
Abstract
Rationale
Intravenous thrombolysis combined with mechanical thrombectomy (MT) has been proven safe and clinical effective in patients with acute ischemic stroke of anterior circulation large vessel occlusion. However, despite reperfusion, a considerable proportion of patients do not recover. Incidence of symptomatic intracerebral hemorrhage was similar between patients treated with the combination of intravenous thrombolysis and MT, as compared to intravenous thrombolysis alone, suggesting that this complication should be attributed to pre-treatment with intravenous thrombolysis. Conversely, intravenous thrombolysis may be beneficial in patients with small clots occluding intracranial arteries with underlying intracranial atherosclerotic disease, not accessible for MT.
Aim
To assess whether direct MT is non-inferior compared to combined intravenous thrombolysis plus MT in patients with AIS due to an anterior circulation large vessel occlusion, and to assess treatment effect modification by presence of intracranial atherosclerotic disease.
Sample size
Aim to randomize 636 patients 1:1 to receive direct MT (intervention) or combined intravenous thrombolysis plus MT (control).
Design
This is a multicenter, prospective, open label parallel group trial with blinded outcome assessment (PROBE design) assessing non-inferiority of direct MT compared to combined intravenous thrombolysis plus MT.
Outcomes
The primary outcome is the score on the modified Rankin Scale assessed blindly at 90 (±14) days. An common odds ratio, adjusted for the prognostic factors (age, NIHSS, collateral score), representing the shift on the 6-category mRS scale measured at three months, estimated with ordinal logistic regression, will be the primary effect parameter. Non-inferiority is established if the lower boundary of the 95% confidence interval does not cross 0.8.
Discussion
DIRECT-MT could result in improved therapeutic efficiency and cost reduction in treatment of anterior circulation large vessel occlusion stroke.
Introduction and rationale
Stroke is a major cause of death and disability worldwide, and of all countries China has the highest age standardized stroke incidence. Contrary to the global trend this incidence is on the rise. 1 The latest National Epidemiological Survey of Stroke in China (NESS-China) reported the age-standardized prevalence, incidence, and mortality rates of stroke were 1114.8/100,000 people, 246.8 and 114.8/100,000 person-years, respectively. Among incident and prevalent strokes, ischemic stroke constituted 69.6% and 77.8%. 2 Early 2015, the outlook of acute ischemic stroke (AIS) changed dramatically over the course of a few months when five trials reported benefit from mechanical intra-arterial treatment (MT) in patients with AIS caused by a large vessel occlusion (LVO) of the anterior circulation.3–7 This resulted in rapid implementation of MT worldwide, with MT also being routinely performed in the China, with an estimated 18,000–20,000 treatments every year. While functional outcomes improved, still a large proportion of patients suffer from poor outcome (dead or severe disability) at follow-up.8,9 Further, the majority of patients included in randomized clinical trials (RCTs) investigating MT and patients treated in clinical practice were pre-treated with intravenous thrombolysis (IVT). 8 Currently, however, there seems to be clinical equipoise regarding the added value of pre-treatment with IVT, warranting randomized clinical trials (RCTs10,11).
The majority of RCTs and observational studies currently investigating this topic include subjects from Western populations. Multiple differences in pathophysiology and organization of stroke care between the Chinese and Western populations make it difficult to generalize results from Western trials. Intracranial atherosclerotic disease (ICAD) is known to be a far more common cause of ischemic stroke in Asians than Caucasians. 12 Of all strokes due to an LVO, 12–30% were reported to be caused by underlying ICAD in East asia. 13 Therefore, rescue treatment with stent implantation is performed frequently; in approximately 23% of patients in a recent Chinese study. 14 Last, reimbursement of medical costs through insurance varies, with a recent study reporting that in middle-aged and elderly the reimbursement rate was approximately 40%. 15 Additional therapy with rtPA cause additional costs of around US$1200 per patient, of which a considerable proportion consist of out-of-pocket expenses for patients in China. These differences warrant studies investigating the effectiveness of pre-treatment with IVT before MT tailored to the Chinese setting. A recent observational study in a Chinese cohort reported no significant difference concerning neurological outcomes in patients treated with direct MT or combined IVT plus MT, with better rates of successful reperfusion and less asymptomatic hemorrhages in the direct MT group. 14
The aim of Direct Intra-arterial thrombectomy in order to Revascularize AIS patients with large vessel occlusion Efficiently in Chinese Tertiary hospitals: a Multicenter randomized clinical Trial (DIRECT-MT) is to assess whether the clinical outcome of direct MT is non-inferior to MT with pre-treatment with IVT in a Chinese population.
