
Abstract
Background:
The adoption of direct oral anticoagulants (DOACs) has changed practice in prevention of stroke in atrial fibrillation (AF). We used Irish data national data on stroke and anticoagulation therapy over 9 years to investigate changes in anticoagulation practice and potential consequences on stroke prevalence and thrombolysis.
Methods:
AF, anticoagulation, thrombolysis, and stroke data from the Irish National Audit of Stroke (INAS) 2013–2021 were reviewed. The proportion of patients with ischemic stroke (IS) and intracerebral hemorrhage (IH) with known AF admitted on anticoagulation was determined. Effects on age distribution in the population and thrombolysis practice were assessed.
Results:
AF data were available on 34,630 of 35,241 individuals (98.3%) included in INAS; median age was 74 years and 56% were male. AF was found in 10,016 (28.9%, 9059 IS, 957 IH). 6313 had known AF prior to stroke (63.1%). The proportion all total IS due to AF decreased by 15.3% (31.3%−26.5%, chi-square = 24.6, p < 0.0001). The proportion of IH did not change significantly (21.6%–20.2%, chi-square = 1.8, p = 0.18). Over the 9 years, 3875 (38.6%) of the subjects with AF were recorded as receiving anticoagulants at admission. In 2013, 4.4% of AF-associated strokes were admitted on a DOAC and 21.4% on warfarin; by 2021, 44.1% were receiving a DOAC and 6.2% warfarin. There was a strong inverse correlation between the proportion of anticoagulated stroke patients and the total proportion of AF-associated strokes over time (r = −0.82, p = 0.006). In contrast, no correlation was found between increasing DOAC usage and IH (r = 0.14, p = 0.71). Increased anticoagulation usage correlated with a reduction in patients ⩾ 80 years (r = −0.83, p = 0.006) and also correlated with a relative reduction of 30.1% in subjects thrombolysed <4 h from onset (r = −0.89, p = 0.001)
Conclusion:
DOACs have led to increased use of anticoagulation, but warfarin use fell by two-thirds. There has been a reduction in the proportion of AF-associated IS without a noticeable increase in IH. Increased anticoagulation correlated with reduced numbers of strokes in those >80 years and in the proportion of patients thrombolysed.
Introduction
Untreated atrial fibrillation (AF) is a major cause of cardioembolism and consequent ischemic stroke (IS).1,2 The Irish National Stroke Register, later incorporated into the National Office of Clinical Audit as the Irish National Audit of Stroke (INAS), was established in 2012 to collect data as to the performance of Irish Stroke Services and to identify areas of weakness in inpatient stroke care in Irish Hospitals. 3 The original INAS data set was developed taking regard of the then recently published North Dublin Population Stroke Study (NDPSS). 4 This found a 31.3% incidence of AF-associated stroke and 21.2% incidence of warfarin-associated intracerebral hemorrhage (IH) in the cohort. Accordingly, data on pre-existent AF and antithrombotic therapy were included in the data set and have been included since then in addition to data on previously unrecognized AF identified during the inpatient stay.
The period covered by the audit corresponds to an increase in adoption and use of direct oral anticoagulants (DOACs) in the primary and secondary prevention of stroke in subjects with AF following granting of European licenses. A prior study predominantly of routinely collected Irish inpatient and prescribing data from 2010 to 20185 showed that there was a large increase in the national expenditure on DOACs and thus prescribing rate over the period but no associated change in AF-associated stroke. We performed an analysis of INAS data to determine any changes in prevalence of AF-associated stroke over the 9 years 2013–2021 and to identify apparent changes antithrombotic prescribing practices over the period.
