
Abstract
Background
Currently there are multiple variations of imaging-based patient selection mismatch methods in ischemic stroke. In the present study, we sought to compare the two most common mismatch methods and identify if there were different effects on the outcome of a randomized clinical trial depending on the mismatch method used.
Aims
Investigate the effect of clinical and imaging-based mismatch criteria on patient outcomes of a pooled cohort from randomized trials of intravenous tenecteplase versus alteplase.
Methods
Baseline clinical and imaging scores were used to categorize patients as meeting either the DAWN mismatch (baseline NIHSS ≥ 10, and age cut-offs for ischemic core volume) or DEFUSE 2 mismatch criteria (mismatch volume > 15 mL, mismatch ratio > 1.8 and ischemic core < 70 mL). We then investigated whether tenecteplase-treated patients had favorable odds of less disability (on modified Rankin scale, mRS) compared to those treated with alteplase, for clinical and imaging mismatch, respectively.
Results
From 146 pooled patients, 71 received alteplase and 75 received tenecteplase. The overall pooled group did not show improved patient outcomes when treated with tenecteplase (mRS 0-1 OR 1.77, 95% CI 0.89–3.51, p = 0.102) compared with alteplase. A total of 39 (27%) patients met both clinical and imaging mismatch criteria, 25 (17%) patients met only imaging criteria, 36 (25%) met only clinical mismatch criteria and, finally, 46 (31%) did not meet either of imaging or mismatch criteria. Patients treated with tenecteplase had more favorable outcomes when they met either imaging mismatch (mRS 0–1, OR 2.33, 95% CI 1.13–5.94, p = 0.032) or clinical mismatch criteria (mRS 0–1, OR 2.15, 95% CI 1.142, 8.732, p = 0.027) but with differing proportions.
Conclusion
Target mismatch selection was more inclusive and exhibited in a larger treatment effect between tenecteplase and alteplase.
Introduction
The exact selection criteria of patients with an ischemic stroke for therapy with either thrombolysis or thrombectomy remain a controversial topic. 1 As time progresses, there are more trials being completed with varying inclusion and exclusion criteria, such as the DAWN trial 2 which required a mismatch between clinical deficit and age-based ischemic core volumes. The EXTEND IA, 3 DEFUSE 3, 4 and Australian tenecteplase trials 5 used an imaging-based target (perfusion-core) mismatch selection criteria for patients with a large vessel occlusion to show a significant treatment effect, but with different imaging perfusion-core criteria to define the mismatch. Alternatively, the negative Alteplase versus tenecteplase for thrombolysis after ischemic stroke (ATTEST) trials 6 did not require any tissue-based imaging selection which suggests that strict inclusion criteria using a mismatch are necessary but which criteria are desirable remain unknown. Importantly, the statistical evidence supporting the validity of these varying imaging or clinical inclusion/exclusion criteria is difficult to directly compare or lacking. As a result, there are now multiple means of classifying patients based on a treatment target which requires direct comparison to investigate the criteria’s effect on an included patient populations’ treatment responsiveness, clinical outcomes, and the number of eligible/excluded patients. It is a challenge to determine which imaging method is superior to the others in terms of best identifying reperfusion therapy responders and excluding those who are either likely to be harmed or who have a good natural history regardless of treatment. Therefore, in the present study, we sought to investigate the effect of clinical and imaging-based mismatch criteria on outcomes of a pooled dataset of randomized clinical trials of ischemic stroke where patients received either intravenous tenecteplase or alteplase. We hypothesized that the use of both clinical-core mismatch and target (perfusion-core) mismatch imaging selection criteria would translate the enhanced clinical outcomes of patients treated with tenecteplase over alteplase compared to non-mismatch patients, but that the two different mismatch selection criteria would include different patients, and hence lead to different treatment effect sizes in a pooled cohort of patients retrospectively analyzed from two clinical trials of tenecteplase versus alteplase. 7
Methods
We pooled data from the Australia-TNK 5 and ATTEST 6 trials and performed retrospective analysis on the enrolled patients. These studies were approved by the local institutional review committees and each participant provided written informed consent.
Imaging acquisition
For both studies, baseline computed tomography (CT) imaging included non-contrast CT (NCCT), CT perfusion (CTP), and CT angiography (CTA) with at least 80 mm of coverage. Follow-up NCCT and CTA were performed with the same acquisition as the baseline scan in ATTEST and at 24–48 h after thrombolysis. Follow-up imaging for the Australia-TNK study was on 1.5 T or 3 T MRI scanners (Siemens Avanto, or Skyra).
