
Abstract
Background:
The first pass effect (FPE) is an independent predictor of functional independence in patients with large vessel occlusion in anterior circulation ischemic strokes. However, whether it predicts outcome in posterior circulation large vessel occlusion (PC-LVO) is uncertain. We aimed to study the frequency, characteristics, and predictors of FPE and its association with clinical outcomes in PC-LVO.
Method:
We performed an analysis from the prospective CICAT Registry. All patients with PC-LVO who underwent endovascular therapy between January 2016 and January 2020 were included. A centrally assessed clinical follow-up was performed at 3 months by blinded investigators. FPE was defined as the achievement of modified Thrombolysis In Cerebral Infarction 3 in a single pass of the endovascular thrombectomy device, and multi-pass effect (MPE) if it was achieved in more than one pass. A multivariable analysis was performed to identify whether FPE is an independent predictor of functional independence defined as a modified Rankin Score of 0–2.
Results:
We analyzed data from 265 patients in who FPE was achieved in 105 (39.6%). Patients with FPE were more likely to achieve functional independence compared to the non-FPE group (52.4% vs 25.1%, p < .001) and the MPE group (52.4% vs 26.7%, p < .001). FPE was independently associated with functional independence (adjusted odds ratio (aOR): 2.10, 95% confidence interval (CI) 1.01-4.37) but MPE was not (aOR: 0.92, 95% CI 0.40-2.13). Independent predictors of FPE were the use of direct aspiration, embolic mechanism of stroke, and the absence of general anesthesia (GA) use.
Conclusions:
FPE is an independent predictor of functional independence in PC-LVO and was associated with a significantly better outcome than MPE.
Introduction
Complete successful recanalization, defined as the presence of a modified Thrombolysis In Cerebral Infarction (mTICI) of 3, has been widely associated with maximal benefits in functional outcome at 3 months.1,2
The first pass effect (FPE), defined as the achievement of mTICI 3 in a single pass of the endovascular thrombectomy device, has been described as an independent predictor of good outcomes in patients with large vessel occlusion (LVO) undergoing endovascular thrombectomy (EVT) in anterior circulation stroke.3,4 Some specific variables, such as the use of a balloon guide catheter and thrombus location, have been related to this FPE. 5
Despite the lack of clear evidence of the clinical benefit of EVT in posterior circulation large vessel occlusion (PC-LVO), current guidelines recommend treating these patients endovascularly.6–9 The factors associated with FPE on PC-LVO and its impact on functional outcome is still poorly understood.10–13
We aimed to study the frequency, characteristics, and predictors of FPE on a PC-LVO population as well as the factors associated with functional independence at 3 months.
Method
Study population
