
Abstract
Introduction
Perihematomal edema in intracranial hemorrhage is influenced by free hemoglobin clearance and inflammation. Serum Haptoglobin (Hp) binds free hemoglobin, affecting heme clearance and free radical production. Of the three Hp phenotypes, Hp 1-1 has the greatest effect on free hemoglobin clearance.
Aim
To determine if individuals with Hp 1-1 phenotype have different rates of early perihematomal edema formation as compared to those with Hp 2-1 and Hp 2-2.
Methods
We determined Hp phenotype, intracranial hemorrhage volume, and rate of early change in perihematomal volume in participants from three prospectively collected intracranial hemorrhage cohorts. The association of Hp phenotypes 1-1, 2-1, 2-2, with early change in perihematomal volume, while controlling for key clinical characteristics was analyzed using a multivariate model.
Findings
One-hundred and sixty-six participants were included: 73 (44%) female, 41 ( 25%) African Americans, 34 (20%) diabetics, 133 (80%) with hypertension, and 75 (45%) active smokers. There were 15 subjects with Hp phenotype 1-1, 86 with 2-1, and 65 with 2-2. In fully adjusted analysis, Hp 1-1 had a significantly increased estimated mean rate of early change in perihematomal volume at 1.15 (95% confidence interval 0.58–1.71) as compared to all other Hp 2-1 or Hp 2-2 containing phenotypes (0.30, 95% confidence interval 0.06–0.54; 0.29 95% CI 0.02–0.56). Neither mortality nor discharge mRS differed between Hp phenotypes.
Conclusion
Haptoglobin phenotype is associated with early change in perihematomal volume. Hp 1-1 phenotype had significantly increased mean rate of early change in perihematomal volume within the first 96 h, suggesting that haptoglobin phenotype may be a key player in understanding the multiphasic progression of perihematomal volume in spontaneous intracerebral hemorrhage. A larger prospective observational study is warranted.
Introduction
Intracerebral hemorrhage (ICH) accounts for approximately 10% of all strokes in the US and is the deadliest form of stroke. 1 The pathophysiology of brain injury in ICH is thought to be biphasic. The first phase occurs within the first hours of hemorrhage where neuronal injury from the toxic effects of hemorrhage is augmented by mechanical forces from hematoma expansion and cerebral edema. 2 Brain edema begins as early as the first minutes after ictus and causes increases in intracranial pressure (ICP). 3 Edema formation is driven by the secondary effects of progressive erythrocyte lysis, hemoglobin (HG) toxicity, neuro-inflammation, and blood brain barrier (BBB) disruption, which contribute to increased perihematomal edema localized immediately adjacent the clot. 2 This resulting perihematomal edema has been associated with worse outcomes in studies of the medical and surgical therapies for ICH.4,5
The second pathophysiologic phase of brain injury in ICH includes oxidative and inflammatory response to injury. This is facilitated by free HG released from the lysis of red blood cells (RBCs). 6 Haptoglobin is an acute phase reactant that scavenges free HG, is excreted from the liver, and found in blood. 7 Haptoglobin limits the reducing effects of free HG through binding, clearance, and production of anti-inflammatory cytokines. 3 In the absence of haptoglobin binding, free HG causes glial activation, BBB disruption, and cell death. 8
Humans have two major Hp alleles, Hp1 and Hp2, with three diploid combinations; Hp1-1, Hp2-1, Hp2-2. 9 The single Hp2 allele is influenced by a series of mutations causing intragenic duplication of an Hp1 DNA fragment. This polymer has the lowest bioavailability of all Hp molecules for HG and potentiates local inflammation. 7 The biological properties of Hp 2-2 may be facilitated, not only by decreased HG binding, but also by the modification of the innate CD163-based macrophage response to injury from free HG. 10 The Hp 1 protein may have superior abilities to reduce the oxidative effects of free HG and has increased associated clearance of free HG as compared to Hp-2. 11
The deleterious biological effect of the diploid Hp 2-2 phenotype has been associated with negative secondary effects of brain hemorrhage in aneurysmal subarachnoid hemorrhage including an increased risk of vasospasm and cerebral salt wasting. 12 We have previously reported improved recovery associated with the Hp 1-1 phenotype in ICH. 13 We believe that this outcome may be mediated by the varying efficacy of heme clearance via Hp-mediated mechanisms and the resultant secondary inflammatory response. 6 Furthermore, data from Asian and American cohorts suggest that both the volume of edema formation and rate of early perihematomal edema formation (ePHE) are associated with increased mortality. 8 Therefore, our primary outcome of interest is ePHE, while controlling for hematoma volume, rather than overall hematoma volume alone. We believe that this biologic model is supported by the literature, and the fact that disease models have demonstrated haptoglobin, in increasing concentrations, in the tissue immediately adjacent the hematoma. 2
Aim
To determine if individuals with Hp 1-1 phenotype have different rates of early perihematomal edema formation as compared to those with Hp 2-1 and Hp 2-2. We hypothesized that perihematomal edema in general and specifically ePHE would be affected differently across diploid Hp phenotypes due to the varied HG binding mediated by Hp, modifying secondary events such as inflammation and perihematomal edema.
