
Abstract
Background:
Major disparities have been reported in recombinant tissue plasminogen activator (rtPA) availability among countries of different socioeconomic status.
Aims:
To characterize variability of rtPA price, its availability, and its association with and impact on each country’s health expenditure (HE) resources.
Methods:
We conducted a global survey to obtain information on rtPA price (50 mg vial, 2020 US Dollars) and availability. Country-specific data, including low, lower middle (LMIC), upper middle (UMIC), and high-income country (HIC) classifications, and gross domestic product (GDP) and HE, both nominally and adjusted for purchasing power parity (PPP), were obtained from World Bank Open Data. To assess the impact of rtPA cost, we computed the rtPA price as percentage of per capita GDP and HE and examined its association with the country income classification.
Results:
rtPA is approved and available in 109 countries. We received surveys from 59 countries: 27 (46%) HIC, 20 (34%) UMIC, and 12 (20%) LMIC. Although HIC have significantly higher per capita GDP and HE compared to UMIC and LMIC (p < 0.0001), the median price of rtPA is non-significantly higher in LMICs (USD 755, interquartile range, IQR (575–1300)) compared to UMICs (USD 544, IQR (400–815)) and HICs (USD 600, IQR (526–1000)). In LMIC, rtPA cost accounts for 217.4% (IQR, 27.1–340.6%) of PPP-adjusted per capita HE, compared to 17.6% (IQR (11.2–28.7%), p < 0.0001) for HICs.
Conclusion:
We documented significant variability in rtPA availability and price among countries. Relative costs are higher in lower income countries, exceeding the available HE. Concerted efforts to improve rtPA affordability in low-income settings are necessary.
Introduction
Recombinant tissue plasminogen activator (rtPA) for acute ischemic stroke treatment was added to the 21st World Health Organization (WHO) Model List of Essential Medicines in 2019, 1 which was 25 years after it was first approved by regulatory bodies and then endorsed by clinical guidelines in the United States, Europe, and elsewhere. At this time, according to marketing information from the drug manufacturer, the treatment has been approved in 109 countries, in the majority for the 0–4.5 h time treatment window.2,3
Despite its established cost-effectiveness,4–7 the proportion of eligible stroke patients receiving rtPA remains suboptimal, and low- and lower-middle-income countries (LMICs) face severe challenges in its implementation.8,9 The population of LMICs is approximately five times the population of high-income countries (HICs) and accounts for a substantial majority of stroke incidence, mortality, and disability. 10 However, a meta-analysis reported that the proportion of rtPA used for eligible patients was substantially lower in low-income countries (LICs) as compared to an increasing treatment rate in LMIC, MIC and the highest in HICs. 11
Disparities in sales prices, insurance coverage, and governmental support across the world have an impact on rtPA availability. In many countries, differences between the public and the private sectors of medical management add to the disparities. This results in major restrictions for eligible patients to treatment access and a considerable impact on stroke disability.
Aims
On behalf of the WSO (World Stroke Organization) Future Leaders program, we conducted a survey to assess the variability in rtPA pricing, availability, and usage in member states of the United Nations. We examined the association between country income gross domestic product (GDP) per capita, health expenditure (HE) per capita and rtPA price, and the affordability of the drug with respect to each country’s HE resources.
Methods
Literature review
We conducted a comprehensive search on PubMed and Web of science using the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines. 12 We included complete articles published in the English language between 1 January 2011 and August 2021.
The search terms were “Stroke” OR “ischemic stroke” OR “cerebrovascular disease” along with Boolean operator AND with one of the following terms: “Thrombolysis,” “rtPA,” “alteplase,” “tenecteplase,” “cost,” “drug cost,” “price” OR “value,” “accessibility” OR “availability.”
We identified 218 articles after duplicate exclusion, of which 17 met the screening inclusion criteria (Supplementary Figure 1). After a full-text review, five articles provided the rtPA sales price, but none in more than one country. Data from these studies are given in Supplementary Table 1.
rtPA pricing and availability survey
A simple questionnaire to collect key information on rtPA pricing, availability, and use was developed through a Google form and was sent to members and membership societies of the WSO (Supplemental Appendix 1).