Pooled imaging analysis
Individual patient imaging was centrally analyzed with commercial software (MIStar, Melbourne, Australia), blind to clinical status and treatment allocation. Image analysis was performed by two stroke neurologists and a clinical scientist. All perfusion imaging was processed using the singular value deconvolution (SVD) algorithm with delay and dispersion correction and previous validated and equivalent thresholds 8 were applied to measure the baseline penumbra and ischemic core volume. 9 The perfusion lesion was defined as tissue with a delay time (DT) of >3 s and the ischemic core as tissue within the perfusion lesion (DT > 3 s) but with a cerebral blood flow of <30% of normal tissue as determined from SVD output. 10 The penumbra was defined as tissue within the perfusion lesion but not within the ischemic core.8,11 The mismatch ratio was determined as the ratio of the perfusion lesion volume to the volume of the ischemic core. Severe hypoperfusion was defined as DT > 8 s.
All baseline CTAs were assessed centrally for occlusion status and site of occlusion. For the pooled analysis, we classified baseline occlusion status as either (i) normal, (ii) partial (using dynamic CTP source images to confirm/exclude residual antegrade flow by assessing if distal arterial branches filled with contrast prior to immediately beyond the occlusion), or (iii) complete occlusion (no antegrade flow). 12 Patients with normal baseline CTA were not included in the recanalization assessments.
Brain hemorrhage outcomes were the occurrence of any parenchymal hematoma (PH), and large PH (PH2), as defined by the Second European-Australasian Acute Stroke Study (ECASS-2).
Imaging mismatch classification
We then classified patients as having target mismatch or no target mismatch based on whether they met target mismatch criteria (absolute mismatch volume >15 mL, mismatch ratio >1.8, baseline ischemic core <70 mL, and volume of severely hypoperfused tissue <100 mL, Illustrative examples of target mismatch in Figure 1).
4
Infarct growth was defined as the growth from baseline CTP ischemic core volume to 24–48 h NCCT or 24 h DWI. All imaging analysis was performed by AB who did not have an analytic role in the previous trials.
Illustrative examples of target mismatch. The top imaging has substantial penumbral volume (green) and a small ischemic core (red) and is therefore classified as having target mismatch. The middle image has a perfusion lesion which is too small (<15 mL) and does not meet the target mismatch criteria. The bottom image has a large ischemic core (>70 mL) and also does not meet the target mismatch criteria.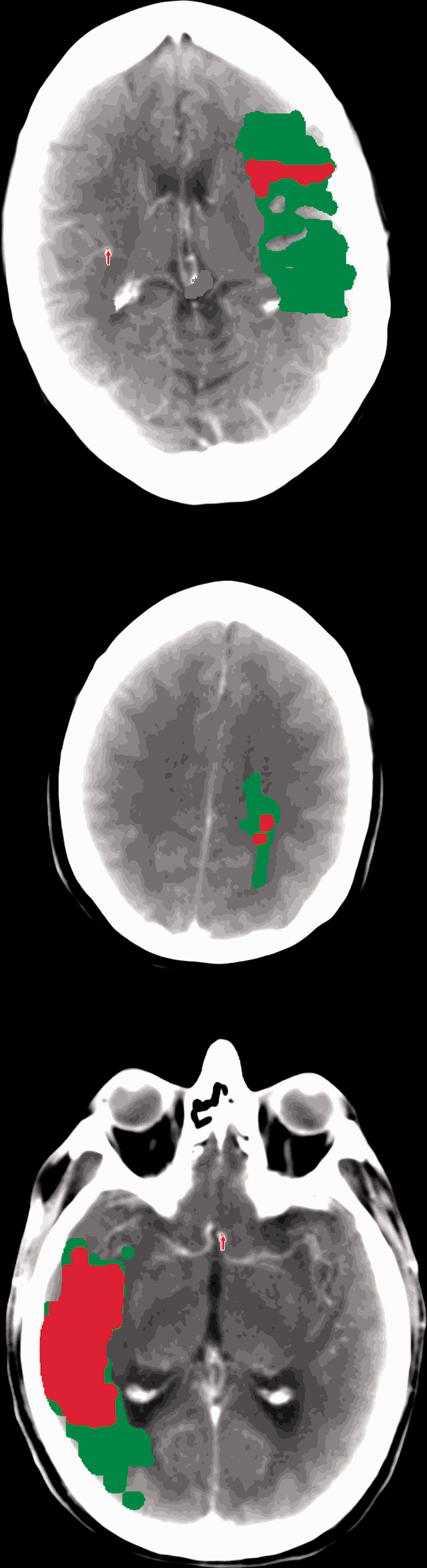
Clinical-core mismatch classification
Using the mismatch criteria from the DAWN trial, 2 patients were classified into one of three categories. Category A was patients 80 years of age or older, a score of 10 or higher on NIHSS, and CTP ischemic core volume of less than 21 ml. Those in Category B were younger than 80 years of age, had a score of 10 or higher on the NIHSS, and an ischemic core volume of less than 31 ml on CTP. Those in Group C were younger than 80 years of age, had a score of 20 or higher on the NIHSS, and had an infarct volume of 31 to less than 51 ml on CTP.