Methods
Patient population
Subjects were recruited from three prospectively collected patient populations between 1st March 2010 and 29th July 2017. Patients presenting with an acute sICH to the Johns Hopkins Hospital or the Massachusetts General Hospital that were recruited into ongoing ICH trials were included in this study. 14 The study was approved by these two participating sites' institutional review boards. The third population was identified as a predetermined subgroup enrolled in the MISTIE III trial. The study design of MISTIE III, a randomized controlled, open-label blinded endpoint phase 3 trial, has been previously described, with local participating centers obtaining institutional review board and ethics committee approval. 15 Subjects identified and included in the present study from the MISTIE III cohort were limited to those who underwent medical management. No subjects that were exposed to surgical intervention were included; details of medical reversal were not available for all sites for all sites. Inclusion of these participants into the current study required each identified subject meet the following criteria; age 18 or older at admission, the presence of an initial and follow-up CT within 96 h, survival to 96 h, and no surgical clot reduction. Those not meeting inclusion criteria or with incomplete demographic or clinical data, were excluded from this investigation. Baseline demographic data included in the present analysis included: age, sex, race, diabetes (DM), hypertension (HTN) (SBP > 140 mmHg), and hyperlipidemia (HLD) (low-density lipoprotein cholesterol > 130 mm/dL), smoking status, prior sICH, and use of anti-platelets or additional anticoagulants. Management or reversal of antiplatelets was left to the discretion of the managing medical team at each institution. Patients who were taking coumadin at the time of presentation were not included in the study. The management of any additional anticoagulation was left to the discretion of the managing medical team in charge of the care of the patient. Each participant had blood samples collected prior to administration of any blood product and stored at −20℃ until analysis. Hp Phenotyping was performed in an internationally recognized, CLEA certified lab using polyacrylamide gel electrophoresis to divide patients into three groups based on Haptoglobin phenotype (1-1, 2-1, 2-2) as completed in previous analysis. 12 To ensure the fidelity of Hp electrophoresis, access to appropriate collection methods were required (samples collected prior to blood product administration, consent received, access to cold storage etc.). As a result, Hp samples were not able to be collected on many potentially eligible participants during the study period. Intracerebral hemorrhage was confirmed by non-contrast head CT. Timing of follow-up interval CT scans