
Abstract
Background:
Stroke is a major global cause of death and disability. Most strokes occur in populations of low-middle-income country (LMIC); therefore, the subsequent disease burden is greater than in populations of high-income countries. Few epidemiological data exist for stroke in Latin America, composed primarily of LMIC.
Aims:
To determine epidemiological measures of incidence, prevalence, and 1-month case-fatality for stroke in Latin America/Caribbean (LAC) during 1997–2021.
Summary of review:
A structured search was conducted to identify relevant references from MEDLINE, WOS, and LILACS databases for prospective observational and cross-sectional studies in LAC populations from January 1997 to December 2021. A total of 9242 records were screened and 12 selected for analysis, seven incidence studies and five prevalence studies. Case-fatality was reported in six articles. Sub-group analysis by age, sex, and income countries was performed. A narrative synthesis of the findings was performed. Meta-analysis was performed using random-effect model to obtain pooled estimates with 95% confidence intervals (CIs). Studies quality was assessed according to the risk of bias criteria described in the Joanna Briggs Institute’s guide. The overall crude annual incidence rate of first-ever stroke in LAC was 119.0 (95% CI = 95.9–142.1)/100,000 people (with high heterogeneity between studies (I2 = 98.1%)). The overall crude prevalence was 3060 (95% CI: 95.9–142.1)/100,000 people (with high heterogeneity between studies (I2 = 98.8%)). The overall case-fatality at 1 month after the first stroke was 21.1% (95% CI = 18.6–23.7) (I2 = 49.40%).
Conclusion:
This review contributes to our understanding regarding the burden caused by stroke in LAC. More studies with comparable designs are needed to generate reliable data and should include both standardized criteria, such as the World Health Organization clinical criteria and updated standard methods of case assurance, data collection, and reporting.
Introduction
Stroke is one of the leading global causes of death and disability. 1 Seventy percent of strokes occur in populations of low-middle-income countries (LMICs), and the subsequent burden of disease is higher than in populations of high-income countries. 1 Some previous studies of stroke showed that incidence is increasing in low- and middle-income countries, by contrast with high-income countries where a 42% decrease in incidence has taken place in the past four decades. 2 It is unclear if this steadily declining trend has been sustained in recent years, particularly in view of the continuing aging of the population and the rise of diabetes mellitus and obesity. 3 However, between 1990 and 2017, the absolute number of people with incident strokes has increased significantly by 81%, the number of people who survived by 95%, and number of deaths caused by stroke by 40%. 2
Latin America, with an estimated population of 680 million inhabitants, has a marked ethnic, cultural, and socioeconomic heterogeneity. 4 Despite the progress that has been made in recent decades, aging and population growth have led to an increase in the prevalence of cardiovascular risk factors, raising absolute numbers of death and disability due to stroke and cardiovascular diseases. 5 In these countries, the burden of stroke was 5–14 disability-adjusted life years per 1000 population (age standardized to 2002), which is higher than in most high-income countries. 6
Research about stroke risk factors and epidemiology is based mostly on studies from North America or Europe. Stroke epidemiology has been poorly studied in Latin America/Caribbean (LAC),7,8 which is primarily composed of LMIC. The most sensitive tool to study stroke is with standardized population-based registries, since the analysis limited to hospital cases or the variation of criteria and definitions can distort the results. 9 The methodological differences between case ascertainment, classification, definitions, and reference populations for standardization are some of the problems in the region. 10 Also, environmental, racial, and sociocultural factors can have a significant impact on the epidemiology of stroke in such a wide area.
The aim of this systematic review was to determine epidemiological measures of incidence, prevalence, and 1 month of case-fatality for stroke in LAC during 1997–2021.
Methods
The protocol for the review was registered in PROSPERO (CRD42022325247). A prevalence and incidence systematic review was developed according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) and Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist (Supplemental Table S.1).
Selection criteria
This review included prospective observational studies (e.g. community-based and cohort studies) reporting the incidence and case-fatality of stroke in 36 countries of LAC (Supplemental Table S.2). Cross-sectional studies for the assessment of the stroke prevalence were also included.
Study populations had to include adult participants with a confirmed stroke diagnosis, which was defined by the studies according to established clinical criteria, including cerebral infarction, intracerebral hemorrhage (ICH), subarachnoid hemorrhage (SAH), or uncertain pathological subtypes.
Studies using retrospective recruitment (e.g. case series and case–control), reviews, commentaries, and editorials were excluded.
Search strategy
A structured and comprehensive literature search was carried out to identify relevant studies from MEDLINE (Ovid), Lilacs and Science Citation Index Expanded (SCI—EXPANDED), Social Sciences Citation Index and Arts, and Humanities Citation Index within ISI Web of Science (WoS) (from inception to May 27, 2022).
The search strategy was similar to the one published by Jones et al. 11 Cochrane stroke strategy terms were combined and filtered by epidemiology studies, including terms for Latin America and Caribbean.12,13 Only studies published in English, Portuguese and Spanish from 1 January 1997 to 31 December 2021 were eligible for inclusion (Supplemental Tables S.3 to S.5). We chose 1997 as a starting year for this review as well as the Stroke Unit Trialists’ Collaboration 14 systematic review, considering this year as a landmark in global standardization for post-stroke care, a couple of years after the intravenous thrombolysis was proven effective treatment for acute ischemic stroke (IS).
Selection process
Before study selection, references obtained were imported into EndNote 20 and duplicates were removed using the automated function, and then manually by reviewer. All references were imported into JBI SUMARI software (http://www.jbisumari.org/) to carry out the selection process. 15
Two independent reviewers (CD and MN) screened and selected all titles and abstracts potentially relevant. The full texts of these articles were independently assessed for eligibility. In cases of multiple publications based on the same patients’ cohort, only those studies including the largest sample size and more complete data were selected to avoid overlapping. Disagreements were resolved by discussion and when it was necessary, a third reviewer was involved to reach consensus.
