
Abstract
Background
The optimal blood pressure lowering target in the acute phase of severe stroke is uncertain. Our aim was to compare the efficacy and safety of individualized blood pressure lowering with standard blood pressure lowering in severe stroke.
Methods
Five-hundred consecutive patients with acute severe stroke and elevated BP were recruited from 26 Chinese hospitals. Eligible patients were randomized into an individualized blood pressure lowering group (with 10–15% reduction in systolic blood pressure from admission level or standard blood pressure lowering group (with a target SBP of <200 mm Hg in acute ischemic stroke and <180 mm Hg in intracerebral hemorrhage). The primary outcome was the proportion of patients with a poor functional outcome at day 90 of enrolment.
Results
Of 483 participants included in the analysis, 242 received individualized blood pressure lowering treatment and 241 received standard treatment. The primary outcome event was observed in 71.1% of the participants in the individualized treatment group and in 73.4% of the standard treatment group (odds ratio with individualized treatment for primary outcome, 0.75; 95% confidence interval, 0.47 to 1.19; p = 0.222). The rates of serious adverse events in the two groups were similar (27.7% vs. 28.2%).
Conclusions
In patients with acute severe stoke, individualized blood pressure lowering treatment did not significantly reduce the rate of three-month death or dependence.
Trial registration
Clinicaltrials.gov, NCT02982655. Registered in 5 December 2016, https://clinicaltrials.gov/ct2/show/NCT02982655
Keywords
Background
Many randomized controlled trials (RCTs) have sought to determine the best strategy for blood pressure (BP) management, but the results remain conflicting and have not provided conclusive evidence for optimal target values in patients with acute stroke.1–5 Moreover, these studies have involved only a few critically ill patients with really severe ischemic or hemorrhage stroke. Above all, those patients with severe stroke often have a higher mortality and disability rate and are particularly susceptible to insufficient cerebral perfusion and most dependent on optimal BP control.6–8 Given the more severe brain edema and dysfunction of cerebral autoregulation in severe stroke, the management of BP is apparently more challenging.
We designed the Controlling Hypertension After Severe Cerebrovascular Event (CHASE) trial to determine the efficacy and safety of a moderate and individualized BP-lowering strategy (10–15% reduction from admission level) in both severe ischemic and hemorrhagic stroke.
Methods
Trial design and patients
The CHASE trial was a prospective, randomized, multicenter, controlled study including patients with acute severe stroke who were treated with an individualized BP-lowering strategy or a standard BP-lowering strategy. This trial was conducted between 1 January 2017 and 31 August 2018, in 26 hospitals in the northwest of China. Details of the protocol have been published 9 and are provided in the supplementary material.
We recruited patients with acute stroke who presented within 72 h after symptom onset, were aged 18 or older, had a Glasgow Coma Scale (GCS) score of ≤12 or a National Institutes of Health Stroke Scale (NIHSS) score of ≥11, and had a systolic BP (SBP) between 150 and 210 mm Hg. Patients were excluded if they received or planned to receive intravenous thrombolysis, mechanical thrombectomy, or decompressive craniectomy for the current stroke; if they presented with subarachnoid hemorrhage; if the current stroke was secondary to a structural abnormality in the brain; if they had a definite contraindication to antihypertensive treatment; and if they had unstable vital signs, existing dementia, pre-stroke disability, or any medical illness that would interfere with the outcome assessments.
As soon as written informed consent was provided from each patient or appropriate surrogate based on national regulations, investigators acquired the result of the allocation from a secure randomization website. Patients were randomized into either an individualized BP-lowering group or standard BP-lowering group (1:1). The participants were blind to the randomization results, whereas the investigators were informed in order to follow a prespecified strategy of BP lowering.
Trial oversight
The study protocol was approved by the ethics committee at each participating site. The trial was registered with ClinicalTrials.gov (NCT02982655). The Quality Control and Assurance Committee adjudicated and verified the case eligibility, protocol adherence, and adverse events. This study received no commercial support. All study investigators were asked to protect personal identity and medical information. Only deidentified data were submitted to the Statistical Analysis Center. The investigators and statisticians vouch for the completeness and accuracy of the data and the fidelity of the trial to the protocol.
Trial interventions
In patients who are assigned to receive individualized antihypertensive treatment (individualized BP-lowering group), the goal was to reduce SBP by 10% to 15% (in a range of 130–180 mm Hg) from the admission level within 2 h after randomization and maintain this level for one week. For participants who were assigned to receive standard BP-lowering treatment, antihypertensive agents were administered when the SBP was >200 mm Hg in acute ischemic stroke (AIS) or the SBP was >180 mm Hg in intracerebral hemorrhage (ICH), and the goal was to maintain the SBP ≤200 mm Hg in AIS and ≤180 mm Hg in ICH for one week. The selection of antihypertensive agents was based on the local availability, and no specific agent was stipulated. Both intravenous and oral agents were used according to needs to achieve different treatment goals.
