
Abstract
Background
India is a large country with geographically diverse populations and varying risk factors. Identification of regional differences can improve healthcare policy decisions.
Aim
To study regional differences in stroke between North and South India.
Methods
We analyzed data from the Indo-US Collaborative Stroke Project, a National Institute of Health-funded multicentre prospective study conducted in five academic centers in India with a US-based coordinating center. Risk factors, severity, mechanisms, management, complications, and outcomes among ischemic stroke patients were compared between North and South Indian centers.
Results
Of the 2066 patients enrolled from North (n = 1060) and South India (n = 1006), North Indian patients were significantly older with fewer men and had lower rates of diabetes (32.8% vs. 38.7%, p < 0.01), dyslipidemia (3.5% vs. 25.7%, p < 0.01), tobacco use (27% vs. 38%, p < 0.001), and alcohol use (30.1% vs. 38.6%, p < 0.01). North Indian patients had higher median National Institute of Health stroke scale scores (10 vs. 9, p < 0.01), more frequent large-artery atherosclerosis mechanism (34% vs. 25.6%, p < 0.001), intravenous thrombolysis (14.0% vs. 6.1%, p < 0.001), and lower rates of pneumonia (10.5% vs. 15.1%, p = 0.02). The three-month outcome (modified Rankin Scale score 0–2, 45.8% vs. 50.3%, p = 0.08) did not differ; however, North Indian patients had higher 90-day mortality (23.5% vs. 13.5%, p < 0.0001).
Conclusions
The substantial regional differences in stroke risk factors and mechanisms may be partly explained by factors such as differing dietary habits and lifestyle, which can be addressed at a national level. Differences in acute and inpatient stroke care suggest a need for better adoption of national stroke management guidelines.
Keywords
Introduction
Stroke is a common and disabling condition, imposing a major health burden especially in low-income and middle-income countries. 1 Regional differences are documented across different parts of the world, for example in the “stroke belts” in USA, Spain, and China.2–4 In China, there is a higher incidence of stroke in the northern areas. Regional differences have been noted in Thailand with higher stroke prevalence rates in cities and central regions. 5 Similarly, in countries such as India and Indonesia, differences in stroke incidence and prevalence have been described between urban and rural areas.6,7
Several differences exist in North and South India in terms of dietary preferences, 8 vitamin D levels, 9 genetic risks, 10 cultural differences, 11 seasonal variations, 12 and air pollution. 13 Conceivably, these differences may induce variations in cardiovascular risk that would be of national importance. In this study, vascular risk factors, stroke mechanisms, inpatient management, and outcome of stroke in North and South India were compared using data from the Indo-US Collaborative Stroke Project (IUCSP).
Methods
The IUCSP is a multicenter prospective hospital-based study funded by US National Institute of Health (NIH) and Department of Biotechnology, Government of India. 14 From January 2012 to December 2014, adults with ischemic stroke admitted within two weeks of symptom onset were enrolled consecutively after obtaining written informed consent. Exclusion criteria included intracerebral haemorrhage, patients discharged from emergency department without admission, and inability to obtain informed consent. Ethics Committees from each participating hospital approved the study.
Detailed methods have been published. 14 Briefly, trained coordinators collected information on demographics, risk factors, thrombolysis, patient management details, complications, investigations, treatment, and outcome at 90 days. Coinvestigators were certified to perform the National Institutes of Health Stroke Scale (NIHSS) and modified Rankin Scale (mRS) and trained in using the web-based “Causative Classification of Stroke” tool for assessing stroke mechanism.
For this analysis, IUCSP patients were categorized as North versus South based upon the location of the enrolling center, as follows: North India included the All-India Institute of Medical Sciences (AIIMS), New Delhi; Postgraduate Medical Education and Research (PGIMER), Chandigarh; and Christian Medical College (CMC), Ludhiana. South India included the Sree Chitra Tirunal Institute for Medical Sciences and Technology (SCTIMST), Trivandrum, and Nizam's Institute of Medical Sciences (NIMS), Hyderabad. Figure 1 shows the center location and the number of patients enrolled per center.