Methods
Design
DIRECT-MT is a multicenter phase III prospective randomized clinical trial with open-label treatment and blinded outcome assessment (PROBE). The intervention is direct MT and the comparator MT with pre-treatment with IVT. Patients are randomized 1:1. Patient flow is depicted in Figure 1. As a quality initiative, all the centers should meet the following minimum criteria: (1) the center should be the local tertiary hospital; (2) the center should have experience in conducting acute stroke trials; (3) the center could carry out both IVT and MT, and have more than 30 cases of MT every year; (4) the previously door-to-needle time (DNT) was less than 60 min, and door-to-puncture time (DTP) was less than 90 min. Currently, 41 centers in China are recruiting patients for the study. Approval of the Institutional Review Board was obtained in January 2018. The first patient was included in February 2018. DIRECT-MT is designed in close collaboration with the principal investigators of MR CLEAN-NO IV, and its pragmatic, non-restrictive design is based on the original MR CLEAN trial.3,16
Patient flow in direct MT.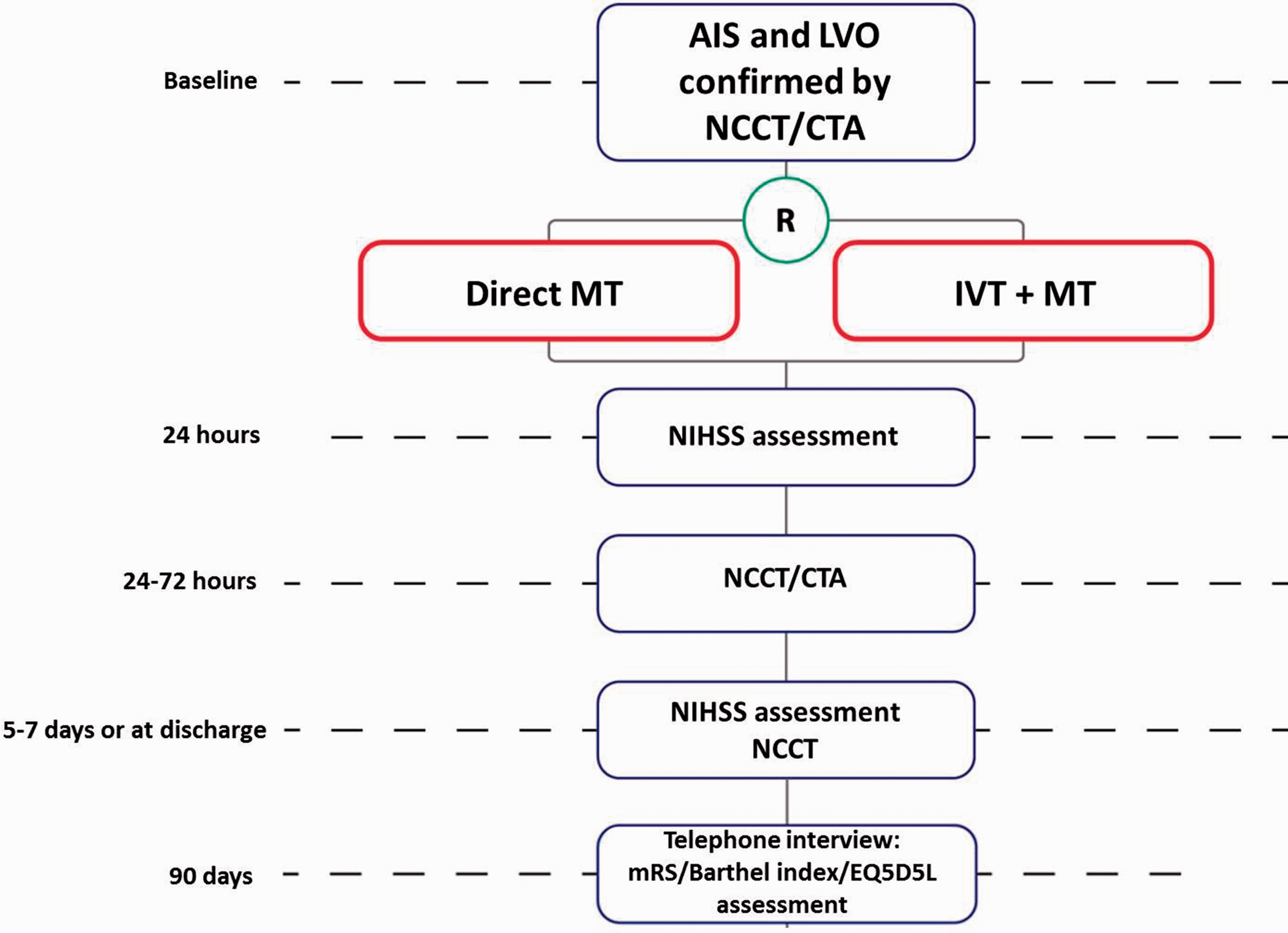
Patient inclusion and exclusion criteria
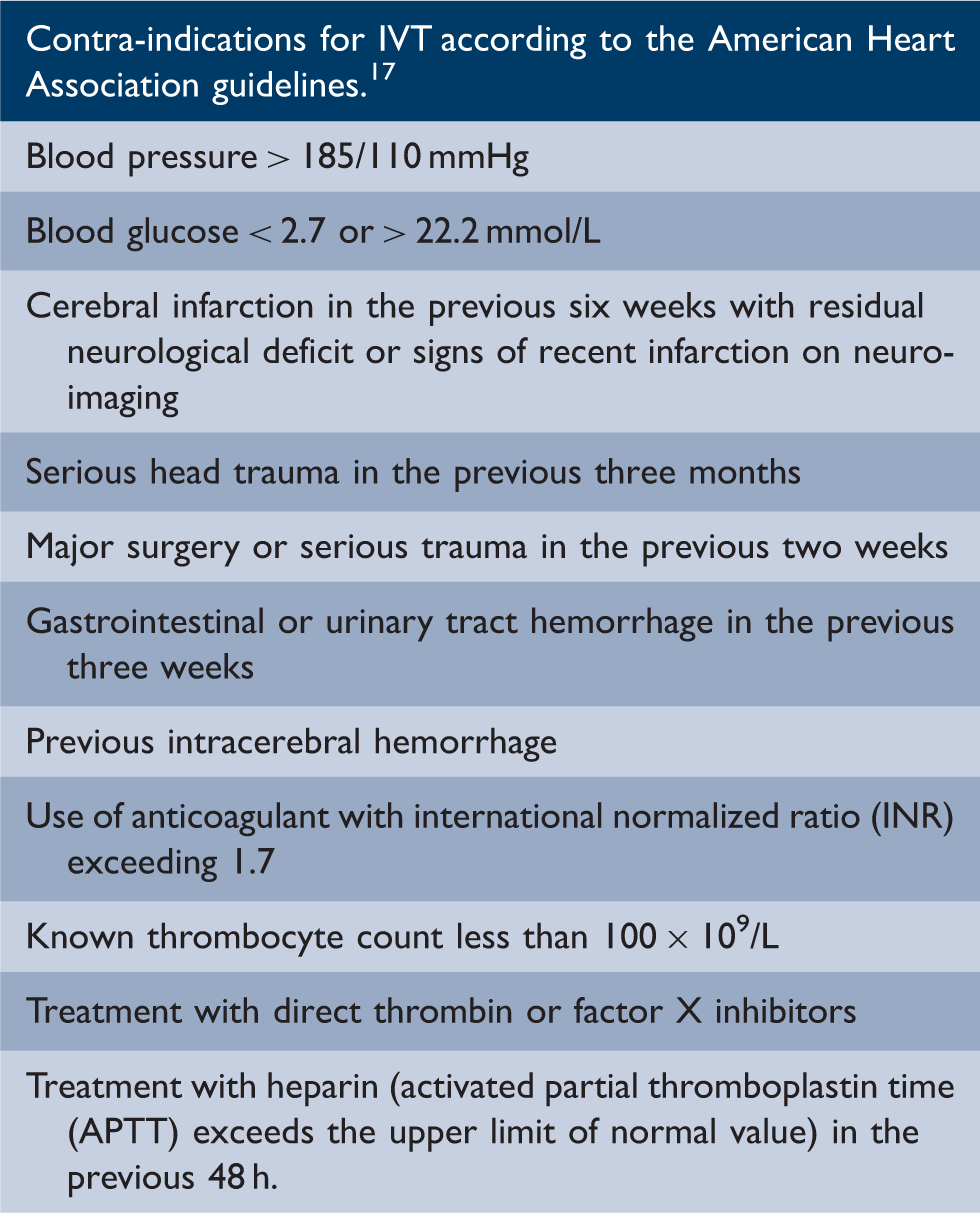
Contra-indications for IVT
Randomization
After an intracranial occlusion has been confirmed and written informed consent has been obtained, randomization is allowed. The randomization procedure is computer- and web-based. Randomization is stratified by center. The trial has two arms: (1) the direct MT group (intervention group) and (2) the combined IVT plus MT treatment (control group).