Trial assessment
At the time of enrolment, demographics, subtypes of stroke, medical histories, and clinical characteristics were recorded. BP was monitored in the nonparetic arm using automatic BP cuffs and was recorded every 2 h during the first 24 h after randomization, every 4 h during day 2 and day 3, every 8 h during day 4 to 7, and at 8 a.m. on the day of discharge. Outcomes at hospital discharge were evaluated using the GCS, NIHSS, Barthel Index (BI), and modified Rankin Scale (mRS). GCS scores range from 3 to 15, with lower scores indicating worse levels of consciousness. NIHSS scores range from 0 to 42, with higher scores indicating a more serious neurologic deficit. BI scores range from 0 to 100, with lower scores indicating lower abilities in activities of daily living. The mRS scores range from 0 to 6, with higher scores indicating higher degrees of disabilities or dependence. Participants were followed up and assessed by telephone at 90 days with the use of BI and mRS. All clinical scores were assessed by qualified investigators who were blinded to the treatment assignments. Adverse events, particularly serious adverse events (SAEs), were monitored and recorded to assess treatment safety.
Outcome measures
The primary outcome measurement was the proportion of patients with a poor outcome at day 90 of enrolment. Poor outcome was defined as dependence (unable to live independently, 3 to 5 on mRS) or all-cause death (6 on mRS). The key secondary outcome was the proportion of participants with a poor outcome (mRS ≥ 3) at hospital discharge. Other secondary outcomes were neurological deficits at hospital discharge (assessed by NIHSS), levels of consciousness at hospital discharge (assessed by GCS), abilities of activities of daily living at hospital discharge and at day 90 of enrolment (assessed by BI), and SAEs.
Statistical analysis
The sample size was set at 500 so that the study would have at least 80% power to detect a 15% relative risk reduction (12% absolute risk reduction) in the primary outcome, from 75% in the standard group to 63% in the individualized BP-lowering group, assuming an overall rate of nonadherence to treatment and loss to follow-up of 8%, with a type I error rate of 5%. The data were analyzed according to the intention-to-treat principle, with the use of SPSS version 22 software (SPSS Inc., Chicago, IL). Two-sided p values ≤ 0.05 were considered significant.
The primary hypothesis was examined first by standard chi-square test. Then we used logistic regression to determine the effect of treatment on the primary outcome and binomial secondary outcomes with adjustment for the effects of age, sex, and GCS score on admission. The effects of treatment on the continuous secondary outcomes were determined by estimating the beta coefficient in the generalized linear model. Subgroup analyses were conducted in patients with different ages (≥65 or < 65 years), different stroke types (ICH or AIS), different SBP levels on admission (<180 or ≥180 mm Hg), with or without history of hypertension, different severity levels on admission (GCS < 8 or ≥8), and different durations from onset to randomization. Adverse events and SAEs were recorded using the terms preferred by the Medical Dictionary for Regulatory Activities.
Results
Study population
From 1 January 2017 through 31 August 2018, a total of 16,029 patients with AIS or ICH were screened in 26 tertiary hospitals in the northwest of China, of whom 500 patients underwent randomization; 250 participants were assigned to receive individualized treatment to lower their BP, and 250 were assigned to receive standard treatment. After exclusion of 17 subjects who withdrew consent or were ineligible as adjudicated by quality control, 242 patients in the individualized BP-lowering group and 241 in the standard BP-lowering group were included in the final analysis (Supplementary Figure S1).