Map of India depicting the location of five academic centers in North and South India.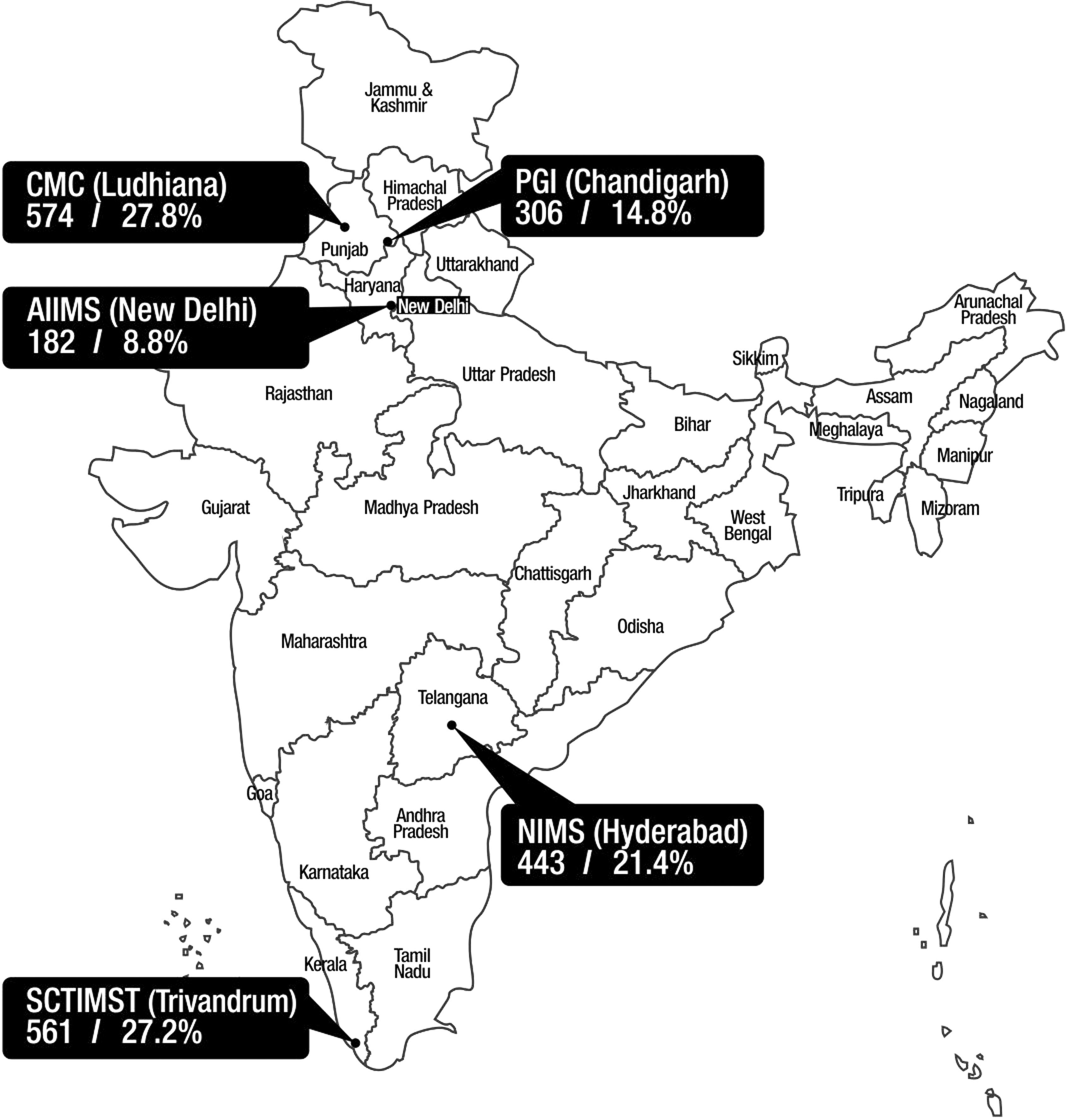
Statistical analysis
Statistical analysis was done using SPSS, version 21.0. Armonk, NY: IBM Corp. Continuous variables are stated as mean with standard deviation or median with interquartile range. Categorical variables are depicted as numbers and percentages. Chi square and Student's t-tests were used as appropriate. Variables which were significant (p < 0.05) in univariate analysis were incorporated in a multivariate analysis to determine independent predictors of good outcome and mortality at three months.