Methods
Data were analyzed from the INAS data set. INAS data were collected by stroke services in each hospital in Ireland admitting more than 25 patients/year.6,7 Data are then validated against routinely collected hospital activity data the Hospital In-Patient Enquiry (HIPE) to ensure that patients admitted with stroke that do not come under the care of stroke services, for example, those admitted under Neurosurgery, Intensive care, or Internal Medicine services are included in the data set. Data are included if there is >80% agreement between HIPE and INAS in identifying acute stroke patients. Data are stored on a central server with local services able to review their own data and summary reports are published annually. With the progressive development of the audit, a greater number of cases have been identified and a greater number of hospitals included in the audit. 7 Because of the increasing number of centers involved and the consequent increasing number of individual cases, proportional data were compared for the 9 years of the audit. All data analyzed is anonymized and data sets of ⩽5 individuals are not included to reduce chances of inadvertent identification. Data are collected for IS and primary IH but not subarachnoid hemorrhage (SAH) as pathways for SAH management in Ireland differ substantially from that for other stroke types. Data for subdural hemorrhages are not collected as these fall outside standard definition of stroke. Permission for analyses is given by the Governance committee of INAS as part of the process of the audit, and while institutional ethics review is not required for data used for this purpose, ethics review by our institutional committee was requested and approval granted.
Data were analyzed using proprietary software. In addition to descriptive data, chi-square analyses were performed to compare relative proportions and Pearson’s correlations to compare continuous variables. Because of the relatively small number of data points and level of variance, regression analysis was not performed. 8 Data used in this study are publicly available and can be requested from the National Office for Clinical Audit, St. Stephen’s Green Dublin. A data access request for is available from their website www.noca.ie.