Baseline characteristics of the participants, according to treatment group
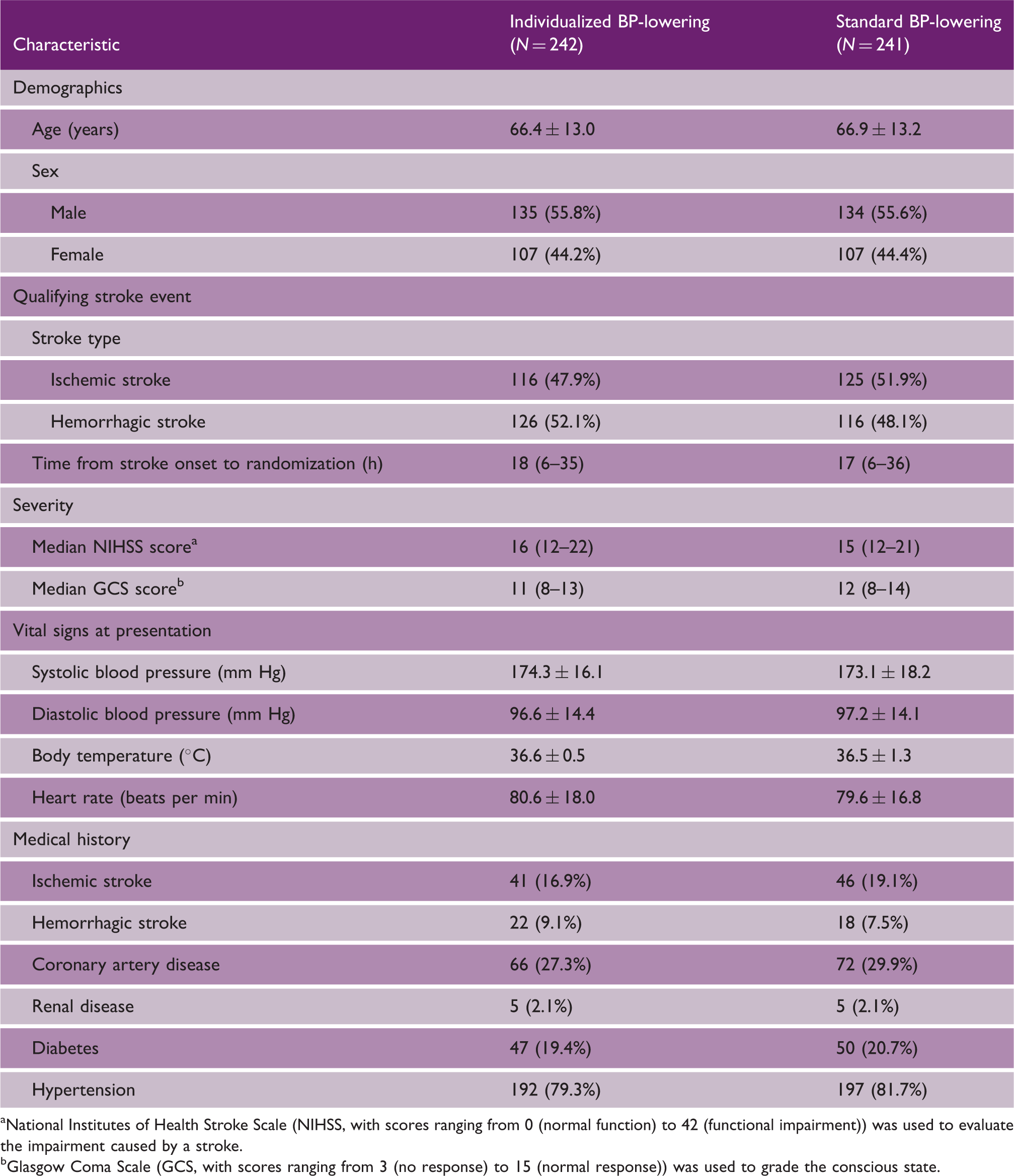
National Institutes of Health Stroke Scale (NIHSS, with scores ranging from 0 (normal function) to 42 (functional impairment)) was used to evaluate the impairment caused by a stroke.
Glasgow Coma Scale (GCS, with scores ranging from 3 (no response) to 15 (normal response)) was used to grade the conscious state.
Intervention
The median time from the stroke onset to the randomization was 18 h in the individualized treatment group and 17 h in the standard treatment group. As shown in Supplementary Table S1, more patients in the individualized treatment group than in the standard treatment group received antihypertensive agents (all: 85.1% vs. 58.1%, p < 0.001; intravenous: 47.9% vs. 22.0%, p < 0.001). Other aspects of background care during the first seven days after enrolment were similar in the two groups.
The mean values of SBP during the first 24 h and seven days after randomization are presented in Figure 1(a), the curve chart of diastolic BP is provided in Supplementary Figure S2. At the first 2 h, the mean SBP was 151.6 mm Hg (12.9% reduced from baseline) in the individualized treatment group as compared with 160.7 mm Hg (6.3% reduced from baseline) in the standard treatment group (a difference of 6.6%, p < 0.001).
