
Abstract
Background
Stroke survivors sit for long periods each day. Uninterrupted sitting is associated with increased risk of cardiovascular disease. Breaking up uninterrupted sitting with frequent, short bouts of light-intensity physical activity has an immediate positive effect on blood pressure and plasma clotting factors in healthy, overweight, and type 2 diabetic populations.
Aim
We examined the effect of frequent, short bouts of light-intensity physical activity on blood pressure and plasma fibrinogen in stroke survivors.
Methods
Prespecified secondary analyses from a three-armed randomized, within-participant, crossover trial. Participants were 19 stroke survivors (nine female, aged 68 years old, 90% able to walk independently). The experimental conditions were sitting for 8 h uninterrupted, sitting with 3 min bouts of light-intensity exercise while standing every 30 min, or sitting with 3 min of walking every 30 min. Blood pressure was measured every 30 min over 8 h and plasma fibrinogen at the beginning, middle, and end of each day. Intention-to-treat analyses were performed using linear mixed models including fixed effects for condition, period, and order, and a random intercept for participant to account for repeated measures and missing data.
Results
Sitting with 3 min bouts of light-intensity exercise while standing every 30 min decreased systolic blood pressure by 3.5 mmHg (95% CI 1.7–5.4) compared with sitting for 8 h uninterrupted. For participants not taking antihypertensive medications, sitting with 3 min of walking every 30 min decreased systolic blood pressure by 5.0 mmHg (95% CI −7.9 to 2.0) and sitting with 3 min bouts light-intensity exercise while standing every 30 min decreased systolic blood pressure by 4.2 mmHg (95% CI −7.2 to −1.3) compared with sitting for 8 h uninterrupted. There was no effect of condition on diastolic blood pressure (p = 0.45) or plasma fibrinogen levels (p = 0.91).
Conclusion
Frequent, short bouts of light-intensity physical activity decreases systolic blood pressure in stroke survivors. However, before translation into clinical practice, the optimal duration and timing of physical activity bouts needs to be determined.
Clinical trial registration
Australian and New Zealand Clinical Trials Registry http://www.anzctr.org.au ANZTR12615001189516.
Introduction
Hypertension is the predominant risk factor for both first and recurrent stroke.1–4 While pharmacological interventions are the mainstay of hypertension management, lifestyle modifications are recognized as an important aspect of long-term management.1,3,5 Hypertension is strongly associated with a sedentary lifestyle.6,7
Spending long periods of time sitting down each day has been associated with an increased risk of cardiovascular disease, mortality, and morbidity.8,9 A recent meta-analysis of over one million adults 10 found an exponential increase in risk of all-cause mortality and cardiovascular disease-related mortality in people who sat > 8 h/day and were also physically inactive (<5 min/day of at least moderate-intensity physical activity). Evidence indicates that stroke survivors fit this profile of high sitting time and very low physical activity,11,12 with average daily sitting time of up to 75% of waking hours, the majority of this sitting accumulated in long, unbroken bouts. Stroke survivors may be particularly vulnerable to the effects of high sitting time on cardiovascular disease with up to 40% suffering a recurrent stroke within 10 years. 13 The mechanisms by which prolonged sitting time exerts its negative effects are not fully understood but increased blood pressure is one possibility.14,15 In addition, long periods of sitting have been shown to increase plasma clotting factors, 16 which in turn increases the risk of ischemic stroke.17,18
Engaging in at least 10 min bouts of regular exercise of at least moderate intensity can reduce resting blood pressure. Decreases in systolic blood pressure of 1.8–10.9 mmHg and diastolic blood pressure of 2.5–6.2 mmHg as a result of regular exercise of at least moderate intensity have been reported for healthy and hypertensive adults, with isometric resistance exercise being most beneficial. 19 However, stroke survivors face considerable barriers to regular engagement in exercise.20,21 Self-report data from the North-East Melbourne Stroke Incidence Study show that only 18% of stroke survivors are exercising regularly at five years after stroke. 22
Reducing time spent in uninterrupted sitting by introducing frequent short bouts of light-intensity physical activity during the day may be an alternative therapeutic target rather than, or in addition to, a program of moderate-intensity exercise. Decreases in resting blood pressure have been seen with frequent (every 20–60 min), short (2–3 min) bouts of light-intensity physical activity in overweight/obese 14 and type 2 diabetic 23 populations. Alternating 30 min of sitting with 30 min of standing in prehypertensive office workers also decreases resting blood pressure. 24 Interrupting sitting time with frequent, short bouts of light-intensity physical activity has also been shown to attenuate the rise in plasma clotting factors associated with long periods of uninterrupted sitting. 16
We therefore investigated the immediate effect of breaking up uninterrupted sitting with frequent, short bouts of light-intensity physical activity on metabolic and cardiovascular markers in stroke survivors. 25 In this paper, we report the effects on resting blood pressure and plasma fibrinogen concentrations. Our specific research question was:
Do frequent (every 30 min), short (3 min), bouts of light-intensity physical activity (either exercising while standing or walking) have an immediate (within one day) effect on resting blood pressure and/or plasma fibrinogen levels?
