
Abstract
Background
Statins are important components of secondary stroke prevention, but there is a concern they may increase the risk of intracerebral hemorrhage. Although this risk may have been overestimated, there is still an open question whether statin therapy should be continued, or even initiated, in patients who have had a recent intracerebral hemorrhage.
Aim
Our aim was to investigate the risk of statin use after an intracerebral hemorrhage with respect to recurrent intracerebral hemorrhage, stroke in general, and death.
Methods
This observational study was based on patients with a first intracerebral hemorrhage in 2004 through 2009. Clinical characteristics, index intracerebral hemorrhage, and recurrent intracerebral hemorrhages were identified by the Swedish Stroke Register; additional data on comorbidities and vital status were retrieved through record linkages to national registers. A propensity score for the likelihood of receiving statins at discharge was developed and used with other established risk factors in a multivariable analysis.
Results
Of 6082 intracerebral hemorrhage patients (mean age 69.6 years), 1097 (18%) were prescribed statins at discharge. During the follow-up (mean 3.1 years), 1434 (23.6%) deaths and 234 (3.8%) recurrent intracerebral hemorrhages were observed. Statin therapy was associated with a reduced risk of death (adjusted hazard ratio: 0.71; 95% confidence interval: 0.60–0.84) but not with the risk of recurrent intracerebral hemorrhage (adjusted hazard ratio: 0.82; 95% confidence interval: 0.55–1.22).
Conclusions
This study provides some reassurance that statins may be safe to use, in at least some patients, after an intracerebral hemorrhage. In patients with intracerebral hemorrhage, statin use was associated with a reduced risk of death, without an increased risk of recurrent intracerebral hemorrhage.
Introduction
Although statins are established components of secondary stroke prevention, 1 there is a concern that they may be associated with intracerebral hemorrhage (ICH). The only randomized clinical trial analyzing statin therapy in secondary stroke prevention, The Stroke Prevention by Aggressive Reduction in Cholesterol Levels 2006, identified an excess risk of ICH associated with statin administration, with 55 hemorrhagic events in the statin group and 33 in the placebo group. 2 A 2009 Cochrane review found an increased risk for ICH in patients who were on statins as secondary preventives, 3 while a later 2012 meta-analysis covering 31 randomized controlled trials found no significant increase of ICH. 4 Today, the risk for ICH with statin use after ischemic stroke has been de-emphasized. 5
However, a controversy still exists in whether statins are beneficial when used in patients who have had a recent ICH. 6 Two meta-analyses published in 2015 suggest statins to have a beneficial effect on survival and functional outcome in patients with ICH.7,8 Many of the included studies were small, and there were substantial between-study variations, leading to unresolved heterogeneity. Moreover, possible selection bias could not be completely ruled out, as healthier patients more often were prescribed statins. 7
In order to investigate an uncommon outcome as recurrent ICH, a large number of subjects is needed. The Swedish health-care system provides an opportunity to follow large cohorts of stroke patients through record linkage of registers. The aim of this observational study was to investigate the risk of statin use after an ICH with respect recurrent ICH, stroke in general, and death. To reduce any selection bias related to the non-randomized design, we used a propensity score (PS) to balance the patient characteristics between statin users and non-users.
Materials and methods
Data sources
Three Swedish comprehensive data sources were linked through the 10-digit unique personal identification number assigned to each person living in Sweden. The main source was The Swedish Stroke Register (Riksstroke), a nationwide quality register for stroke care, 9 which includes data on approximately 96% of all stroke patients in Sweden. 10 Riksstroke served as source for index and recurrent ICH events and use of statins on admission and at discharge. Information on comorbid diseases was retrieved from The National Patient Register (NPR), 11 which includes data on diagnoses as International Classification of Diseases 10th revision (ICD-10) codes for all hospitalizations in Sweden since 1998. Information on the date and cause of death was provided by the Cause of Death Register (CDR), 12 which includes data on death certificates of all Swedish citizens. All analyses, performed in agreement with privacy legislation in Sweden, were approved by the Regional Ethical Review Board in Uppsala, Sweden (Reg. No. 2009/355). The linkage of data was approved and performed by the Swedish National Board of Health and Welfare. The linked database was subsequently managed by Uppsala University Hospital, Sweden.