was left up to the treatment teams discretion based on standard medical management and institutional protocols of the included centers. For this study, the apriori definition of follow-up interval CT scans was defined as the first clinically indicated CT scan, with a maximal time limit set, requiring included all included participants to have a follow-up interval scan within the first 96 h of admission. Early perihematomal edema formation (ePHE) is defined as edema occurring within the first 96 h. 8 Given the observational nature of this investigation, the apriori decision was made to quantify the rate of ePHE as the difference in ePHE volume between follow-up and initial CT head divided by hours between scans, providing results as change in cc's/h.5,16 This decision was made to provide the most conservative estimate for rate of change of ePHE within this sample. Semiautomated, computerized volumetric analysis of CT scans was used to assess intracerebral hemorrhage volume as well as perihematomal edema. Perihematomal edema volume was defined as an area of hypodensity immediately adjacent to the area of hemorrhage, and hypointense in comparison to the other unaffected hemisphere. Expert reviewers were blinded to the Haptoglobin phenotype. Secondary outcomes of interest included: mortality, and functional recovery on discharge, defined by the modified Rankin score (mRS). While all subjects included in the present study were required to have complete demographic and clinical variables, subjects were not excluded from the final cohort if secondary analysis variables were missing.
Additional clinical, imaging, biological and outcome variables were considered when designing the present study. Such variables considered included, but not limited to, duration intensive care admission, duration of intubation, hematoma location, Glasgow Coma Scale, and National Institutes of Health Stroke scale; however, these variables were inconsistently collected between cohorts as these were not defined apriori. As such these variables were excluded from analysis, including secondary analysis to limit type 1 error.
Statistical analysis
Haptoglobin genotype associated with demographics and clinical characteristics
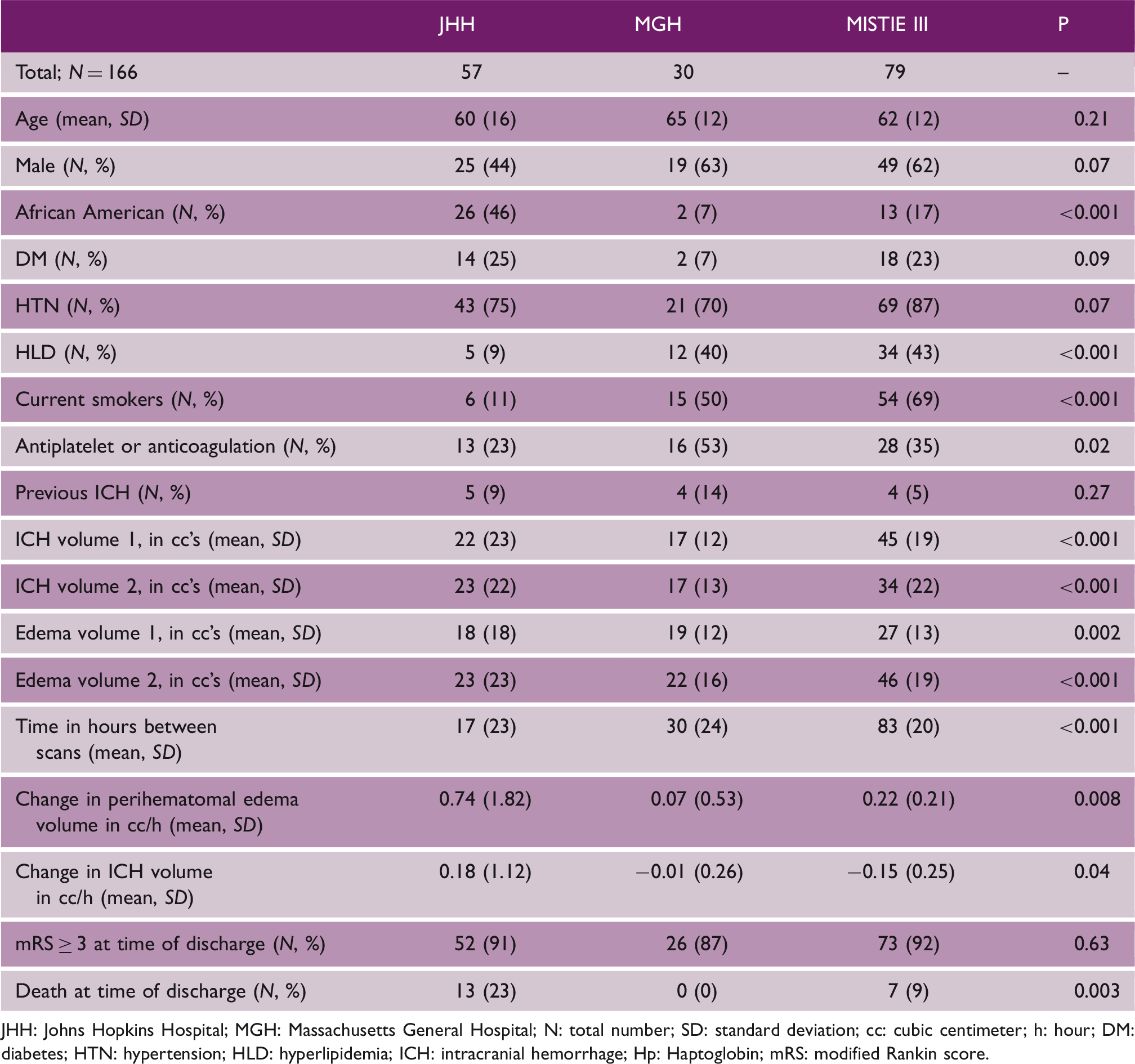
JHH: Johns Hopkins Hospital; MGH: Massachusetts General Hospital; N: total number; SD: standard deviation; cc: cubic centimeter; h: hour; DM: diabetes; HTN: hypertension; HLD: hyperlipidemia; ICH: intracranial hemorrhage; Hp: Haptoglobin; mRS: modified Rankin score.
Haptoglobin phenotype associated with demographics and clinical characteristics
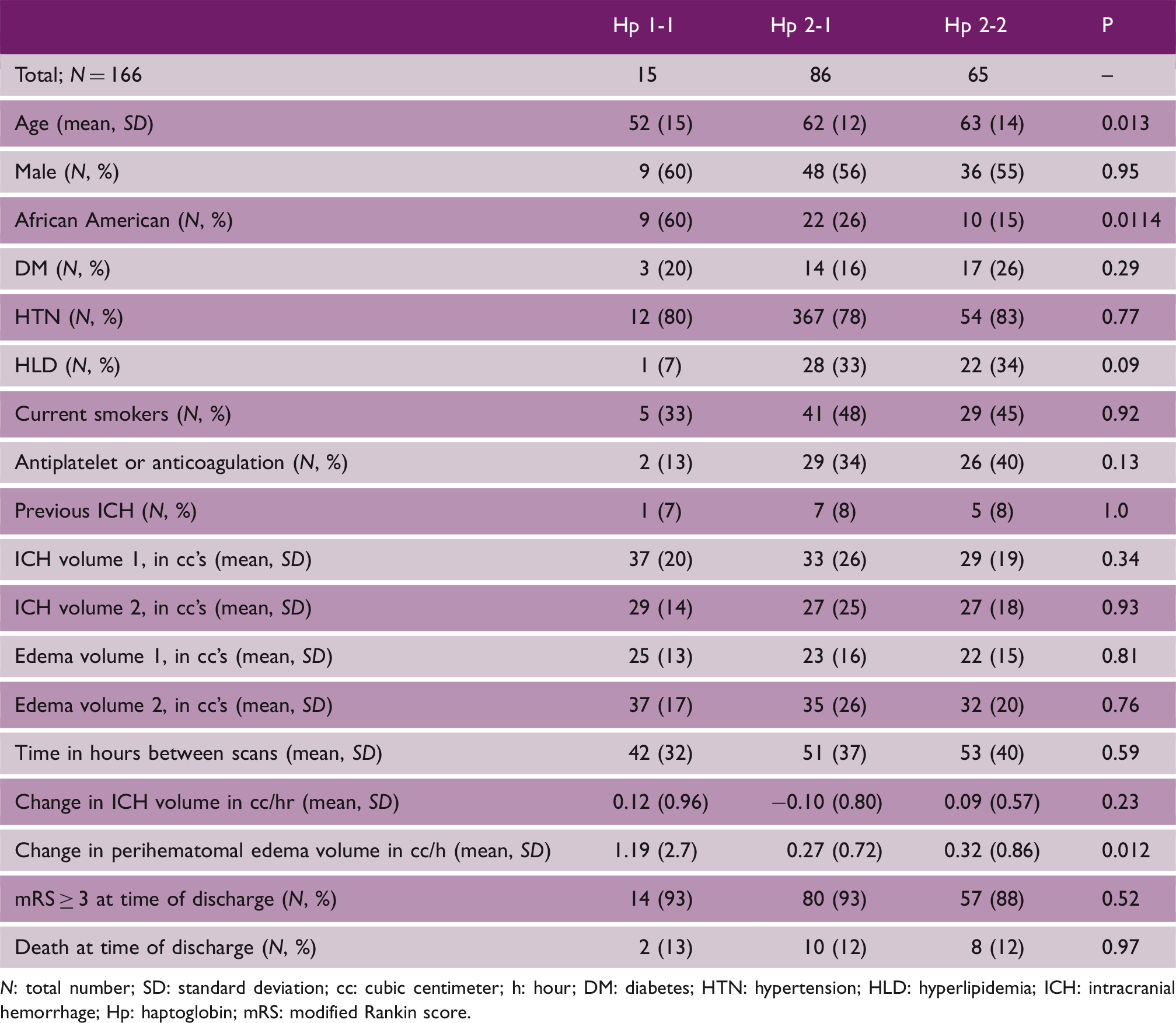
N: total number; SD: standard deviation; cc: cubic centimeter; h: hour; DM: diabetes; HTN: hypertension; HLD: hyperlipidemia; ICH: intracranial hemorrhage; Hp: haptoglobin; mRS: modified Rankin score.