Outcomes measures
Main outcomes were the cumulative incidence, prevalence per 100,000 people and 30-day case-fatality of stroke in LAC between January 1997 and December 2021.
Data extraction
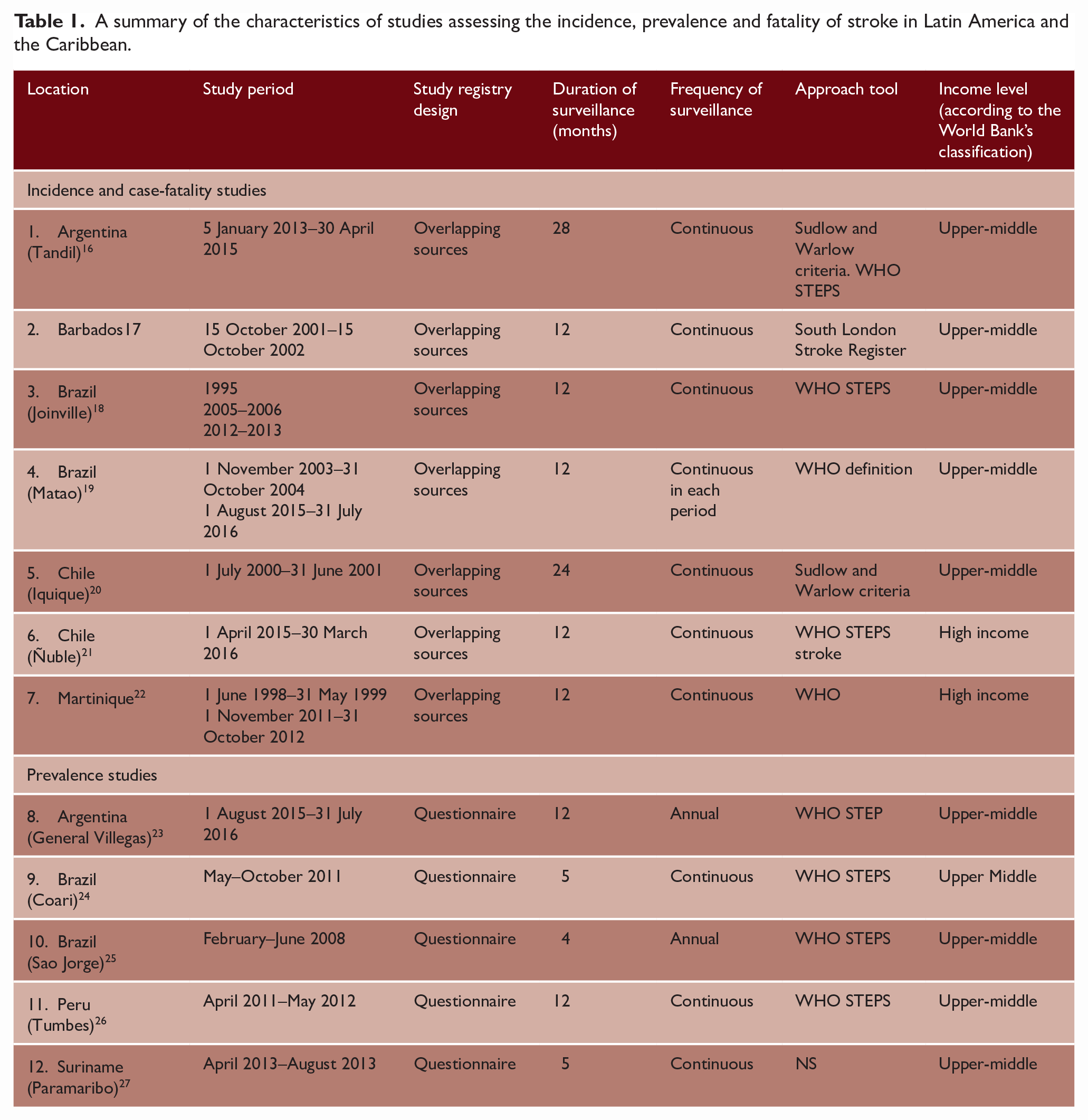
Two reviewers extracted data (CD and MN) independently using a standardized form piloted on a small number of included studies. Extracted data included: author and year of publication, study period, location, study design, sample size, mean age, and population type. Eligible studies were prepared for synthesis (tabulating the characteristics of each study) (Table 1).
A summary of the characteristics of studies assessing the incidence, prevalence and fatality of stroke in Latin America and the Caribbean.
Quality study and risk of bias assessment
The quality of studies was evaluated by two independent reviewers for each study design, using the Joanna Briggs Institute (JBI) 28 checklists for cohort or prevalence studies. Subsequently, disagreements were resolved by discussion and when it was necessary, a third reviewer was involved to facilitate consensus (Supplemental Table S.6).
Data synthesis and analysis
For incidence and prevalence rates, results were reported as presented in the original studies with the 95% CI. CIs were calculated if not available. Age-adjusted incidence was reported. Case-fatality data were reported as presented in the original studies, with the percentage of deaths within the first 30 days of the stroke. Analysis by type of stroke was reported in incidence, prevalence, and case-fatality data. The country income groups were classified according to the World Bank’s country classification. 4
Descriptive statistics were used to describe the studies characteristics; mean value with standard deviation (SD) for continuous data, and frequency in percentage and its 95% CI, for categorical variables.
The heterogeneity across the studies was assessed through visual inspection of the forest plot, and determining the χ2 and I2 statistics, and sub-group analysis. Meta-analysis was performed using metaprop command and forest plots were generated to summarize overall estimates. A random-effect model was used to obtain pooled estimates with 95% CIs.
Publication bias was assessed with Egger’s test to determine a potential risk of reporting bias. Metabias command was formed for each analysis in incidence, prevalence, and case-fatality.
All analysis was performed in STATA v.17.1/SE software (College Station, TX: StataCorp LLC).
Results
Study selection
A total of 9242 articles were identified, of which 1941 duplicates were removed. After reading the titles and abstracts, 116 potential full texts were screened for eligibility. Finally, 12 articles were included.16–27 The PRISMA flow chart is shown in Figure 1.