Blinding
As this is an open label trial, the treatment allocation is known to both the treating physician and the patient. A blinded, trained investigator will procure the information concerning clinical outcome at three months using standardized forms and procedures. Based on these reports, members of the outcome committee who are blinded for treatment allocation assign the final score on the modified Rankin scale. Neuro-imaging will be also assessed by a core-laboratory blinded for treatment allocation. To report to the data safety monitoring board (DSMB), outcome data will be combined with data on treatment allocation by an independent trial statistician. Members of the steering committee are kept blinded of results of interim analyses of efficacy and safety.
Intervention
Patients randomized to receive standard care will start with IVT (alteplase) according to the guidelines of the American Heart Association, 17 i.e. 0.9 mg/kg alteplase infused in 1 h, with a maximum dose of 90 mg, directly followed by MT. The trial organization strives to reduce delays in the MT due to IVT administration to an absolute minimum. Thrombectomy in these patients can start prior to end of infusion of the alteplase. Patients randomized to the intervention group proceed directly to MT without prior IVT administration. Mechanical thrombectomy is thus standard performed in both groups. The trial recommended the random to puncture time should be less than 60 min. All stent retriever devices approved by the China food and drug administration (CFDA) for MT are allowed in the trial as the first treatment strategy. Aspiration devices may be used as second option if the interventionist determines first strategy has failed. Particular device choice for specific patients is left to the interventionist.
If necessary local application (intra-arterial) of alteplase is allowed in both arms of the DIRECT-MT study. Patients pre-treated with IVT should not receive more than 30 mg alteplase during intra-arterial treatment. Delivery of alteplase in shots of 5 mg in 5–10 min intervals is recommended. An equivalent dose of 400,000 U urokinase, delivered in shots of 50,000–100,000 U, in 5–10 min time intervals, is also accepted as escape medication in individual cases. If successful reperfusion (eTICI 2b-3) is not achieved in the direct MT group, IVT with 0.9 mg/kg may be initiated if the 4.5 h window or maximum dose is not exceeded.