CICAT (Codi Ictus Catalunya) is a government-mandated, prospective, hospital-based dataset in which all stroke codes are included in Catalonia. From January 2016 to January 2020, a total of 24,553 consecutive stroke codes were reported. A total of 3167 EVT were performed, and 41 (1.29%) patients were excluded from the analysis due to lack of 3 months follow-up. Finally, 265 patients with pc-LVO who were fully studied were included in the study (Figure 1).
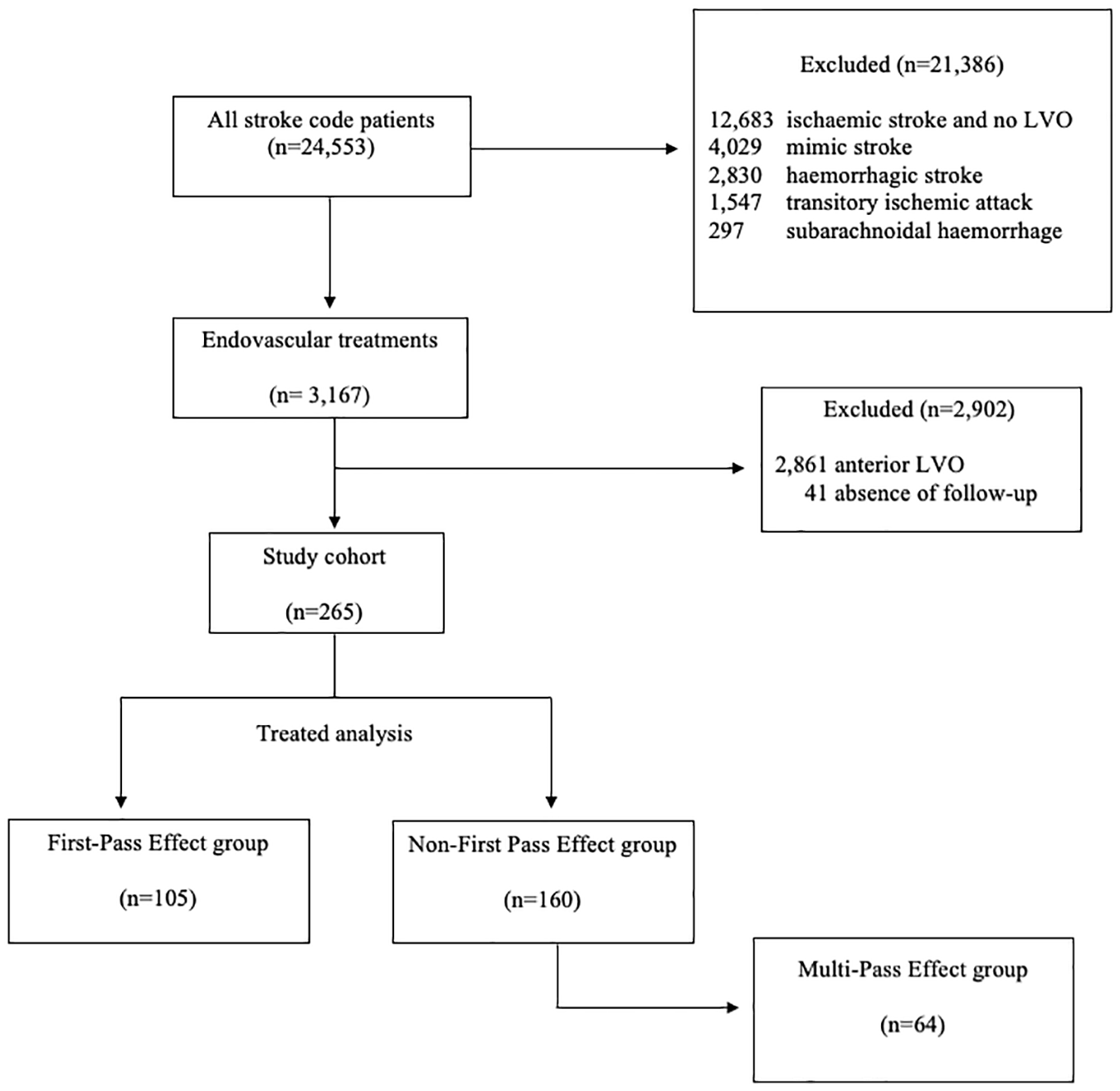
Study flowchart.
All patients included in this study have an angiographic confirmation of acute arterial occlusion of the basilar artery, posterior cerebral artery (PCA), or intracranial vertebral artery, less than 12 hours from stroke onset, a baseline pc-ASPECTS ⩽6 and a National Institute of Health Stroke Score (NIHSS)⩾6 or high disabling symptomatology.
The purpose of this study was approved by the governmental Catalan Review Board and the local Ethical Committee (codi CEIM 2021.071).
Variables
We collected demographical, clinical, and radiological data from all the patients who underwent EVT with at least one device pass.
In the current study, complete successful recanalization was defined by the presence of a modified Thrombolysis In Cerebral Infarction (mTICI) of 3 in the final cerebral angiography. FPE was considered if mTICI 3 was achieved in the first pass of the device. All other patients were classified in “non-FPE” group. For a second analysis, if mTICI 3 was achieved beyond the first pass, it was defined as multi-pass effect (MPE).
Neurological status was assessed by certified stroke neurologists at admission and during the whole follow-up by using the NIHSS, and all endovascular procedures were completed by neurointerventionsts and neuroanesthesiologists.
The occlusion site was evaluated by computed tomography angiography and confirmed by cerebral angiography run prior to the EVT.
Functional outcome at 3 months was centrally assessed by blinded evaluators of the Catalan Stroke Program using a structured telephone interview of the modified Rankin Score (mRS).
The primary outcome was the rate of functional independence (mRS score ⩽ 2) at 3 months. Secondary outcomes were anesthesia choice, technique during EVT, and mortality at 3 months.
Statistical analysis
The baseline characteristics were compared using the Student t test or the Mann–Whitney U test for continuous variables and the χ2 test for categorical variables. Univariate analyses were performed to study variables associated with clinical outcome and FPE. Continuous variables are shown as mean (standard deviation, SD) or median [interquartile intervals] and were compared with the Student t test, analysis of variance, Mann–Whitney, or Kruskal–Wallis tests as appropriate. Categorical variables were reported as proportions.
Logistic regression was used to study the association between FPE and the primary outcome and to adjust for possible confounders. Variables showing a trend toward significance (p value < .1) were entered in the multivariable logistic models.
Data were analyzed with SPSS version 22.0 software, and all tests were performed with a 5% significance level.
Results
Two hundred and sixty-five patients were included in the study. The median age was 72 [63–80] years and 103 (38.9%) were female.