Method
Design
This paper reports predefined secondary outcomes from the Breaking Up Sitting Time after Stroke (BUST-Stroke) study,
25
a randomized, crossover trial (Figure 1). Stroke survivors were recruited from stroke support groups and outpatient services within the Hunter New England Health District. The study was conducted in a supervised laboratory setting at the Hunter Medical Research Institute (Newcastle, Australia). Participants sat for 8 h/day under three conditions: 8 h of uninterrupted sitting (SIT), 3 min bouts of light-intensity exercises in standing every 30 min (STAND-EX), or 3 min of walking every 30 min (WALK). The order of the conditions was randomized. Participants fasted overnight and abstained from caffeine, alcohol, and exercise (at moderate-to-vigorous intensity) for the 48 h prior and standardized meals were provided for breakfast and lunch. To control for differences in plasma volume, water intake was matched across conditions. Outcomes were measured across the day by a researcher not blinded to condition. There was a minimum four-day washout period between conditions. Outcomes were measured across the day during each experimental condition. The trial was registered (ANZTR 12615001189516), the full protocol published,
25
ethical approvals from Hunter New England Health District (#15/10/21/4.05) and University of Newcastle Human Research Ethics Committees (#H-2015-0437) granted. Written informed consent was obtained from all participants.
Flow of participants through the study showing condition order. *One participant did not complete the exercises while standing condition (STAND-EX) due to repeated cannulation failure. SIT: sitting for 8 h uninterrupted; STAND-EX: sitting with 3 min of light-intensity exercise while standing every 30 min; WALK: sitting with 3 min of walking every 30 min.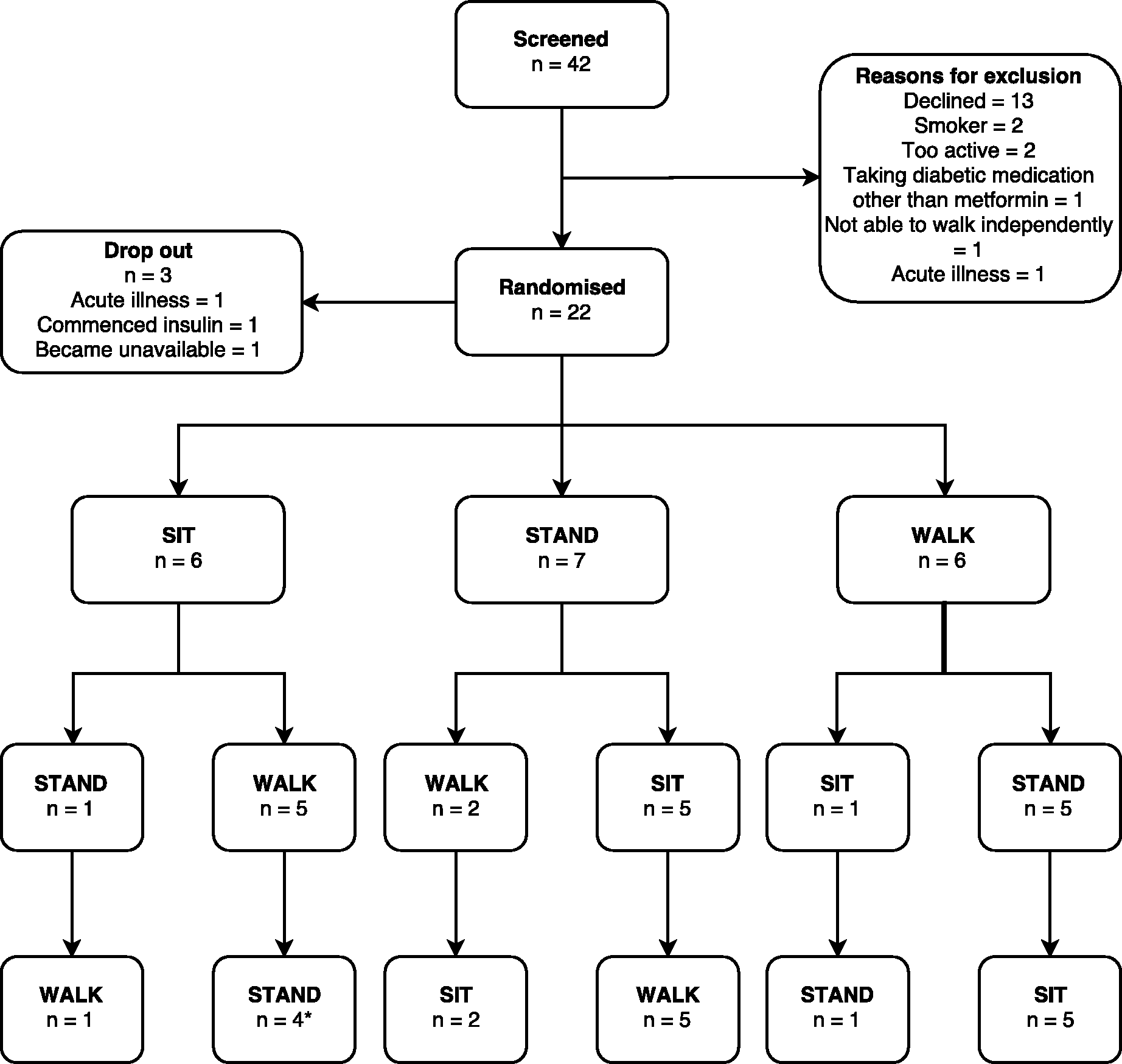
Participants
Stroke survivors were eligible for the study if they were > 3 months and < 10 years after stroke and able to walk with minimal assistance (functional ambulation classification ≥ 2). They were excluded if they self-reported sitting <4 h/day, self-reported carrying out moderate-to-vigorous physical activity >150 min/week, had a body mass index >45 kg/m2, and/or were taking diabetic medication other than metformin. Participant demographic and clinical information was collected in order to describe the sample.