Statistical analysis
Statistical analysis was performed using Stata version 14. Firstly, we compared between trials the baseline clinical and reprocessed imaging data of Australia-TNK and ATTEST using Wilcoxon rank-sum test and Fisher exact tests where appropriate. We also compared the patient characteristics between the mismatch categories using Wilcoxon rank-sum test and Fisher exact tests where appropriate. Next, patients were categorized as either having imaging mismatch and/or clinical mismatch. We then compared the clinical outcomes of patients receiving either tenecteplase 0.25 mg/kg or alteplase 0.9 mg/kg between mismatch categories separately for patients with imaging mismatch or clinical mismatch using a fitted multivariable logistic regression model adjusted for patient age and baseline NIHSS, to calculate the odds ratio of mRS 0–1, mRS 0–2, and mRS 5–6. Imaging outcomes were rates of brain hemorrhage (any PH), infarct growth, and recanalization. Clinical characteristics compared included the baseline, 24 h, and change in NIHSS, patient age, and time to treatment.
Results
Comparison between treatment groups.
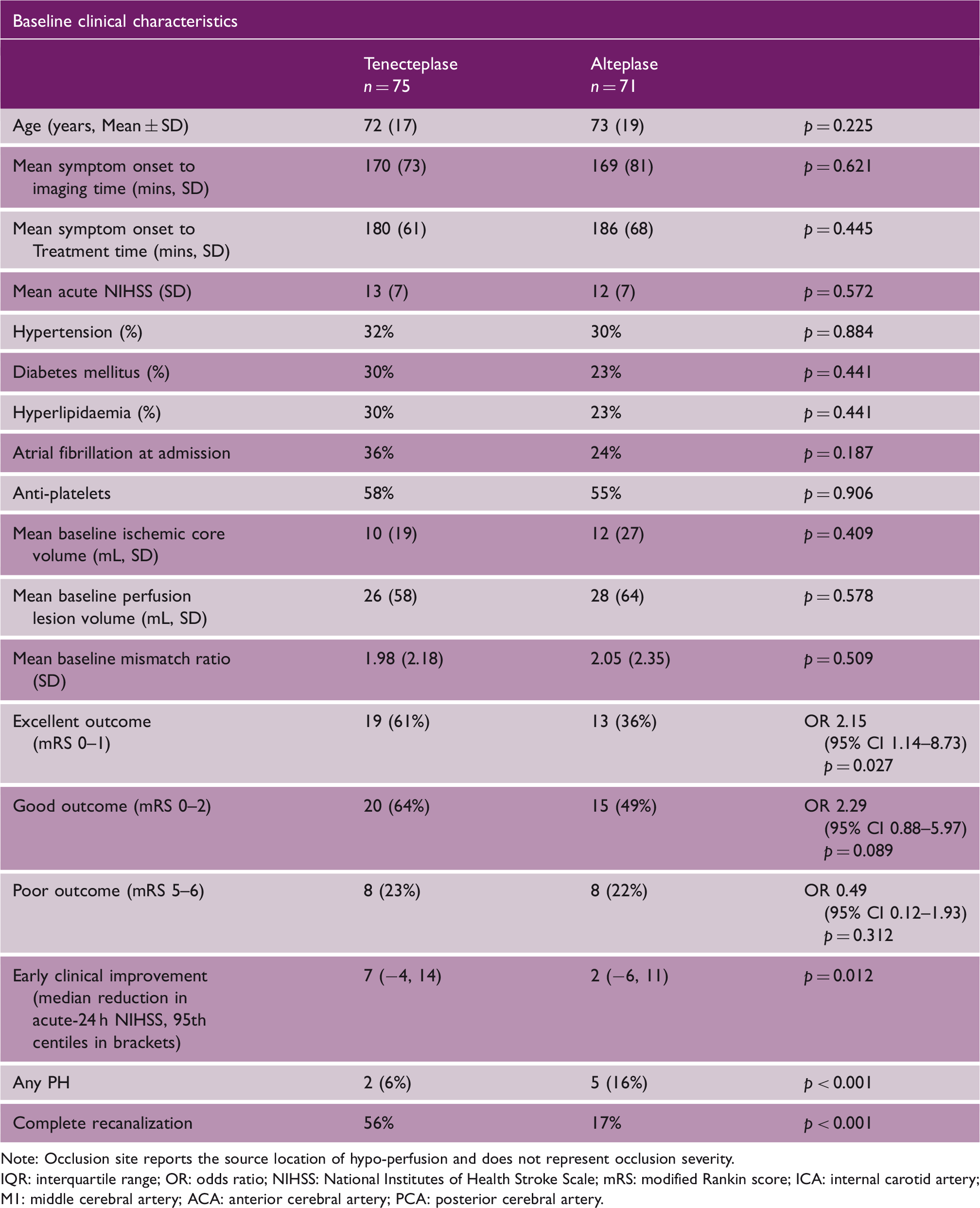
Note: Occlusion site reports the source location of hypo-perfusion and does not represent occlusion severity.