Results
Demographics, risk factors, severity, and mechanisms
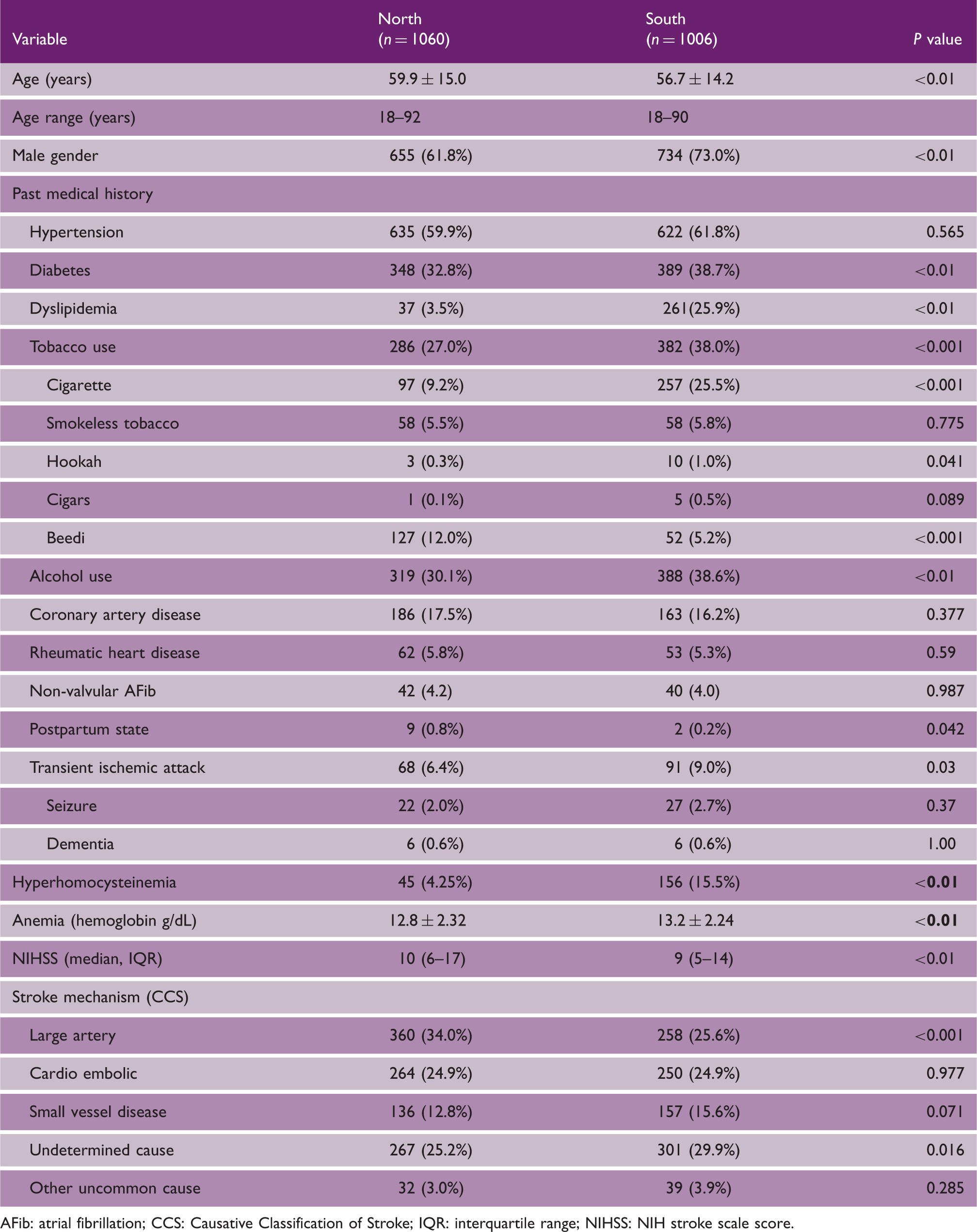
AFib: atrial fibrillation; CCS: Causative Classification of Stroke; IQR: interquartile range; NIHSS: NIH stroke scale score.