FPE was achieved in 105 (39.6%) patients. No statistically significant differences were observed in baseline characteristics between patients presenting FPE versus no-FPE. Intravenous thrombolysis administration rate and NIHSS at admission were similar in the two groups. No differences were observed in pc-ASPECT scores and occlusion arterial locations (Table 1).
Baseline, procedural characteristics, and outcomes.
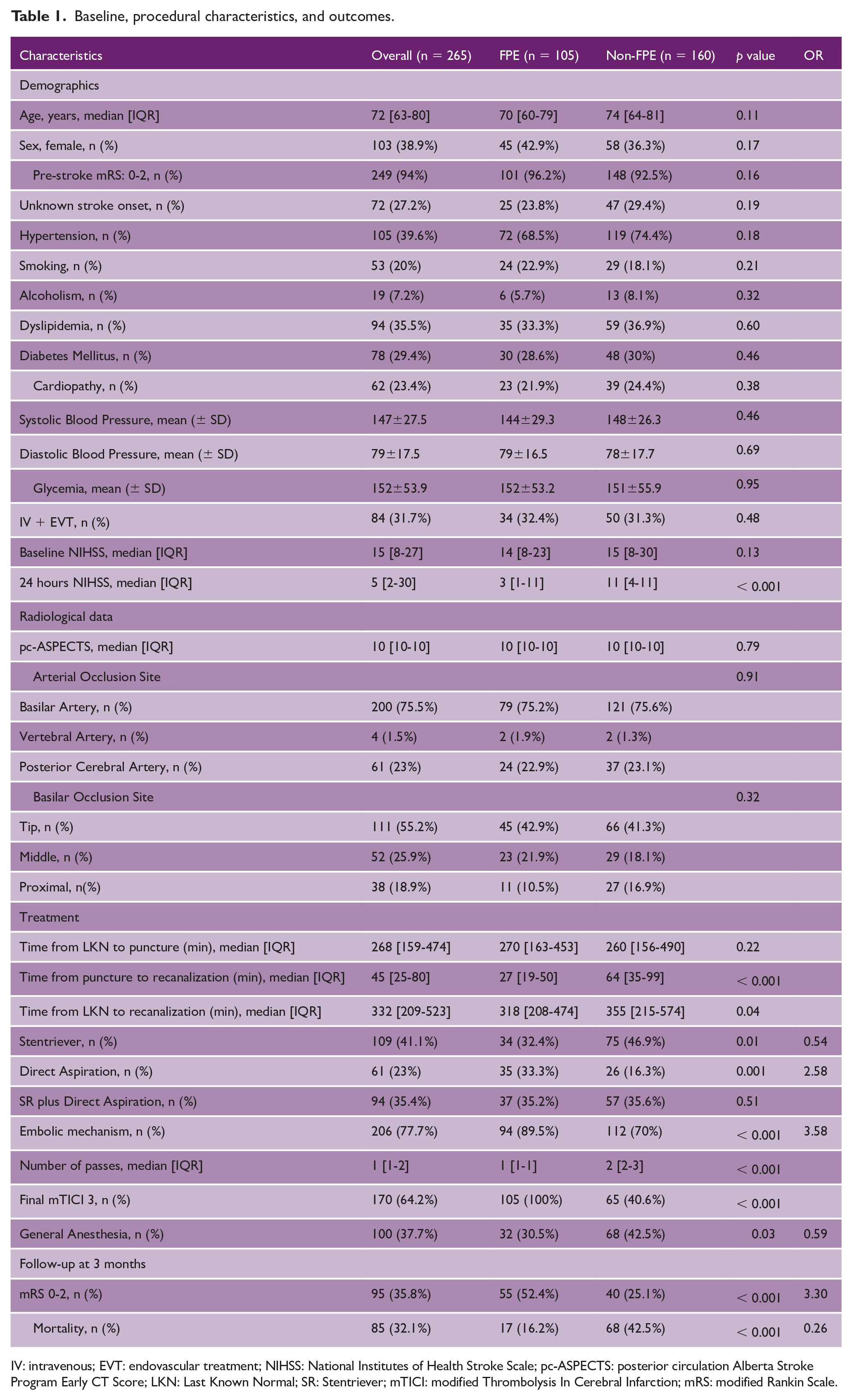
IV: intravenous; EVT: endovascular treatment; NIHSS: National Institutes of Health Stroke Scale; pc-ASPECTS: posterior circulation Alberta Stroke Program Early CT Score; LKN: Last Known Normal; SR: Stentriever; mTICI: modified Thrombolysis In Cerebral Infarction; mRS: modified Rankin Scale.
Patients from the FPE group had significantly shorter times from puncture to recanalization (27 vs 64 min, p < .001) and from last known normal (LKN) to recanalization (318 vs 355 min, p = .04). However, times from LKN to puncture were similar in both groups (270 vs 260, p = .22).