Experimental conditions
The three experimental conditions were 8 h of uninterrupted sitting (SIT), 3 min bouts of light-intensity exercise while standing (marching on spot, small amplitude squats, calf-raises) every 30 min (STAND-EX), and 3 min bouts of light-intensity walking every 30 min (WALK). To confirm that the STAND-EX and WALK conditions met the definition of light-intensity physical activity, heart rate (using a pulse oximeter) and ratings of self-perceived exertion (BORG 0–10 scale) were measured immediately after each activity bout. To confirm that participants had not changed their activity level during the four days preceding each experimental condition, activity was monitored using an activPAL3 (PAL Technologies Ltd) activity monitor which contains a triaxial accelerometer and inclinometer, and is highly accurate in measurement of sitting and standing postures in people with stroke. 26 This small, lightweight monitor was waterproofed and worn attached to the anterior thigh on the nonparetic limb for 24 h/day for the four days preceding each condition and during each experimental day.
Outcome measures
Outcomes were systolic and diastolic blood pressure and plasma fibrinogen concentration. Resting blood pressure was measured using a Welch Allyn Connex 6700 Vital Signs monitor at the beginning of the day and at 30 min intervals thereafter, immediately prior to activity bouts (STAND-EX and WALK). Measurements were taken in the seated position on the arm contralateral to the intravenous catheter and on the same arm for each measurement. Two blood pressure readings were taken approximately 2 min apart. The second measure was recorded and used in analyses.
Plasma fibrinogen was measured from blood samples taken at the beginning (9 am), middle (12 pm), and end of the day (3 pm) in a 4 ml sodium citrate collection tube from an intravenous cannula inserted at the beginning of the day. Blood samples were refrigerated immediately, centrifuged between >1 and < 2 h postcollection, aliquoted and stored at −80°. Fibrinogen was analyzed by a hospital-based pathology service using the Clauss fibrinogen assay in duplicate.