Acute and in-hospital management and clinical outcomes
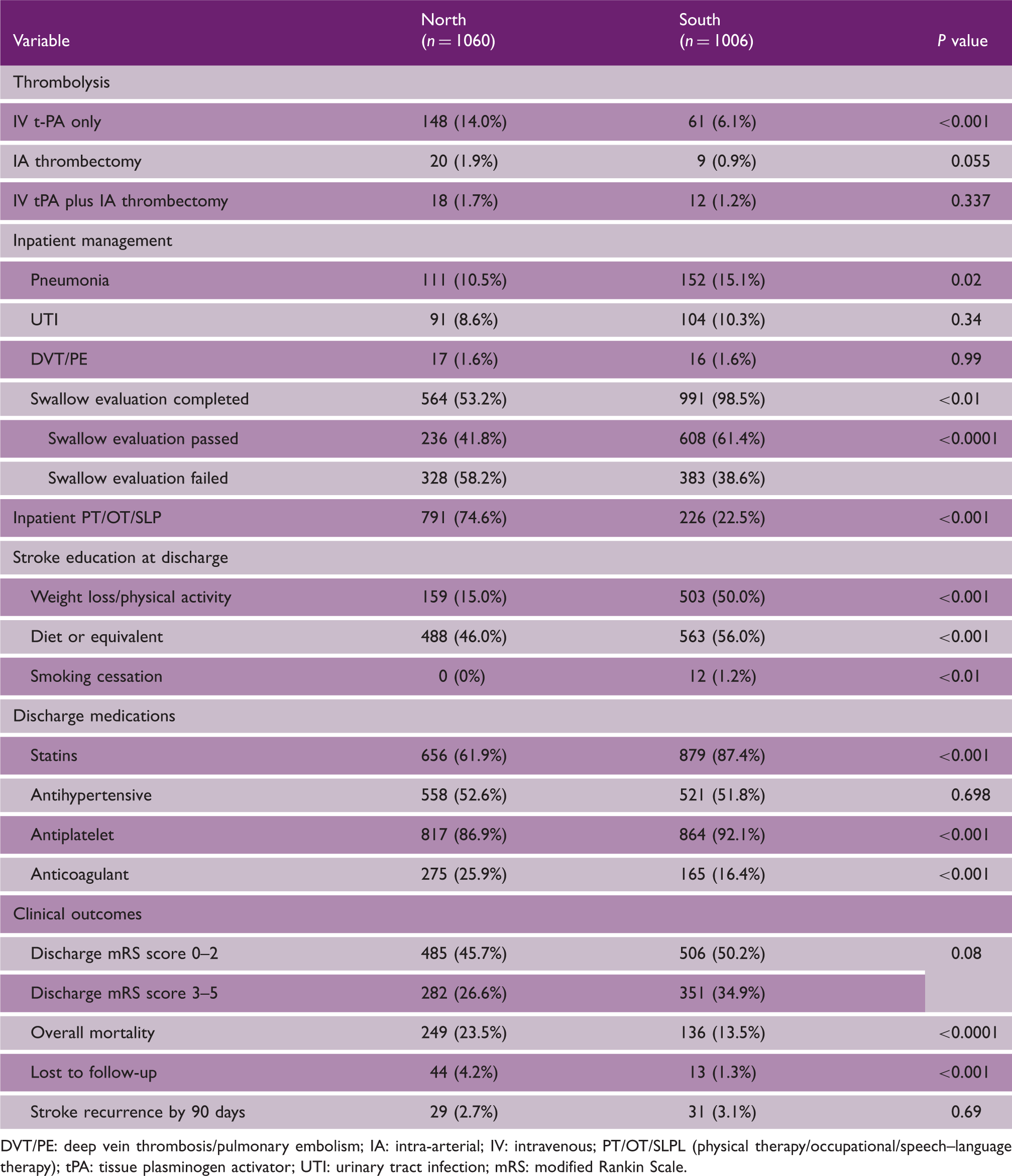
DVT/PE: deep vein thrombosis/pulmonary embolism; IA: intra-arterial; IV: intravenous; PT/OT/SLPL (physical therapy/occupational/speech–language therapy); tPA: tissue plasminogen activator; UTI: urinary tract infection; mRS: modified Rankin Scale.