The following information was obtained: rtPA availability in a country’s stroke treating hospitals, coverage by (public and/or private) insurance, year of approval by the regulatory entities, current official price per 50 mg vial, including value-added tax (VAT), if applicable, cost in 2020 US dollars (USD), and any potential price differences between public and private hospitals.
We selected the 50 mg vial pricing because of its availability in all countries included, even though rtPA treatment of a patient over 60 kg body weight (bw) always requires more drug and probably the opening of a second vial given the standard dose of 0.9 mg/kg bw, except for Japan, where the approved dose is 0.6 mg/kg bw.
For countries with >1 response to our survey with different price ranges, we recontacted the contributors to confirm the actual price for that country.
For each country, the proportion of hospitals that offer rtPA was classified as a minority (<35%), approximately half (35–65%), or a majority (⩾65%). We also collected the best available information regarding the nationwide proportion of acute stroke patients receiving rtPA, and insurance coverage status classified as full, partial, or none.
Financial metrics
The World Bank Open Data (https://data.worldbank.org/) was used to collect the following metrics per country, using the most current data available: gross domestic product (GDP) in 2020 USD, nominal and adjusted for purchasing power parity (PPP); 2020 GDP per capita nominal and adjusted for PPP; HE as percentage of GDP; and HE per capita nominal and adjusted for PPP. The most current available HE data used in this study are from 2018. Countries were classified according to income tier as HIC, UMIC, LMIC, and Low.
To ensure that rtPA prices were contemporaneous with financial metrics (i.e. 2020 prices for 2020 GDP and 2018 prices for 2018 HE), given that the prices were reported in 2020 USD, prices for 2018 were adjusted for inflation using the Consumer Price Index Inflation calculator by the Bureau of Labor Statistics, US Department of Labor (https://www.bls.gov/data/inflation_calculator.htm).
Statistical analysis
Continuous variables are reported as means (± standard deviation) or median (interquartile range). Normality was assessed by visual inspection and the Shapiro–Wilk test. The Wilcoxon rank-sum test was used for two-group comparisons and the Kruskal–Wallis test for more than two-group comparisons. Categorical variables are presented as percentages and compared by chi-square test.
To better characterize the impact of listed rtPA price within the context of each country’s financial capabilities, price was further analyzed as percentage per capita GDP (2020) and percentage per capita HE (2018).
We assessed the association between income classification and financial metrics, HE, and rtPA pricing. We hypothesized that countries in higher income tier would have significantly higher HE and accordingly higher rtPA prices compared to countries in lower income tiers. We also hypothesized that rtPA cost requires a significantly higher proportion of per capita GDP and HE in LMIC and UMIC as compared to HICs.
Analyses were conducted using JMP Pro 14 (SAS, North Carolina, USA).
Results
Survey answers, geographic and key financial metrics of included countries
A total of 80 respondents from 71 countries answered our survey between July and September 2021. Fifty-nine countries were included in the final analysis. Six countries were excluded due to rtPA unavailability, and six due to remaining uncertainty regarding the price.
The geographic distribution, population, income tier, and financial metrics of included countries are summarized in Figure 1 and detailed in Supplementary Table 2. Twenty-seven (46%) countries were classified as HIC, 20 (34%) as UMIC, and 12 (20%) as LMIC. The representative proportion of these countries, according to the World Bank data classification, were: 27/80 (34%) HIC, 20/55 (36%) UMIC, and 12/55 LMIC (22%). Of the six countries excluded due to rtPA unavailability, three were LIC, and three were LMIC. No LIC remained in the final analysis.