Mean systolic blood pressure during the first seven days after randomization. The dashed vertical line indicates 2 h, and I bars 95% CIs. (a) Total, at the first 2 h the mean SBP was 151.6 mm Hg (12.9% reduced from baseline) in the individualized treatment group as compared with 160.7 mm Hg (6.3% reduced from baseline) in the standard treatment group (a difference of 6.6%, p < 0.001); (b) ischemic stroke, at the first 2 h the mean SBP was 150.8 mm Hg (11.5% reduced from baseline) in the individualized treatment group as compared with 161.9 mm Hg (4.8% reduced from baseline) in the standard treatment group (a difference of 6.7%, p < 0.001); (c) intracerebral hemorrhage, at the first 2 h, the mean SBP was 152.2 mm Hg (13.9% reduced from baseline) in the individualized treatment group as compared with 159.2 mm Hg (8.2% reduced from baseline) in the standard treatment group (a difference of 5.7%, p < 0.001).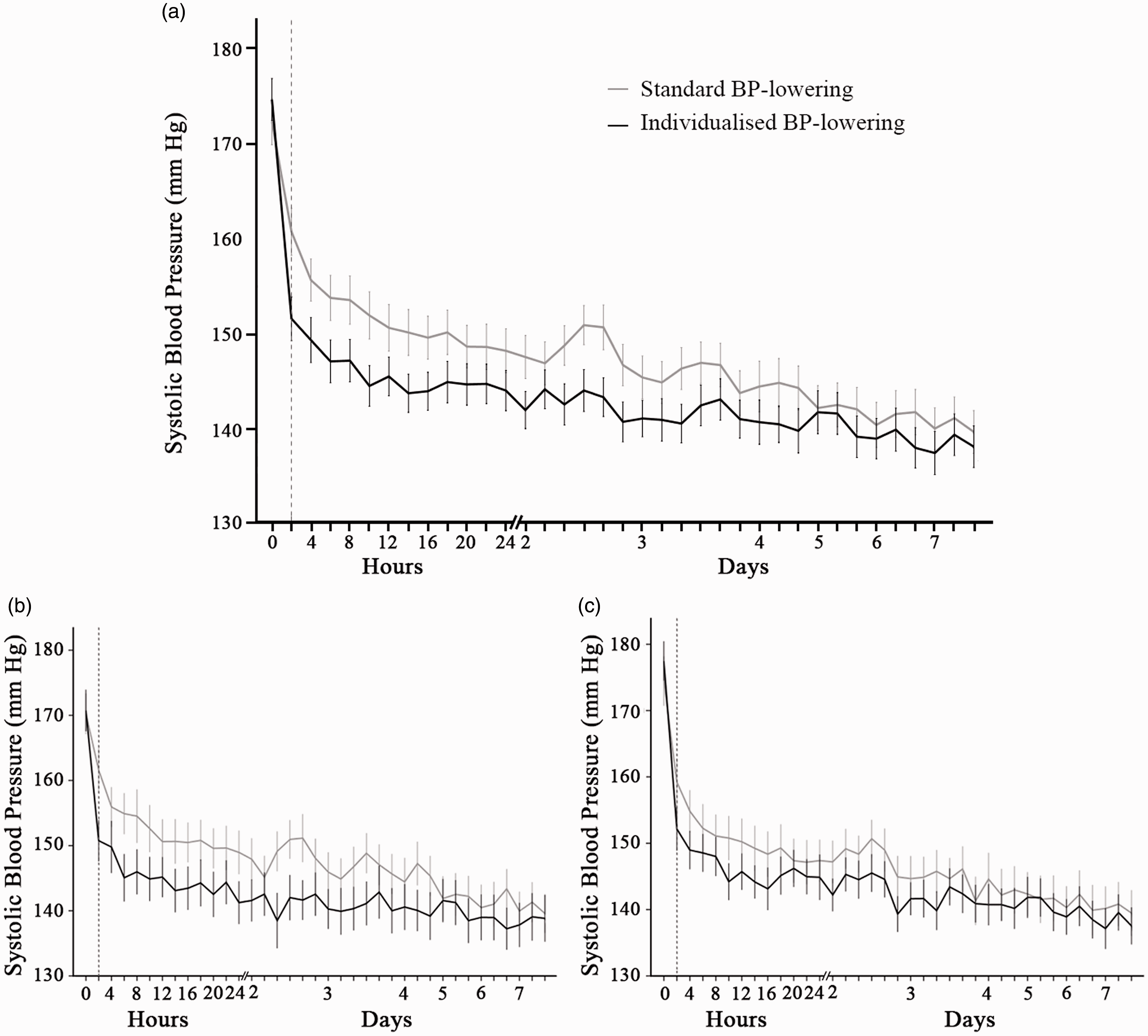
In the first 24 h, the mean SBP was 144.0 mm Hg (17.0% reduced from baseline) in the individualized treatment group and 148.2 mm Hg (13.3% reduced from baseline) in the standard treatment group. At day 7, the mean SBP was 138.1 mm Hg (20.5% reduced from baseline) in the individualized treatment group and 139.7 mm Hg (18.1% reduced from baseline) in the standard treatment group. From the second day to the seventh day after randomization, mean levels of SBP in both the individualized treatment group and standard treatment group continued to decline slightly in general and fluctuated during each day, with peaks in the daytime.