The rates of antihypertensive medications were largely similar; however, statins and antiplatelet agents were used significantly less often while anticoagulants were used more often in North India.
The proportion of patients who achieved good three-month outcome (mRS, 0–2) was comparable in both groups. However, North India had higher mortality at 90 days. There was no significant difference in the rates of stroke recurrence.
Predictors of good outcome (mRS 0-2) and mortality at 90 days
Univariate analysis: predictors of good outcome and mortality
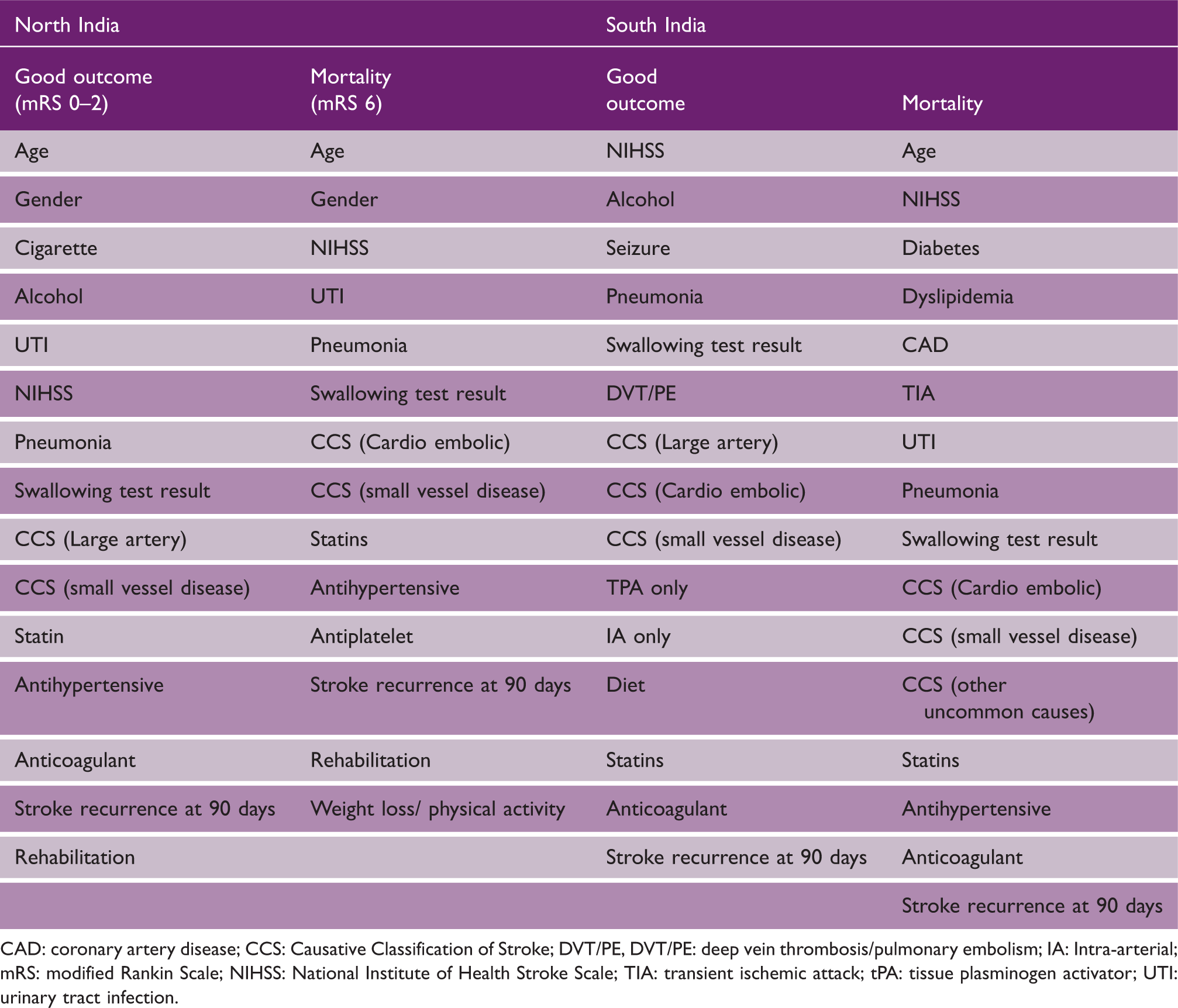
CAD: coronary artery disease; CCS: Causative Classification of Stroke; DVT/PE, DVT/PE: deep vein thrombosis/pulmonary embolism; IA: Intra-arterial; mRS: modified Rankin Scale; NIHSS: National Institute of Health Stroke Scale; TIA: transient ischemic attack; tPA: tissue plasminogen activator; UTI: urinary tract infection.
