
Abstract
Rationale
People with stroke experience falls at more than twice the rate of the general older population resulting in high fall-related injuries. However, there are currently no effective interventions that prevent falls after stroke.
Aims
To determine the effect and cost-benefit of an innovative, home-based, tailored intervention to reduce falls after stroke.
Sample size estimate
A total of 370 participants will be recruited in order to be able to detect a clinically important between-group difference of a 30% lower rate of falls with 80% power at a two-tailed significance level of 0.05.
Methods and design
Falls after stroke trial (FAST) is a multistate, Phase III randomized trial with concealed allocation, blinded assessment, and intention-to-treat analysis. Ambulatory stroke survivors within five years of stroke who have been discharged from formal rehabilitation to the community and who have no significant language impairment will be randomly allocated to receive habit-forming exercise, home safety, and community mobility training or usual care.
Study outcomes
The primary outcome is the rate of falls over the previous 12 months. Secondary outcomes are the risk of falling (proportion of fallers), community participation, self-efficacy, balance, mobility, physical activity, depression, and health-related quality of life. Health care utilization will be collected retrospectively at baseline and prospectively to 6 and 12 months.
Discussion
The results of FAST are anticipated to directly influence intervention for stroke survivors in the community.
Introduction and rationale
Compared to the general population, people with stoke experience falls at more than twice the rate of the general older population (73% compared with 30%), 1 resulting in high numbers of fall-related injuries. 2 At this rate, of the 475,000 Australians living with the effects of stroke in 2017, 3 over 340,000 can be expected to experience a fall. Stroke survivors are also likely to be repeat fallers and the consequences of falls severely jeopardize their long-term health and well-being. 4 For example, falls can result in hip fracture, leading to a downward spiral of immobility, reduced confidence and incapacity leading to institutionalization. Falls are the main cause of hospitalization from injury after stroke. 1 Fall and fall injury after stroke also places a substantial strain on the disability and aged health care systems.
Despite the prevalence of stroke, high rate of falls after stroke, and over three decades of research in falls prevention in the general population, relatively few randomized trials have tested falls interventions for stroke survivors. A systematic review of falls risk factors for stroke 4 concluded that prevention should be multidimensional and a systematic review of falls risk factors for the general population recommended tailored interventions for higher risk groups. 5 The two randomized trials that have investigated falls after stroke6,7 were not effective and involved exercise that was segregated from daily routines. Consequently, there are currently no effective interventions that prevent falls after stroke. 8
The aim of this Phase III randomized trial, therefore, is to determine both the clinical effect and the cost-benefit of an innovative intervention to reduce falls. The intervention combines exercise, community mobility, and home safety training, but most significant is that the exercise is habit forming because it is integrated into daily routines.
9
Specific research questions are:
effective in reducing both the rate of falls and the proportion of people falling over a one-year period, effective in improving community participation, self-efficacy, balance, mobility, physical activity, depression, and health-related quality of life, and cost-effective?
Methods
Design
The “
Patients and therapists
People with stroke will be screened and invited to participate if they are 50 years and over, within 5 years of their first stroke; have been discharged from formal rehabilitation and are community-dwelling; are able to walk 10 m across flat ground with or without an aid; and are capable of providing consent (defined as <5 errors on the Short Portable Mental Status Questionnaire). They will be excluded if they have moderate to severe receptive aphasia (defined as a score of <7/10 on the comprehension component of the Frenchay Screening Aphasia Test 10 ).
Therapists will be eligible to deliver the intervention if they are physical or occupational therapists registered with the Australian Health Practitioner Regulation Agency.
Randomization
Walking speed measured with usual walking aids will be used to stratify the allocation of participants to groups because it has been found to be associated with community ambulation. 11 Within each of three strata (<0.4, 0.4–0.8, >0.8 m/s), participants will be allocated randomly to either the experimental or control group. Randomization will be conducted after the baseline measurement and the schedule concealed from the recruiter by using an offsite, independent and automated service.
Intervention
The experimental group will receive a home-based intervention consisting of habit-forming exercise, home safety, and community mobility training, tailored to their level of disability. The faster walkers (>0.8 m/s) will have most emphasis on habit-forming exercise, the slower walkers (<0.4 m/s) will have most emphasis on home safety training, while the middle group (0.4–0.8 m/s) will have a combination of both habit-forming exercise and safety training. All groups will receive community mobility training. Habit-forming exercise will utilize the successful Lifestyle integrated Functional Exercise (LiFE) program which has been shown to be beneficial for older people with a history of two or more falls or an injurious fall.
12
Activities which challenge balance and strength will be incorporated into specific daily tasks. They will be performed intentionally and consciously until they become automatically triggered (i.e., habitual) and embedded in daily activities. Feedback, monitoring, and positive reinforcement will be used to enhance performance of these activities and self-efficacy of the participants. Rather than a prescribed set of exercises conducted several times a week, activities will occur whenever the opportunity arises during the day. An activity challenging balance by reducing base of support might involve a tandem stand while working at the kitchen bench, and over time could be progressed to standing on one leg. An activity increasing strength by bending the knees might involve squatting instead of bending at the waist to close a drawer, and over time could be progressed to squatting to close a lower drawer.