Beta estimate for effect of each demographic and clinical characteristic on rate of change in early perihematomal edema (ePHE)
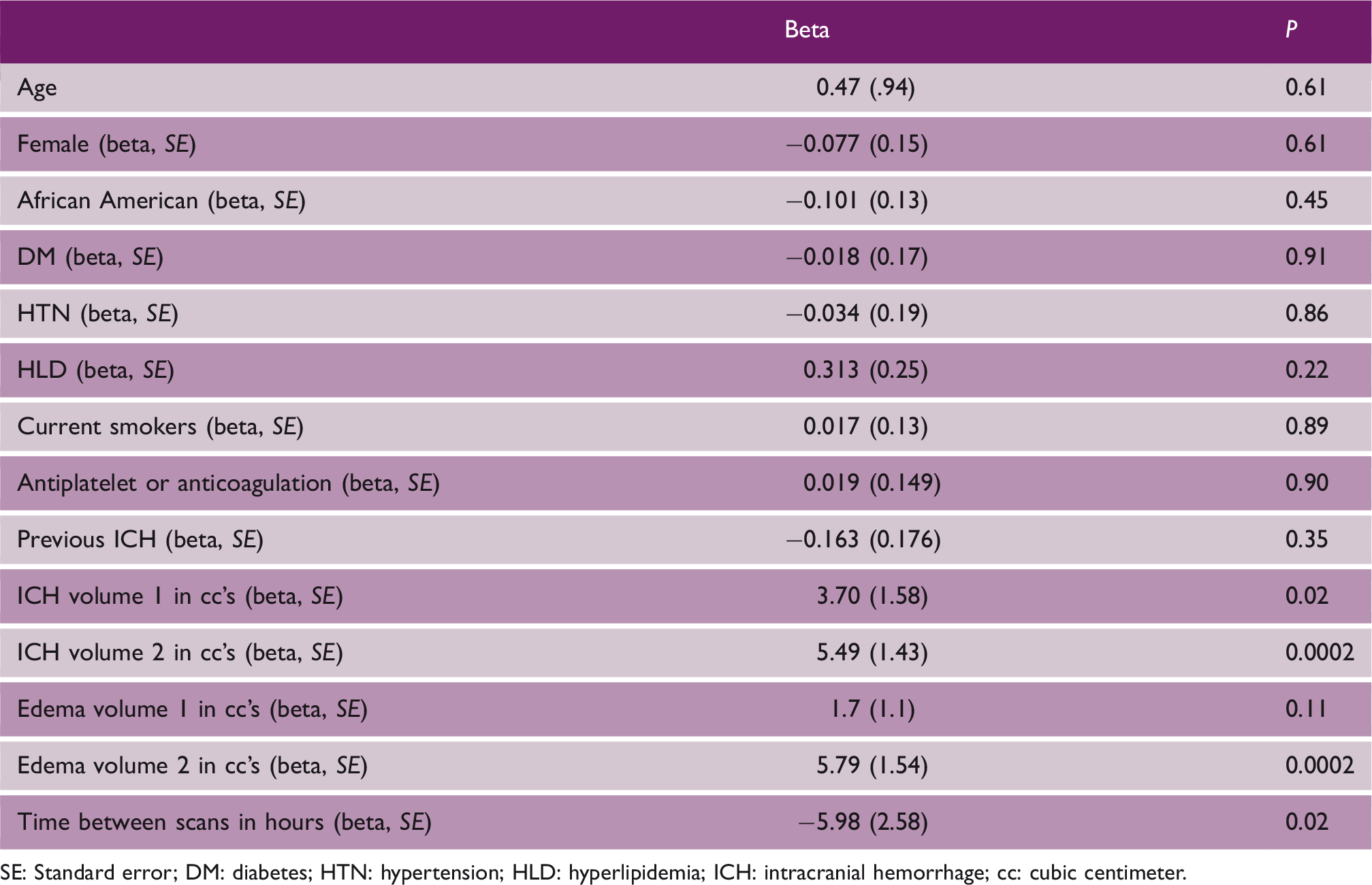
SE: Standard error; DM: diabetes; HTN: hypertension; HLD: hyperlipidemia; ICH: intracranial hemorrhage; cc: cubic centimeter.
Multivariate analysis incorporating linear and logistic regression was used to analyze the relationship between Haptoglobin phenotype and ePHE. Three models were initially proposed to determine the relationship of Haptoglobin phenotype to ePHE. These included an unadjusted model, a model adjusted for age, race, diabetes (DM), HTN, and smoking. A third and final model adjusting for change in ICH volume over time (cc/hr) was proposed. The included covariates age, race, DM, HTN, and smoking were selected based on our univariate results associating them with either ePHE or with Haptoglobin phenotype. Additionally, biologic plausibility was considered in covariate selection. The variables gender, HLD, and antiplatelet/coagulation medication were omitted given our limited power, the lack of biologic plausibly, and their similarity to other included variables.