IQR: interquartile range; OR: odds ratio; NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin score; ICA: internal carotid artery; M1: middle cerebral artery; ACA: anterior cerebral artery; PCA: posterior cerebral artery.
Pooled analysis (clinical-core vs. target mismatch agreement)
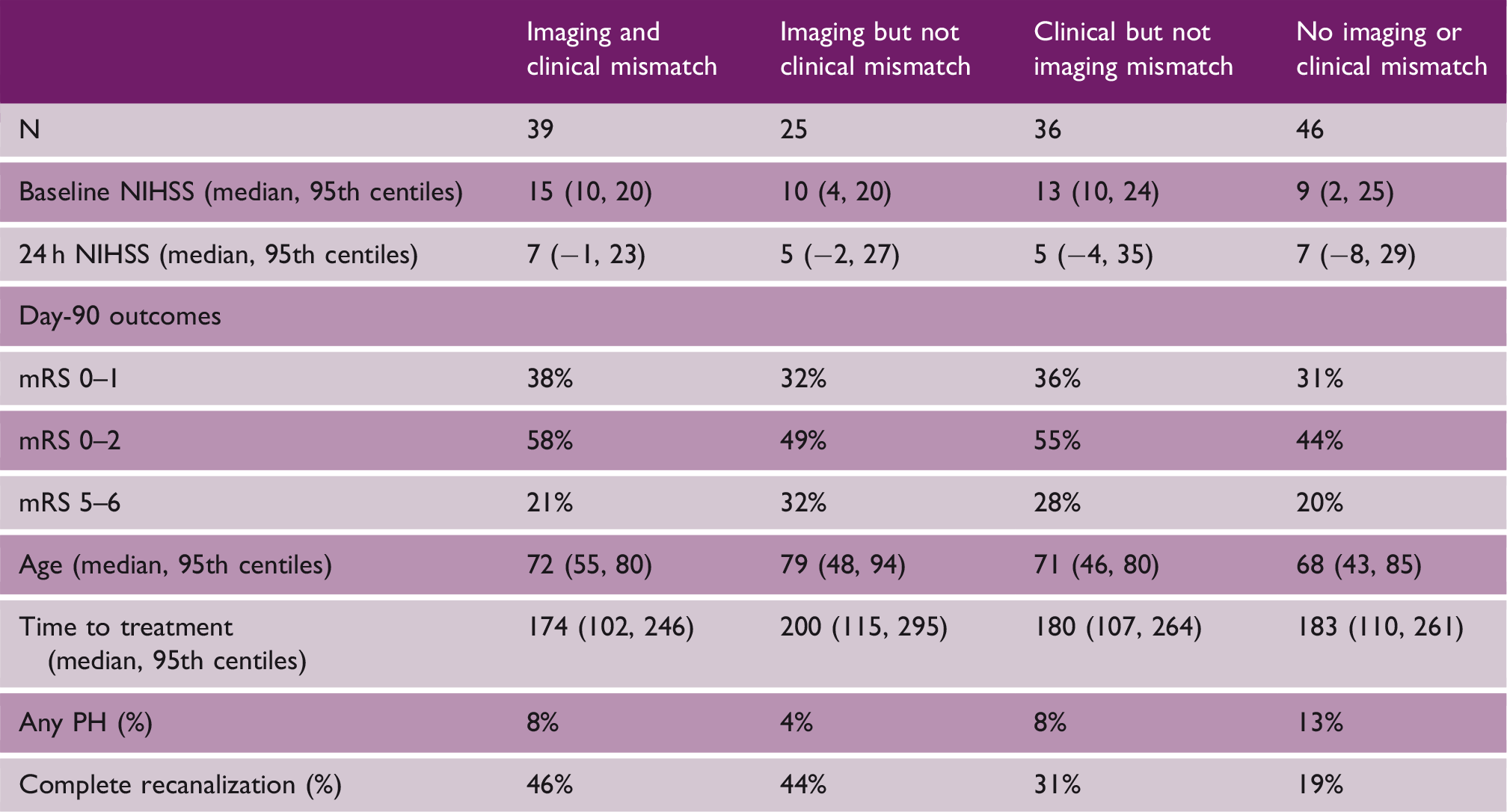
From the pooled data, a total of 39 (27%) patients met both the clinical-core and target mismatch criteria, 25 (17%) patients met the target mismatch but not the clinical-core mismatch criteria, 36 (26%) did not meet the target mismatch but did meet the clinical-core mismatch criteria, and finally 46 (32%) did not meet either of the imaging or mismatch criteria. Of the 25 patients who met the target mismatch but not the clinical-core mismatch criteria, 12 (48%) had a baseline NIHSS <10, and 13 (52%) had a baseline infarct core volume above the age-related clinical-core mismatch criteria. In the 36 patients that did not meet the target mismatch but did meet the clinical-core mismatch criteria, 26 (72%) had a baseline perfusion lesion below 15 mL, with the remaining 10 (28%) having a mismatch ratio <1.8. The median mRS of patients who met the clinical-core but not the target mismatch criteria was 2 (range 0–4).