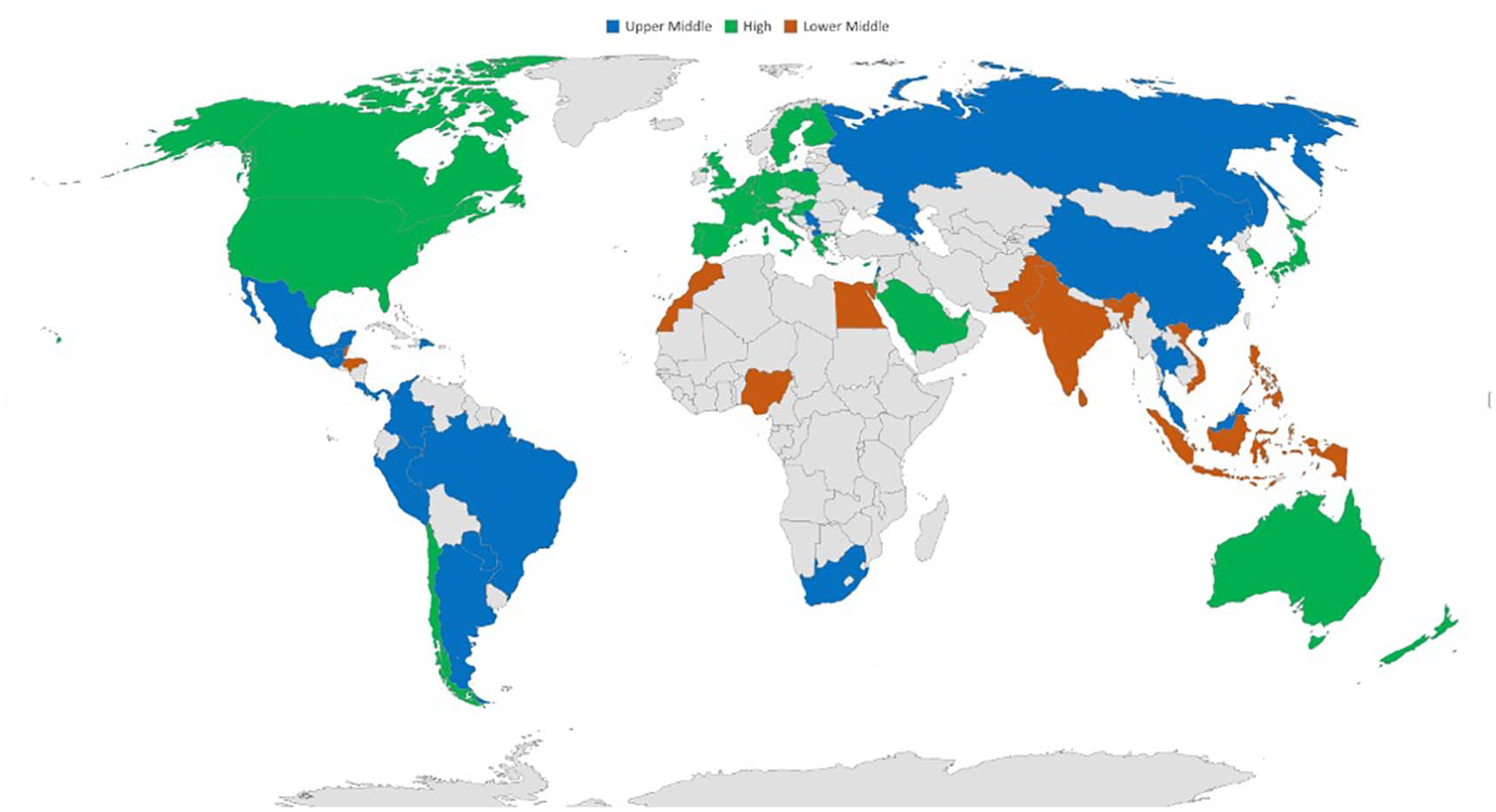
Geographical distribution and income classification of countries included in the analysis.
rtPA cost and its association with financial metrics
The results of rtPA cost in the different countries are summarized in Table 1. The median rtPA listed price for a 50 mg vial was USD 600, interquartile range (IQR) (475–1000), ranging from a minimum USD of 200 to a maximum of 4500. HICs have significantly higher nominal and PPP-adjusted per capita GDP, HE and percentage of their GDP allocated to HE (p < 0.0001) (Table 1). However, rtPA price is non-significantly higher in LMIC USD (755, IQR (575–1300)) compared to UMIC USD (544, IQR (400–815)) and high-income USD (600, IQR (526–1000)), p = 0.27.