Statistical analysis
The study was powered to detect differences in postprandial glucose and insulin concentrations, as specified in the published protocol. 25 A statistical analysis plan was prepared a priori. Differences between experimental conditions for systolic and diastolic blood pressure, and plasma fibrinogen were analyzed by intention to treat, using linear mixed models including fixed effects for condition, period, and order, and a random intercept for participant to account for repeated measures. In separate analyses, we examined the influence of prespecified effect modifiers on blood pressure (including habitual sitting time, body mass index, sex, and walking speed) by adding interaction terms between condition and the effect modifier (along with main effects). Finally, subgroup analyses were performed to examine the effect of condition on systolic blood pressure in patients with and without hypertension. All analyses were undertaken in SPSS version 23; significance was set at p < 0.05 (two tailed).
Flow of participants through the study
Participant characteristics
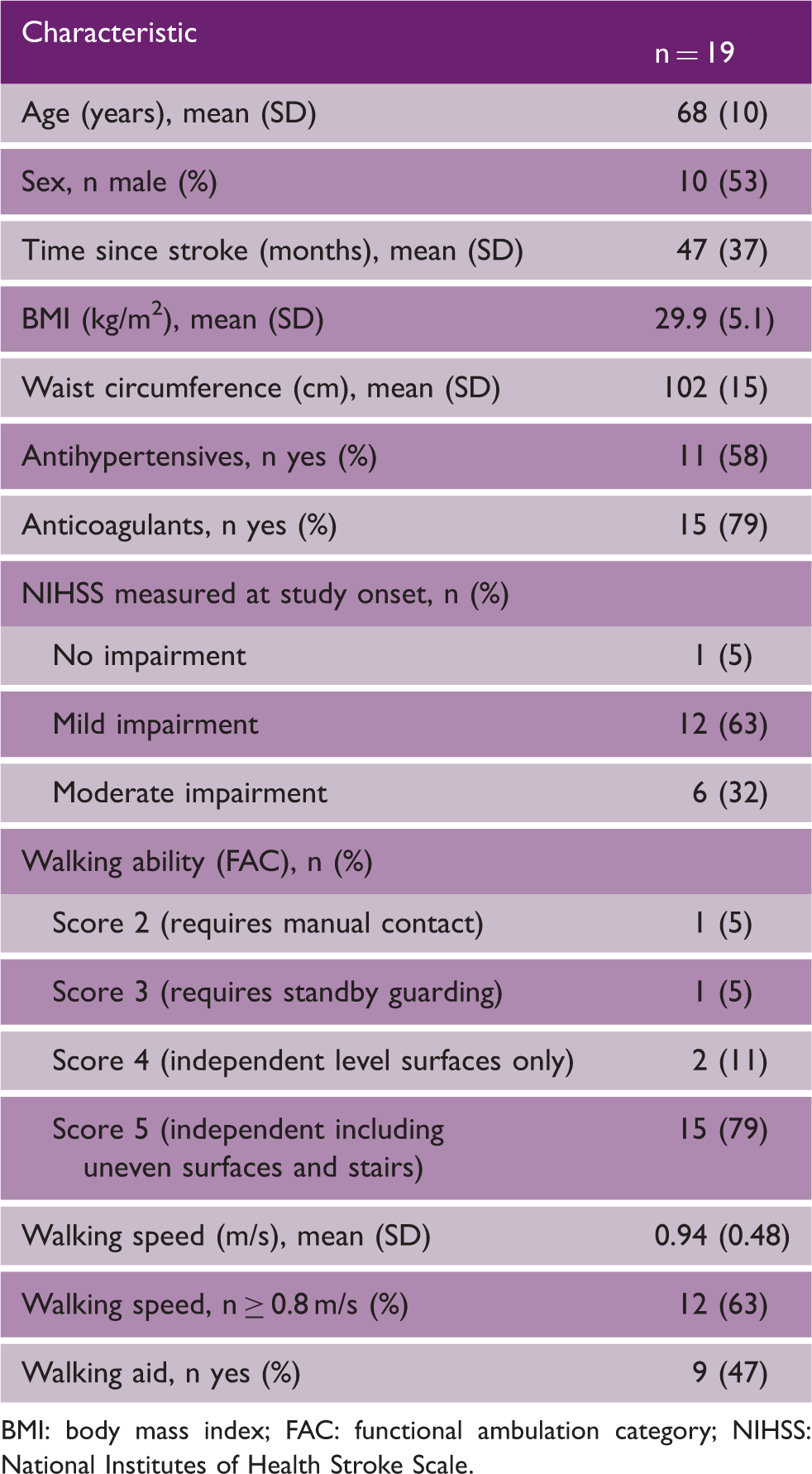
BMI: body mass index; FAC: functional ambulation category; NIHSS: National Institutes of Health Stroke Scale.