Clinical outcomes
The results of the primary and secondary outcomes were complete in all the 483 participants included. At 90 days, 172 of the participants (71.1%) in the individualized treatment group had a poor outcome as compared with 177 (73.4%) in the standard treatment group. The individualized BP-lowering treatment had an odds ratio (OR) of 0.89 (95% confidence interval (CI), 0.47 to 1.19; p = 0.222) for a 90-day poor outcome with an adjustment for age, sex, and baseline GCS as compared with standard BP-lowering treatment (Table 2). The ordinal distributions of the mRS score were similar in the two groups (Figure 2 and Supplementary Table S2), and no significant shift was found in the mRS score between two groups (OR −0.072, 95%CI −0.39 to 0.25, p = 0.610; Cochran–Mantel–Haenszel shift test
10
).
Distribution of scores on the Modified Rankin Scale, according to treatment group. The percentage of participants with each score on the modified Rankin scale is shown in or above each cell. Scores range from 0 to 6, with 0 indicating no symptoms, 1: no clinically significant disability, 2: slight disability, 3: moderate disability, 4: moderately severe disability, 5: severe disability, and 6: death. Primary, secondary, and safety outcomes, according to treatment group The analysis was adjusted for age, sex, and baseline Glasgow Coma Scale (GCS) score. The