Patients
This observational cohort consisted of adult ICH patients (identified by the ICD-10 code I61), registered in Riksstroke between April 2004 and June 2009, surviving discharge with at least 30 days. The 30-day wash-out period was chosen to minimize the impact of discrepancies in the dates derived from different registers, to reduce the influence of acute case fatality, as well as to reduce the influence of comorbidity, which may have influenced the decision to use statins. We excluded patients with previous stroke (ischemic or hemorrhagic), unknown status regarding statin use and variables essential for the calculation of the PS, as well as patients with extreme values (<0.05 or >0.995) on the PS. The decision to exclude recurrent strokes was based on the ambition to study a homogenous population of ICH patients and, as statins are used in secondary prevention after an ischemic stroke, to avoid confounding by indication.
Definitions and assessment of variables and outcomes
Riksstroke provided information on age, sex, level of consciousness on admission, living conditions, activities of daily living (ADL) before stroke, and use of antithrombotics and statins. Antithrombotics included warfarin (the only oral anticoagulant available in Sweden at that time) and antiplatelets (aspirin 91%).
Data on cardiovascular risk factors and comorbidities (i.e. diabetes (E10-14 and ICD-10), hypertension (I10), ischemic heart disease (I20-25), atrial fibrillation (I48), heart failure (I50, I10; I13.0, and I13.2), cancer during the three years preceding the index-ICH (C00-97), dementia (F00-02 and F03.9), renal disease (N18-19), liver disease (K70-77), alcohol abuse (E244, F10, G312, G621, G721, I426, K292, K70, K860, O354, P043, Q860, T51, Y90-91, Z502, and Z714), previous major hemorrhage, and smoking were retrieved from Riksstroke and/or NPR. Riksstroke was the source of information on smoking habits, and NPR was the source of information on heart failure, ischemic heart disease, cancer, dementia, alcohol abuse, and previous hemorrhage. The assessment of major hemorrhage is previously presented in detail. 13
Our primary study outcome was recurrent ICH (I61), stroke of any type (I61, I63, or I64), or death from any cause. The outcomes were defined by their occurrence in Riksstroke (ICH, stroke), or CDR (death), excluding the first 30 days following discharge from the index stroke. The patients were followed until December 2008 (cause of death), December 2009 (ICH, stroke), and October 2010 (all-cause death) for a mean of 3.1 years with respect to the outcomes (range: 1 month to 6.5 years).
Statistical methods
Unadjusted yearly risk was calculated as the number of first events per 100 person years at risk. Kaplan–Meier curves were examined in order to detect major deviations from the proportional hazard assumption. We analyzed the data in three Cox proportional hazard regression models; unadjusted, with adjustment for age, sex and other explanatory variables; and in a model including a PS for the likelihood of being prescribed statins. This PS was based on explanatory variables, which included age, sex, level of consciousness at admission, living conditions, ADL-function, cardiovascular risk factors, other comorbidities, and drugs on admission. A PS was created from a logistic regression and ranged from 0 to 1. We applied our models to a cohort consisting of ICH survivors without extreme values of the PS score, i.e. below 0.05 and over 0.95, and in pairs of patients matched on their PS-score. In a sensitivity analysis, we also applied our models to all ICH survivors and to those without missing data on variables included in the PS-score, in addition we performed analyses stratified on the PS-score, producing pooled estimates. The Statistical Analysis System (SAS software, version 9.4, SAS Institute, Cary, NC) was used for all analyses.
Results
During 2004 through 2009, we identified 7463 patients with ICH who survived more than 30 days. Of these, 499 (6.7%) were excluded because of missing data on essential PS-variables, and 882 (11.8%) were excluded due to extreme PS values. The mean age of the remaining 6082 patients was 69.9 years. Of these patients, 1097 (18%) were prescribed statins after discharge. Patients who were excluded due to missing or extreme data did not differ significantly from included patients regarding age, sex, comorbidity, level of consciousness at admission, or medication.