Results
Over the 9 years, data on 35,241 stroke events were collected of whom AF data were available on 34,630 (98.3%). Median age of the population over the period was 74 years (interquartile range (IQR) = 65–82 years) and 56% were male. Numbers of patients identified by the audit increased from 2790 in 2013 to 5239 in 2021 (Table 1). This 2021 value represented 90.5% of potential stroke cases identified by HIPE. Number of participating hospitals increased from 9 in 2013 to 24 in 2021. Proportion of stroke in the oldest age group ⩾80 years declined from 36.2% to 33.3% over the period (relative reduction 8%) and the proportion of those <65 years in turn increased by the same absolute value (23.9%–26.8%) (Table 1). Proportion of stroke in women declined significantly over the period from 46.4% in 2013 to 42.6% in 2021 (chi-square = 10.65, p = 0.001).
Stroke numbers and age distribution collected as part of the Irish National audit of stroke (INAS) database by year 2013–2021 inclusive.
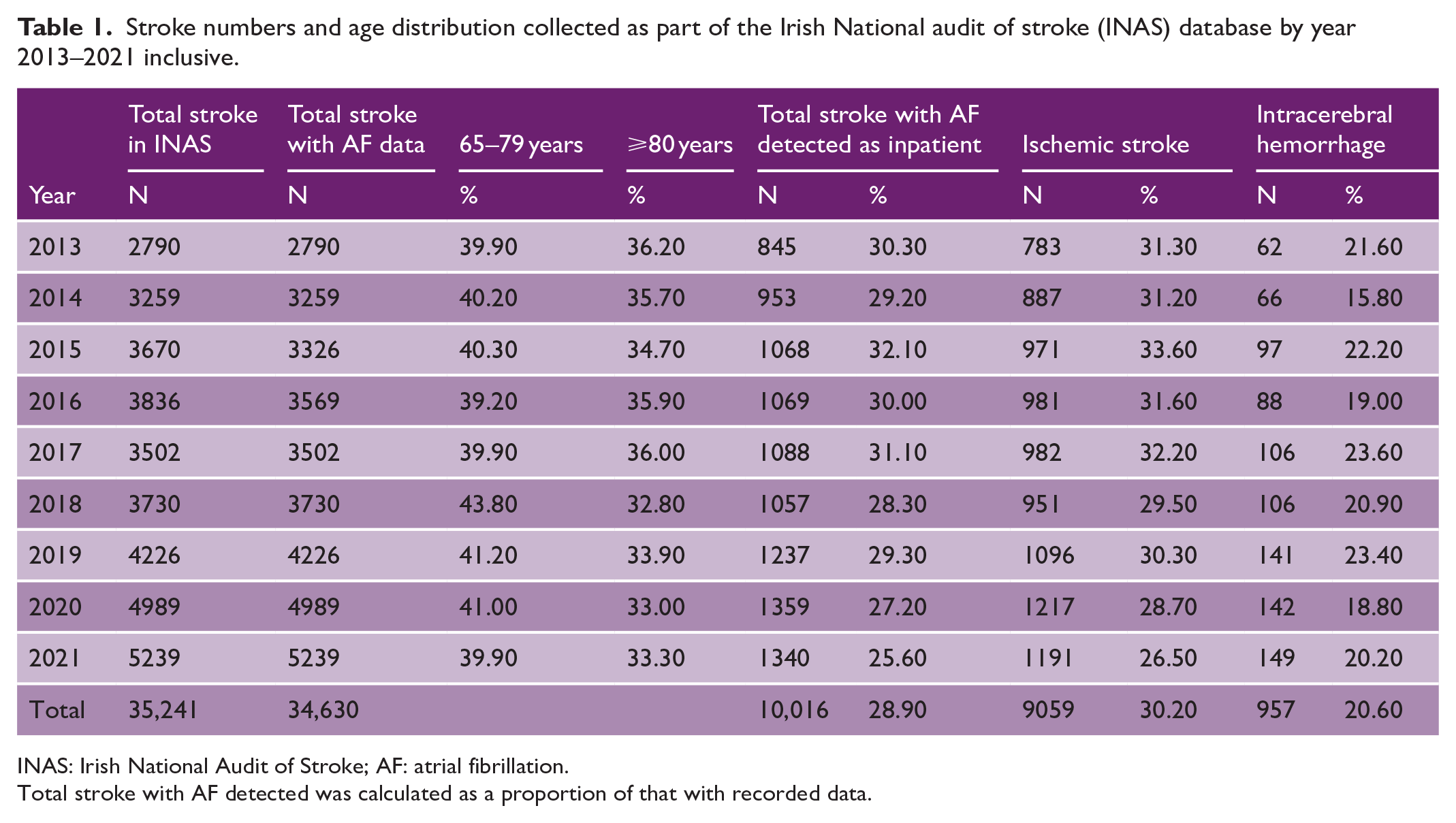
INAS: Irish National Audit of Stroke; AF: atrial fibrillation.
Total stroke with AF detected was calculated as a proportion of that with recorded data.
Over the 9-year period, AF was found in 10,016 cases (9059 IS, 957 IH) representing 28.9% of all admissions. Of these, 6313 had known AF before admission (63.1%). There was a significant decrease in the proportion of patients admitted in AF between 2013 (31.3%) and 2021 (26.5%) (15.3% relative reduction, chi-square = 24.6, p < 0.0001). This decline was almost entirely due to a reduction in the proportion of ISs in AF. The proportion of hemorrhagic strokes dropped only slightly and non-significantly over the time period (21.6%–20.2%, chi-square = 1.8, p = 0.18).
Of the 10,016 AF cases, 3875 (38.6%) were already prescribed anticoagulant therapy on admission. This proportion increased steadily (Table 2) over the 9-year period. A further 1197 were prescribed antiplatelet therapy (12.0%). Only 89 (0.89%) subjects were receiving dual antiplatelet and anticoagulant therapy on admission.
Characteristics of anticoagulation and thrombolysis therapy in patients with known AF admitted 2013–2021.