Associations between income classification and rtPA price and financial and health expenditure metrics.
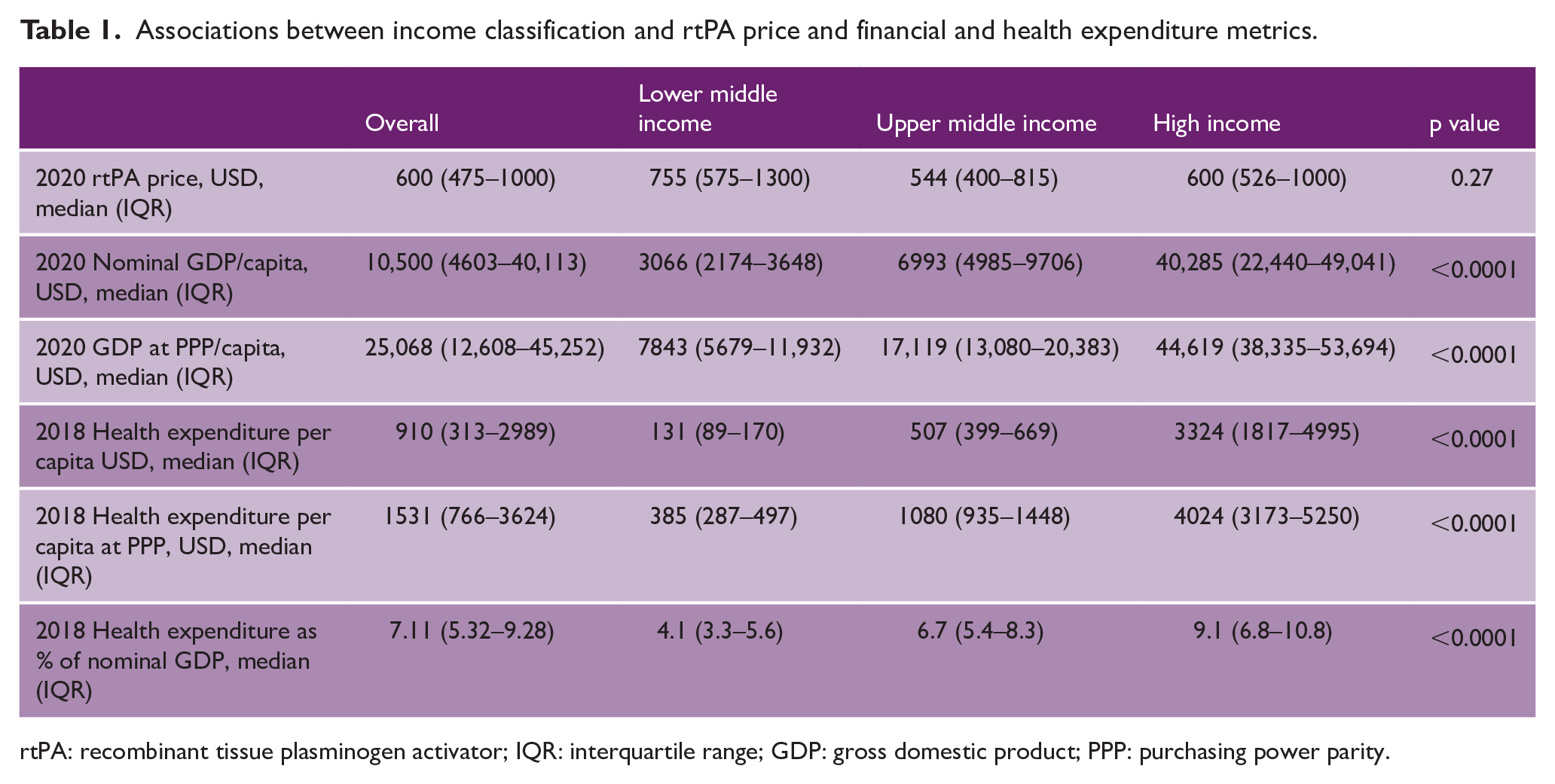
rtPA: recombinant tissue plasminogen activator; IQR: interquartile range; GDP: gross domestic product; PPP: purchasing power parity.