Characteristics on admission of 6082 patients with intracerebral hemorrhage by statin treatment at discharge
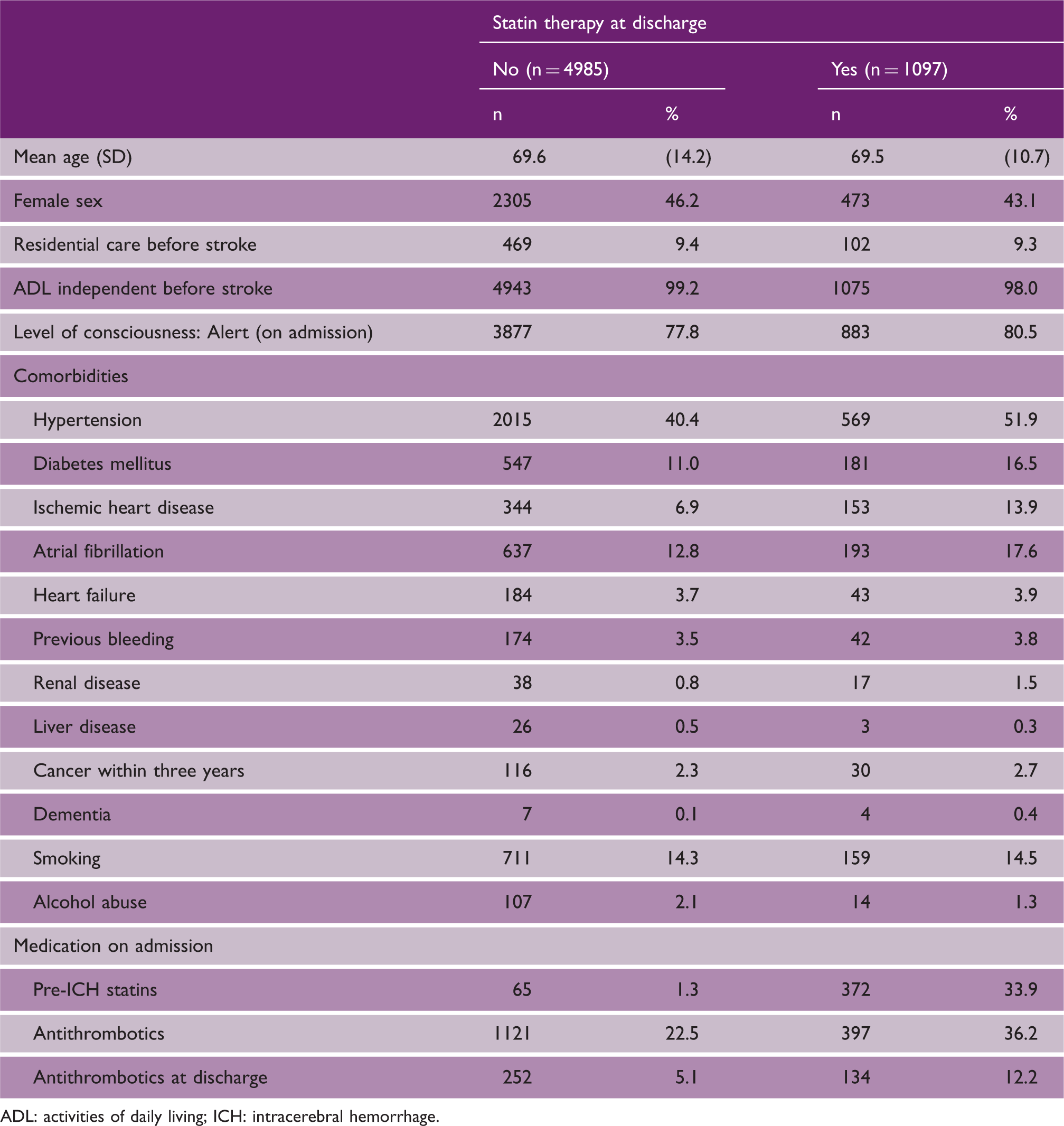
ADL: activities of daily living; ICH: intracerebral hemorrhage.
Recurrent ICH or ischemic stroke
During follow-up, 234 (3.8%) of the patients had a recurrent ICH and 584 (9.6%) had any type of recurrent stroke, which corresponds to a yearly risk of 1.2% and 3.1% for any stroke type. Kaplan–Meier curves for disease-free survival are plotted in Figure 1, panel a (ICH) and panel b (ICH or ischemic stroke). In both these figures, the curves diverge, but four years after the index-ICH, and near the end of the study period, they converge, which may or may not be an effect of chance.