Multivariate logistic regression analysis: good outcome (mRS 0–2) at 90 days
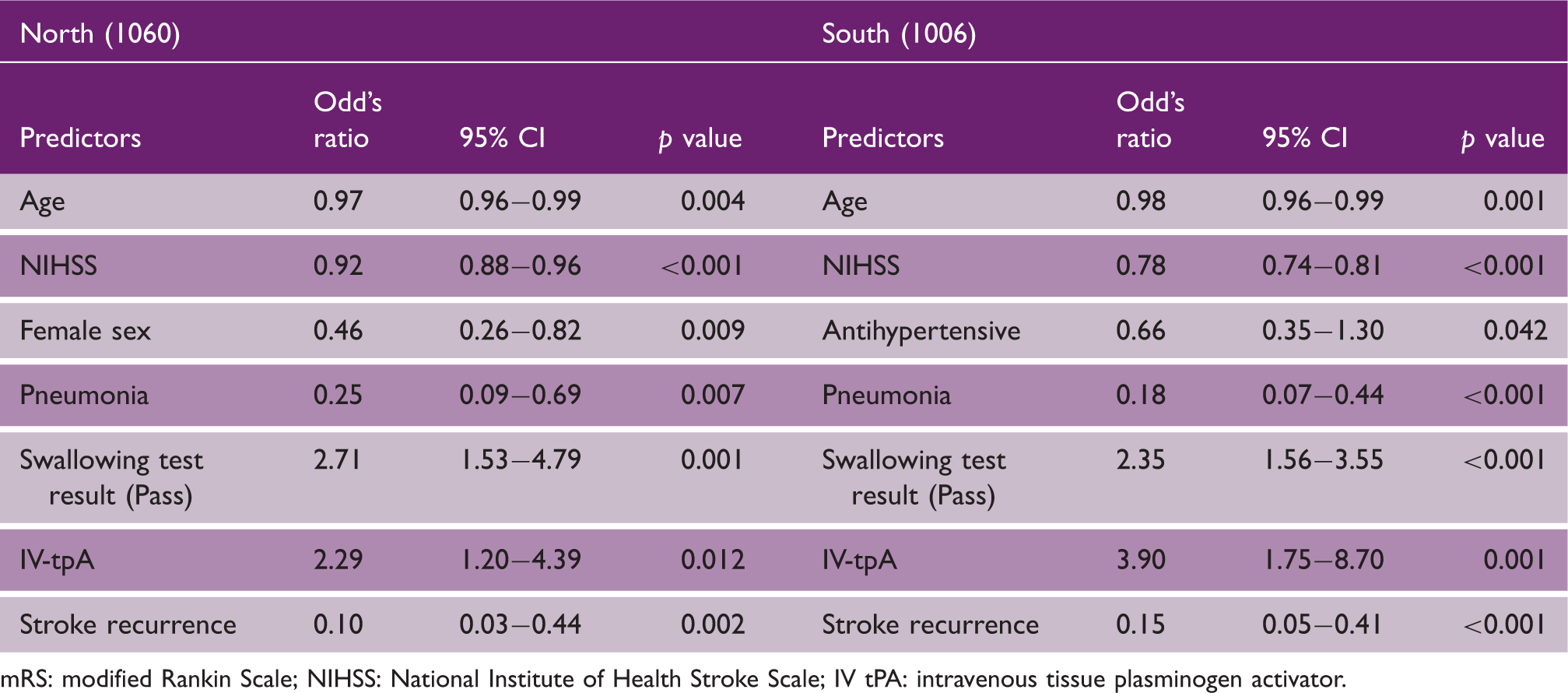
mRS: modified Rankin Scale; NIHSS: National Institute of Health Stroke Scale; IV tPA: intravenous tissue plasminogen activator.