rtPA as percentage of per capita GDP and HE
Results are summarized in Table 2. RtPA price requires a significantly higher percentage of GDP and HE in LMIC compared to HIC. The median rtPA price equaled 24.3%, IQR (19.9–52.5%) of nominal yearly GDP per capita in LMIC, versus 2.2%, IQR (1.3–3.4) in HICs, p < 0.0001.
rtPA price as percentage of per capita GDP and HE and its association with income classification.
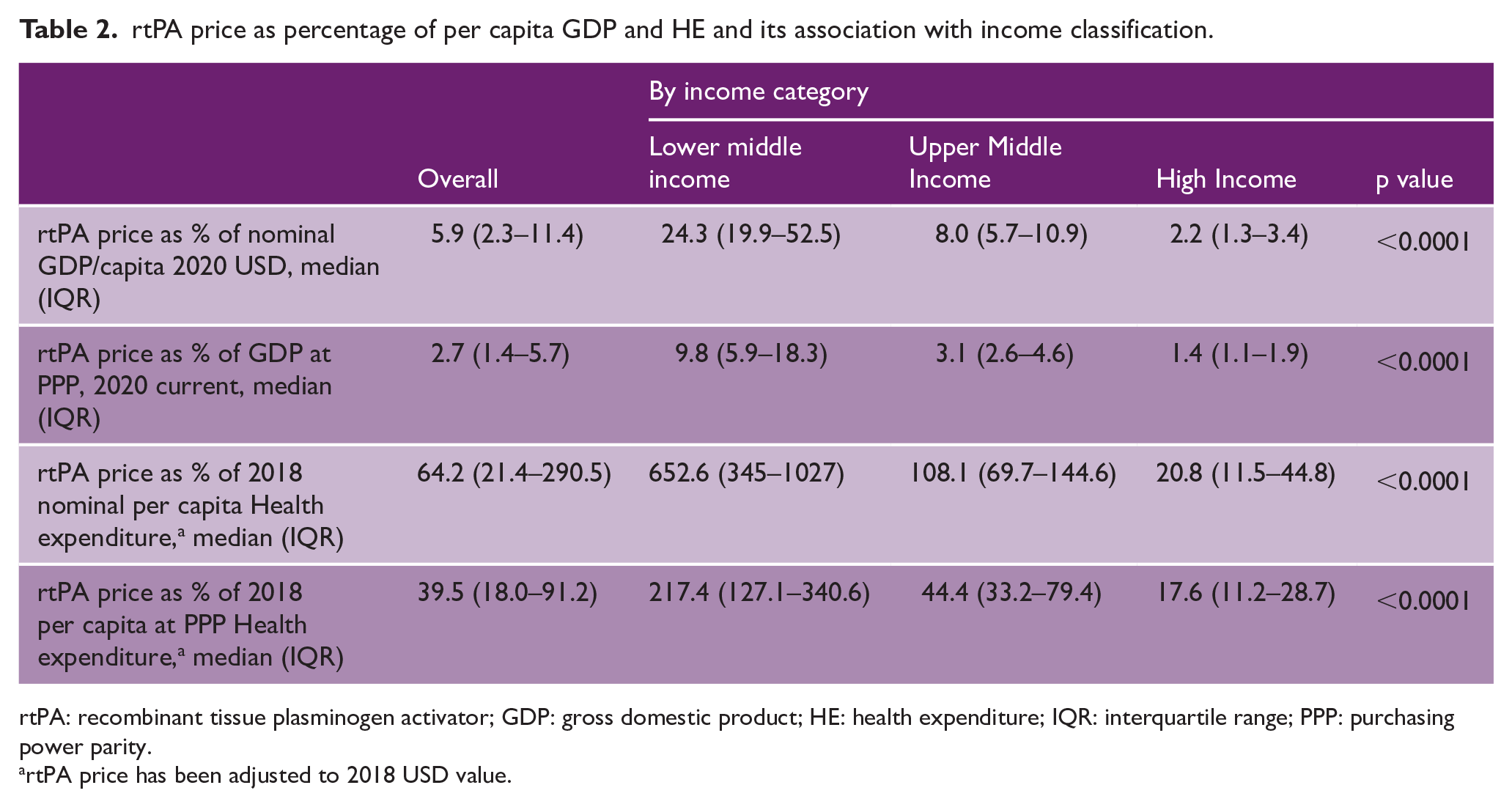
rtPA: recombinant tissue plasminogen activator; GDP: gross domestic product; HE: health expenditure; IQR: interquartile range; PPP: purchasing power parity.