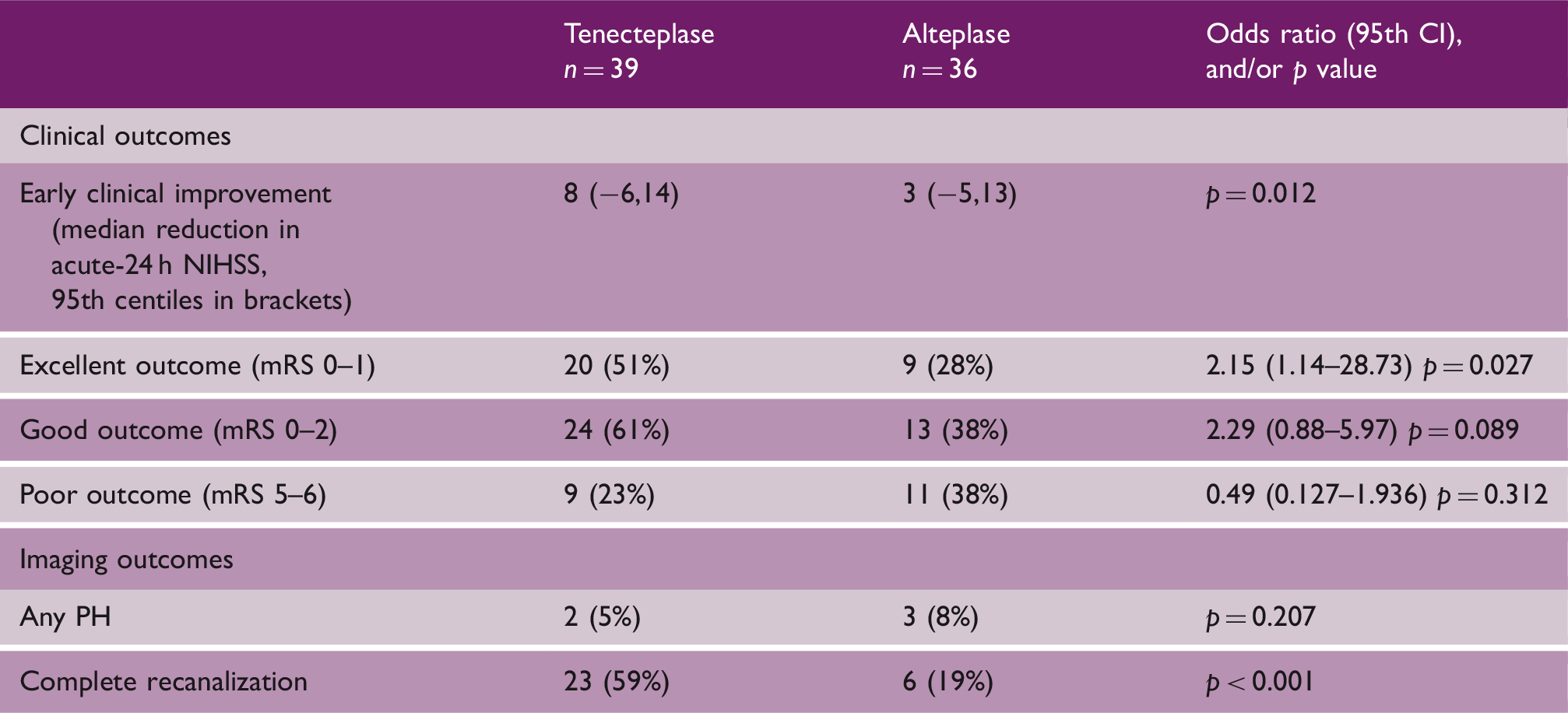
Of patients meeting both imaging and clinical mismatch (N = 39), tenecteplase resulted in significantly improved rates of excellent 90-day clinical outcome (mRS 0–1, OR 2.61, 95% CI 6.81–1.34, p = 0.018, Figure 2). Patients not meeting any mismatch criteria had the highest rate of PH (mismatch 7%, non-mismatch 13%, p = 0.044) and the lowest NIHSS change from baseline to 24 h (mismatch 7, non-mismatch 2, p = 0.037). Additionally, patients without clinical and imaging mismatch had a lower rate of complete vessel occlusion at baseline (mismatch 63%, non-mismatch 21%, p < 0.001) and recanalization at 24 h (mismatch 41%, non-mismatch 19%, p < 0.001).