Discussion
IUCSP delivered consistent and precise data on stroke risk factors, thrombolysis, complications, and outcomes from India.14,15 India is a land of “nations within nations” with huge diversity in culture, language, and geographical conditions. Most of the work on regional differences in stroke in India has been on urban versus rural differences.16,17 The five participating centers in this study are the leading tertiary research centers in India situated in two zones (north and south). They capture a huge catchment area of referral in North as well as South India. The centers in North India cater to states like Delhi, Punjab, Himachal Pradesh, Jammu & Kashmir (J&K), Bihar, and parts of Uttar Pradesh and Rajasthan (Figure 1). The centers in South India receive patients from Kerala, Telangana, Andhra Pradesh, and parts of southern Tamil Nadu.
Recently, Indian Council of Medical Research (ICMR) published the disease burden trends of all states from 1990 to 2016. 18 They grouped states based on epidemiological transition levels (ETLs), defined as “ratio of all-age DALYs due to communicable, maternal, neonatal, and nutritional disorders (CMNNDs) versus those due to non-communicable diseases (NCDs) and injuries together” (0.56–0.75 lowest ETL, 0.41–0.55 lower–middle ETL, 0.31–0.40 higher–middle ETL, ≤ 0.30 highest ETL). A ratio lower than one implied a higher burden of NCDs and injuries. In 1990, most of the states had ratios more than 1, while most states in 2016 had ratio less than 1 indicating heavy increase in NCDs in the country. The proportion of NCDs and injuries to CMNNDs was more in southern states like Kerala and Tamil Nadu and relatively lowest in Northern states like Bihar and Uttar Pradesh. In our study, the states in the South India have higher–middle (Telangana, Andhra Pradesh) and highest (Kerala, Tamil Nadu) ETLs. The Northern states have lowest (Bihar, Uttar Pradesh, Rajasthan), higher middle (Delhi, Haryana, J&K), and highest (Punjab, Himachal Pradesh) ETLs.
Our results show the regional differences in various risk factors for stroke. The epidemiological transition happening more in south might account for the higher occurrence of conventional risk factors in South India. In the ICMR study, Kerala and Tamil Nadu had the largest share of NCDs. Even though cigarette smoking rates were less in north, there was variability in local tobacco exposure (beedi smoking). The higher rates of beedi exposure and anemia may be contributed by the relatively less developed states like Bihar and Uttar Pradesh. Our findings were consistent with the risk factor prevalence, assessed by a cross-sectional study on 1983 participants from 1600 villages in 18 states of India, that smoking was more common in South India and chewing tobacco was more common in North India. 17 Although smoking and tobacco exposure were significant risk factors, practically no one received stop smoking advice. The American Heart Association (AHA) 2018 Stroke guidelines recommend that health workers strongly counsel every patient with acute ischemic stroke, who has smoked during previous year to quit smoking.19,20 This is an example of an area for improvement where tobacco deaddiction can start from hospital admission.
Notably dyslipidemia is very low in North (3.5%) compared to South (25.69%). There are very few studies on epidemiology of dyslipidemia in India and available data show prevalence ranging from 10% to 15% in rural and 25–30% in urban populations. 21 This is much lower than Western population and moreover there is paucity of details of dyslipidemia in India. Few studies from India have shown higher levels of triglycerides and lower high-density lipoprotein (HDL) levels (“atherogenic dyslipidemia”). Atherogenic dyslipidemia has strong association with diabetes and metabolic syndrome and is common in South Asian population. High carbohydrate diet may be linked to this lipid profile abnormality. 22 The Indian Council of Medical Research–India Diabetes (ICMR-INDIAB) study conducted in four states showed that there is a regional disparity in dyslipidemia with high rates of hypercholesterolemia and low-density lipoprotein-C (LDL-C) seen in Tamil Nadu (18.3%) and Chandigarh having high triglyceridemia (38.6%), highest rates of low HDL-C in Jharkhand (76.8%) and highest rates of high LDL-C in Tamil Nadu (15.8%). 23 Fitheart study reported regional differences in lipid profiles across 20 states of India using fasting blood samples from 46,919 subjects aged 18–96 years. Kerala had the highest mean cholesterol levels. 21 Kinra et al. had shown in their study on prevalence of risk factors in rural India that dyslipidemia is more common in South than North India. 17 All these factors would have contributed to the regional disparity of higher dyslipidemia in South India in our study.