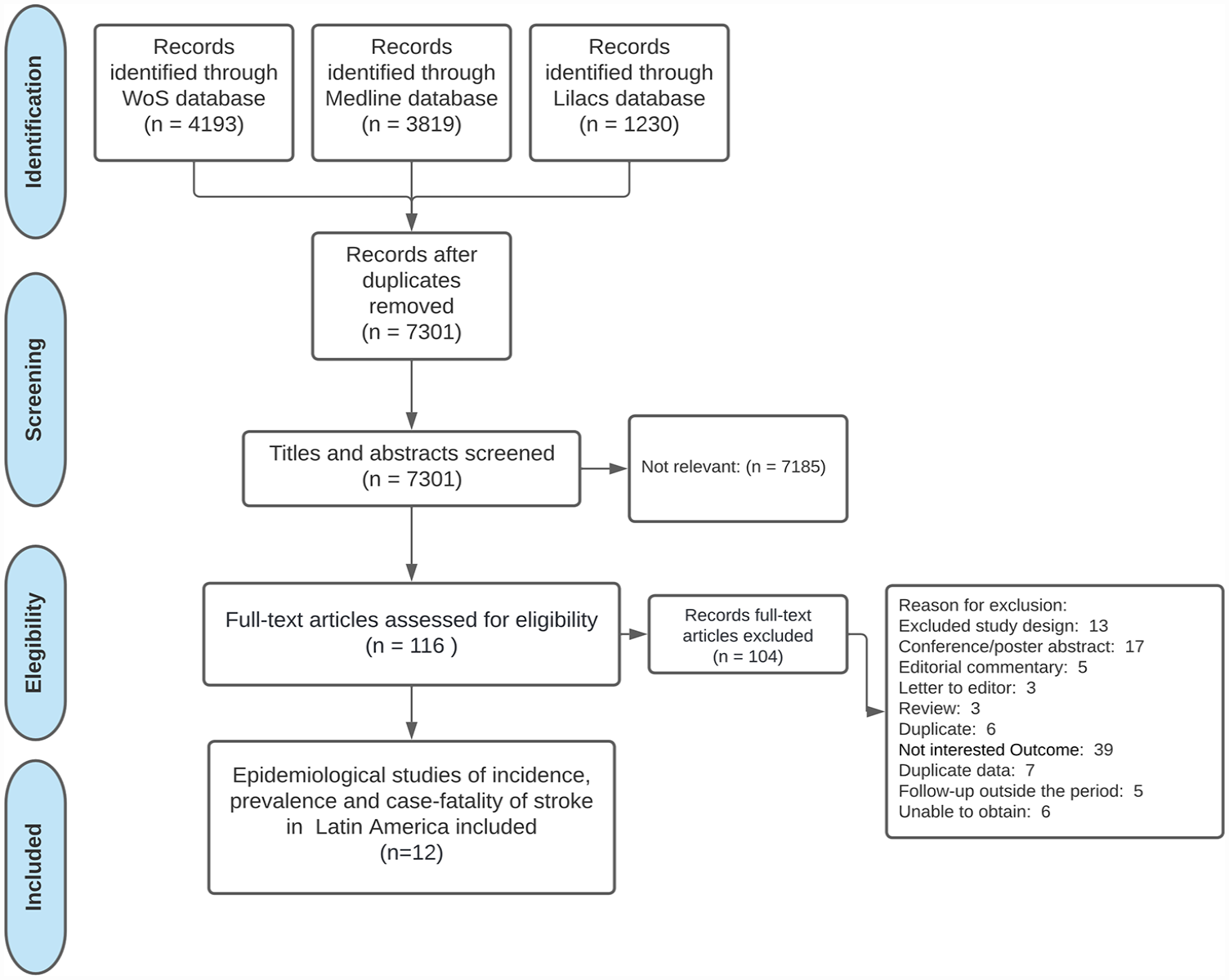
The PRISMA flow diagram.
Characteristics of the included studies
The review included 12 articles: seven cohort studies for incidence and 1-month case-fatality analyses, 16 – 22 and five cross-sectional studies for prevalence analysis. (Table 1).23–27 The articles included participants with stroke diagnosis confirmed by clinical criteria. Data from Brazil (n = 4) followed by Argentina (n = 2) and Chile (n = 2) were the most frequent, the earliest study period was in 1998–1999, 22 and the most recent in 2015–2016 (Figure 2).19,23
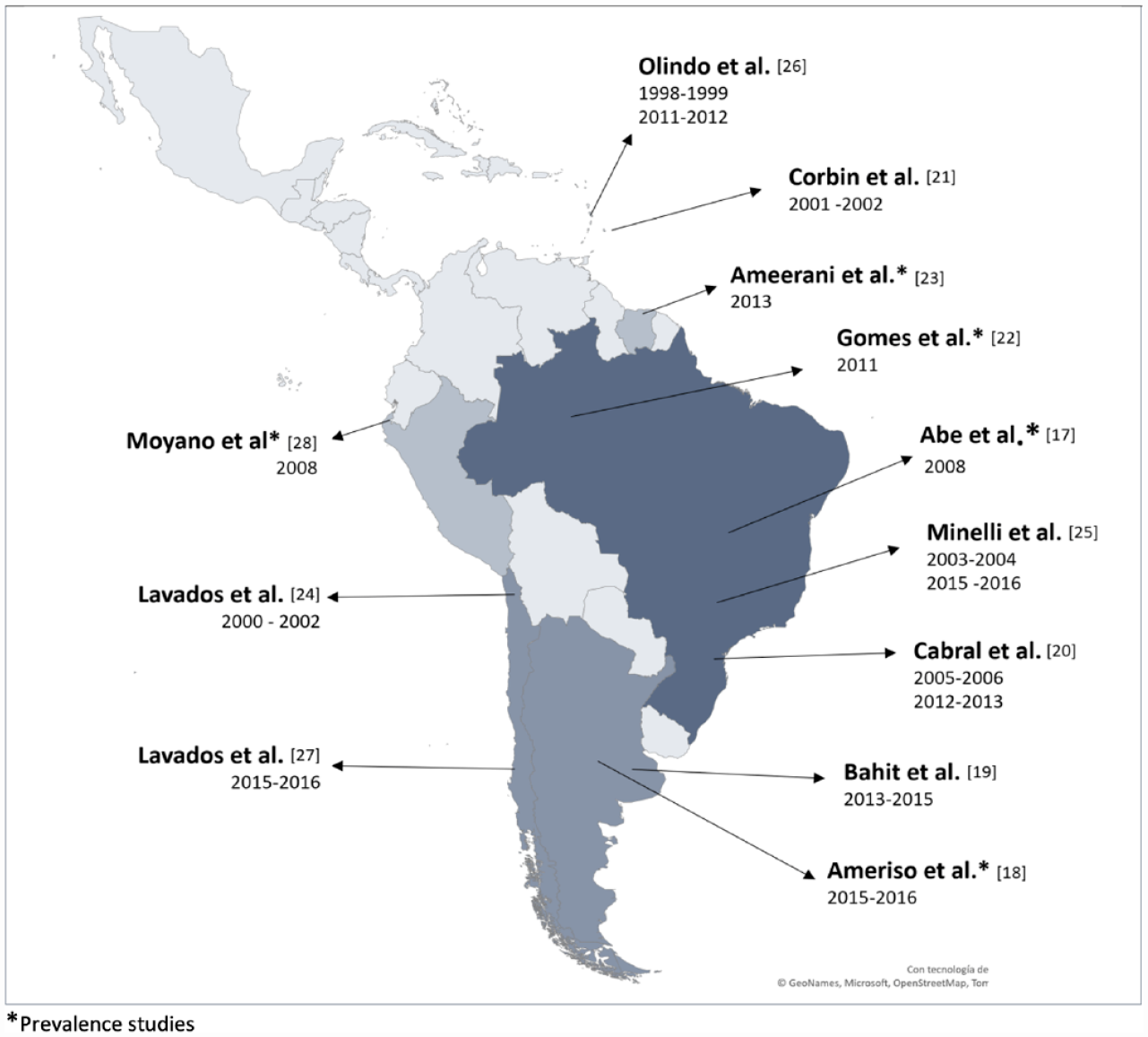
Location of studies assessing the incidence and prevalence of stroke in Latin America and the Caribbean.
The population denominator contemplated in the review was 4,405,227 inhabitants (mean = 293,681.8, SD = 343,974.2). All countries were classified as upper-middle income, except Chile 21 and Martinique 22 that were high-income countries according to the World Bank’s classification. 4 Information on the ethnic composition of the population could not be obtained.