rtPA price has been adjusted to 2018 USD value.
Median rtPA price equaled 652.6%, IQR (345–1027%) of nominal yearly per capita HE versus 20.8%, IQR (11.5–44.8%) in HICs, p < 0.0001.
Similarly, one dose of rtPA requires a significantly higher percentage of GDP and HE in LMIC compared to UMIC, and in UMIC compared to HIC (Supplementary Table 3).
rtPA availability and insurance coverage
rtPA availability is summarized in Table 3. Overall, the treatment is available in a majority (>65%) of hospitals in 21 (40%) countries, whereas in 27 (51%) countries it is available in <35% of hospitals.
rtPA availability and association with income classification.
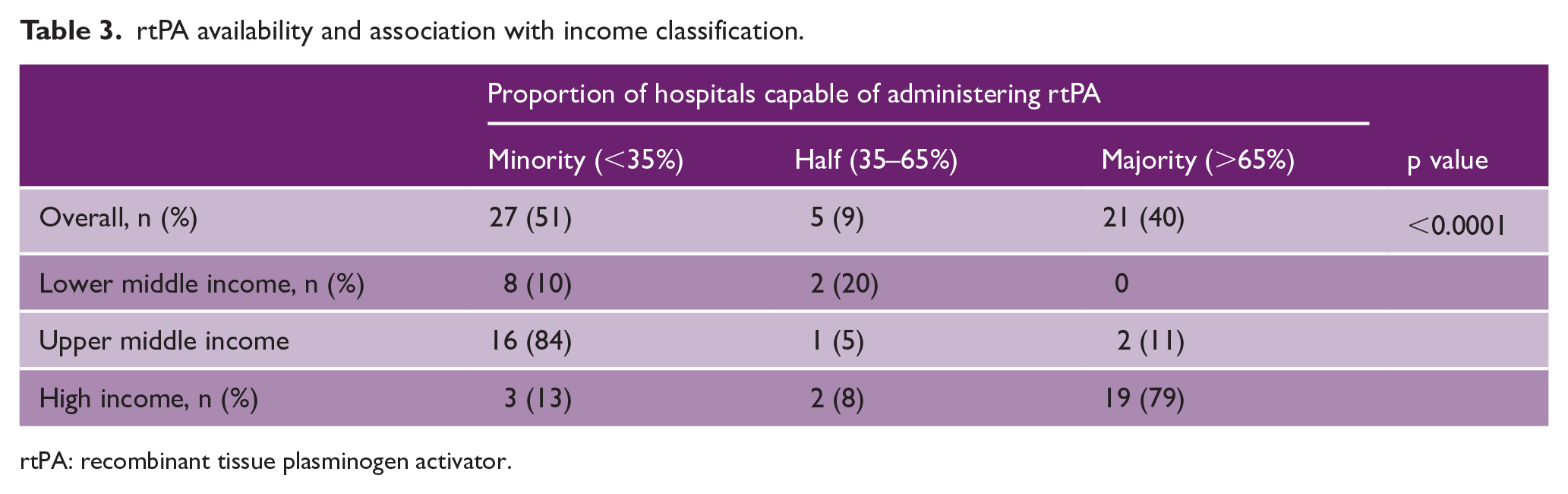
rtPA: recombinant tissue plasminogen activator.