Final analysis of haptoglobin phenotype predicting mortality, death at time of discharge, and poor mRS (mRS ≥ 3) was completed. mRS of 3 or greater was chosen as poor functional recovery given this outcome has been used in prior studies investigating cerebral edema and intracerebral hemorrhage. 17 Analysis of mortality and discharge mRS was completed using the models adjusted for previously; model 1, unadjusted, model 2 adjusted for age, race, HTN, DM, and smoking, model 3 adjusted additionally for change in ICH volume. All statistical analyses were done using SAS software (Cary, NC). Statistical significance was predetermined at p < 0.05.
Results
Our final cohort included 166 participants, with demographic and clinical characteristics by haptoglobin phenotype included in Table 1. Demographic and clinical characteristics between cohorts were well balanced with respect to age, gender, DM, HTN, and previous incidence of intracerebral hemorrhage (Table 2).
A total of 9% of the total study population (n = 15) were identified as Haptoglobin 1-1 genotypes. Fifty-two percent of the population were identified as Haptoglobin 2-1 (n = 86) and 39% (n = 65) were Haptoglobin 2-2 (Table 2). Table 2 shows the association of Hp genotype with demographic and clinical variables of our cohort, similar to the incidence by gender, race, and cardiovascular risk factors previously reported in the literature. 18 Importantly ICH volumes one and two, PHE volume at time one and two, and change in ICH volume were not associated with Hp. The mean time between scans was not significantly different between haptoglobin groups (p = 0.52; Table 2). The variable ePHE was significantly different between haptoglobin groups (p = 0.012). The association of demographic and clinical factors on ePHE within our cohort was investigated (Table 3). Initial ICH and PHE volume and as well as follow-up ICH and PHE volume were significantly associated with change in PHE.
Estimated mean rate of change in perihematomal edema (ePHE) by haptoglobin phenotype. Model 1: unadjusted effect of haptoglobin on perihematomal edema; Model 2: adjusted for age, race, diabetes, hypertension, smoking status; Model 3: model 2 plus change in intracranial hemorrhage volume over time (cc/hr.)
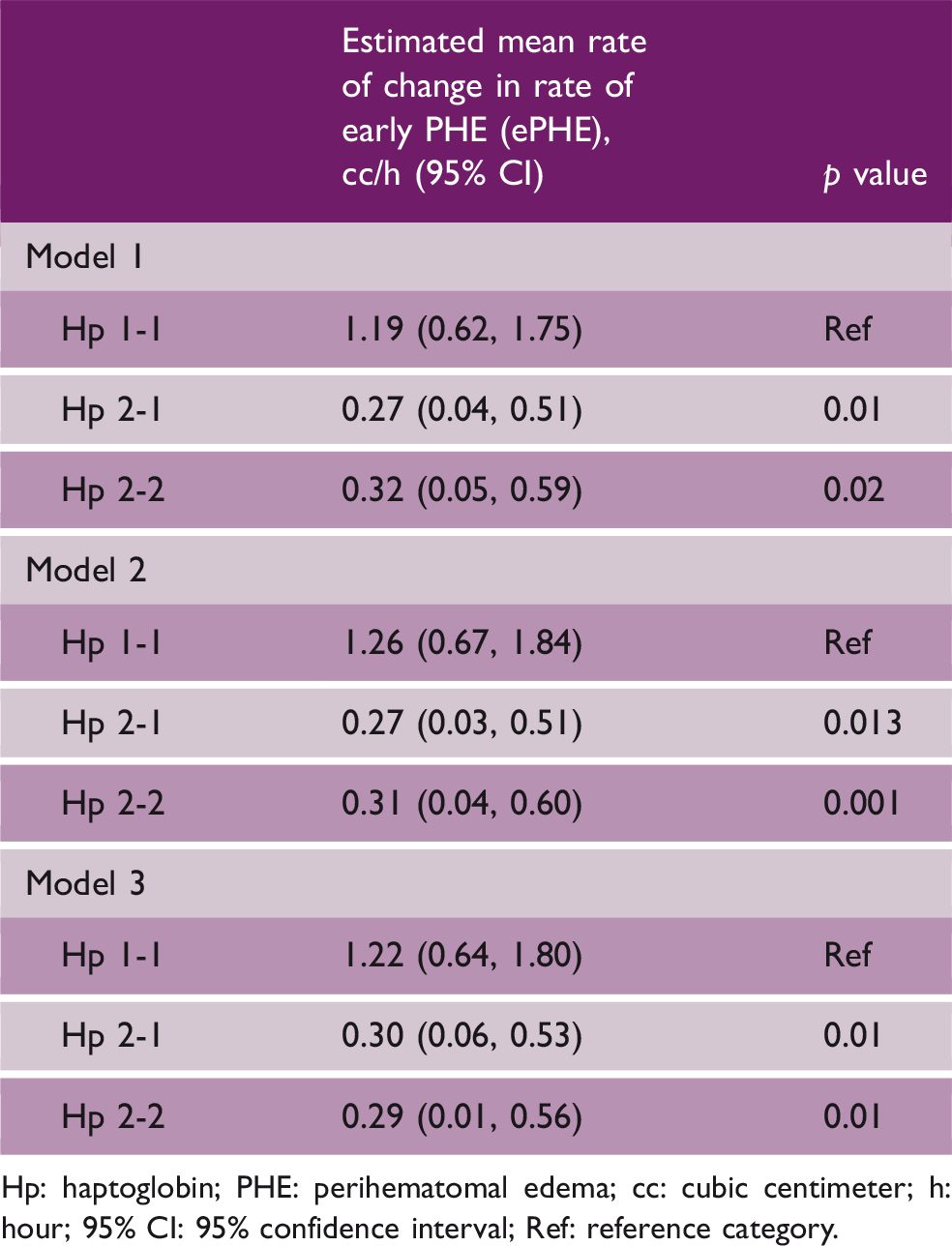
Hp: haptoglobin; PHE: perihematomal edema; cc: cubic centimeter; h: hour; 95% CI: 95% confidence interval; Ref: reference category.