Kaplan–Meier survival curves for patients with ICH by statin use. (Panel a: recurrent intracerebral hemorrhage; panel b: recurrent stroke; and panel c: all-cause death).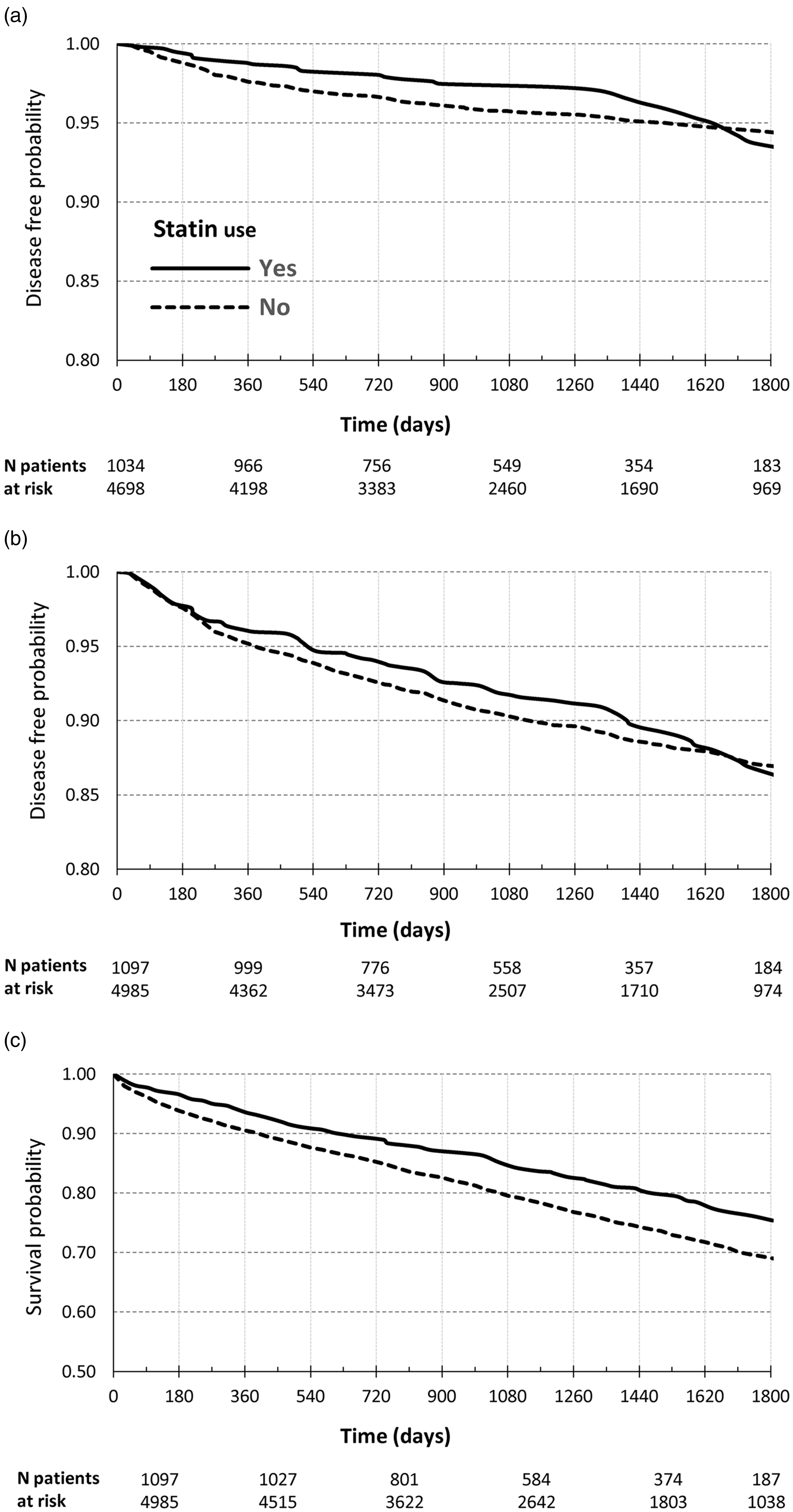
After adjustment for PS, statin therapy was not associated with neither an increased or decreased risk of recurrent ICH (hazard ratio (HR): 0.82; 95% confidence interval (CI): 0.55–1.22) nor with an altered risk for stroke of any type (HR: 0.86; 95% CI: 0.67–1.10); however, the trend was towards a decreased risk. Further adjustment for antithrombotic treatment at discharge did not significantly change the results (HR: 0.82; 95% CI: 0.55–1.23 for recurrent ICH, and HR: 0.84; 95% CI: 0.65–1.08 for stroke of any type). Unadjusted and adjusted HR for the risk of recurrent ICH and stroke of any type are displayed in Figure 2, panels a and b.