Design of the trial.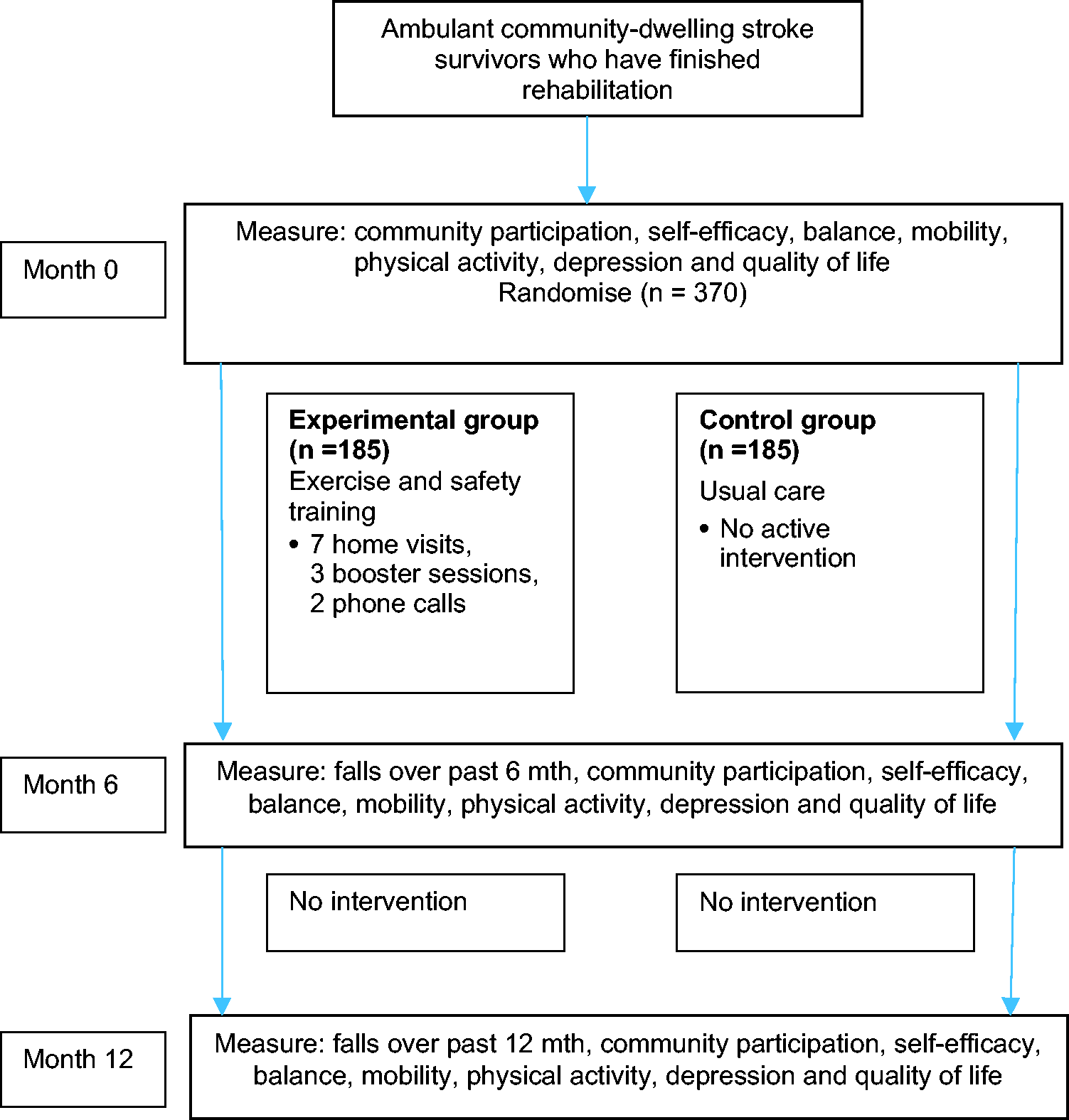
The home safety intervention will focus on environmental adaptations to reduce fall hazards and protective behaviors to reduce risk. The Westmead Home Safety Assessment 13 and the Falls Behavioural Scale for Older People 14 will be used to identify environmental fall hazards and risks, taking into account their level of disability. The intervention will incorporate strategies for enhancing self-efficacy, cueing and monitoring to boost adherence, and engagement of the participant in planning, decision making, and follow through of solutions. Participants will have access of up to $200 to cover costs of simple home adaptations, such as non-slip strips, double-sided tape to secure carpets, LED sensor globes to improve night lighting, in addition to referral to usual home modification services in the community. Participants will be encouraged to safely practice activities in the home and community within their current capabilities.
The community mobility intervention will focus on mobilizing outside the home in the garden or to the letterbox, outings to shops and in local community, to neighbors, with friends, at family places, or to travel further afield for shopping or medical appointments. A community mobility goal will be individualized and jointly devised with a family member where appropriate. Goals may include being a passenger in a car, using public transport, or walking around a crowded shopping center. Where relevant a session will include supported mastery to boost confidence and skill. The mobility community goal and home safety recommendations will be reviewed during the last home visit and again at 12 months.