Clinical and imaging evaluation
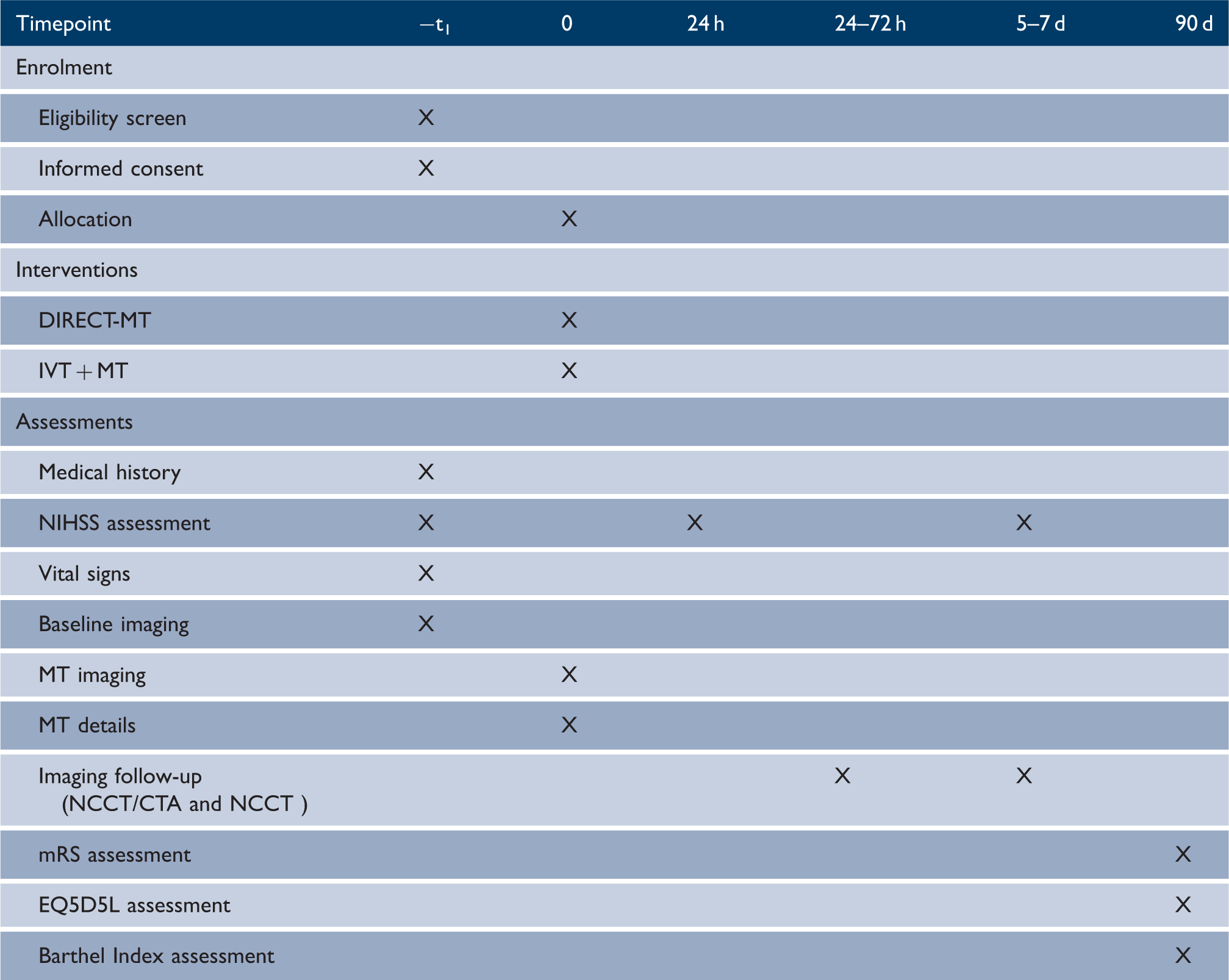
Timing of all procedures in DIRECT-MT
Primary outcome
The primary outcome is the score on the modified Rankin Scale assessed at 90 ± 14 days after randomization.
Secondary outcomes
Secondary outcomes are: (1) death within 90 ± 14 days; (2) pre-interventional reperfusion assessed on first intracranial DSA; (3) eTICI 19 score on final angiography of MT; (4) score on the NIHSS at 24 ± 6 h and 5–7 days, or at discharge; (5) recanalization rate at 24–72 h by CTA; (6) Final lesion volume at 5–7 days on NCCT 20 ; (7) score on the EuroQoL 5-dimensions 5-level (EQ5D-5L) 21 and Barthel index 22 at 90 ± 14 days; (8) dichotomous clinical outcome on the mRS at 90 ± 14 days.
Safety outcomes are the following: (1) hemorrhages according to the Heidelberg criteria 23 ; (2) sICH scored according to the Heidelberg criteria; (3) embolization in new territory on angiography during MT; (4) occurrence of aneurysma spurium; (5) occurrence of groin hematoma; (6) infarction in new territory at 5–7 days 24 ; (7) death from all causes within 90 ± 14 days.