We found a significant association between income tier and proportion of hospitals with rtPA availability (p < 0.0001). Nineteen (79%) of HICs have availability in >65% of their hospitals, but there is no LMIC reporting >65% availability.
RtPA coverage information is summarized in Supplementary Table 4: 35 (65%) countries offer full coverage. HICs and UMICs were significantly more likely to offer full coverage than LMICs (p < 0.0001). All five (9%) countries in which the patients have to bear the full cost for rtPA out-of-pocket are LMICs.
Discussion
In the present survey across all continents, we analyzed the variability in rtPA pricing among different countries and its association with financial metrics and HE. We found that, despite significantly lower per capita GDP and HE, the median rtPA price in LMICs is non-significantly higher than HICs. As a result, rtPA is significantly less affordable in LMICs where its median price exceeds the annual per capita HE. Hospitals in HICs are significantly more likely to offer rtPA compared to LMICs and cost coverage is also significantly better in HICs.
The rtPA has for long been shown to be a cost-effective treatment for acute ischemic stroke.4–7 However, significant barriers remain in treatment implementation worldwide, leading to disparities in drug availability and treatment access.11,13,14 Several interconnected economic and societal factors contribute to these disparities, such as increasing sales prices and governmental and private medical insurance coverage policies. 13 Funding for health insurance systems in LMIC is limited, and establishment and operating costs are prioritized over medication coverage. Our study findings highlight the magnitude of the problem: the median rtPA price for a 50 mg vial of rtPA in LMICs is over seven times the allocated per capita HE. Thus, as shown in our and previous studies, providing thrombolysis free of cost by the state is often not feasible in many LMICs.13,14 As a result, drug cost is passed along to stroke patients being in an emergency situation who often face the dilemma of either paying out of pocket or declining treatment. One study in Iran found that only 30% of Iranian rtPA-eligible patients could afford the treatment. 15 Another study in India showed that only 5 out of 22 rtPA-eligible patients could afford the drug costs. 16 Our study found that median rtPA price equals 24% of per capita GDP in LMICs, underscoring the affordability issues identified in several prior studies.
Limited availability of thrombolysis in resource-limited countries has important public health ramifications, considering that the bulk of the global burden of stroke is borne by LICs and LMICs. 17 Despite decreasing trends of stroke incidence and mortality rates, LICs and LMICs still account for 86% of stroke-related deaths and 89% of stroke-related Disability-Adjusted Life Years (DALYs) globally. 10 Age-standardized stroke-related DALYs is 3.7 times higher in LICs compared to HICs. 10 Importantly, a considerable proportion of acute strokes in LICs and LMICs occur at younger ages, further magnifying the societal impact. Treatment access and affordability are not limited to acute stroke reperfusion treatment but involves primary and secondary prevention and recovery and rehabilitation therapies as well, 18 further compounding the burden of stroke in these regions. In addition, the ongoing COVID-19 pandemic has further stressed economic and health resources globally and more so in the resource-deprived countries; this leads to a further decline of the already strained systems of stroke care including the availability and accessibility of rtPA in many LMICs.
This is the first study to assess the cost, availability, and disparities of rtPA usage among different economic environments worldwide. Our findings highlight the pressing need to bridge the wide gaps in the accessibility to optimal acute stroke treatment between HICs and LICs and LMICs. Close collaboration of major stakeholders, including public health insurance agencies, private insurers, medical societies and organizations, and the pharmaceutical industry, will be necessary to develop sustainable and context-appropriate strategies to improve the delivery of quality stroke care in low-resource settings. Despite the significant existing hurdles, recent examples of successful implementation of reperfusion therapies within the public health system in a UMIC context highlight the feasibility of such an endeavor and can guide similar future efforts.19,20
Our study has limitations. Despite our global outreach, we received responses only from 71 of 193 countries in which rtPA is approved and registered. Africa was especially underrepresented with only four countries included in the final analysis. This is mainly due to the fact that rtPA is largely unavailable in most African countries, thus supporting our main finding of limited drug availability in low-resource settings. Data were obtained from a survey which could introduce potential bias; we could not independently verify the accuracy of reported prices and the usage rates in each country. We adjusted for inflation to 2018 USD prices where necessary using a US-based inflation adjustment tool. Given that inflation rates vary widely among countries, this might have led to over- or under-estimation of computed 2018 rtPA prices.