Incidence reports
From seven articles that reported incidence, three of them reported two registration periods.18,19,22 Therefore, ten study periods were identified (Table 2). We identified a total number of 4835 patients with first-ever stroke in a sample of 4,369,876 persons, from which 2390 were women (49.8%). The mean age of the study periods that reported age data was 69.0 ± 3.5 years.16–18,20–22 Type of stroke was classified by computed tomography (CT) and/or magnetic resonance imaging (MRI). The mean of the percentage of brain images performed was 91.7% and ranged from 90% 21 to 99.4%. 22
Summary of the epidemiological data from study periods assessing the incidence in Latin America and the Caribbean.
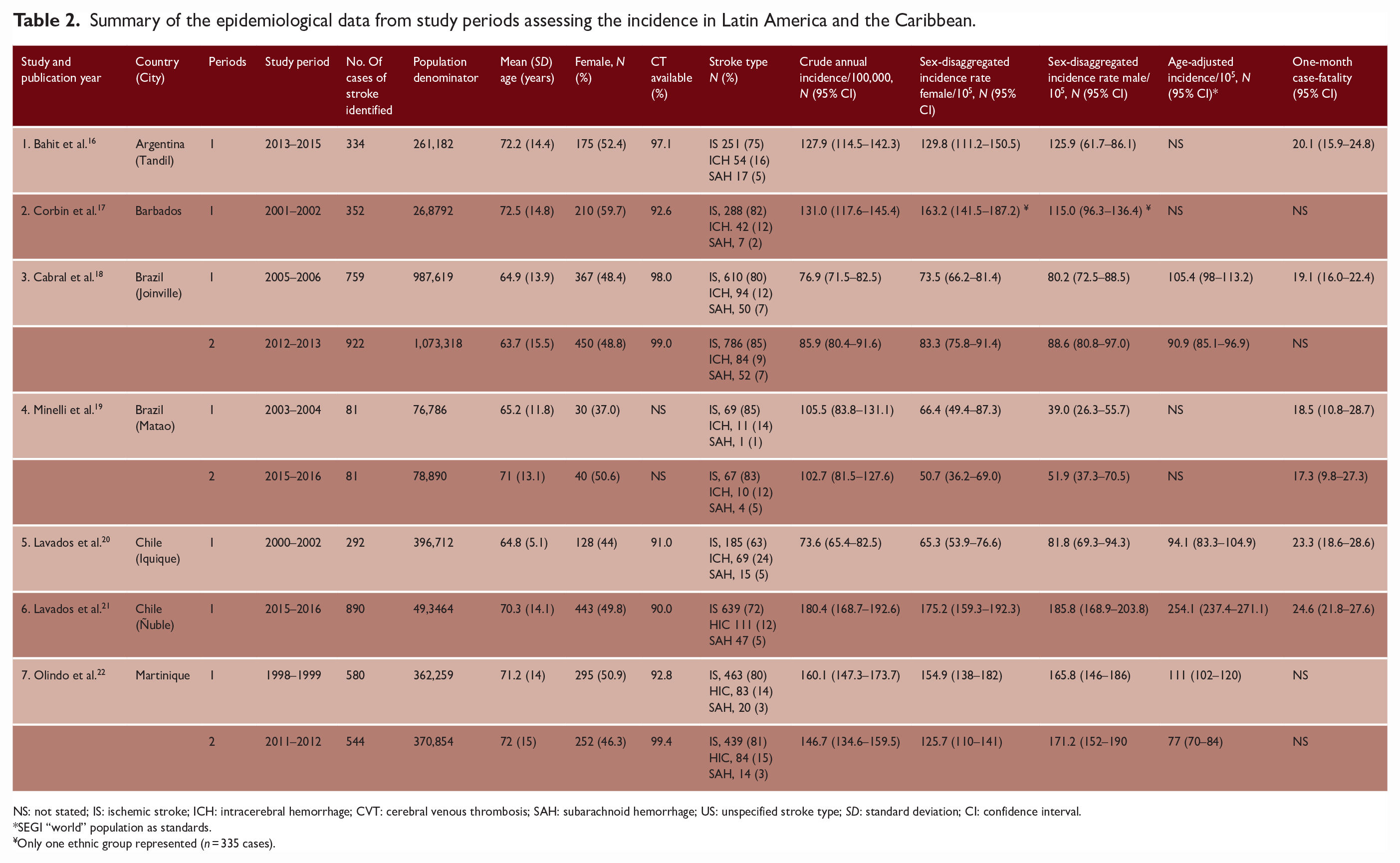
NS: not stated; IS: ischemic stroke; ICH: intracerebral hemorrhage; CVT: cerebral venous thrombosis; SAH: subarachnoid hemorrhage; US: unspecified stroke type; SD: standard deviation; CI: confidence interval.