Compliance with trial method
Participants did not alter their activity levels over the course of the trial. The mean stepping time per day over the four days prior to the first condition undertaken by each participant was 70 (SD 39) min and this did not change during the washout period between conditions one and two (63 (SD 36) min) or the washout period between conditions two and three (64 (SD 36) min, p = 0.66). Participants were continuously supervised during the experimental days and complied fully with the protocol, completing all activity breaks as scheduled. Objective data from the activPAL monitor confirm this with average sitting time during the SIT, STAND-EX, and WALK conditions of 7.6 (SD 2.1), 7.5 (SD 0.6), and 7.2 (SD 1.0) hours, respectively.
Mean (SD) of measures of compliance collected at the end of each activity averaged across the day for each condition (n = 19)
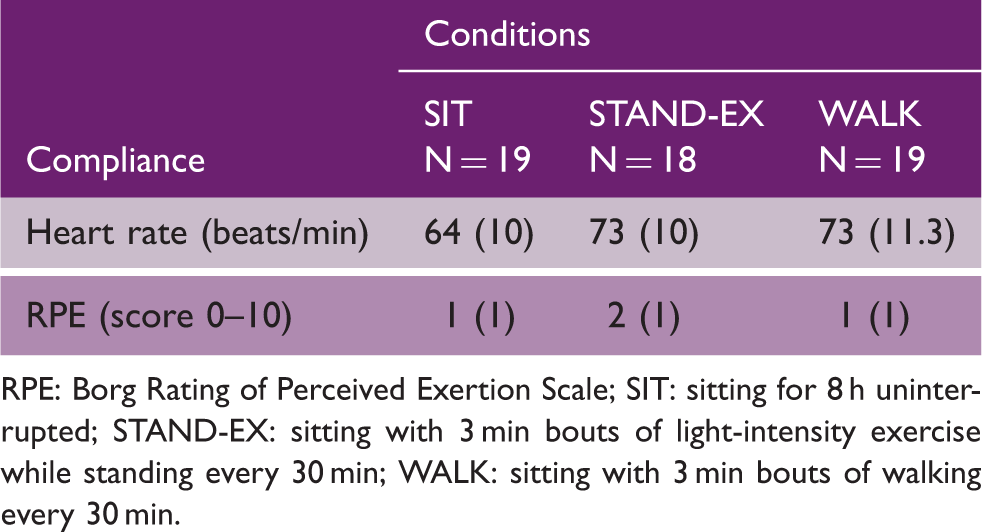
RPE: Borg Rating of Perceived Exertion Scale; SIT: sitting for 8 h uninterrupted; STAND-EX: sitting with 3 min bouts of light-intensity exercise while standing every 30 min; WALK: sitting with 3 min bouts of walking every 30 min.