Hazard ratio in ICH patients. (Panel a: recurrent intracerebral hemorrhage; panel b: recurrent stroke; and panel c: all-cause death). PS: propensity score.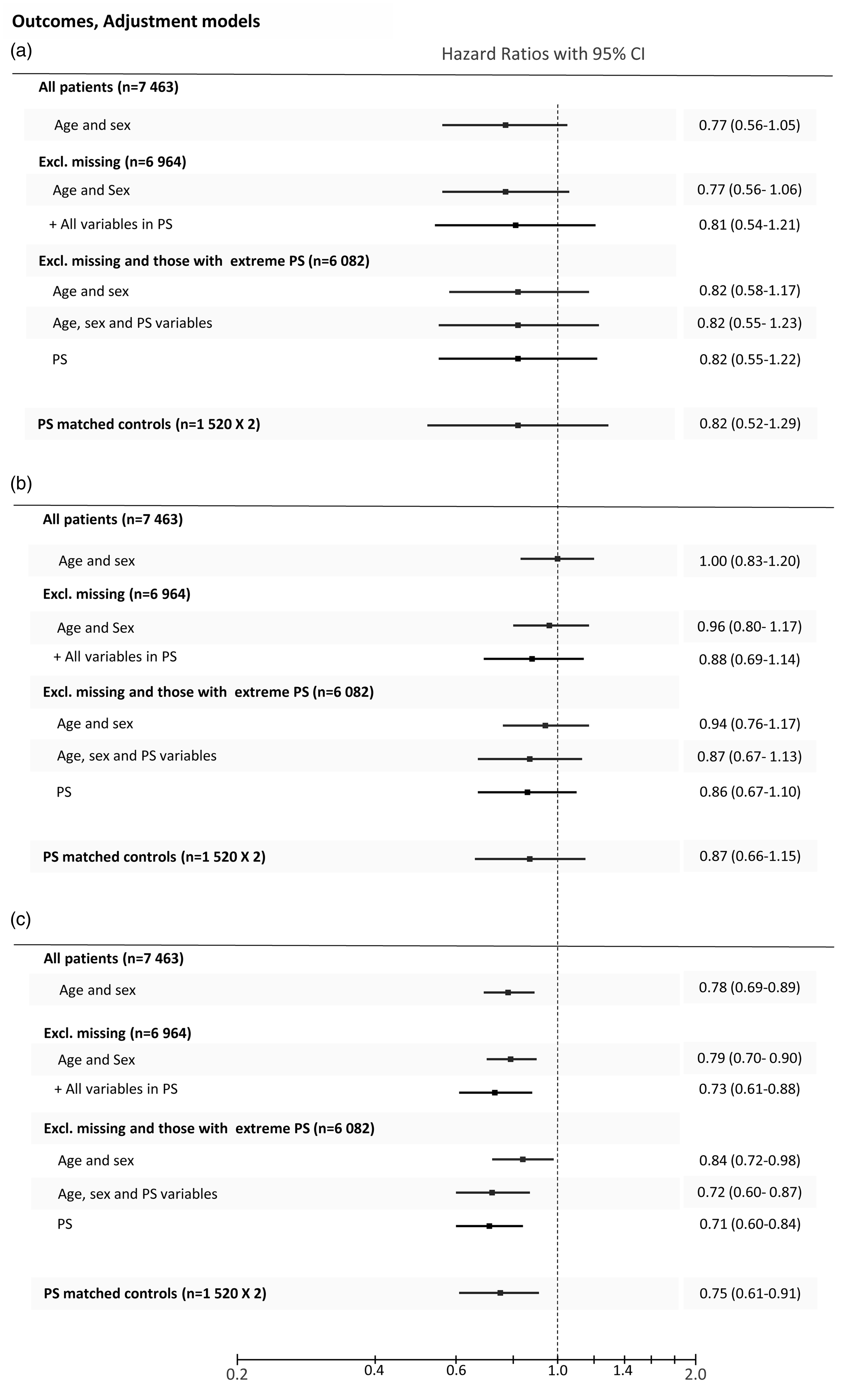
All-cause death
During follow-up, 1434 (23.6%) of the patients died, corresponding to a yearly risk of 7.1% for death. A Kaplan–Meier survival curve is shown as Figure 1, panel c. After adjustment for PS, statin therapy was associated with a reduced risk of death (HR: 0.71; 95% CI: 0.60–0.84). Further adjustment for antithrombotic treatment