modified Rankin scale (with scores ranging from 0 (no symptoms) to 6 (death)) was used to grade the degree of disability. The poor outcome was defined as a score of 3 to 6. Barthel index (with scores ranging from 0 (dependent) to 100 (independent)) was used to grade the degree of dependence in the daily activities. Since the Barthel index, NIHSS, and GCS scores are continuous variables, beta was the regression coefficient for the treatment effect (standard BP-lowering group divided by individualized BP-lowering group) in the generalized linear model. A beta of 0 indicates no effect of the treatment on the outcome.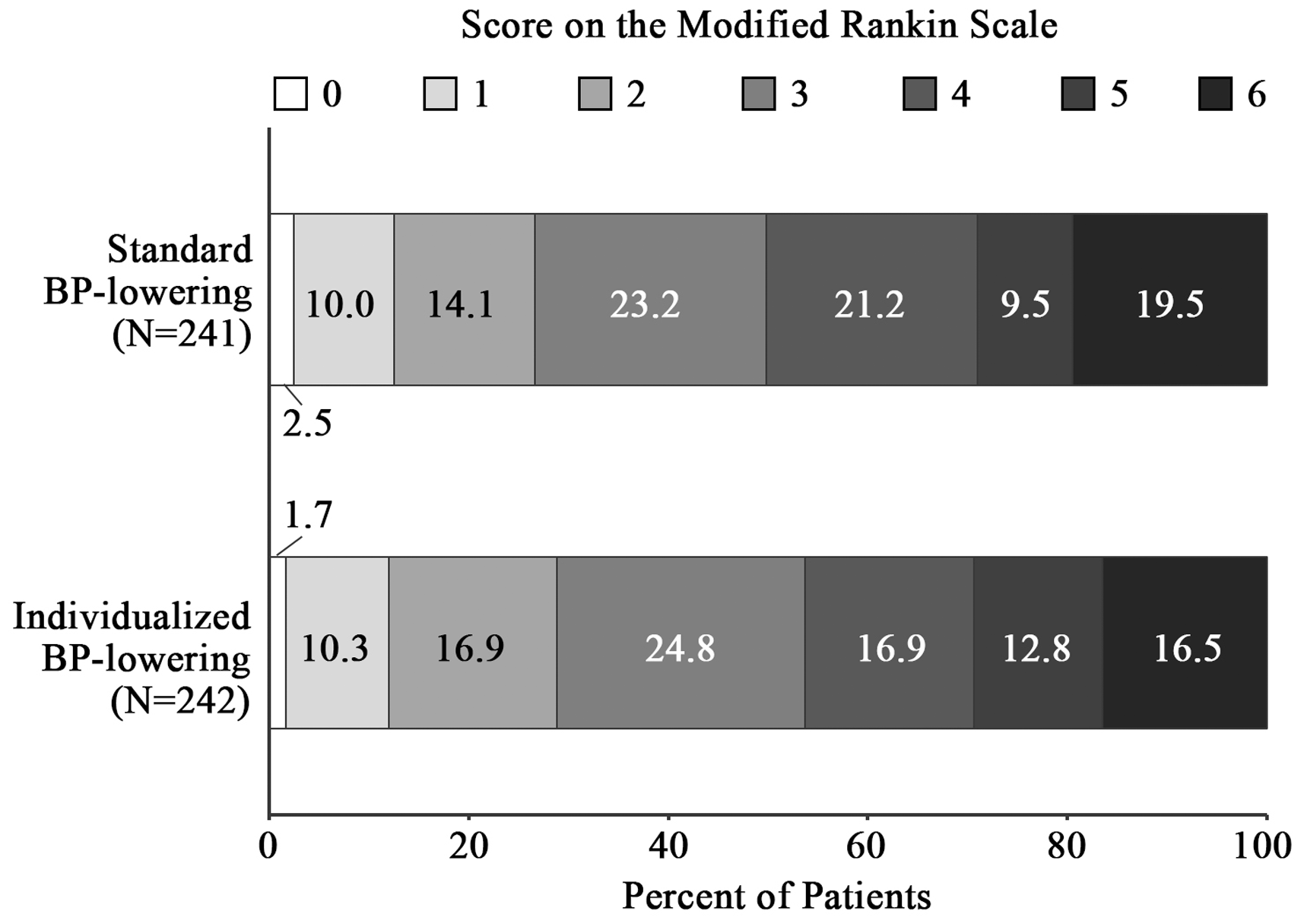
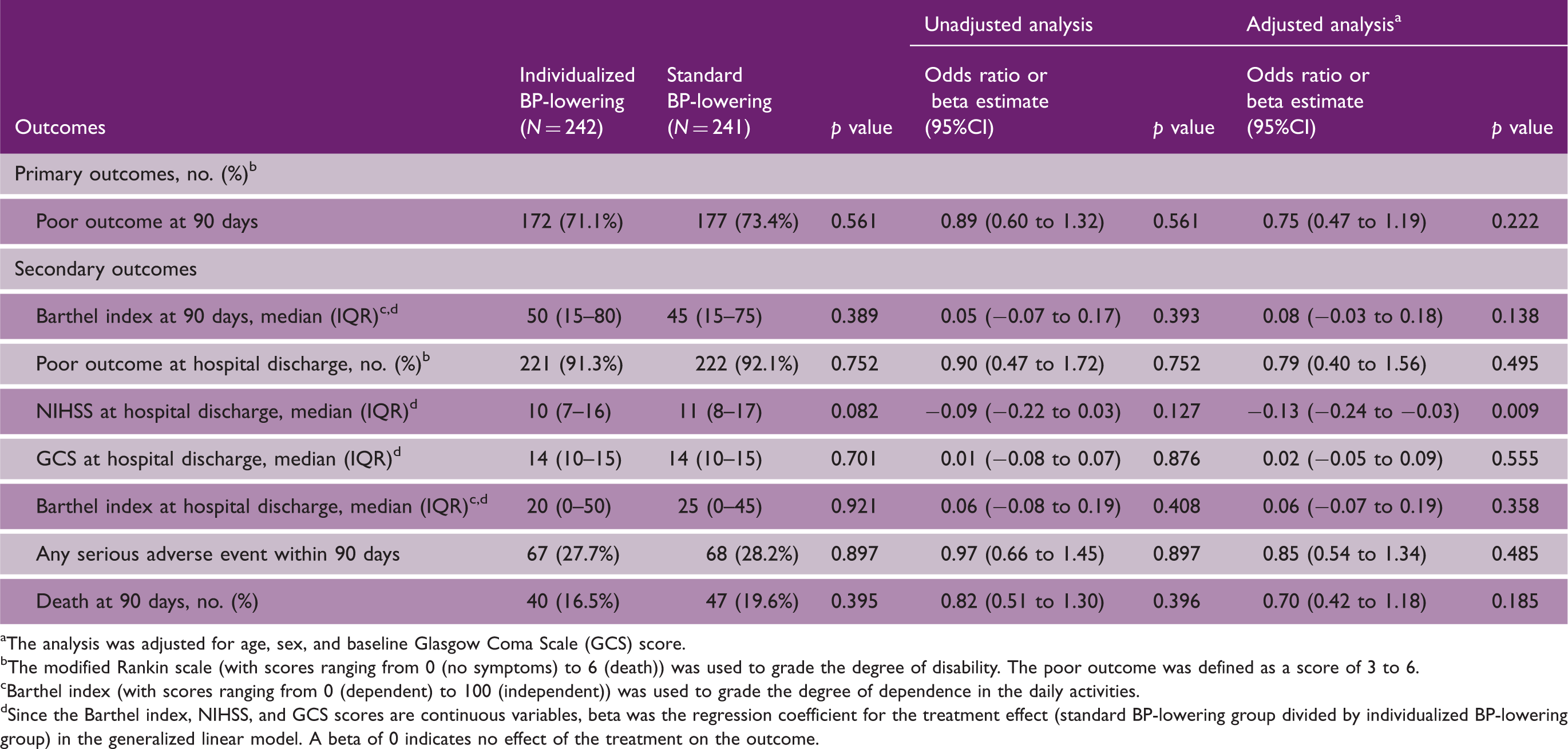
There were no significant between-group differences in GCS, BI, or poor outcome at hospital discharge nor in BI at 90 days. The generalized linear analysis showed that the individualized BP-lowering treatment had a significant effect on reducing the neurological deficits at hospital discharge as evaluated by NIHSS (beta estimate, −0.13; 95%CI −0.2 to −0.03; p = 0.009) as compared with standard BP-lowering treatment with an adjustment for age, sex, and baseline GCS. The reduction in NIHSS from baseline to hospital discharge was significantly greater in the individualized treatment group than in the standard treatment group (p = 0.013; Supplementary Table S3).