Safety reporting
Adverse events (AEs) and serious adverse events (SAEs) are defined according to the ICH GCP guidelines 25 and are reported as required by local legislation.
Data safety monitoring board (DSMB)
An independent DSMB chaired by a neurologist, and including a neuro-interventionist and an independent methodologist/statistician monitors the trial. The DSMB plans to hold two interim analysis meetings when 1/3 and 2/3 cases have finished the 90 ± 14 days follow-up, and the analysis will assess the occurrence of adverse events by center and by procedure. During patient enrollment, interim analyses of mortality and available major outcomes and other requested analyses will be supplied confidentially to the chairman of the DSMB. Based on these analyses the DSMB advises the Steering Committee if the randomized comparisons in DIRECT-MT have provided both (1) “proof beyond reasonable doubt” that for all, or specific subgroups of patients, one particular treatment is clearly beneficial or detrimental concerning a net difference in outcome, and (2) evidence reasonably expected to influence patient management. No precise criteria of proof beyond reasonable doubt can be formulated, but a difference between treatment arms of three standard deviations or more concerning outcomes might be needed to justify premature termination or modification of the trial.
Sample size calculation
Our estimates are based on the mRS distribution in the control group of the trial, derived from the MR CLEAN trial's intervention arm 3 : mRS 0: 3%; mRS 1: 9%; mRS 2: 21%; mRS 3: 18%; mRS 4: 22%; mRS 5: 6% and mRS 6: 21%. A favorable treatment effect was assumed with a common odds ratio (cOR) of 1.16, corresponding to a 4% absolute increase in the rate of mRS scores of 0–2. The trial is powered to assess non-inferiority. The trial accepts a rather strict lower bound −5% chance of good functional outcome after intervention. This translates into a lower bound of 0.8, for the primary effect parameter, which is an odds ratio.
To demonstrate non-inferiority, the lower limit of the two-sided 95% confidence interval of the cOR should not cross the pre-specified non-inferiority boundary of 0.8. In a Monte Carlo simulation with 5000 runs we computed the proportion of positive trials, for a given sample size. A sample size of 710 was determined to detect the pre-defined non-inferiority with a power of 80% and two-sided alpha of 0.05. Covariate adjustment has been shown to reduce sample sizes up to 25%.26,27 We chose to assume a more conservative 15% sample size reduction through adjustment for age, baseline NIHSS, collateral status, pre-stroke mRS and time from onset to randomization . We estimated that anticipating a 5% dropout rate due to withdrawal of consent, a final sample size of 636 was determined, 318 per arm.
Statistical analysis
An adjusted common odds ratio (acOR) representing the shift on the 6-category mRS scale measured at three months, estimated with ordinal logistic regression, will be the primary effect parameter. Adjustment for the following prognostic variables will be performed: age pre-stroke mRS, time from onset to randomization, stroke severity (NIHSS) and collaterals. Adjusted and unadjusted estimates with their corresponding 95% confidence intervals will be reported. The primary aim of the study is to assess non-inferiority of direct MT compared to IVT with MT. To do so, we will determine whether the lower bound of the 95% CI of the adjusted common odds ratio crosses our pre-specified non-inferiority boundary of acOR = 0.8.
Secondary outcomes will be analyzed using linear, logistic, or ordered regression analysis method, with the same adjustments as the primary outcomes.
All analyses will be performed according to the intention-to-treat principle. Baseline data will be presented according to treatment allocation with descriptive statistics. Missing values for baseline characteristics will be reported. Missing baseline characteristics will be imputed with multiple imputation methods. Differences of treatment effect in specific subgroups will be assessed by testing for interaction of the pre-defined baseline variable with treatment allocation. Modification of treatment effect by the following variables will be assessed: tertiles of time from onset of symptoms to randomization, groin puncture and revascularization, extracranial carotid obstruction, occlusion location, collateral grades 0 to 3 as defined by Tan, 28 and thrombus perviousness. 29
Ethical considerations
The study is conducted according to the principles of the Declaration of Helsinki. 30 Investigators should adequately explain the details of the clinical trial, including known, foreseeable risks and possible adverse events, etc., to the subject or to the guardians of subjects without capacity for civil conduct or with limited capacity for civil conduct. After full and detailed explanation, subjects, as well as the investigators, sign their name and date on the informed consent form. As at least half of the AIS patients are expected to suffer from aphasia, lack understanding of their disease, or have other acute cognitive symptoms, we have determined that if: (1) the ethics committee agrees in principle, and (2) investigators believe that participating in the clinical trial is in the subjects' own interest, patients can enter the clinical trial if their guardians should sign the name and date before inclusion in the trial. The medical ethical committee and research board of the Changhai Hospital, Shanghai, approved this study in China (CHEC-2018-003).