at discharge did not significantly change this (HR: 0.70; 95% CI: 0.59–0.83). Unadjusted and adjusted HR for the risk of death are displayed in Figure 2, panel c.
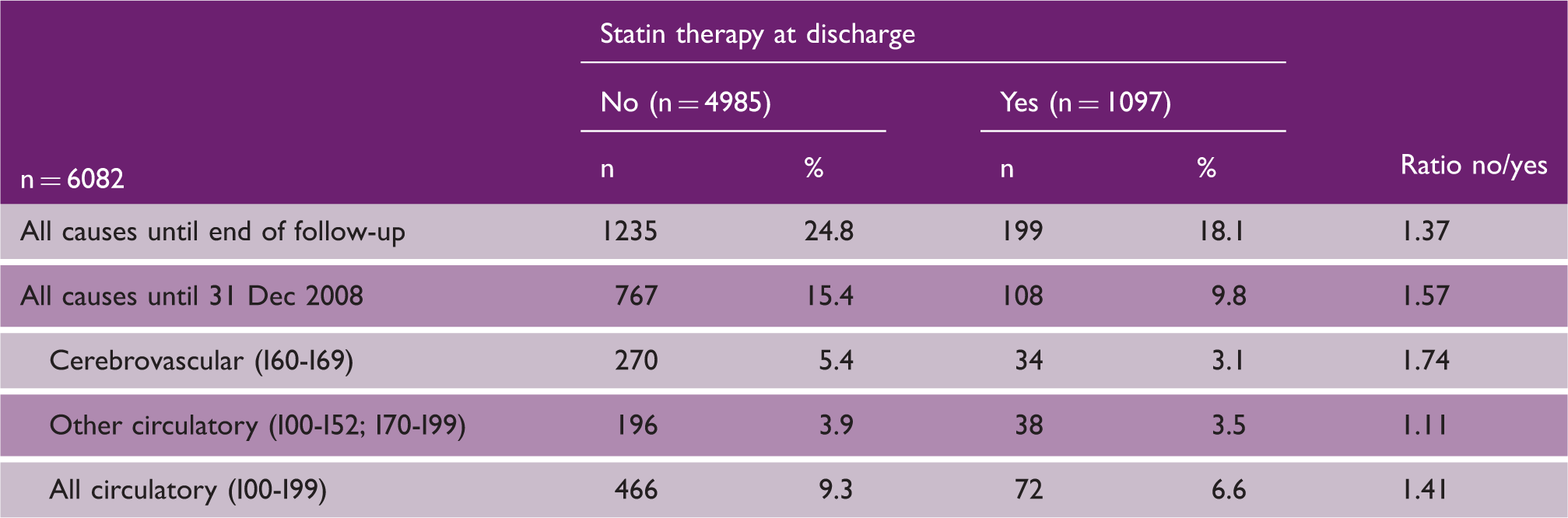
Causes of death
Causes of death in 6082 patients with intracerebral hemorrhage by statin treatment at discharge.
Discussion
In this observational study of patients with ICH, we demonstrated an association between subsequent statin therapy and reduced risk of death without an increased risk of stroke, including recurrent ICH.