The use of direct aspiration (DA) as a first-line strategy was more frequent in the FPE (33.3% vs 16.3%, p = 0.001) and a final mTICI of 3 was significantly higher in this group (100% vs 40.6%, p < .001). General anesthesia was significantly less used in the FPE group (30.5% vs 42.5%, p = .03).
Patients in whom FPE was achieved had significantly better neurological status at 24 h (NIHSS: 3 vs 11, p < 0.001), a better functional outcome at 3 months (mRS 0–2: 52.4% vs 25.1%, p < .001, odds ratio (OR):3.30), and lower mortality (16.2% vs 42.5%, p < .001, OR:0.26).
Table 2 shows the results of the unadjusted and adjusted logistic regression model demonstrating the association between the FPE and favorable functional outcome at 3 months of follow-up. In the multivariable analysis, FPE was the only variable identified as an independent predictor of functional independence (adjusted OR, 2.8 (95% confidence interval [CI], 1.29–6.06); p = .009). On the other hand, age and general anesthesia (GA) were identified as independent predictors of poor outcome.
Univariate and multivariable regression model for functional independence at 3 months.
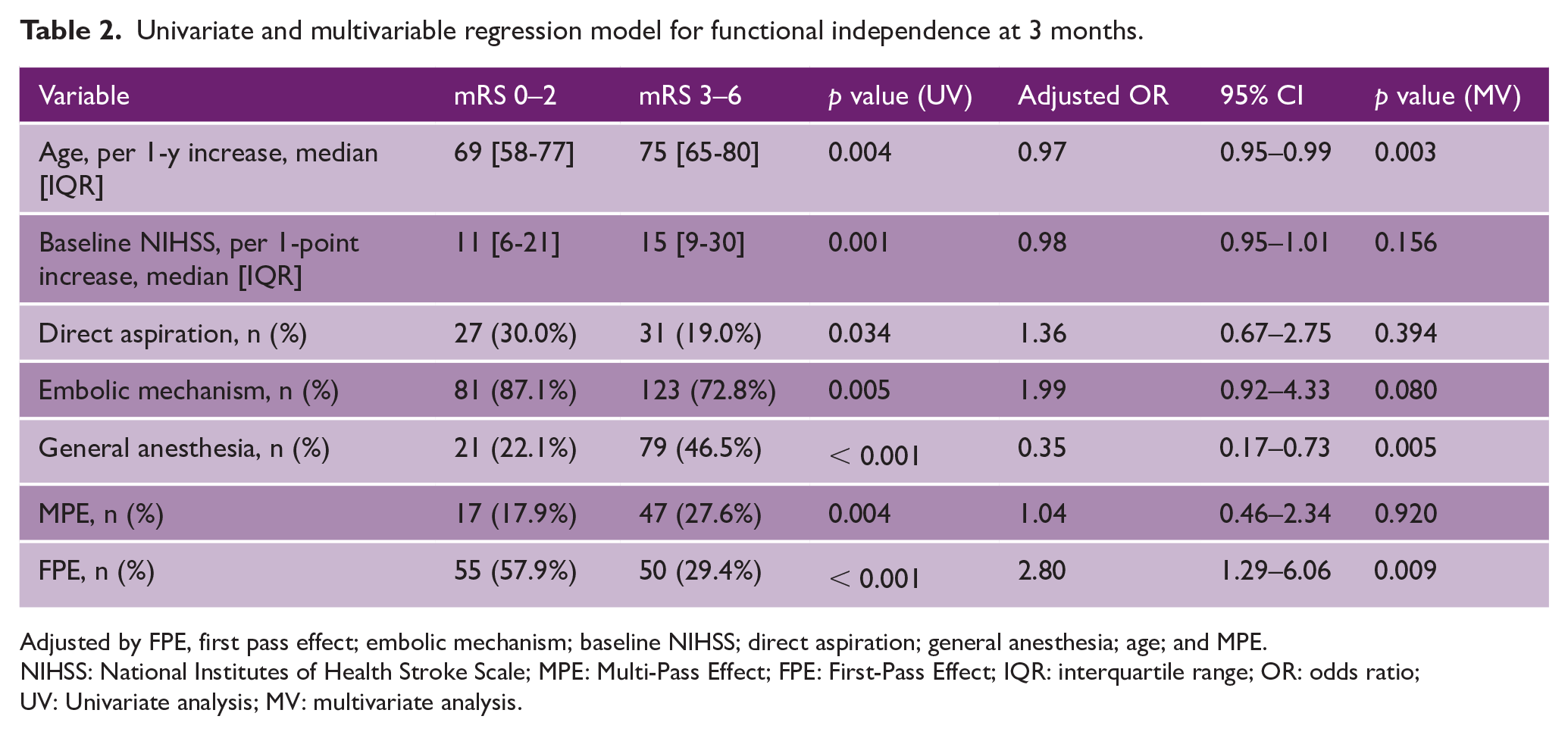
Adjusted by FPE, first pass effect; embolic mechanism; baseline NIHSS; direct aspiration; general anesthesia; age; and MPE.