Study organization
The sponsor of the trial is Changhai Hospital affiliated to the second military medical university, China. The trial is executed in collaboration with MR CLEAN-NO IV investigators. The first patient was recruited in February 2018, and the study is currently actively recruiting with 597 patients recruit to the end of May. A document detailing the organizational structure behind the DIRECT-MT trial, including all committees and a list of the DIRECT-MT investigators is added to Appendix 1.
Discussion
DIRECT-MT is a phase 3 randomized clinical trial with a PROBE design assessing non-inferiority of direct MT compared to IVT combined with MT in the Chinese population concerning patient outcome on the mRS at three months. The trial design is based on the MR CLEAN-NO IV trial executed in Europe, and has been tweaked to fit the Chinese setting.
Multiple RCTs are currently randomizing patients to receive direct MT or IVT with MT. The SWIFT-DIRECT (NCT03192332) and MR CLEAN-NO IV (ISRCTN80619088) trials both draw most of their patients from mainland Europe. Another study, DIRECT-SAFE (NCT03494920), has started recruitment in Australia with the aim of expanding to New Zealand, Taiwan and Europe. As with most major RCTs before, only few patients of East Asian descent will be included in the trials. Therefore, none of those trials is set-up to provide results generalizable to the Chinese population. In line with all but the MR CLEAN-NO IV trial, DIRECT-MT assesses non-inferiority of direct MT compared to IVT with direct MT. Primary endpoint of the MR CLEAN-NO IV is superiority of direct MT over IVT plus MT. In line with the MR CLEAN trial however, no formal imaging-based exclusion criteria have been installed. Essentially all patients eligible for MT and IVT according to local guidelines can be included in the trial.
To execute DIRECT-MT, the DIRECT-MT investigators work closely together with the MR CLEAN-NO IV investigators from the Netherlands. The largely similar design and similar outcome definitions allow for individual patient pooling of trial data after conclusion of the trials. This will result in increased power to detect small treatment effects and to explore effects in important (predefined) subgroups including but not limited to those defined by thrombus characteristics (thrombus perviousness, clot burden, density), quartiles of time from onset of symptoms to randomization, groin puncture and revascularization, ipsilateral extracranial carotid tandem lesion, occlusion location, collateral score, and large vessel occlusion due to different etiologies (intracranial atherosclerosis, cardioembolism, extracranial carotid atherosclerotic lesion, other extracranial carotid disease, unknown). Further, we will also be able to shed more light on potential inter-population differences concerning the effect of the intervention.