Odds of mortality by haptoglobin phenotype. Unadjusted; odds of mortality predicted by Hp phenotype alone. Model 2; adjusted for age, race, diabetes, hypertension, and smoking. Model 3; adjusted for model 2 and change in ICH volume (cc/h)
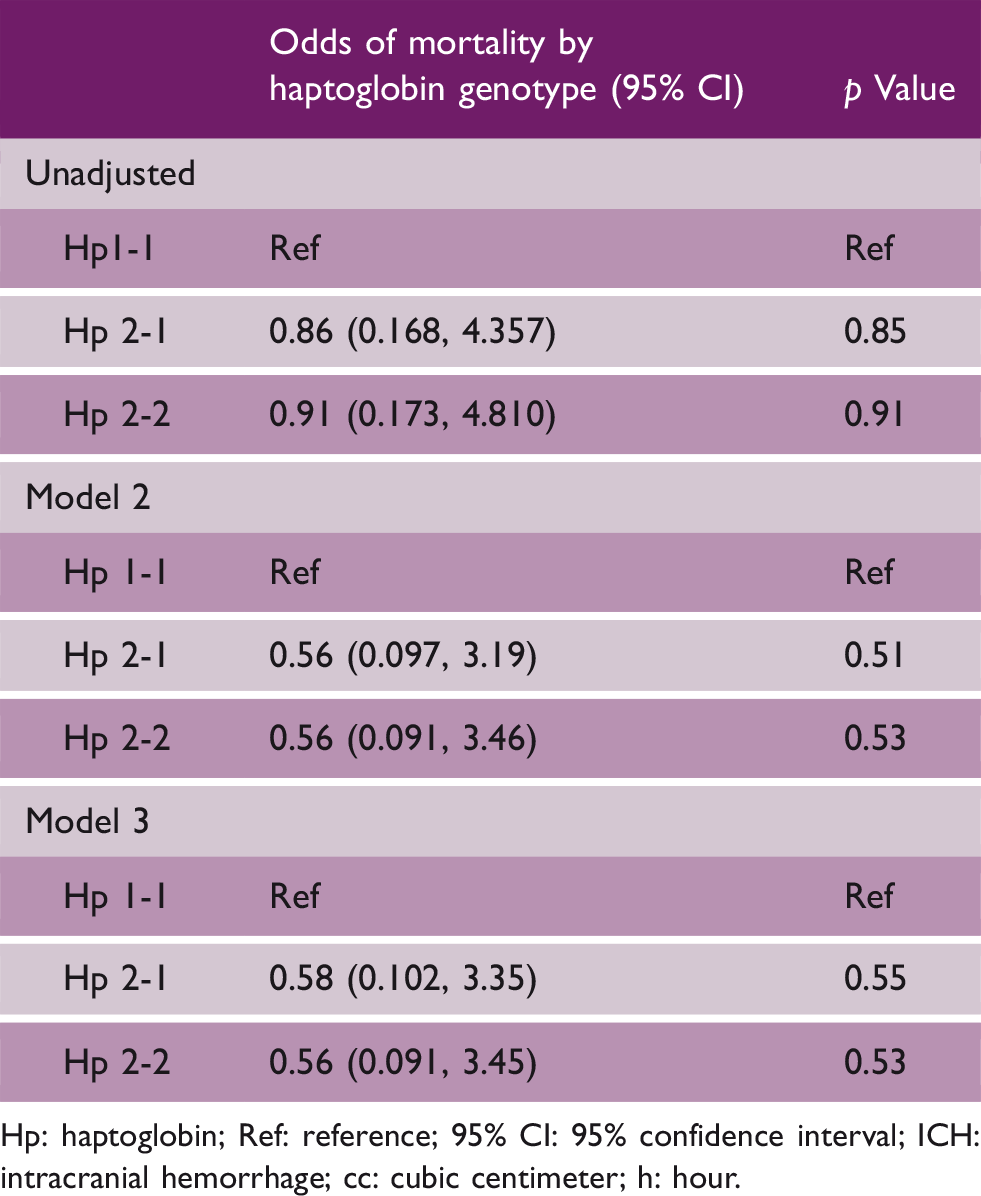
Hp: haptoglobin; Ref: reference; 95% CI: 95% confidence interval; ICH: intracranial hemorrhage; cc: cubic centimeter; h: hour.