Effect of experimental conditions
Estimated marginal mean (SE) of outcomes (averaged across the day for each condition) and mean (95% CI) difference between conditions (n = 19); from linear mixed modeling
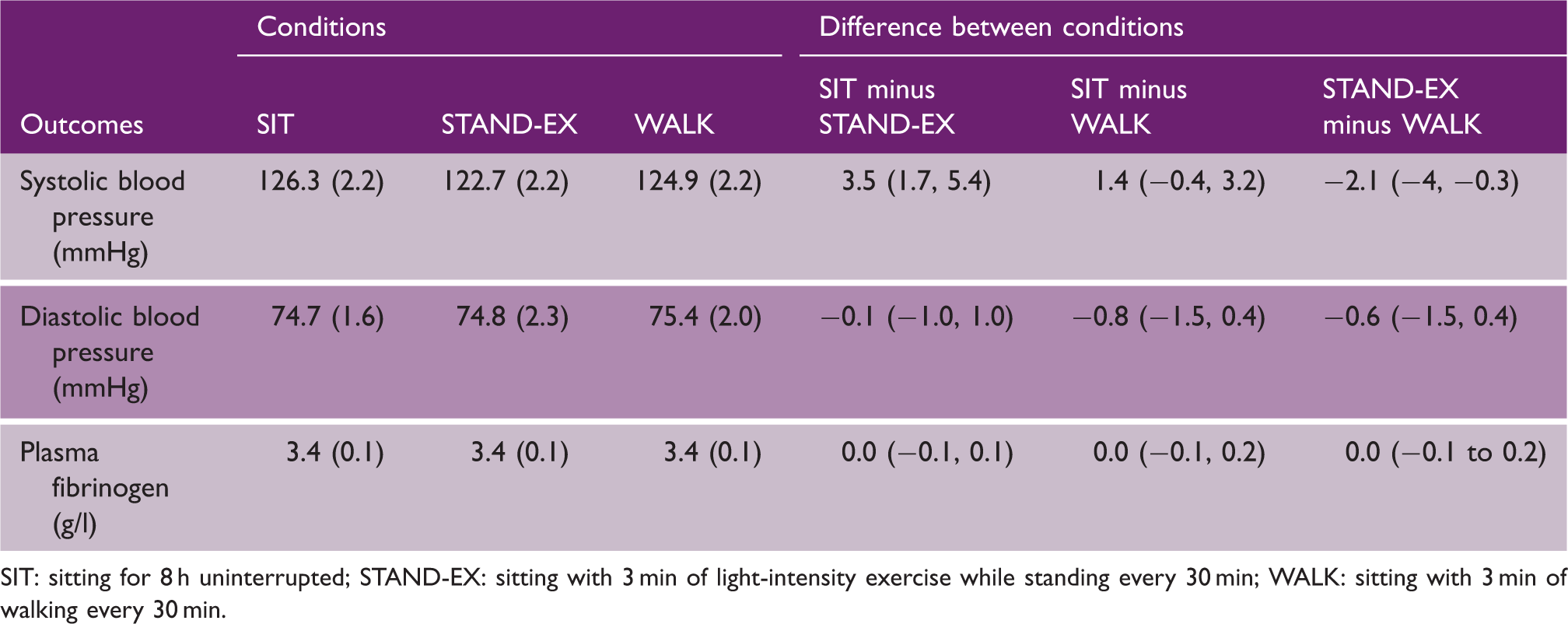
SIT: sitting for 8 h uninterrupted; STAND-EX: sitting with 3 min of light-intensity exercise while standing every 30 min; WALK: sitting with 3 min of walking every 30 min.
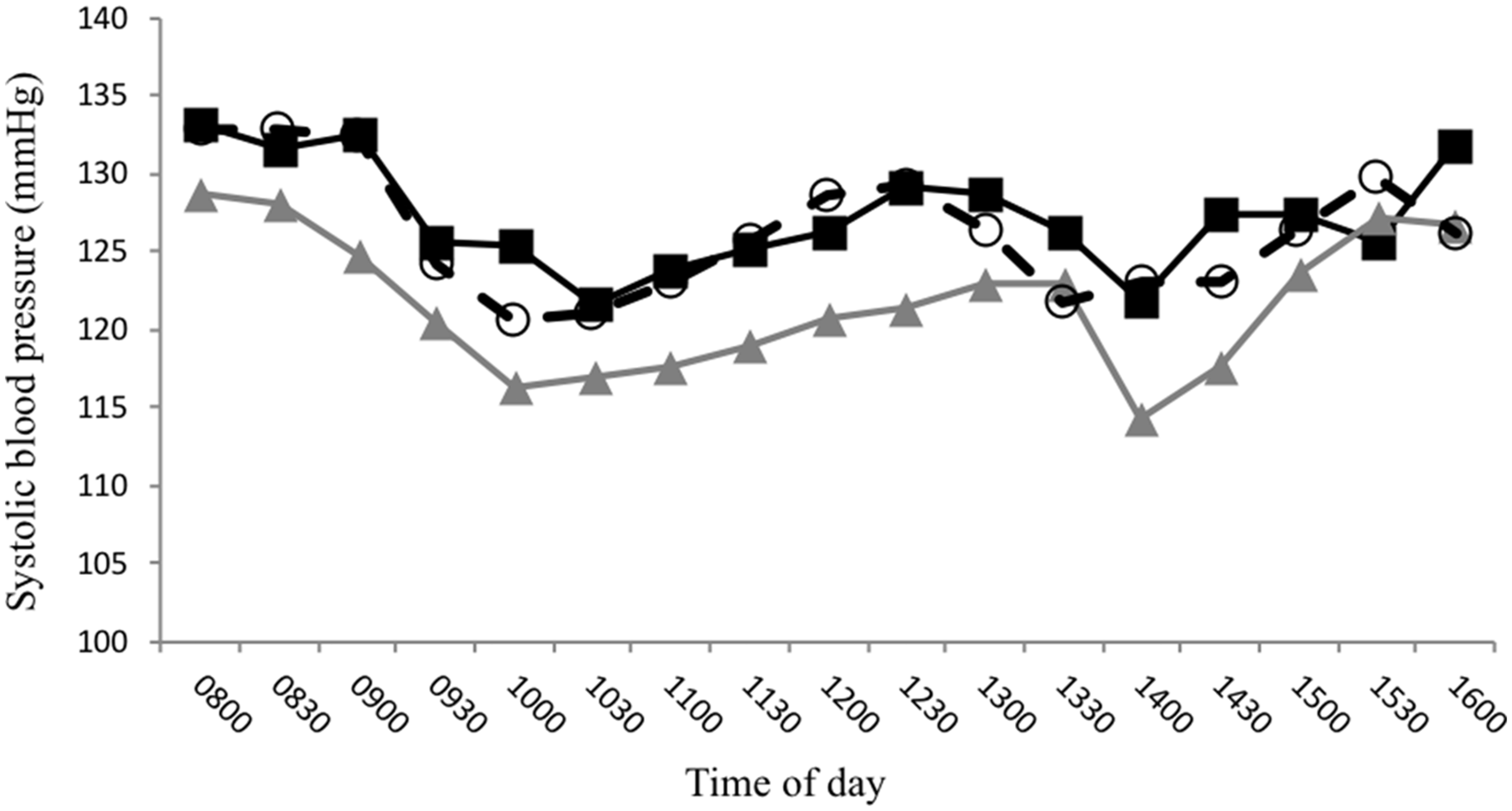
Mean systolic blood pressure in mmHg across the day for the (a) SIT (open circles), (b) STAND-EX (triangles), and (c) WALK (closed squares) conditions.
Antihypertensive medication modified the effect of STAND-EX and/or WALK (p = 0.006) but walking speed (p = 0.145), habitual daily sitting time (p = 0.733), body mass index (p = 0.897), and sex (p = 0.450) did not. For participants not taking antihypertensive medications (n = 8, 42%), WALK decreased systolic blood pressure by 5.0 mmHg (95% CI −7.9 to 2.0) and STAND-EX decreased systolic blood pressure by 4.2 mmHg (95% CI −7.2 to −1.3) compared with SIT. For participants taking antihypertensive medications (n = 11, 58%), only STAND-EX decreased systolic blood pressure by −3.4 mmHg (95% CI −5.7 to −1.0).
Discussion
In ambulatory chronic stroke survivors, we observed that frequent, short bouts of light-intensity exercises while standing decreased systolic blood pressure, regardless of whether participants were taking antihypertensive medication or not. In addition, frequent, short bouts of light-intensity walking decreased systolic blood pressure in those stroke survivors who were not taking antihypertensive medication. Neither exercising while standing nor walking decreased diastolic blood pressure or plasma fibrinogen levels.