SEGI “world” population as standards.
Only one ethnic group represented (n = 335 cases).
The crude annual incidence of first-ever stroke was heterogeneous, ranging from 73.6/100,000 20 to 180.4/100,000 21 people per year (Supplemental Figure S.1). The overall crude annual incidence of first-ever stroke in LAC was 119.0 (95% CI = 95.9–142.1)/100,000 people per year (Figure 3). High heterogeneity was observed (I2 = 98.1%). The age-adjusted incidence reported on the basis of Segi’s WORLD ranged from 77/100,000 in Martinique 22 to 254.1/100,000 in Ñuble, Chile. 21
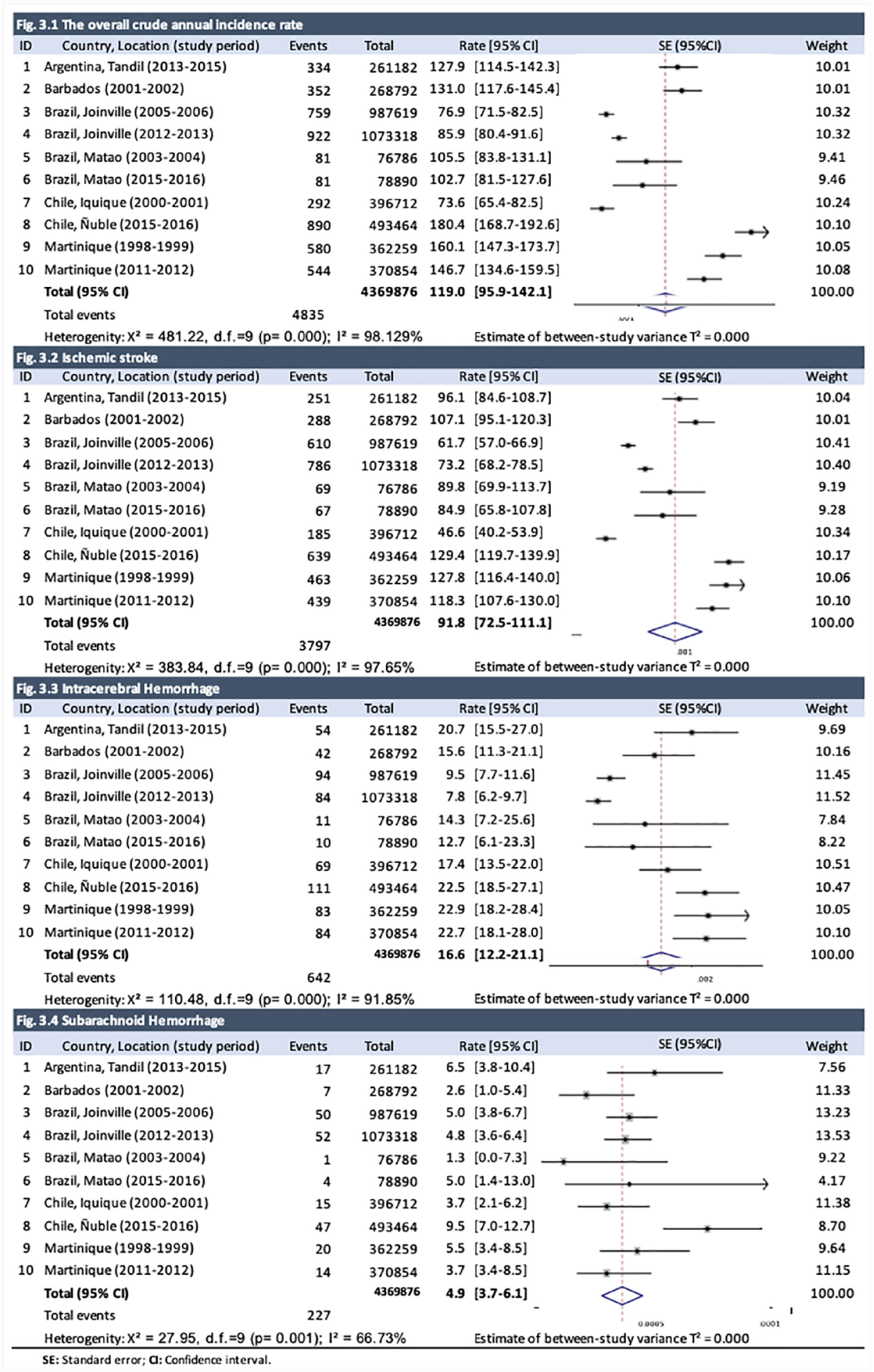
Overall crude annual incidence of first-ever stroke per 100,000 people in Latin America and the Caribbean and by stroke sub-group.