Odds of poor mRS (≥3) by haptoglobin phenotype. Unadjusted; odds of poor mRS predicted by Hp phenotype alone. Model 2; adjusted for age, race, diabetes, hypertension, and smoking status. Model 3; adjusted for Model 2 and change in ICH volume (cc/h)
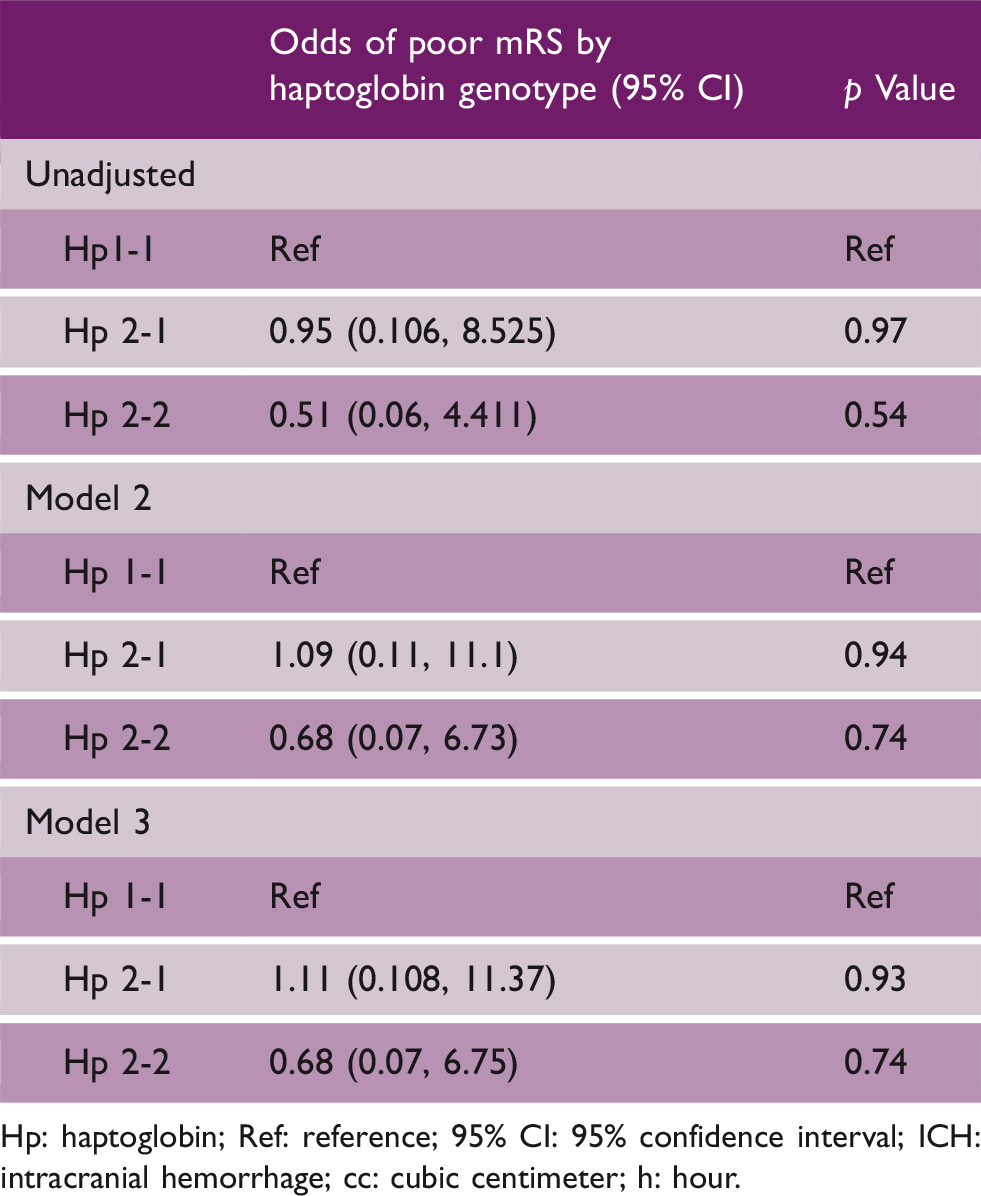
Hp: haptoglobin; Ref: reference; 95% CI: 95% confidence interval; ICH: intracranial hemorrhage; cc: cubic centimeter; h: hour.
Discussion
This is the first study to investigate the association of the rate of early perihematomal edema formation and haptoglobin phenotype. The proportion of Hp 1-1 and 2-1, 2-2 phenotypes within our study cohort is similar to national averages reported in the literature. 18 We observed increased rates of early perihematomal edema formation within the first 96 h in patients with the Hp 1-1 phenotype. This result is counter to our previously reported findings13,17 and our present study's primary hypothesis. This association, identifying increased ePHE formation with Hp 1-1 phenotype likely reflects the dynamic effect of early CD163 macrophage mediated 19 HG clearance on secondary brain injury and downstream inflammation; an observation that builds on earlier work investigating the role of Hp phenotype in sICH outcomes and recovery.13,20
The pathophysiology of PHE formation in ICH is complex and biphasic, 8 with the initial injury mediated primarily via mechanical hematoma formation augmenting brain injury through increased ICP. The second phase contributing to edema formation is driven, in part, by the effect of progressive erythrocyte lysis and resultant HG toxicity to the surrounding neuronal tissues. 2 Here in this perihematomal region, Hp scavenges free HG, which is then cleared via CD163-mediated mechanisms.20–22 The overall efficacy of Hp–heme–CD163-mediated clearance is related to overall perihematomal edema formation.2,3 While Hp-mediated heme clearance extends beyond the first 96-h period, 2 the temporal influence of efficient Hp–heme–CD163-mediated clearance on edema formation remains largely unknown. 19 The greater mean rate of ePHE observed for the Hp 1-1 subgroup in the present study, likely begins to elucidate the temporal effect of efficient Hp–heme–CD163-medicated clearance 19 within the perihematomal space early post ICH ictus.2,5
The CD163-mediated clearance of heme in the perihematomal space begins with erythrophagocytosis of RBCs recognized by externalized CD36. 23 These RBCs undergo complement mediated lysis 24 depositing free HG and iron in the perihematomal tissues. The ensuing degradation products have both direct and secondary neurotoxic effects on the surrounding neuronal tissues. This inflammatory injury disrupts basement membranes and tight junctions thereby increasing perihematomal edema. 3 Once HG is degraded, haptoglobin diffuses naturally across the BBB, 25 binding free HG and creating the Hp–HG complexes. These complexes in turn bind to monocyte CD163 receptors. This new Hp–HG–CD163 complex is more rapidly cleared, 26 where the efficacy of clearance is directly proportional to haptoglobin phenotype 27 and the magnitude clearance directly influences secondary injury. 27 The maximal protective effects are seen in those with Hp 1-1 phenotype 27 and when clearance is continued beyond three days post ictus. 28 While the temporal clearance of HG has been known, the temporal effect of CD163-mediated clearance on outcomes in ICH has only recently been described, 19 and is likely the mechanism explaining the discordance in the present study's findings with those previously reported.