Hyperhomocystinemia was more prevalent in South in our study but it has been documented in both north and south Indian population. 24 In the Hordaland Homocysteine Study, smokers had higher homocysteine levels than smokers. 25 A case–control study from North India had shown that MTHFR C677T gene polymorphism might be a risk factor of small vessel stroke. 26 In our study, south group had more smokers and small vessel stroke which along with genetic and dietary factors would have contributed to hyperhomocystinemia.
The stroke was more severe, with higher median NIHSS and large artery atherosclerosis in North India. Swallowing tests were administered in 53% patients of North and 99% of South. Among those patients who underwent swallowing tests, 42% passed in North while 61% passed in South. Severity of stroke and more posterior circulation stroke in north might have contributed to lesser frequency of swallowing testing and higher failure rates. But interestingly, pneumonia was more common in South group which may be due to frequent swallowing assessment with failures or due to better protocols for detection of pneumonia.
The rate of atrial fibrillation (AF) was comparable (North 4.2% vs. 4.0% South). The Trivandrum stroke registry from South India had reported prevalence of AF in stroke patients as 7.8%. 27 Ludhiana stroke registry from North India had 10% atrial fibrillation in ischemic stroke patients. 28 Khurana et al. had reported 18% AF among ischemic stroke patients admitted within 8 h. 29
IVT was much higher in North (13.96% vs. 6.06%). The centers in North were responsible for starting IVT in India more than a decade ago.29–31 One of these centers (AIIMS, New Delhi) delivers IVT for free of cost. Most of the acute stroke patients reach hospital by own vehicles or private transportation. Good roads and lesser traffic are added advantages for centers like PGIMER, Chandigarh. Among the patients who received IVT and/or intra-arterial treatment, 60.2% of patients in north had used private transportation and 30.6% had patients transferred from other hospitals, while in south, 62.2% were transferred from other hospitals and 25% arrived using private transportation. The centers in south had better coordination with local hospitals in transferring patients to comprehensive stroke centers. Another reason for the different rates of thrombolysis is preferential admission of stroke patients requiring intervention in few centers in North. Due to high patient load and fewer in-patient bed availability, many minor strokes and non-acute stroke patients might not get admission in centers in North.
The regional difference in antiplatelet and anticoagulants use may reflect the individual preferences of neurologists in North and South India. It shows the real-world practices in this part of the world rather than strict adherence to guidelines. In-patient rehabilitation was more in North India. The rehabilitation team in North India consists of trained neuro-physiotherapists who are part of stroke team and delivers physiotherapy and occupational therapy to both in-patients and patients in follow up on out-patient services. Unfortunately, post-acute transfers for rehabilitation are uncommon in India due to the lack of infrastructure.
North India had more severe stroke (higher NIHSS, more duration of stay, and lesser swallowing test attempts) which could account for the higher mortality at three months. Moreover, since there was no difference in mortality at hospital discharge, factors affecting the care of severe stroke patients at home might have influenced the mortality. The poor social indicators of the catchment area of North cause poor local healthcare delivery system and poor post stroke support system for these patients.
Limitations
The study was a hospital-based analysis of ischemic stroke patients in two zones of India. Though the participating centers are leading tertiary care hospitals, they cannot be truly representative of both zones as some states may not be covered by these centers. Admission bias could have been there as there is shortage of beds and thus more severe stroke patients get preferential admission. The health care challenges in rural India and private hospitals are different and our results may not reflect them.
Conclusion
The regional differences in stroke between North and South India showed that the conventional vascular risk factors are more common in south supporting the epidemiological transition ongoing in India. The regional differences in stroke mechanisms, management, complications, and outcomes are opportunities for improvement in stroke care delivery systems.
Footnotes
Authors' note
M.V. Padma and Aneesh B. Singhal shared senior authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from NINDS R21NS077442 and Dept. of Biotechnology India (Singhal, PI: Indo-US Collaborative Stroke Registry and Infrastructure Development).