NIHSS: National Institutes of Health Stroke Scale; MPE: Multi-Pass Effect; FPE: First-Pass Effect; IQR: interquartile range; OR: odds ratio; UV: Univariate analysis; MV: multivariate analysis.
A final mTICI of 3 was achieved in a total of 169 patients (63.8%). Of these, 105 (61.8%) were in the FPE group, and in 64 (37.9%) patients, the mTICI 3 was obtained in more than one pass (MPE). When comparing the two groups, MPE was significantly associated with lower functional independence odds compared to the FPE group (26.7% vs 52.4%, p < .001) and with higher mortality (40.6% vs 16.2%, p < 0.001) (Figure 2 and supplementary material, Table 1).
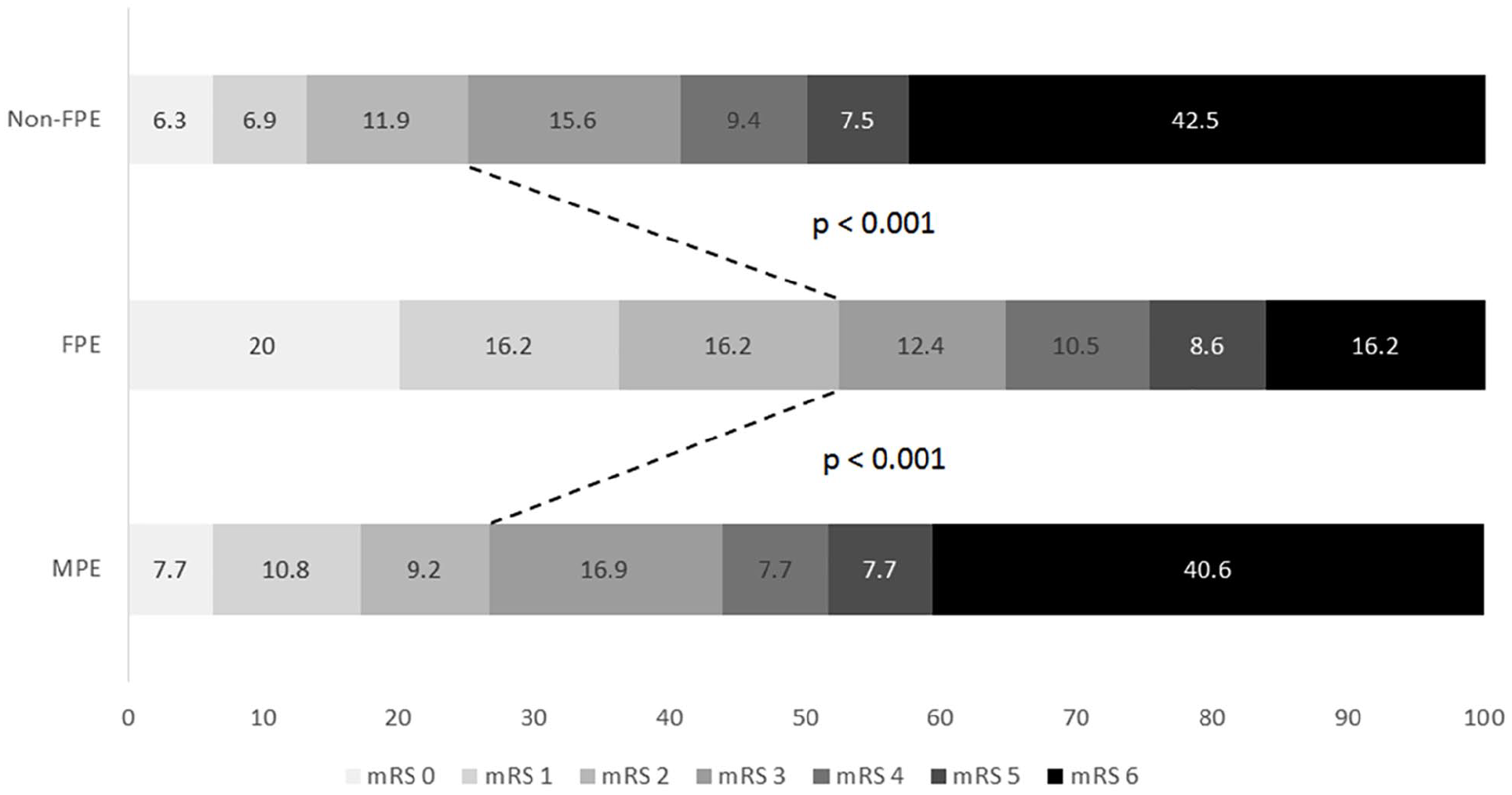
modified Rankin Scale at 3 months distribution according to non-FPE, FPE, and MPE.