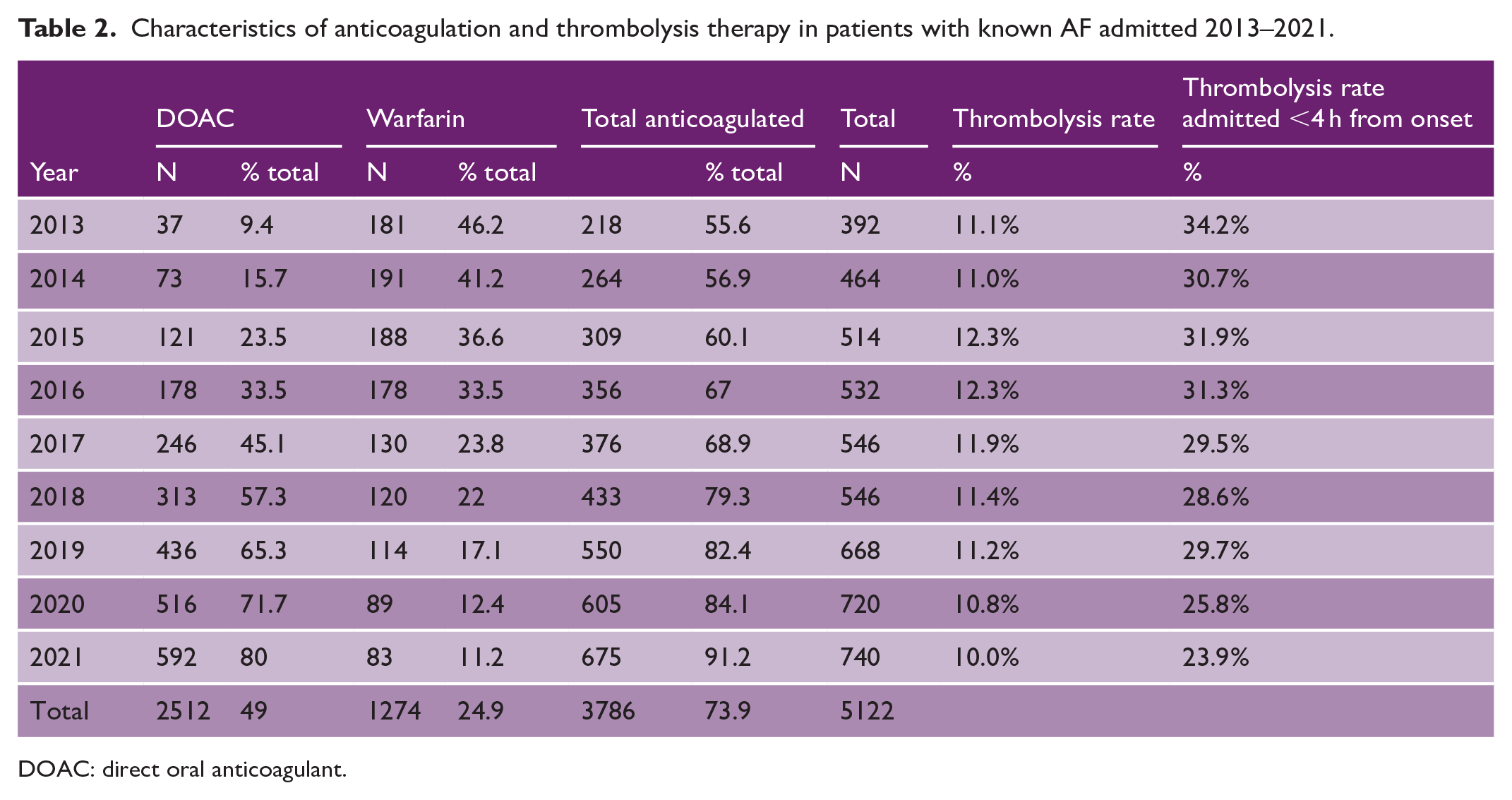
DOAC: direct oral anticoagulant.