According to the stroke subtype, the crude annual incidence of first-ever IS ranged from 46.6 20 to 127.8/100,000 22 people per year, ICH rate ranged from 9.518 to 22.9/100,000 22 people per year, and SAH rate ranged from 1.3 19 to 9.5/100,000 21 people per year. High heterogeneity was observed in these analyses with I2 of 97.6%, 91.8%, and 66.7%, respectively. The LAC overall crude annual incidence was 91.8 (95% CI = 72.5–111.1)/100,000 people per year, 16.6 (95% CI = 12.2–21.1)/100,000 people per year and 4.9 (95% CI = 3.7–6.1)/100,000 people per year for IS, ICH, and SAH, respectively (Figure 3).
Regarding age groups, the crude annual incidence of first-ever stroke was 3.8 (2.8–4.9)/100,000 people per year in the 0- to 34-year-old group (I2 = 32.6), 33.8 (25.8–41.8)/100,000 people in the 35- to 44-year-old group (I2 = 62.8), 127.8 (101.6–154.0)/100,000 people in the 45- to 54-year-old group (I2 = 83.9), 252.8 (210.9–294.7)/100,000 people in the 55- to 64-year-old group (I2 = 81.9), 580.3 (504.6–656.0)/100,000 people in the 65- to 74-year-old group (I2 = 78.5) and 1202.3 (1007.4–1391.1)/100,000 people in the 75 years old or older group (I2 = 91.2) (Supplemental Figure S.2)
Prevalence reports
Five studies reported prevalence (Table 3).25,27 Of a total of 35,342 persons, 684 respondents were classified as stroke victims.
Summary of the epidemiological data from studies assessing the prevalence in Latin America and the Caribbean.
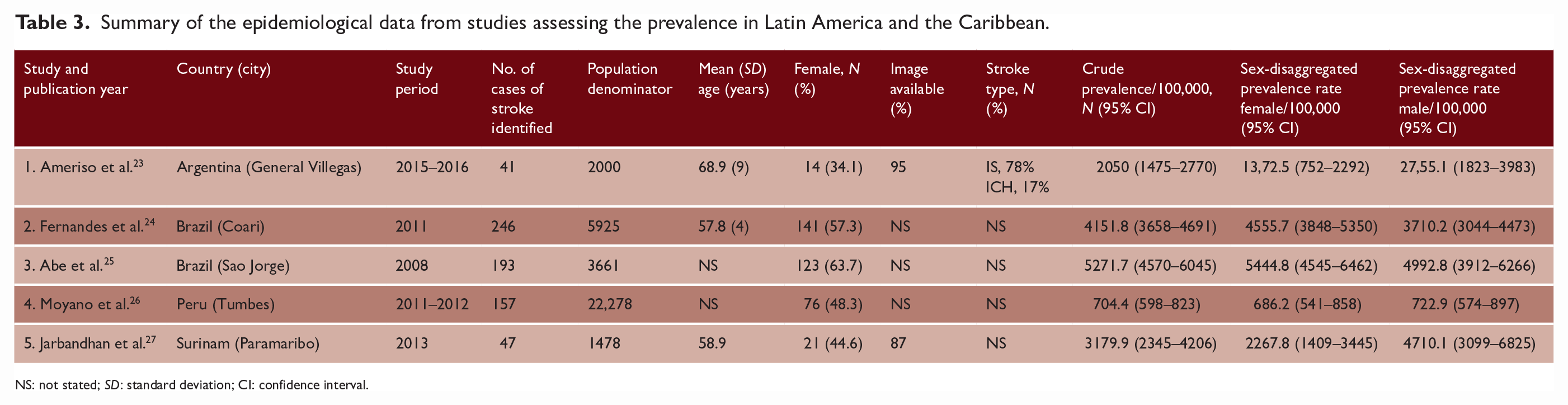
NS: not stated; SD: standard deviation; CI: confidence interval.
The crude prevalence ranged from 704.4/100,000 to 5271.7/100,000 people per year.25,26 High data heterogeneity was found (I2 = 98.8%). The overall LAC crude prevalence was 3060.1 (95% CI = 1090.6–5023.6)/100,000 people (Figure 4).
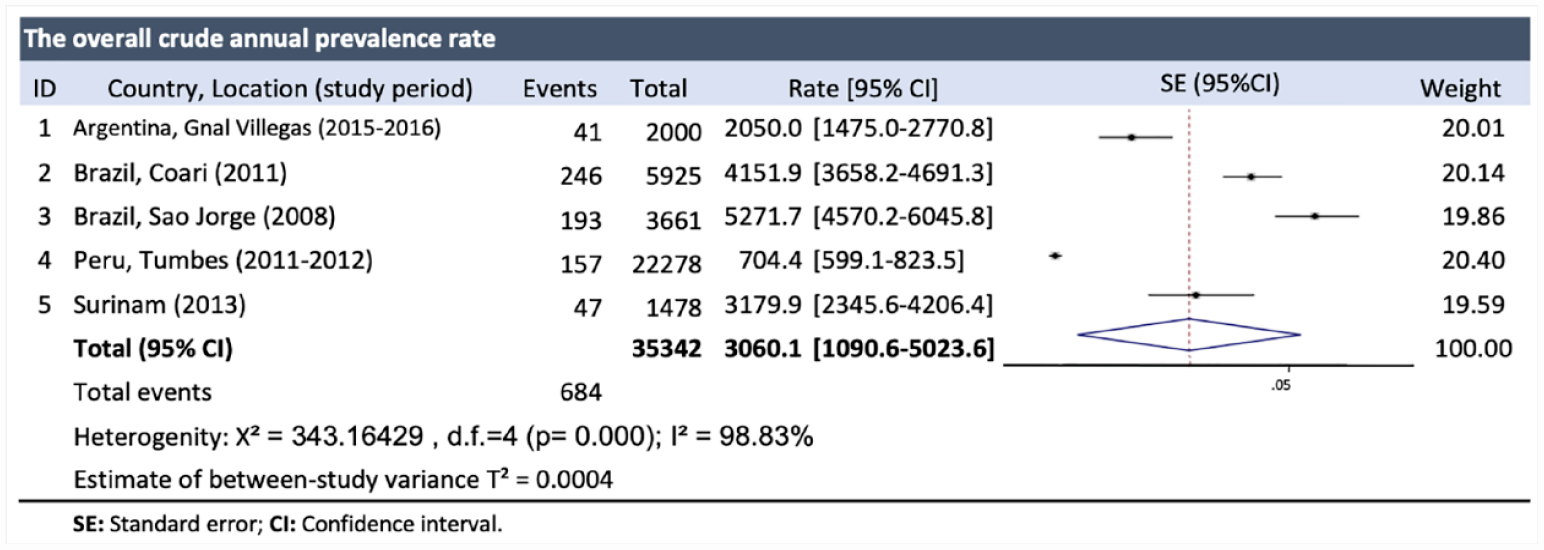
Overall crude prevalence per 100,000 people in Latin America and the Caribbean.