A Box Forrest plot showing the impact of treatment mismatch selection criteria on the treatment effect of tenecteplase compare to alteplase in ischemic stroke patients.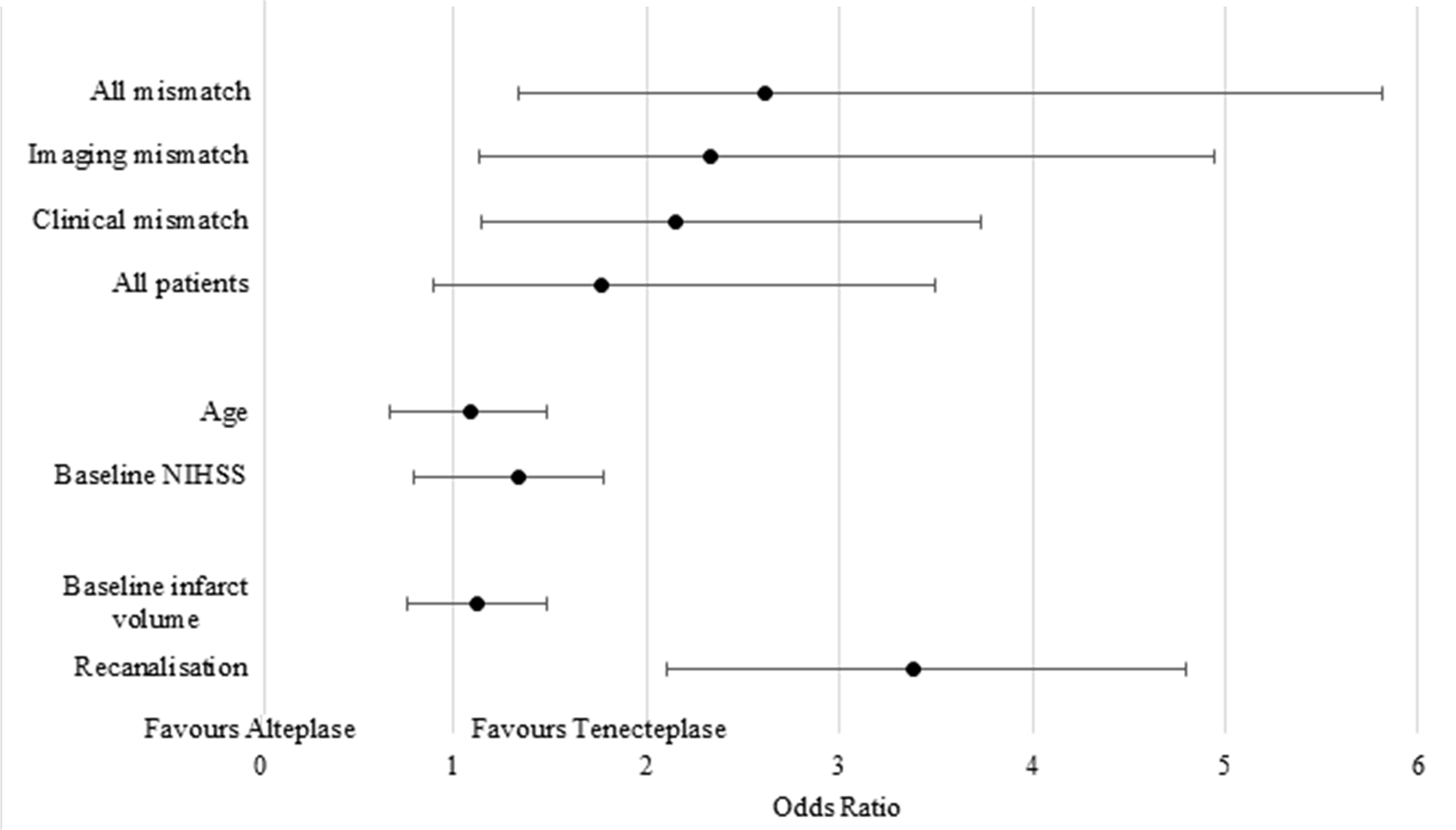
Pooled analysis (clinical-core mismatch patients): Tenecteplase versus alteplase
Comparison between treatment groups in patients meeting the clinical mismatch criteria
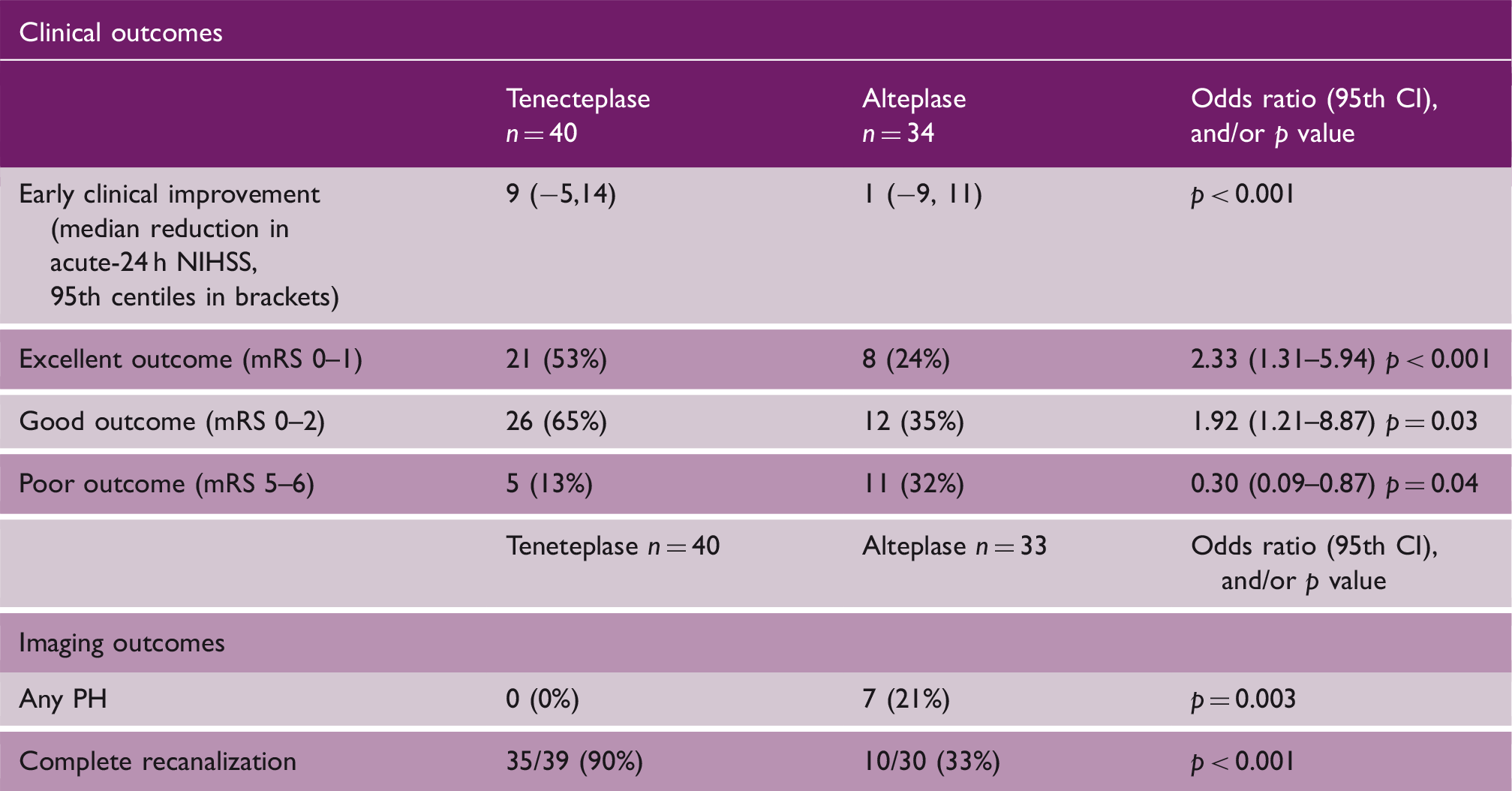
Of the 71 patients not fulfilling clinical-core mismatch criteria, 38 (53%) patients with age >80 were excluded due to baseline ischemic core volume >21 mL, the median being 27 mL. Fourteen patients less than 80 years old (20%) were excluded due to a larger ischemic core (>51 mL). Patients not fulfilling clinical mismatch who were treated with tenecteplase had significantly higher rates of complete recanalization (56% tenecteplase vs. 17% alteplase, p < 0.001). However, compared to alteplase patients, tenecteplase patients without clinical-core mismatch did not have better rates of excellent clinical outcome (mRS 0–1 OR, 0.973, 95% CI 0.357–2.651, p = 0.357), good clinical outcome (mRS 0–2 OR, 0.92, 95% CI 0.37–2.659, p = 0.598), or poor clinical outcome (mRS 5–6 OR, 1.021, 95% CI 0.323–3.229, p = 0.472). Tenecteplase patients without clinical-core imaging mismatch did not have less infarct growth (tenecteplase 22 mL vs. alteplase 10 mL, p = 0.206), although, again, rate of PH did tend to be lower (tenecteplase 5% vs. alteplase 16%, p = 0.163).
Pooled analysis (target mismatch patients): Tenecteplase versus alteplase
Comparison between treatment groups in patients meeting the imaging mismatch criteria
The imaging and clinical outcome measures of patients with/without mismatch criteria.