In 2021, 66.9% of patients found to be in AF had the diagnosis before admission. 81.1% of these subjects with known AF were anticoagulated equating to 50.4% of all individuals with AF receiving anticoagulation and a further 3.4% on an antiplatelet. Anticoagulation practice changed significantly over the 9-year period. In 2013, 4.4% of AF-associated strokes were admitted on a DOAC compared with 21.4% on warfarin. By 2021, 44.1% of AF-associated strokes were admitted on a DOAC and 6.2% on warfarin.
There was a strong negative correlation found between proportion of stroke patients admitted receiving anticoagulation and the proportion of AF-associated strokes of total strokes (r = −0.82, p = 0.006 Pearson’s correlation) (Figure 1(a)). There was no significant correlation found between DOAC usage and IH (r = 0.14, p = 0.71) (Figure 1(b)). Change in proportion of patients ⩾80 years admitted over the 9 years correlated strongly with measures of anticoagulation prevalence including proportion of patients with known AF (r = −0.83, p = 0.006) and proportion of stroke ultimately found to be in AF (r = −0.77, p = 0.015) who were already anticoagulated on admission.
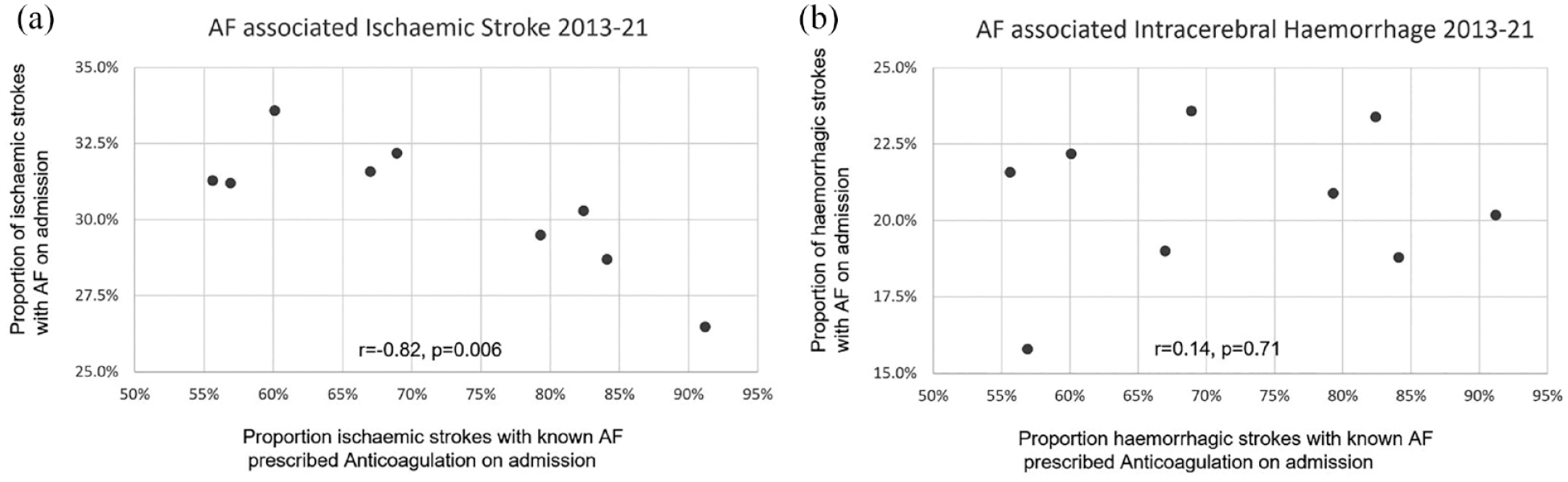
(a) Correlation between proportion of subjects with ischemic stroke admitted with known AF who were receiving anticoagulation pre-stroke with proportion of AF-associated ischemic strokes of total ischemic stroke admissions. Correlation between proportion of subjects admitted with intracerebral hemorrhage admitted with known AF on anticoagulation with proportion of AF-associated intracerebral hemorrhage of total admitted with intracerebral hemorrhage.