The activity bouts consisted of 3 min of either exercising while standing or walking at light intensity, every 30 min. Each condition was closely supervised, ensuring that the activity bouts were carried out. Furthermore, heart rate and perceived effort both increased modestly, confirming that the activity bouts were performed at light intensity. The participants were mildly disabled; 90% of them walked independently with 63% walking at speed consistent with the ability to ambulate in the community. 27 In our participants, blood pressure was largely controlled and near normal when averaged across the day; 60% of the participants were taking antihypertensive medication. Importantly, we found the benefit of light-intensity exercises while standing persisted regardless of whether participants were taking antihypertensive medication or not. Therefore, frequent, short bouts of light-intensity physical activity may play an important role in long-term blood pressure management. We know that regular engagement in moderate-to-vigorous intensity exercise has been shown to be associated with a 5 mmHg reduction in systolic blood pressure in people with stroke. 28 Our findings suggest that frequent, short bouts of light-intensity physical activity across the day could provide similar benefit. Furthermore, this approach may be achievable for stroke survivors, given that meeting recommended moderate-to-vigorous physical activity levels is difficult for stroke survivors.20–22
The magnitude of systolic blood pressure reduction observed in our study (3–5 mmHg) is commensurate to that found in studies involving similar experimental conditions in overweight/obese 14 and type 2 diabetic 23 populations. Importantly, it is also of clinical relevance. A meta-analysis of 10 trials of blood pressure-lowering agents for secondary stroke prevention found a 5.1 mmHg reduction in systolic blood pressure was associated with a 22% reduction in the odds of having a stroke. Furthermore, there is strong evidence for the linear relationship between lower blood pressure and reduced stroke risk,1,29 with no evidence of a J-curve.