As expected, the time from puncture to recanalization was shorter in the FPE group (Table 1). The independent predictors of FPE after adjusting by potential confounders were the use of DA (aOR 2.27 (95% CI, 1.18-4.35); p = .014), the embolic mechanism of stroke (aOR 3.09 (95% CI, 1.42-6.70); p = .004), and the absence of GA use (aOR 0.52 (95% CI, 0.29–0.93); p = .029) (Table 3).
Multivariable regression model for FPE.
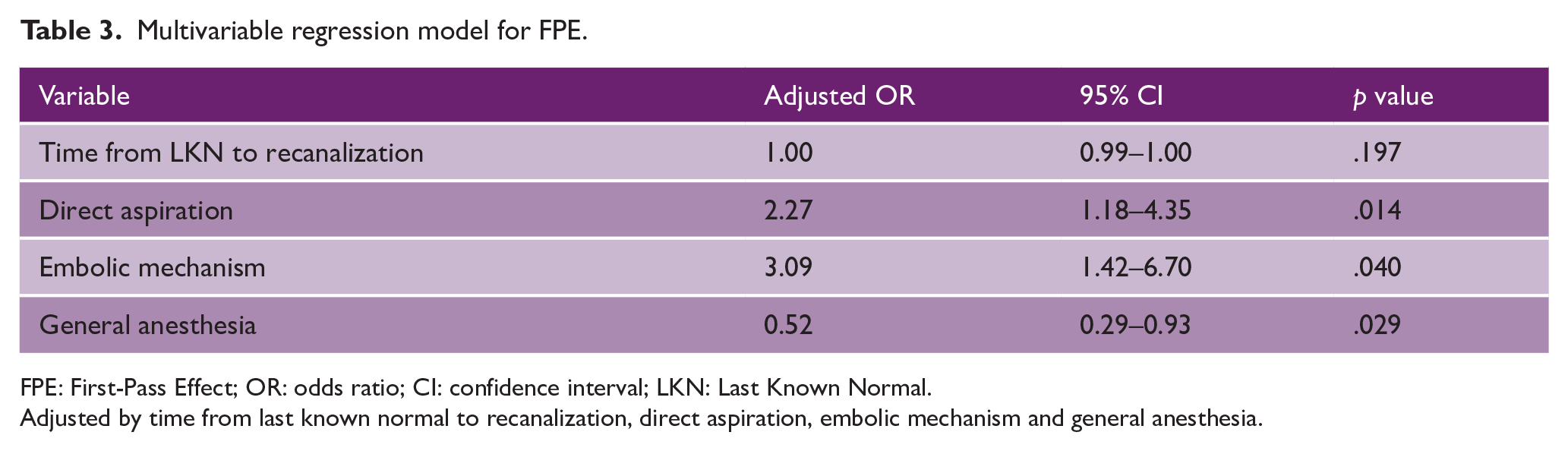
FPE: First-Pass Effect; OR: odds ratio; CI: confidence interval; LKN: Last Known Normal.
Adjusted by time from last known normal to recanalization, direct aspiration, embolic mechanism and general anesthesia.
In patients with arterial recanalization (mTICI 2b-3), the rate of functional independence with one device pass was 47.6%, 32.2% with two passes, 27.3% with three passes, 20.0% with four passes, and 18.2% with more than four passes. The rate of functional independence in the group of patients with no recanalization (mTICI 0-2a) was 16.2% (Figure 3).