The home-based tailored intervention will be delivered during seven home visits over Weeks 1–7 followed by three booster sessions at Weeks 13, 15, and 23 with two phone calls during Weeks 9 and 19. Interventionists will receive training in the implementation of the intervention including therapist and participant manuals. 15 Participants will record practice using weekly logs to monitor adherence to the exercise program and will complete the Exercise Adherence Rating Scale. 16 Adherence to home safety recommendations and community mobility goals will be reviewed at 6 and 12 months. Fidelity checks of both interventionists and measurers will be carried out.
The control group will receive usual care which will equate to no active intervention. This reflects the current situation for community-dwelling stroke survivors discharged from rehabilitation in Australia, where opportunities for rehabilitation largely cease by 6 months.17
Primary outcome
Falls will be recorded prospectively from baseline daily on falls calendars returned via (e)mail monthly. The rate of falls will be reported at 6 months for the previous 6 months and at 12 months for the previous 12 months, calculated from the falls calendars. Falls will be defined according to consensus statements and Cochrane review recommendations as “an unexpected event in which the participant comes to rest on the ground, floor, or lower level.”
18
Secondary outcomes
Proportion of fallers and information about fall injuries. Community participation measured using the disability component of the Late Life Function and Disability Index
19
and two self-reported questions estimating how much and to what satisfaction the individual participates in life outside the home. Self-efficacy measured using two questions about falling when carrying out usual activities in the home and community rated using a Likert scale of “not at all” to “very concerned.” Balance measured using the balance component of the Short Physical Performance Battery
20
and the Step Test.
21
Mobility measured as preferred and fast walking speed over 5 m
22
and by two self-reported questions estimating maximum distance and duration of walking. Physical activity measured using the Incidental and Planned Exercise Questionnaire
23
and the function component of the Late Life Function and Disability Index.
19
Health-related quality of life measured using the EQ-5D (5L).
24
Depression measured using the Patient Health Questionnaire-2.
25
In order to carry out an economic analysis, information will be collected about health care utilization retrospectively at baseline for the past 12 months and prospectively every 6 months after baseline. Information about regular help with activities of daily living will also be collected using a simple count. In order to identify potential barriers and solutions to widespread implementation of the intervention, a qualitative process evaluation will be undertaken using questionnaires (including the Self-Report Behavioural Automaticity Index
26
to explore habit formation) and interviews of participants and therapists via a semi-structured interview. Verbatim transcripts of interviews will be generated and thematically coded.
Data monitoring body
LC has overall responsibility for the trial and all adverse events will be reported to the relevant ethics committee by CD. Regular fidelity checks of intervention will be undertaken by KS. Data safety and monitoring will be overseen by an experienced researcher (Professor Ian Cameron) independent of the trial. He will receive an interim report on adverse events after every 50 participants and will be responsible for stopping recruitment in the case of multiple serious adverse events.
Sample size estimates
The sample size was calculated for the primary outcome. A negative binomial model for the number of falls is assumed 27 with alpha (measure of over-dispersion in negative binomial regression model) assumed to be 0.8 and rate of falls of the control group assumed to be 1.8 falls/person/year based on Dean et al. 7 Assuming a 15% loss to follow-up, with a two-sided level of significance of 5% and power of 80%, a sample size of 185 per group is required to detect a 30% lower rate of falls in the experimental compared with the control group.
Statistical analyses
Analyses will be conducted on an intention-to-treat basis. The between-group rate of falls will be analyzed using negative binomial regression. 28 The between-group proportion of fallers will be analyzed using logistic regression. Other outcome measures will be analyzed using analysis of covariance (ANCOVA) and presented as mean between-group differences (95% CI).
Study organization and funding
FAST is funded by the National Health and Medical Research Council, Australia. Trial organization, data management, and monitoring is supported by The University of Sydney, Australia.
Discussion
FAST will establish the effectiveness of a home-based, tailored intervention (habit-forming exercise, community mobility and safety training) in reducing falls after stroke, thereby potentially reducing the economic and social burden that results from the consequences of falling. By recruiting community dwelling stroke survivors and testing interventions delivered by allied health professionals in the home and community we will ensure that the intervention will reflect what could be readily achieved in Australia using National Disability and Insurance Scheme and Reablement and Restorative programs.
Summary and conclusions
FAST will test the effect of home-based, tailored intervention to reduce falls. A sample of community-dwelling stroke survivors will be randomly assigned to habit-forming exercise and safety training, or usual care. The primary outcome measure will be falls. The trial has concealed allocation, blinded measurement and an intention-to-treat analysis.
Footnotes
Authors’ contributions
LC, CD, and LA conceived the study. LC, CD, LA, NL, AC, KS, SI, EP, TJ, GH, VM, and BG contributed to the design of the study and procurement of funding. SM and SD have worked on the project to establish procedures and coordinate the trial. CD and LA drafted the manuscript and all authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: FAST is funded by the National Health and Medical Research Council, Australia. Trial organization, data management, and monitoring is supported by The University of Sydney, Australia.