Supplementary Tables S4 and S5 listed adverse events and SAEs, respectively. The rates of any SAE within 90 days and 90-day mortality were similar between the two groups. Consistent with the results in all total participants, no heterogeneity was found across predefined subgroups (Supplementary Figures S3 to S5). The SBP data in patients with AIS and patients with ICH were presented in Figure 1(b) and (c).
Discussion
In this prospective, randomized study, individualized compared with standard BP-lowering treatment was not associated with a substantial reduction in three-month dependency in patients with acute devastating stroke, but individualized BP-lowering treatment alleviated neurological deficits at hospital discharge compared with conventional treatment. Meanwhile, it was shown that there was no evidence of increased SAEs or neurological deterioration between two groups. The finding that moderate antihypertensive treatment after acute severe AIS or ICH shows no evidence of harm and a potential benefit of neuro-recovery.
Two meta-analyses including RCTs in which lowering of BP was started versus placebo of AIS or hemorrhagic stroke concluded that there is insufficient evidence that lowering BP during the acute phase of stroke improves functional outcome.11,12 Moreover, patients requiring critical care were underrepresented in most trials. Until now, the clinical evidence of early BP control for patients with severe stroke has been very limited. The CHASE study attempted to look for answers to the following three problems: (1) is BP lowering needed in the acute phase of severe stroke? (2) how is the appropriate BP-lowering range determined for acute severe stroke? (3) is there a reasonable therapeutic time window for raised BP after stroke onset?
Higher levels of SBP were indicated to be positively associated with poor stroke outcome, 13 but aggressive BP control during acute stroke might reduce cerebral blood flow and worsen the outcome because of the impairment in cerebral autoregulation.14,15 Although many efforts have been made to explore the benefits of BP lowering for patients with acute stroke, no consensus has been reached so far. For patients with AIS, the results of the angiotensin-receptor blocker candesartan for treatment of acute stroke (SCAST) study 16 indicated that careful BP-lowering treatment with candesartan is not beneficial and even has a harmful effect on patients with acute stroke and raised BP. The effects of antihypertensive treatment after acute stroke in the Continue or Stop Post-Stroke Antihypertensives Collaborative Study 2 were neutral compared with antihypertensive treatment with placebo. As for patients with ICH, the Intensive blood pressure Reduction in Acute Cerebral hemorrhage Trial-2 study showed that intensive BP lowering improved three-month functional outcome; 4 however, the antihypertensive treatment of Acute cerebral hemorrhage II (ATACH-2) study later found that intensive BP lowering significantly raised the rate of renal adverse events and did not reduce mortality or morbidity compared with standard treatment. 5 One of the important reasons for those controversial results might be due to a single-target antihypertensive intervention instead of an individualized BP-lowering treatment in the above studies.
Results of a subgroup analysis indicated that patients with a large decrease (≥28 mm Hg) in SBP had a significantly increased risk of early adverse events relative to patients with a small decrease. 17 In addition, post hoc analysis of the China antihypertensive trial in acute ischemic stroke (CATIS) study investigated the effect of early BP lowering in AIS patients with different severities, and no beneficial effect of early BP reduction was found in patients with severe AIS. 18 However, the wide range for BP reduction (10% to 25%) proposed by CATIS increased the complexity and uncertainty in interpreting their results. While there is no established definition of “nonaggressive” BP reduction, a BP reduction of 25% seems to be too aggressive for patients with severe stroke, especially those with cerebral hypoperfusion. In our study on acute severe stroke, we proposed a moderate individualized BP-lowering strategy (10–15% reduction in SBP from admission level).
Overall, the RCTs focusing on ICH included patients within 24 h or less after stroke onset,4,19–21 and additional studies focusing on AIS or different types of stroke enrolled patients with a longer term from the stroke onset to the randomization. The Acute Candesartan Cilexetil Therapy in Stroke Survivors 1 and a subgroup analysis of the Prevention Regimen for Effectively Avoiding Second Strokes trials 22 included patients within 72 h after AIS onset. The Controlling Hypertension and Hypotension Immediately Post Stroke (CHHIPS) trial included patients within 36 h after acute hemorrhagic or ischemic stroke onset. 23 The median time from the stroke onset to the randomization was similar in the CHASE study (18 h) and some previous of RCTs for AIS (15–20 h).3,24,25 Based on pragmatic considerations, we chose the cut off of 72 h for BP-lowering management in the early time period after stroke onset.