There was also a strong negative correlation found with data on thrombolysis rate. Thrombolysis rate of subjects with IS admitted within 4 h declined from 34.2% in 2013 to 23.9% in 2021, a 30.1% relative drop. Rate of thrombolysis <4 h correlated very strongly negatively with measures of anticoagulation use. Known AF receiving anticoagulation on admission (r = −0.89, p = 0.001), all AF receiving anticoagulation on admission (r = −0.88, p = 0.001) (Table 2). There are two interventional neuroradiology–led thrombectomy services in Ireland. Thrombectomy data have only been routinely collected by INAS since 2016 and numbers increased from 157 to 422 (269%) over that period which may also have affected the thrombolysis rate.
Discussion
The proportion of patients admitted with AF-associated stroke who have been prescribed anticoagulation prior to stroke has increased very significantly over the 9 years of the study. 2021 was the first year where more than half of all patients admitted with AF-associated stroke were already prescribed anticoagulation prior to admission. Over the period, the proportion of stroke patients admitted in AF has reduced significantly and this correlated strongly with the proportion of subjects with established anticoagulation on admission, which likely reflects increased population levels of anticoagulation. The proportion of IHs in anticoagulated subjects has not increased. The increase in the prevalence of anticoagulation in the stroke patients with AF correlated strongly with the decrease in proportion of subjects ⩾80 years and the decrease in the proportion of patients with IS presenting within 4 h of symptom onset.
The study has some limitations. The data were collected as part of a national audit process, rather than as an observational study. The purpose of data collection is to monitor and improve patient care and seeks to collect data on all subjects; thus, the population study may be more representative than in an observational study where consent for some patients may be unavailable. However, the context of an audit means that data on all potential cofactors of interest are not collected for both ethical and resource reasons. Data collection in this context is not formally consented, and the purpose for each data item must be justified in terms of quality improvement or monitoring performance. INAS does not routinely collect data on subarachnoid hemorrhages as the care pathway and guidelines for management for these in Ireland differ from other strokes. Triage and care of these patients are often organized between Emergency Departments and Neurosurgical services, and the data are not available to stroke services for collection.
Data were analyzed as proportions as recruitment to the audit has become more complete over the decade and overall numbers of patients have increased. We feel that the data from the earlier years are representative as it is consistent with the largest population study performed in the country, the NDPSS 4 that was completed just before the inception of the audit. Furthermore, the data submitted by the relevant stroke screens is validated against routinely collected activity and coding data from the hospitals often using a reconciliation process to confirm it and the data are collected predominantly by Clinical Nurse Specialists working in Stroke services. However, the number of hospitals evaluated, although admitting >90% of hospitalized strokes in the country, were comparatively small for statistical purposes; thus, only strong correlations were found to be significant at conventional levels and type I error is a risk. Similarly, the group sizes were too small to satisfactorily conduct regression analysis because of population variance. 8 Confirmation would require similar studies be performed in a larger group of hospitals, which in the case of Ireland, would mean inclusion of a second country.
Collection of data on anticoagulation status of Irish patients admitted with AF-associated stroke began at the initiation of the National Stroke Register in 2013. This was soon after the granting of licenses for three of these agents for this indication by the European Medicines Agency 9 (dabigatran and rivaroxaban 2011, apixaban 2012) and before edoxaban received permission in 2015. The majority of patients receiving these drugs are eligible for some financial support from the Irish state and the expenditure over the period increased nearly 12-fold between from €5.3 million in 2010 to €63 million in 2020. 5 It is notable that while the proportion of those admissions prescribed DOACs increased by >850% over our study period, the proportion prescribed warfarin reduced by >75%, despite the European Guidelines not recommending DOAC above warfarin until 201610 and the UK and Irish stroke guidelines only recently mandating DOAC above warfarin in 2023. 11 This represents a very substantial change in practice. In comparison, a recent US study of over 400,000 individuals found more modest increases in anticoagulation 2011–2020 a non-stroke, community study with rates rising from 56.3% to 64.7% and a smaller reduction in use of vitamin K antagonists. 12 Ireland does not collect data on national anticoagulant prescribing specifically for AF, but we feel that the increasing proportion of subjects admitted with known AF receiving anticoagulation is a good proxy for this. The significant drop in the proportion of women admitted with stroke over the period may also be related to the change from vitamin K antagonist to DOAC therapy. A recent study from Scotland, a neighboring country with similar population characteristics, showed that women with non-valvular AF were significantly less likely to be prescribed vitamin K antagonists, but this disparity was less following the wider introduction of DOACs. 13 A similar change in Ireland may explain the significant drop in the proportion of strokes in women.