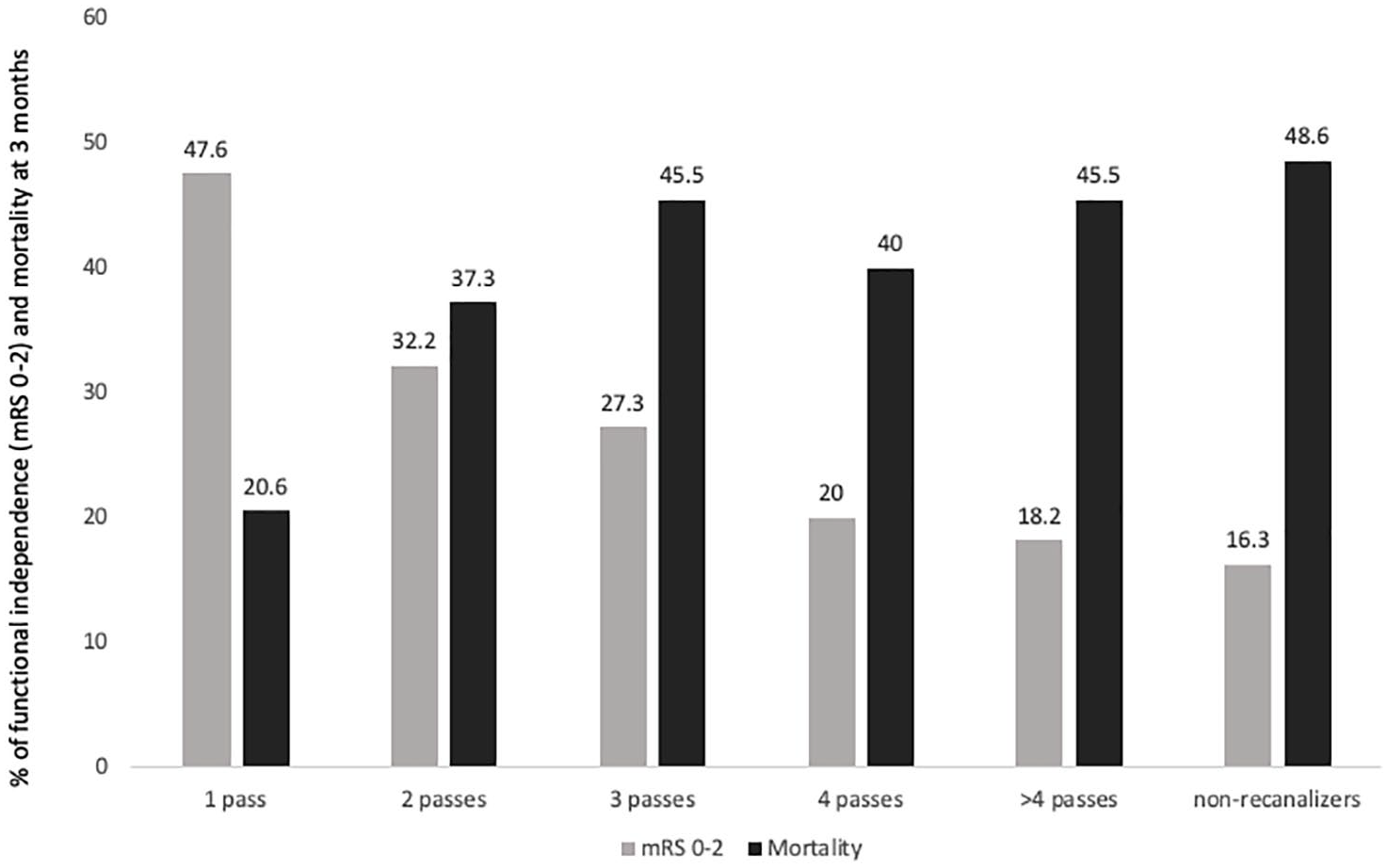
Rates of functional independence and mortality at 3 months for each number of device passes in recanalizers (mTICI 2b-3) and non-recanalizers (mTICI 0-2a).
Discussion
In our series, the presence of FPE seems to be critical in identifying patients with a high likelihood of functional independence at 3 months in patients with PC-LVO undergoing endovascular treatment. The absence of FPE was associated with worse outcomes and higher mortality compared to the FPE group. Moreover, MPE was significantly associated with poorer outcomes compared to FPE. The independent predictors of FPE were the DA use, embolic source of stroke, and the absence of GA use.
Our conclusions are comparable with previous studies in the anterior circulation. Basing their results on the NASA registry, Zaidat et al. reported significantly higher functional independence at 3 months in the FPE group compared to the non-FPE group (55.1% vs 31.3%, P < 0.0001) and compared with any TICI 3 beyond the FPE (61.3% vs 55%). The use of balloon guide catheter and the absence of internal carotid artery terminus occlusion were predictors of FPE. 3 Other studies report similar data with a net benefit of FPE in anterior circulation LVO.14–16
Some studies have highlighted the importance of achieving complete recanalization in the first pass, rather than in multiple passes in the anterior circulation.17,18 In this context, we report similar data, with significantly higher rates of functional independence in patients from the FPE group, compared to patients with mTICI 3 in more than a single pass, and in the multivariable analysis, we identify the FPE but not the final mTICI 3 as an independent predictor of functional independence. Moreover, the rate of functional independence declines progressively while the mortality increases from the first pass to the second and beyond passes, although the rates of functional independence are still higher when more than four passes are required to achieve recanalization compared with non-recanalizers (Figure 3).