There was not enough information about stroke subtype prevalence.
One-month case-fatality reports
Six registry periods reported 1-month case-fatality.16,19–21 A moderate heterogeneity was observed between studies (I2 = 49.4%). The overall case-fatality at 1 month after the first stroke was 21.1% (95% CI = 18.6–23.7). The reported 1-month case-fatality ratio ranged from 17.3% (95% CI = 9.8–28.6) in Matao, Brazil 19 to 24.6% (95% CI = 21.9–27.6) in Ñuble 21 (Figure 5).
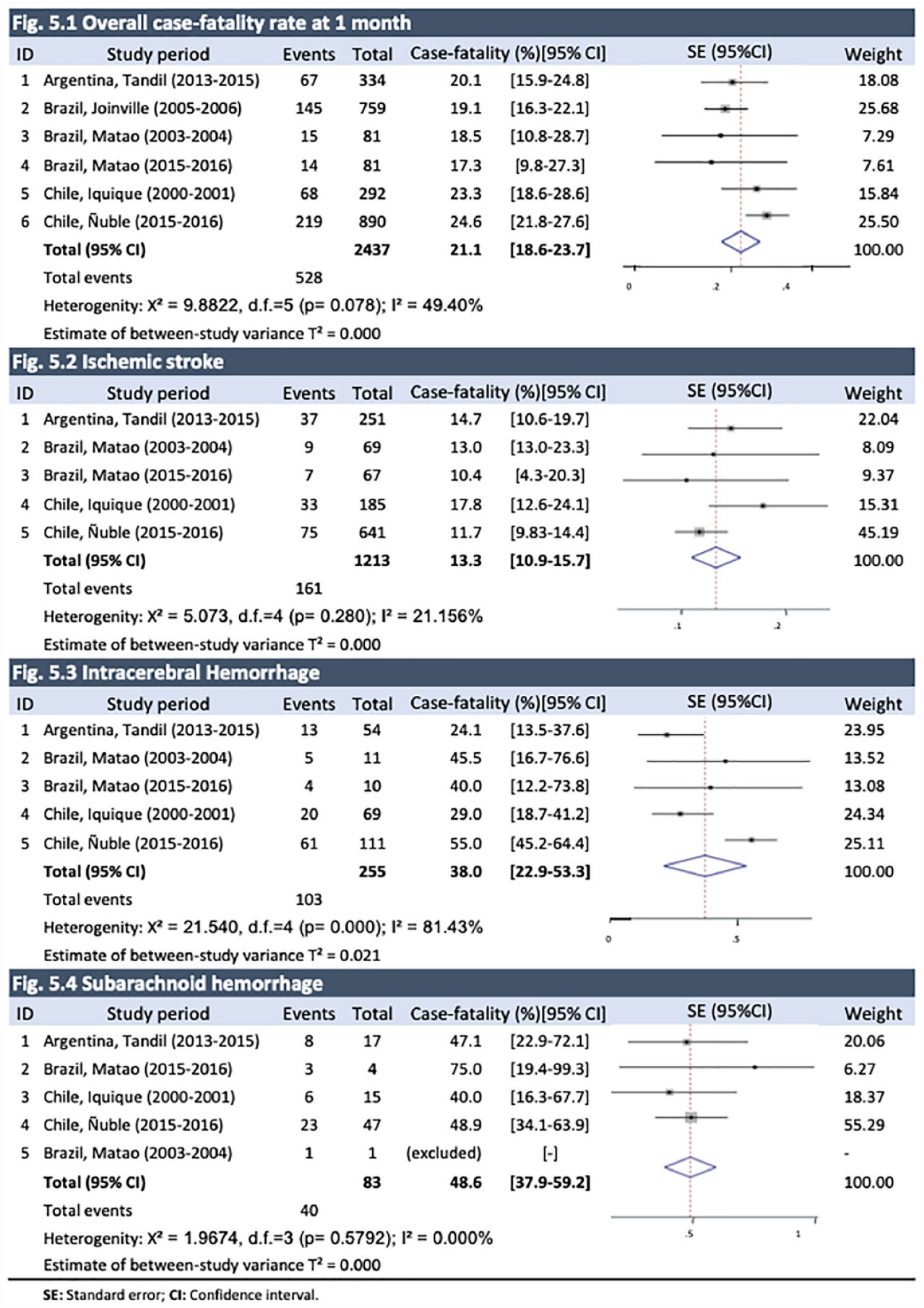
Overall case-fatality at 1 month after the first stroke in Latin America and the Caribbean and by stroke sub-group.
The overall 1-month case-fatality in IS was 13.3% (95% CI = 10.9–15.7) and for ICH 38.0% (95% CI = 22.9–53.3). SAH was the most fatal type of stroke, with an overall 1-month case-fatality of 48.6% (95% CI = 37.9–59.2) (Figure 5).