In a previous analysis primarily of HIPE data until 2018, 5 we found no significant reduction in AF-associated stroke despite a large increase in the proportion anticoagulated. It is reassuring that we have now found a small but significant decrease in the proportion of AF-associated strokes consistent with the published trial data14–17 without an increase in rate of hemorrhagic stroke. This supports the finding of the Averroes study 18 that showed no difference in risk of hemorrhagic stroke between subjects receiving apixaban and aspirin for AF. The NDPSS, 4 carried out before the DOACs were introduced, showed an association between anticoagulation with warfarin and hemorrhagic stroke and any slightly increased risk of IH that may be associated with the increase in DOAC prescribing may have been offset by the transfer away from warfarin. 19
The apparent reduction in proportion of stroke in people 80 years and over, and the strong correlation with indices of anticoagulation use is notable. AF is a condition associated with increasing age 20 and increasing age is also associated with increased risk of cardioembolism. 21 It is therefore perhaps unsurprising that the incidence of stroke in this population appears to have declined associated with the relatively rapid adoption of DOACs as a safer form of anticoagulation. The corollary, however, is that the proportion of strokes at younger ages seems to have increased in proportion to the reduction in older people. This is particularly the case in patients <65 years where AF-associated stroke is proportionally much less frequent.
Likewise, anticoagulation with DOAC is currently a contraindication to thrombolysis therapy in stroke, and unlike in warfarin, there is no current easy means of determining if the anticoagulation level is subtherapeutic to permit use of thrombolysis. The strong correlation between the increased use of DOAC and the decreased rate of thrombolysis in stroke patients presenting to hospital within a typical treatment window is thus perhaps unsurprising and additional research studying the safety of thrombolysis in subjects receiving DOACs would be valuable. 22
While it is encouraging that the great majority of subjects who had been recognized as having AF pre-stroke were anticoagulated it is of concern that so many had unrecognized AF when they suffered their stroke. This adds an increased impetus for considering the efficacy of screening for AF in at risk groups. 23 This has previously been shown likely to be effective in the Irish context24,25 with a large, remote, older rural population. In terms of generalizability of our findings, recent data rates of pre-stroke anticoagulation are not easily identified, reviews carried out for the Stroke Alliance for Europe 26 showed that Irish anticoagulation practice pre- and post-stroke was typical of other European countries as was other secondary prevention practice. 27 In recent surveys of practice, rates of thrombolysis and thrombectomy identified by the INAS28,29 were similar to those of other Western European countries. Although it is recognized that anticoagulation can only prevent a proportion of stroke, INAS is currently undertaking a more in-depth study looking a patients admitted with stroke while anticoagulated to determine whether practice change may improve the effectiveness of the intervention. The data collected by INAS is for hospitalized strokes, which are thought to represent >90% of strokes occurring in the country. 4
In conclusion, the introduction of the DOACS has been associated with a large increase in the proportion of subjects anticoagulated pre-stroke. We have also noticed a reduction in the proportion of strokes that are AF associated. This has not been associated with an increase in the proportion of hemorrhagic stroke.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was conducted by staff of the Irish National Audit of Stroke. There were no external funding organizations.