The evidence and impact of FPE on functional independence in patients with PC-LVO is more limited. Jadhav et al. reported a series of 80 patients with basilar artery occlusion, of them, 19 (23.8%) achieved FPE, slightly lower percentages compared with our series in which we also include vertebral and PCA occlusions, that could influence these differences. The authors state that they were unable to perform multiple logistic regression due to the limitations of the sample data. 10
Recently, Alexandre et al. published a series of 191 patients with basilar and vertebral arterial occlusions. They concluded that female sex and the use of large-bore catheters were independently associated with FPE mTICI 2b-3. On the other hand, baseline NIHSS and pc-ASPECTS were associated with functional outcomes; however, in this study, FPE mTICI 2b-3 was not a predictor of good outcome. They reported similar rates of FPE mTICI 3 (42.9% vs 39.6%) and independent functional outcomes compared to our series (38.2% vs 35.8%, respectively). No analysis regarding the FPE mTICI 3 and functional outcome was reported in this study. 11
Also, den Hartog et al. published their experience from MR CLEAN Registry. In a retrospective analysis from 224 patients, they found an association between FPE and functional independence but with no differences between FPE and MPE groups. The authors did not identify any factor associated with FPE. 12
Finally, ETIS investigators identified FPE (TICI 2c-3) in approximately one-third of patients with basilar occlusions, and FPE was associated with favorable outcomes. The authors identified atheromatous etiology as a negative predictor of FPE, 13 comparable results with those that we present in our study where the embolic mechanism was independently associated with FPE, a finding that is in line with the underlying embolic substrate in most cases of tip basilar occlusions, in which successful recanalization is more likely to be achieved.19,20
FPE has been related to the technique during the EVT in some studies. Di Maria et al. 21 concluded that local anesthesia and thromboaspiration were independent predictors of FPE in a report of 1,832 patients from the ETIS Registry treated endovascularly.
Zaidat et al., 22 in a series of 715 patients from the STRATIS registry, identified that the use of a longer stent was independently associated with FPE, with no impact on clinical outcome. Ducroix et al. 23 did not find statistical associations between the use of stent retriever nor contact aspiration and the FPE. In our series, we reported higher use of DA in the FPE group, and this technique remains as an independent predictor of FPE in the multivariable regression model, but it was not independently associated with good outcomes. In this line, some other studies have reported a potential benefit in terms of higher recanalization rates by using DA as a first-line strategy in basilar occlusion but with no association with FPE.24,25
The main strengths of this study are the high data quality due to systematic, prospective, multicenter, and central blinded outcome data collection at 3 months by a mandatory governmental registry and the largest series published so far exploring the effect of FPE in PC-LVO. Moreover, this is the first study that correlates the superiority of FPE versus MPE on functional independence in all posterior circulation strokes. However, our study has some limitations. First, it is a retrospective analysis, despite the data having been collected prospectively in the CICAT mandatory stroke registry, there is missing data in 1.29% of all EVT due to lack of follow-up at 3 months. Second, the final mTICI was provided by local investigators although they were blinded to this analysis, and the recanalization rates reported are similar to other studies.11–13 Third, the relatively low sample of patients avoids some robust secondary analysis such as direct comparison between FPE and MPE. Fourth, the specific size of stent retriever and aspiration catheter was not available for all patients in our dataset, we were, therefore, unable to assess a correlation between the size of the device and FPE.
Conclusion
In our study, FPE is independently associated with functional independence in patients with PC-LVO treated endovascularly. Endovascular techniques and strategies in PC-LVO should be focused on achieving a complete successful recanalization in a single pass of the endovascular thrombectomy device due to its association with favorable clinical outcomes compared to any MPE.
Supplemental Material
sj-docx-1-wso-10.1177_17474930221089772 – Supplemental material for First pass effect in posterior circulation occlusions: Analysis from the CICAT registry
Supplemental material, sj-docx-1-wso-10.1177_17474930221089772 for First pass effect in posterior circulation occlusions: Analysis from the CICAT registry by Mikel Terceño, Yolanda Silva, Saima Bashir, Ángel Chamorro, Natalia Pérez de la Ossa, María Hernandez-Pérez, Carlos Castaño, Pol Camps-Renom, Denisse Wenger, Pere Cardona, Carlos Molina, Ana Rodríguez-Campello, David Cánovas, Francisco Purroy, Mercè Salvat-Plana and Joaquín Serena in International Journal of Stroke
Footnotes
Correction (March 2023)
Article updated online to correct Mercé Salvat-Plana’s affiliation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was sponsored by RETIC INVICTUS Plus RD16/0019, Instituto de Salud Carlos III, European Regional Development Fund (ERDF).
ORCID iDs
Data availability statement
The data that support the findings of this study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.