Risk of bias in studies
We used the JBI 28 Critical Appraisal Checklist for study reporting cohort and prevalence data to assess the 12 included studies that revealed incidence, case-fatality, and prevalence. The grade (yes, no, or unclear) is shown in Supplemental Table S.6. Most of the incidence studies indicated that statistical methods were adequate. Prevalence studies had insufficient coverage of the identified sample (Supplemental Table S.6).
Publication bias
Publication bias was ruled out with Egger’s test in incidence, prevalence and case-fatality studies. All results had a p-value > 0.05 (Supplemental Table S.7).
Discussion
In this article, we present a systematic review of the incidence, prevalence, and case-fatality of stroke for LAC. Limited epidemiological data were found, representing only seven of the 36 LAC countries. Nevertheless, the valuable information available was derived from high-quality studies, representing the leading countries in stroke burden research in the region, such as Brazil and Chile. These results are a first approximation of quality epidemiological parameters, although collaborative academic research efforts in LAC are a priority to improve the information in the region, as it has been previously suggested. 29
Large variation was detected in the stroke crude incidence rates in the region, ranging from 73.620 to 180.4/100,000, 21 with increasing rates in older age groups. Even though previous reports have considered LAC within the lowest stroke burden regions in the world, 30 this information contributes to evidencing wide differences between countries.
When the age-adjusted incidence was analyzed, the lowest values were found in Martinique (77/100,000) and the highest values were found in Ñuble, a region of southern Chile (254.1/100,000), being both high-income countries. The higher values for Ñuble, Chile may be related to the fact that the study was conducted in an underserved, low-income population in Chile with a high prevalence of cardiovascular and environmental risk factors. In addition, the design was a population-based study that captured all strokes, even the mildest. It is also possible that the incidence of IS is increasing due to the high prevalence of vascular risk factors in an aging population. 21 The evidenced large variation in age-adjusted stroke incidence between LAC countries is similar to what was previously informed by the global burden diseases (GBDs) for 2019, 1 but the recently reported increased incidence in one of the high-income countries of the region (Chile) is a concern that will require a careful oversight.
Regarding stroke prevalence, only five studies were found,23–27 reporting data with large variation. Figures ranged from 705/100,000 in Perú 26 to 5271.7/100,000 in Brazil. 25 All of them were cross-sectional studies, but they used different definitions and age groups, making comparisons difficult. Despite these limitations, the crude prevalence ranges in middle-income countries were in line to those reported by the GBD for LAC.31,32 Stroke experts and policy makers in Latin America have addressed the increase in stroke prevalence that has occurred in recent decades, 32 but more research on stroke prevention, incidence, prevalence, and outcomes is needed to obtain a better approximation of the impact of these estimates.
Overall case-fatality at 1 month after the first stroke of 21.1% was low compared to other regions of the world. 30 One-month case-fatality had low-moderate heterogeneity found across studies. This finding may reflect the degree of development and local resources of countries included in this study, since its values were similar to those reported by other studies that analyzed mainly high- and middle-income countries. 32
Strengths and limitations
One of the main strengths of this systematic review is that we covered the last three decades, which made possible to estimate epidemiological information over a long period. In addition, the study was mostly based on population-based research that met the criteria for an ideal stroke revision, 33 ensuring that the data were complete and comparable and provided the most precise estimates of incidence, prevalence, and early case-fatality of stroke.
Our study has some limitations. First, meta-analysis techniques were used in data with high heterogeneity. This was decided because the interpretation of heterogeneity in systematic reviews of prevalence and incidence is controversial, since it is expected to find clinical, methodological, and statistical heterogeneity when studying a large area and different populations. It has been argued that I2 may not be discriminative and should be interpreted with caution. 34 As most previous prevalence systematic reviews, we presented the results with ranges and also point estimates including prediction intervals for a correct interpretation. Second, restricting our analysis to published reports might have introduced publication bias; nevertheless, this bias is likely to be small because uncited publications may not be relevant given the strict methodology required to diagnose and report stroke studies. Finally, this analysis can be limited by the fact that the analyzed countries had upper-middle or high incomes, leaving other LAC countries underrepresented, 29 and because it is very difficult to compare countries in such a wide area with large differences even within countries over time in terms of income, level of education, access to health services, ethnicity, and sociocultural determinants.
Conclusion
In summary, the results of this review contribute to our understanding regarding the burden caused by stroke in LAC. More studies with comparable designs are needed to generate reliable data and should include both standardized criteria, such as the World Health Organization 33 clinical criteria and updated standard methods of case assurance, data collection, and reporting. 35 More research is required in middle-low- or low-income populations in LAC, given their low representation. This information should be examined further to determine whether gender differences exist in these populations.
Supplemental Material
sj-docx-1-wso-10.1177_17474930221143323 – Supplemental material for Stroke in Latin America: Systematic review of incidence, prevalence, and case-fatality in 1997–2021
Supplemental material, sj-docx-1-wso-10.1177_17474930221143323 for Stroke in Latin America: Systematic review of incidence, prevalence, and case-fatality in 1997–2021 by Carlos Delfino, Marilaura Nuñez, Claudia Asenjo-Lobos, Francisca Gonzalez, Amy Riviotta, Francisca Urrutia, Pablo Lavados, Craig S. Anderson and Paula Muñoz Venturelli in International Journal of Stroke
Footnotes
Acknowledgements
The authors acknowledge Mr Gabriel Cavada for his statistical support.
Data accessibility statement
The data that support the findings of this study are available from the corresponding author (P.M.) upon reasonable request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PMV receives research grants from ANID Fondecyt Regular 1221837. PML reports research support from Clínica Alemana de Santiago and Boehringer Ingelheim, research grants from The George Institute and Clínica Alemana de Santiago. ANID FONDECYT and FONIS. Speakers’ honoraria from Boehringer Ingelheim. Steering Committee honoraria form Bristol-Meyes-Squibb. The other authors declare no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.