In line with the findings of Dempsey et al., 23 we found light-intensity exercises in standing more effective than walking for decreasing systolic blood pressure. This suggests that the intensity of the activity undertaken during the bouts may be important. In studies where participants have broken up uninterrupted sitting time with static standing, decreases in blood pressure have been smaller. 24 The light-intensity exercises while standing in our study (marching on spot, small amplitude squats, calf-raises) are likely to have recruited larger muscle groups than walking only. As such, the exercises may have been similar to resistance exercises, which have a greater hypotensive effect compared with aerobic exercise. 19
Long periods of uninterrupted sitting leads to a rise in plasma clotting factors such as fibrinogen. 16 Frequent, short bouts of light-intensity physical activity attenuate this rise in clotting factors in overweight/obese 16 populations. Fifteen (79%) of our participants were taking regular anticoagulant medication, which may explain why we did not see a rise in plasma fibrinogen levels during the uninterrupted sitting condition, or a difference between conditions.
The main strength of our study was the high internal validity and controlling for potential confounding variables. The order of the experimental conditions was randomized, the amount of water consumed during the day was kept constant to prevent potential differences in plasma volume, and the activity bouts were closely supervised. The processing and analyses of fibrinogen blood samples were blinded to condition, but the measurement of blood pressure was not. We measured blood pressure twice and recorded the second measurement. The American Heart Association Guidelines 30 recommend using an average of two measurements. However, our methods for measuring blood pressure were consistent for all participants and conditions. In this study, we were interested in within-participant differences in blood pressure between conditions, meaning that absolute values were less important. The average baseline systolic blood pressure was inexplicably lower for the STAND-EX condition compared with other conditions; however, we adjusted for this in the statistical models. Measurement of fibrinogen concentrations involved intravenous cannulation and blood draws, and as such may have induced a stress response that could have influenced blood pressure measures. However, the crossover design of the trial, the random allocation of the condition order, and the controlling for condition order in the statistical analyses should have accounted for this. This study was powered for the primary outcomes of glucose and insulin and may have been underpowered to detect between-group differences in blood pressure and plasma fibrinogen. It is possible that with a larger sample size the reduction in systolic blood pressure during the walking condition relative to the sitting condition (mean difference 1.4 mmHg (95% CI 0.4–3.2)) may have been statistically significant. However, in the case of the diastolic blood pressure and fibrinogen data, the small between-group differences and largely symmetrical confidence intervals suggest that larger sample sizes would be unlikely to result in between-group differences in these outcomes. In other words, we can be confident that our results represent a true effect, rather than a lack of statistical power.
The magnitude of the decrease in systolic blood pressure of 3–4 mmHg is promising and of clinical relevance, given the strong linear relationship between blood pressure and risk of stroke. 1 However, matching the frequency and duration of the activity bouts used in this study (strictly 3 min of activity every 30 min) is unlikely to be feasible and sustainable in everyday life. The next step is to test more practicable doses of frequent, short bouts of light-intensity physical activity and whether the effect is maintained in the long term, and this is underway (ACTRN12617001517369).
Footnotes
Author’s note
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank all participants involved and Professor Louise Ada for her assistance in manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a Stroke Foundation of Australia Seeding Grant (2015) and John Hunter Hospital Charitable Trust Grant (2016). Associate Professor English was supported by National Heart Foundation Future Leaders Fellowship (#101177). Prof Dunstan was supported by an NHMRC Senior Research Fellowship (NHMRC #1078360). Prof Bernhardt was supported by a National Health and Medical Research Council Established Research Fellowship (#1058635). The Florey Institute of Neuroscience and Mental Health and Baker Institute acknowledge the Victorian State Government’s Operational Infrastructure Support Program.