Tenecteplase is considered a safe and effective alternative option for thrombolysis21–23 and attractive for low-resource settings given its simpler mode of administration. However, it lacks regulatory approval for ischemic stroke in a majority of countries and is not yet listed for stroke on the WHO Model List of Essential Medicines. Accordingly, we received limited information on Tenecteplase pricing in our survey (22/59 countries) and we were unable to verify the reported price in most of them, precluding meaningful analysis.
Our study has several strengths: although not all survey invitees responded, our final sample included a representative collection of countries including all continents and different income classifications. HICs, UMICs, and LMICs were represented, informed by leading stroke clinicians who chose to be members of the WSO, strengthening the validity of our findings. For financial metrics and HE, we used a publicly available and well-established data source and included both nominal and PPP-adjusted estimates of GDP and HE, facilitating between-country comparisons. In addition to raw rtPA prices, we further examined its relation to per capita GDP and HE, facilitating the interpretation of the findings within each country’s individual economic capabilities.
In summary, we documented marked variability in rtPA price among countries. Despite limited financial capabilities, the relative cost of rtPA is much higher in LMICs, exceeding the available annual per capita funds for HE. Concerted efforts to improve rtPA affordability in low-income settings are necessary.
Supplemental Material
sj-docx-1-wso-10.1177_17474930221082446 – Supplemental material for Regional and national differences in stroke thrombolysis use and disparities in pricing, treatment availability, and coverage
Supplemental material, sj-docx-1-wso-10.1177_17474930221082446 for Regional and national differences in stroke thrombolysis use and disparities in pricing, treatment availability, and coverage by Ana Claudia de Souza, Ivy Anne Sebastian, Wan Asyraf Wan Zaidi, Ahmed Nasreldein, Danira Bazadona, Pablo Amaya, Ahmed Elkady, Meron Awraris Gebrewold, Pongpat Vorasayan, Nune Yeghiazaryan, Patrik Michel, Pooja Khatri, Jeyaraj Durai Pandian, Sheila Cristina Ouriques Martins, Werner Hacke and Vasileios-Arsenios Lioutas in International Journal of Stroke
Supplemental Material
sj-pdf-1-wso-10.1177_17474930221082446 – Supplemental material for Regional and national differences in stroke thrombolysis use and disparities in pricing, treatment availability, and coverage
Supplemental material, sj-pdf-1-wso-10.1177_17474930221082446 for Regional and national differences in stroke thrombolysis use and disparities in pricing, treatment availability, and coverage by Ana Claudia de Souza, Ivy Anne Sebastian, Wan Asyraf Wan Zaidi, Ahmed Nasreldein, Danira Bazadona, Pablo Amaya, Ahmed Elkady, Meron Awraris Gebrewold, Pongpat Vorasayan, Nune Yeghiazaryan, Patrik Michel, Pooja Khatri, Jeyaraj Durai Pandian, Sheila Cristina Ouriques Martins, Werner Hacke and Vasileios-Arsenios Lioutas in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.C.d.S. declares lecture fees from Boehringer Ingelheim (BI); S.C.O.M. declares lecture fees from BI, Medtronic, Pfizer, Bayer, and Novartis; W.H. declares scientific cooperation with BI for over 25 years. He is on the steering committee of ANGELS and has received travel support and honoraria from BI; J.D.P. declares expert honoraria fees and travel support from BI since 2016 and is coordinator for ANGELS program in India; P.K. received funds from Genentech for the PRISMS trial of alteplase and scientific advisory board of HAMLET. P.M. was on advisory board and received speaker fees by BI more than 5 years ago; P.A. receives lecture fees from BI, Boston Scientific, and Abbott structural heart.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.