To the best of our knowledge, this is the first prospective, randomized study of acute hypertension control after severe stroke. The CHHIPS trial, 23 the SCAST trial 16 and the Efficacy of Nitric Oxide in Stroke (ENOS) trial 26 included both AIS patients and ICH patients and investigated the effect of a moderate BP-lowering treatment. The CHHIPS trial concluded that the moderate BP-lowering treatment was safe and halved the three-month mortality compared with the control group, whereas the SCAST trial and ENOS trial found no indication that the moderate BP-lowering treatment was beneficial in patients with acute stroke and elevated BP. Most or even all of the patients included in the above trials had no impairment of consciousness, and the median baseline NIHSS in these trials was 9 to 11. Therefore, for patients with severe stroke, the above findings need to be re-examined and validated. Considering that it is similar in pathomechanisms and clinical consequences after acute cerebral injury induced by severe ischemic and hemorrhagic stroke, our study also included both AIS and ICH patients with elevated BP and investigated the effect of moderate individualized BP lowering (10% to 15% reduction from baseline) on three-month outcome.
Limitations
The strengths of this trial include the secure online central randomization, strict quality control, and high rates of adherence to treatment and follow-up. Some limitations of this study should also be noted. First, the sample size of this study might be under-powered for treatment effects overall and between ischemic and hemorrhagic stroke. Second, we used a range of available antihypertensive agents that may have different effects on BP and outcomes, but this was consistent with what we do in real-world medical care. Third, for some patients with mildly elevated SBP in the individualized treatment group, oral antihypertensive agents rather than intravenous agents were used to manage BP, and oral agents were not as easy to titrate as intravenous agents. However, in everyday medical care, clinicians also prefer oral antihypertensive agents over intravenous agents for patients with mildly elevated high SBP, such as 150–160 mm Hg. Fourth, we excluded patients who received thrombolysis or endovascular treatment which were main therapies for acute stroke. However, these therapies have limited therapeutic time window and strict criteria, less than 30% of AIS patient were eligible for thrombolysis 27 and only 2.7% of AIS patients met the criteria of thrombectomy. 28 Therefore, the findings of this study can be generalized to major population of severe stroke. In addition, the time from onset to enrolment was longer in some patients with acute AIS than what was reported in some other recent stroke studies, because AIS patients with a short time to onset usually choose endovascular treatments, and they were excluded from this trial. Fifth, although several secondary outcomes were assessed at hospital discharge, and discharge assessment made communication easier with patients and families, the results of these assessments may be biased by more factors than those performed on a specific day after onset. Sixth, early SBP is also important for secondary prevention in stroke, but we failed to include it in the outcome assessments. We will continue the follow-up and investigate the effect of early BP management on the secondary prevention in the further study. Moreover, the limited statistical power, the lack of imaging data, and the lack of measurements of cerebral blood flow autoregulation were also limitations in this study.
Conclusions
Individualized lowering of BP in patients with acute severe stroke was safe but did not result in a significantly lower rate of poor outcome at three months as compared with standard treatment. A positive effect of individualized BP lowering on the recovery of neurological deficit at hospital discharge was observed; however, this still needs to be further validated.
Supplemental Material
sj-pdf-1-wso-10.1177_1747493020932784 - Supplemental material for Controlling Hypertension After Severe Cerebrovascular Event (CHASE): A randomized, multicenter, controlled study
Supplemental material, sj-pdf-1-wso-10.1177_1747493020932784 for Controlling Hypertension After Severe Cerebrovascular Event (CHASE): A randomized, multicenter, controlled study by Fang Yuan, Fang Yang, Jingjing Zhao, Feng Fu, Yi Liu, Changhu Xue, Kangjun Wang, Xiangjun Yuan, Dingan Li, Qiuwu Liu, Wei Zhang, Yi Jia, Jianbo He, Jun Zhou, Xiaocheng Wang, Hua Lv, Kang Huo, Zhuanhui Li, Bei Zhang, Chengkai Wang, Li Li, Hongzeng Li and Wen Jiang in International Journal of Stroke
Footnotes
Authors' contributions
WJ was principal investigator, developed the trial, sought and obtained funding, and was responsible for the overall running, analysis, and writing of the manuscript. F Yuan and F Yang were trial managers, contributed to data collection and interpretation, and wrote the first draft of the manuscript. JZ contributed to the trial design, analyzed the data and reviewed the manuscript. FF, YL, CX, KW, XY, DL, QL, WZ, YJ, JH, JZ, XW, HL, KH, ZL, BZ, CW, LL and HL were regional coordinating investigators who contributed to the trial design, recruited patients, and critically revised the manuscript. All authors took responsibility for the final manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this published article. The detailed datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Consent for publication
Applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CHASE trial is funded by the Shaanxi Province Key Research and Development Projects (2013KTZB03-02-02 and 2017ZDCXL-SF-02-02).
Ethics approval
The study protocol was approved by the ethics committee at each participating site. Written informed consent was obtained directly from the patient or an appropriate surrogate, based on local ethics committee recommendations.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.