In a rodent model of ICH investigating the effects of CD163-mediated clearance, 19 CD163−/− knockouts (i.e., those will less effective Hp–heme clearance 27 ) initially out performed wildtypes on neurocognitive evaluations, and exhibited a lower mortality rate during the first 48 h 19 post ictus. Furthermore, during the initial 48 h post ictus, CD163 + / + rodents (those with more efficient Hp–heme clearance 27 ) demonstrated hemorrhages of overall greater size. 19 However, when followed beyond the first 48 h, mortality increased and neurocognitive testing declined for the CD163 knockouts. 19
The observations from this rodent model parallel the observations of the present study in relation to the literature. Collectively our findings suggesting that inefficient clearance of hp–heme complexes early post ICH ictus may be protective regarding hematoma and edema volumes. This is clinically manifested by smaller early perihematomal edema volumes in those with inefficient heme clearance, as in the individuals with Hp 2-1, 2-2 phenotypes in the present study. However, when the observation period is not censored to first 96 h, as in the present study, the role of secondary neuronal injury manifested by HG degradation is amplified in those with decreased efficacy of heme clearance (i.e., Hp 2-1,2-2), and the downstream effect on long-term morbidity and mortality is seen. 29 In vitro ICH studies investigating Hp-mediated CD163 sequestration and clearance of heme suggest direct downstream effects on the oxidative environment within a hematoma. 30 It is therefore this secondary phase of cerebral injury driven by neuronal inflammation in the setting of ICH, exacerbated in those with Hp 2-1, 2-2 phenotypes, which contribute to the worst overall outcomes reported elsewhere in the literature.12,13,31 Therefore, our observation that Hp 1-1 had greater ePHE would be congruent with our growing understanding of the phasic relationship between Hp–heme–CD163 clearance and the overall nonlinear relationship between neuronal inflammation beyond 96 h in ICH. 7 The current study was unable to reproduce the findings related to morbidity and mortality seen previously in ICH because the present cohort had incompletely reported long-term outcomes and was underpowered to investigate this question.
Limitations in our study include a small sample size with a total of 166 participants. Subjects were excluded from our sample if demographic or clinical variables were missing, allowing for potential bias. As mentioned in the methods, Hp phenotyping was not uniformly available at all sites throughout the entire study period, therefore excluding otherwise potentially eligible ICH patients; another source of potential bias. Our sample was selected from geographically separate sites and enrolled over the span of several years. This effect is likely limited however, given that many of the statistically different baseline demographic and clinical characteristics between enrollment cohorts were more evenly distributed by haptoglobin phenotype groupings. The CTs acquired were obtained at the discretion of the clinical team at each institution of enrollment. This fact led to significant variation in the time intervals that CT scans were obtained. Therefore, the possibility of undetected bias, such as disease classification bias and disease severity bias, is distinctly possible. Additionally, our analysis attempts to control for some of these effects by standardizing ICH change and early perihematomal edema effect by time, however, this assumes the change in ICH volume and edema are linear. However, there is growing evidence to suggest that the rate of change in perihematomal edema formation in ICH may not be most accurately represented via linear models during the first three days post ictus. 32 The Hp 1-1 phenotype represents < 10% (n = 15) of our study population offering the possibility of type 1 error, however this reflects the general proportion of the Hp1-1 genotypes within the US population. 18 Lastly, in our analysis we could not account for all differences in medical intervention. We did however only include patients who were managed medically (no surgical interventions) and controlled for common risk factors associated with ICH and perihematomal edema formation (age, race, blood pressure). 33 An additionally important limitation is antiplatelet and non-coumadin anticoagulation reversal between sites (as coumadin at time of enrollment was an exclusion criteria). This could potentially influence hematoma expansion; however, our analysis attempted to control for hematoma expansion by controlling for hematoma growth overtime. Lastly, all the factors controlling brain edema are not known and long-term clinical outcomes in sICH are influenced by events beyond 96 h.
This is the first study of sICH patients to demonstrate a plausible genetic factor affecting the early formation of perihematomal edema. Our present evidence suggests significant differences and heterogeneity in ePHE formation in sICH. A genetic basis in edema formation may explain a portion of the heterogeneity of edema formation and ultimately patient outcomes in ICH patients and trials. While we submit this present evidence cautiously, the authors believe the findings provide justification for a well-designed, prospective observational study. Required to validate the current study's findings, standardized imaging and medical management protocols as well as standard outcome measures, including 90-day mortality and mRS measurements must be required in future study designs.
Our study suggests that haptoglobin phenotype influences the rate of early PHE formation. Biological pathways identified by genetic associations affecting edema formation offer insight to potential pharmacologically remediable biological pathways that could reduce the rates of early edema formation in sICH and improve clinical outcomes. These data are only preliminary, and a larger well-designed prospective observation study is required to better assess the effects of haptoglobin phenotypes on clinical outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
Dr Hanley reports grants from NIH and personal fees from BrainScope, Neurotrope, Op2Lysis, Portola Pharmaceuticals, and medicolegal, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Michael R Halstead is supported in part by the American Academy of Neurology Medical Education Research Fellowship.
Dr Hanley is supported by the National Institutes of Health (U01NS080824 and U24TR001609).