Patients who have had ICH are at high risk for both ischemic and hemorrhagic strokes as recurrent events, 14 and it is therefore desirable to provide an effective protection against both these main types of stroke. Previously there has been a concern that statins would increase the risk of ICH.
Regarding ischemic stroke, there is now overwhelming evidence that statins are effective in preventing recurrent strokes. 15 A more intense reduction in low-density lipoprotein cholesterol levels produce further reductions of that risk. 16 In addition to cholesterol lowering, statins have pleiotropic effects, which may contribute to their protective effects, but also lead to unwanted side effects, including an increased bleeding risk. 5 The mechanism by which statins might amplify ICH remains unclear, 6 but it is possible that they may promote an increase of microbleeds, which are frequently observed in patients with cerebral amyloid angiopathy. One study reports statin use to be associated with such microbleeds in patients with ICH, 17 but it remains to be confirmed if microbleeds may serve as surrogate markers for ICH risk.
Two meta analyses,7,8 essentially covering the same primary studies, evaluated the use of statins in relationship to ICH. Both suggest statin use to be associated with reduced mortality and improved functional outcomes in patients with ICH in addition to a trend towards better long-time survival with statins. A weakness with these studies is that the results were not adjusted for potential confounders, such as severity of the hemorrhage, comorbidities, or medication.
A recent observational study, comprising 2457 patients, used PSs to adjust for confounders. 18 This study demonstrates an association between statins and reduced mortality and disability, but the follow-up period was only three months, and the mean age of the patients was only 62 years. 18 Our study adds substantial longer follow-up, both on survival and recurrent events. Moreover, the mean age in our study was 70 years, extending the results to an older population.
An interesting observation in our study was that survival had a stronger association with statins than recurrent ICH or stroke. This finding can be explained by statins’ beneficial effects on the risk of other diseases, most notably myocardial infarction, 16 thereby potentiating its stroke-preventing effect. However, our study could not confirm a substantial altered risk for death due to other circulatory diseases, including myocardial infarction, as we did not have access to causes of death during total follow-up.
The advantages with our study were its large size and its use of a well-established comprehensive stroke register. Furthermore, by record linkage of data from two additional registers, we were able to build an extensive data set, containing reliable information on comorbidities and survival. The follow-up time was considerably longer than in previous studies, in which the follow-up period was limited to three months.7,8,18
Some limitations must also be acknowledged. This was an observational study, with the weaknesses that are associated with such studies. Although we have adjusted the results for many confounders, we cannot completely rule out residual confounding. For example, there was only limited information on stroke severity (i.e. alertness upon admission), and use of statin was not equally distributed (82% vs. 18%). We had no information regarding the location of the bleeding. Patients with lobar microbleeds have a higher risk of ICH, 19 and such patients may be especially vulnerable in this respect. Information regarding the localization of the initial ICH would therefore have been of interest, in order to differ between lobar and deep bleedings. The time point when statin therapy was initiated during hospital stay was not known. According to one study, in-hospital statin use may be an important factor. 7 We only had data on statin prescription before admission, and at discharge, but no information on patient persistence to statin treatment after hospitalization. Information on dosage of statins was not available. This may have increased slightly during the study period, but the breakthrough for high doses did not come until 2010. 16 Our mean time of follow-up period was limited to 3.1 years, and the Kaplan–Meier curves suggest a favor to avoid statins near the end of follow-up. This might indicate a need for a longer follow-up period with respect to stroke, and preferably an on-treatment analysis. Finally, our observational study was based on Swedish data, and it is unclear if the results can be generalized across different nations or races.
This study provides some reassurance that, in at least selected patients, statins may be safe to use after an ICH. Patients discharged with statins had a lower mortality and a trend towards lower stroke recurrence, including ICH. There is still a question as to whether the results are valid for all types of ICH. In particular, lobar hemorrhages, which are related cerebral amyloid angiopathy, may be a case for concern. Further studies should address this matter, and also whether the use of statins is warranted in still higher ages.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: At the time of study, KMH was employed at AstraZeneca R&D. SÅ, BF, and PA have no conflicts of interest in relation to this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.