Major differences between DIRECT-MT and MR CLEAN-NO IV
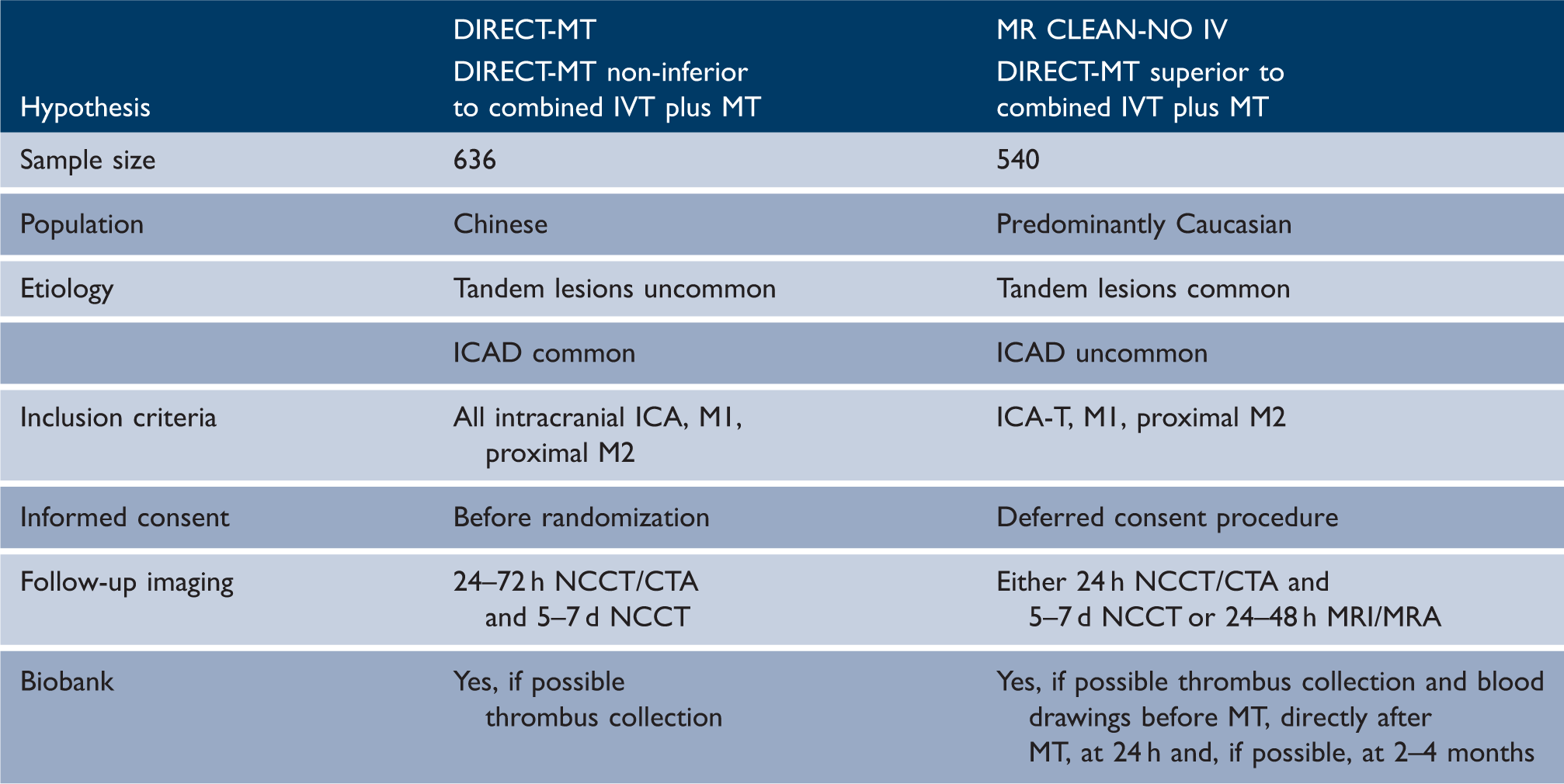
The study design has some limitations, potential risks. First, the large number of participating centers spread out across China could predispose to potential data quality issues. To overcome this, an independent CRO performs 100% data verification for all centers. Further, frequent investigator meetings are used to provide feedback and to discuss potential avenues for improvement. Second, we assume that a proportion of approximately 30% of all included patients could have underlying ICAD. 31 While there is no data from randomized clinical trials supporting stenting of these underlying lesions, this is commonly performed in China and other Eastern Asian countries. As this treatment might modify the effect of IVT, we collect detailed data during the intervention, including data concerning the used intracranial stents and concomitant medication and will perform a pre-defined subgroup analysis in patients with and without objectified ICAD.
Summary and conclusions
DIRECT-MT is a phase 3 RCT with PROBE design, assessing whether direct MT is non-inferior to IVT and MT in the Chinese population, the trial is tailored to the Chinese setting and will provide new insights regarding the necessity to use IVT before treatment with MT. This will aid in the refinement of acute ischemic stroke treatment in patient from China and the rest of the world.
Clinical trial registration
ClinicalTrials.gov Identifier: NCT03469206.
Roles and responsibilities
The committees are provided in Appendix 1.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DIRECT-MT is funded by the Stroke Prevention and Control Engineering Commission of National Health and Family Planning Commission of the People's Republic of China (GN-2017R0001), and Wu Jieping Medical Foundation.