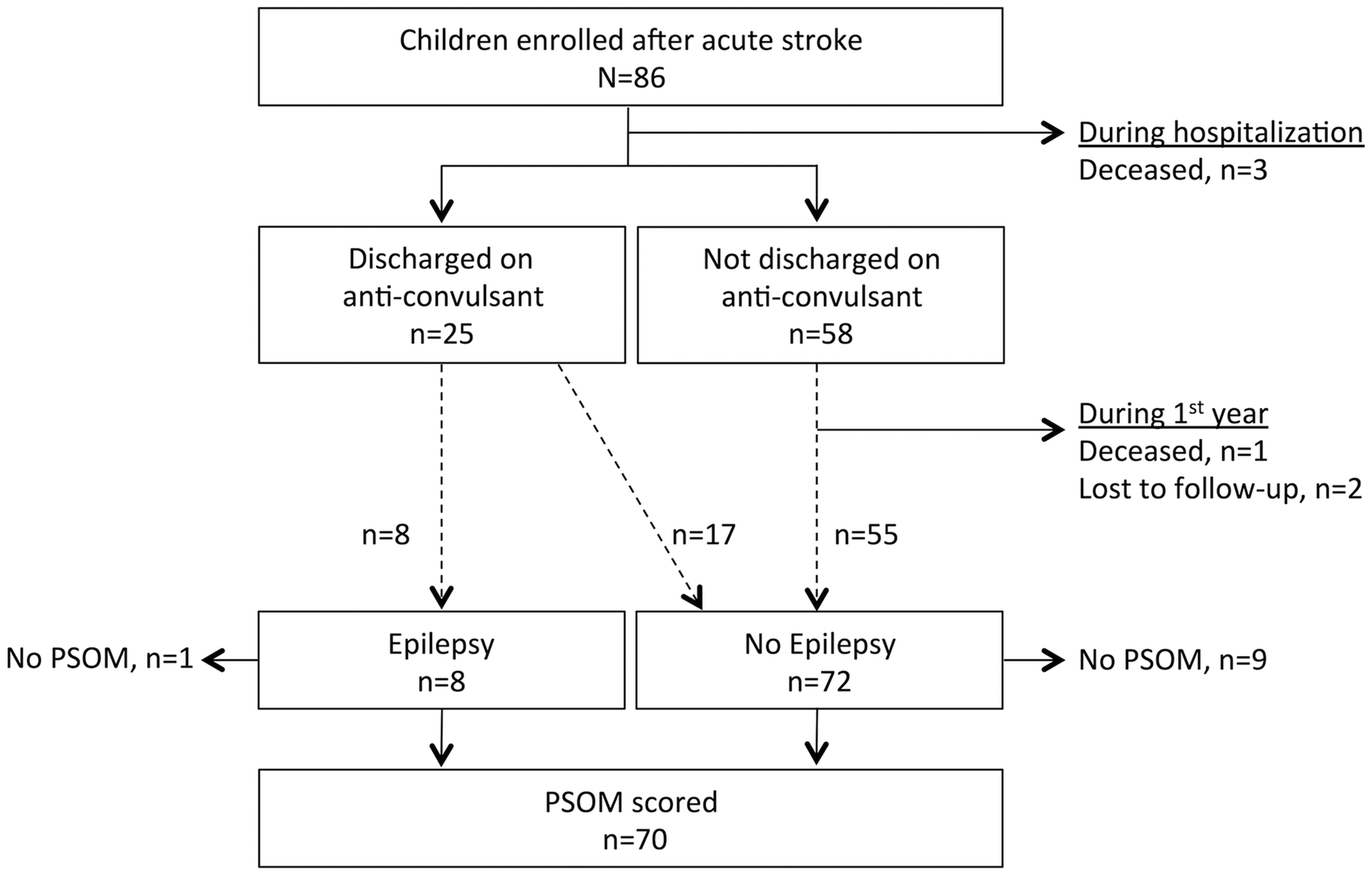
In unadjusted analyses, middle cerebral artery (MCA) territory infarct, cortical location, hemorrhagic transformation, and epilepsy at 1 year were each associated with poorer outcome, while disposition to home was associated with better outcome (online Supplementary Table 1). In our multivariable analysis, we included each of these variables and also included variables for a longer duration of acute seizures, discharge from the stroke hospitalization on an anticonvulsant and anticonvulsant use at 1 year. In the multivariable model, only MCA stroke (OR = 4.9, confidence interval (CI) = 1.1–21.3) and epilepsy (OR = 24.1, CI = 1.5–380) remained associated with higher PSOM scores.
Discussion
Among pediatric AIS survivors, outcomes were worse among children who developed epilepsy during the first year post-stroke. Epilepsy was strongly associated with the poorer neurologic outcome even after adjusting for infarct characteristics, anticonvulsants, and other potential confounders.
The implication of a median PSOM of 0.5 in our study and a similar median 1-year PSOM of 0.75 in a United Kingdom pediatric AIS cohort 9 is that children’s recovery after stroke is generally good. A PSOM of 0.5 indicates a deficit detectable in a single domain without functional impairment. In comparison, the subgroup of children with post-stroke epilepsy had a median PSOM of 6, indicating impaired or missing function in multiple domains.
Extensive brain injury may worsen outcomes and separately increase epilepsy risk. Infarct size has been related to neurologic outcome after childhood stroke 8 and is a predictor of epilepsy after neonatal stroke. 10 A second possible explanation for the association between epilepsy and the neurologic outcome is that anticonvulsants could affect outcomes. While we did not find evidence for this, we observed a wide variation in anticonvulsant choice and duration of treatment that could mask an existing association. A third possibility is that epileptogenesis or the seizures that are generated could be detrimental to recovery. How a neural network in a person evolves to become seizure prone remains largely unknown. The latency period before the onset of post-stroke epilepsy provides an opportunity to study epileptogenesis, its affect on stroke recovery in children and the possibility of developing an intervention to improve outcome. 11
The lack of measured infarct size and PedNIHSS at stroke onset to measure severity is a limitation of our study, but to account for degree of brain injury we controlled for other infarct characteristics (MCA territory, hemorrhagic transformation, cortical location) and other markers of initial stroke severity (acute seizure duration, hospital disposition). Our study is also limited by the small number of outcomes, the possibility of confounding by indication for anticonvulsant treatment and a lack of electroencephalogram data.
Summary
Post-stroke epilepsy is associated with poorer 1-year outcomes among childhood AIS survivors. While insufficient to determine causality, this association warrants further investigation.
Supplemental Material
Supplementary table -Supplemental material for Children with post-stroke epilepsy have poorer outcomes one year after stroke
Supplemental material, Supplementary table for Children with post-stroke epilepsy have poorer outcomes one year after stroke by Christine K Fox, Lori C Jordan, Lauren A Beslow, Jennifer Armstrong, Mark T Mackay, Gabrielle deVeber and on behalf of the SIPS Investigators in International Journal of Stroke
Footnotes
Authors’ contributions
Drs Fox, Mackay, and deVeber contributed to study design. Dr Fox performed statistical analyses and drafted the manuscript. Drs Fox, Jordan, Beslow, Armstrong, Mackay, and deVeber substantially contributed to the acquisition and interpretation of data; critically reviewed and revised it for important intellectual content, approved the final work and have participated sufficiently to take responsibility for the content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Pediatric Epilepsy Research Foundation (112010-007), the NIH (2K12NS001692-11 and KL2TR000143), and the Auxilium Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.