Of the 72 patients not fulfilling imaging mismatch criteria, 62(86%, Table 4) were excluded due to an absolute penumbral volume <15 mL, the majority being <10 mL (78%, 56/72). Seven patients (10%) were excluded due to a large ischemic core (>70 mL). Despite much better complete recanalization with tenecteplase (83% vs. 41% rtPA, p = 0.006), there were no differences in the rate of excellent clinical outcome (mRS 0–1, OR 0.86, 95% CI 0.32–2.24, p = 0.751), good clinical outcome (mRS 0–2, 0.71 OR, 95% CI 0.28–1.80, p = 0.471), or poor clinical outcome (mRS 5–6, OR 1.46, 95% CI 0.30–7.06, p = 0.342) in tenecteplase versus alteplase patients without target mismatch. Lastly, patients without target mismatch did not have less infarct growth (7 mL vs. 12.6 mL alteplase, p = 0.544), or lower rates of PH (tenecteplase 6% vs. alteplase 8%, p = 0.692) with tenecteplase.
Discussion
In the present analysis, we have demonstrated that in a pooled population comprising of two randomized tenecteplase versus alteplase trials, that tenecteplase results in significantly better clinical outcomes regardless of the mechanism of “mismatch” selection. Additionally, we compared the impact of two different mismatch criteria on the results from randomized trial data comparing tenecteplase to alteplase and found that patient selection with target mismatch was more inclusive and resulted in a larger treatment effect compared to clinical-core mismatch selection. We have previously shown that applying multimodal CT-based selection criteria significantly enhanced a studies ability to detect a clinical improvement in patients due to tenecteplase treatment, due to a higher rate of effective reperfusion seen with tenecteplase. 13 In this study, however, we compared different patient selection methods to show that the imaging-based target mismatch approach resulted in a lower proportion of hemorrhages and poor clinical outcome in the tenecteplase-treated group (but not in the clinical-core mismatch selected group).
Importantly, these results demonstrate that applying patient selection to a trial dataset substantially increases the power to detect a treatment effect (if there is one). This is evident as roughly one-half of the patient cohort was excluded from some analysis due to failure to meet any criteria, yet the overall results still showed a statistically significant result for treatment benefit of tenecteplase over alteplase. Without such mismatch criteria, it may be necessary to have a substantially larger sample size which could potentially take much longer to collect. The criteria which mostly prevented patient inclusion as clinical-core mismatch was the NIHSS cut off of 10. This cut-off ensures that patients have a substantial acute clinical deficit yet does not provide data on the tissue status of patients, such as occlusion location, perfusion lesion volume, or ischemic core volume. For thrombectomy, confirmation of a large vessel occlusion would be required; however, when considering intravenous thrombolysis, visible occlusion is not mandatory. Therefore, the NIHSS cut-off in clinical-core mismatch criteria excludes a substantial number of patients with “mild” stroke but without a large vessel occlusion who may benefit from thrombolysis, and as such the generalizability of this classification may be limited. However, both the clinical and imaging mismatch approaches resulted in an overall treatment responsive result to thrombolysis with tenecteplase compared against alteplase, and less poor outcomes using the target mismatch approach.
Several study limitations should be mentioned. This analysis was performed post hoc on a patient population which had already been screened and may not be representative of every day clinical practice. Next, the DAWN criteria have been published primarily in only patients with a thrombectomy treatable large vessel occlusion, whereas the current patient cohort was not required to have a large vessel occlusion in order to be randomized into one of the two trials making up this cohort. This may partially explain some of the lack of generalizability found by this analysis since large vessel occlusion patients often have a high baseline NIHSS and more would have been included. Importantly, there are limited guiding criteria with which to select non-large vessel occlusion patients for thrombolysis currently which may limit the generalizability of these study results.
In conclusion, we have demonstrated that patient selection with a mismatch approach provides greater power to detect change for reperfusion therapy clinical trials but selecting the more severe end of patients on the ischemic stroke spectrum. Moreover, target mismatch-based selection appeared to be more inclusive for a thrombolysis cohort and exhibited in a larger treatment effect between the two interventions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
WSO884529 Supplemetal Material - Supplemental material for Comparing mismatch strategies for patients being considered for ischemic stroke tenecteplase trials
Supplemental material, WSO884529 Supplemetal Material for Comparing mismatch strategies for patients being considered for ischemic stroke tenecteplase trials by Andrew Bivard, Xuya Huang, Christopher R Levi, Bruce CV Campbell, Bharath K Cheripelli, Chushuang Chen, Dheeraj Kalladka, Fiona C Moreton, Ian Ford, Stephen M Davis, Geoffrey A Donnan, Keith W Muir and Mark W Parsons in International Journal of Stroke
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.