
Abstract
Background:
Chronic ischemic lesions (CILs) are frequent findings in patients with acute ischemic stroke, but their phenotypes and relevance in young adults with embolic stroke of undetermined source (Y-ESUS) remains uncertain. We aimed to compare Y-ESUS patients with CIL to those without CIL and assessed the association of CIL and its phenotypes with the presence of patent foramen ovale (PFO).
Methods:
This prospective longitudinal, multicenter cohort study enrolled consecutive patients 50 years and younger with ESUS from October 2017 to October 2019 in 41 stroke research centers in 13 countries. Local investigators adjudicated presence and phenotypes of CIL on routine brain imaging (either magnetic resonance imaging (MRI) or computed tomography (CT)).
Results:
Overall, 535 patients were enrolled (mean age = 40.4 (standard deviation (SD) = 7.3) years, 238 (44%) female). CILs were present in 76/534 (14.2%) patients with a median count CIL count of 1.0 (interquartile range (IQR) = 1–2), 42/76 (55%) had at least one cortical phenotype and 38/76 (50%) at least one non-cortical phenotype. Y-ESUS with CIL were less often female (32% vs 47% in non-CIL Y-ESUS), were older (mean 43 vs 40 years), had more often hypertension (42% vs 19%), diabetes (17% vs 7%), and hyperlipidemia (34% vs 18%). CIL Y-ESUS were independently associated with lower stroke recurrence (relative risk (RR) = 0.17 (0.05–0.61)). In Y-ESUS with PFO, CILs were less frequent in probable pathogenic PFO than with probable non-pathogenic PFO (6.1% vs 30% p< 0.001).
Conclusion:
One in seven Y-ESUS patients has additional CIL. CILs were associated with several vascular risk factors, lower probability of a pathogenic PFO, and lower stroke recurrence.
Introduction
Among older patients suffering first-ever ischemic stroke, those with additional chronic ischemic brain lesions (CILs) have been shown to represent a high-risk vascular subgroup. 1 Given diverging temporal trends in stroke incidence with less favorable trends at younger ages, there is an urgent need to better understand the etiology and prevention of stroke at younger ages. 2 In the “Longitudinal young adults with embolic stroke of undetermined source” (Y-ESUS) study, 14% had additional CIL. 3 The clinical relevance of this imaging biomarker in this patient population has not been clarified.
According to the Risk of Paradoxical Embolism (RoPE) Study database, evidence of a prior stroke on baseline imaging was associated with the absence of PFO in cryptogenic stroke patients. 4 However, the mean age of the RoPE cohort was around 15 years older than in the Y-ESUS cohort, 3 and phenotypes of CIL (cortical vs non-cortical) as well as the anatomical location were not specified. 4 We hypothesized that Y-ESUS patients with a CIL (especially non-cortical) are less likely to have a PFO on work-up and that those with CIL would less likely have PFO-associated stroke.
Therefore, we analyzed the Y-ESUS database to describe frequencies and phenotypes of CIL in Y-ESUS and to characterize the subgroup of Y-ESUS with additional CIL in terms of age and the vascular risk profile. Furthermore, we aimed to assess the association of PFO with the presence of any CIL as well as phenotypes (cortical vs non-cortical localization) of CIL in Y-ESUS.
Materials and methods
Patients
Details on the study methodology have been deposited at https://clinicaltrials.gov/ (Unique Identifier NCT03185520) and have been published previously. 3 Briefly, this is a longitudinal, multicenter cohort study with enrollment from October 2017 to October 2019 in 41 stroke centers in 13 countries and a mean follow-up period of 12 months ending in October 2020. Patients were eligible if they had an imaging-confirmed diagnosis of ESUS, were 50 years or younger, had given written informed consent, and had no specific cause of the ischemic stroke identified according to the defined ESUS criteria. 5 Exclusion criteria included a close affiliation with the investigational site, and enrollment in an investigational study on ESUS.
Neuroimaging
Local investigators adjudicated presence and total count of CIL on a standardized electronic case report form on clinically acquired brain imaging (either magnetic resonance imaging (MRI) or computed tomography (CT)). Those were defined as radiologically unambiguous chronic brain infarction.6,7 The presence of CIL was adjudicated regardless of a medical history of stroke.
CILs were mapped in the following anatomical locations: right hemisphere, left hemisphere, brainstem, and cerebellar hemispheres. Supratentorial CILs were classified into cortical, subcortical, or uncertain phenotype, whereas infratentorial CILs were classified according to the structures involved (midbrain, pons, medulla, right cerebellar hemisphere, left cerebellar hemisphere, midline cerebellar location). Information on unspecific white matter hyperintensities was not collected. We classified the CIL into a cortical or non-cortical phenotype. A cortical phenotype was defined as having CIL in a cortical supratentorial area or in a cerebellar hemisphere and the non-cortical phenotype was defined as having CIL in a subcortical supratentorial area or in the brainstem. In some patients, raters were unable to adjudicate whether there was cortical involvement and those are labeled as uncertain phenotype.
Clinical baseline and follow-up data collection
The acquisition of data on baseline imaging, acute treatment, clinical presentation, and secondary prevention has been reported previously. During data collection, attempts were made to minimize missing data. In this study, a complete case analysis was conducted. Clinical outcome events were collected at 12 months or at the end of study.
Outcomes
The main outcomes were (1) the presence of any CIL, (2) the presence of cortical CIL and anatomical distributions of CILs, (3) recurrence of stroke within 12 months after the index stroke, and (4) the presence of any PFO and pathogenic PFO.
PFO analysis
For the subanalysis on the association of CIL and PFO, we restricted the analysis to those patients who had site-specific adequate work-up for PFO: either transesophageal echocardiography (here, use of color Doppler was sufficient to rule-in PFO) or transthoracic echocardiography with a bubble test and Valsalva maneuver. We compared differences between patients with and without CIL regarding the overall PFO presence (chi-square test), RoPE Score 8 (Wilcoxon rank sum test) as well as the PFO-Associated Stroke Causal Likelihood (PASCAL) Classification System (chi-square test).9,10 This PASCAL classification categorizes patients into three groups (unlikely, possible, and probable) based on the likelihood of a causal relationship between their PFO and stroke. This system combines the RoPE Score with the presence of high-risk PFO features, such as an atrial septal aneurysm or a large-sized shunt.
Statistical analysis
Baseline demographic and clinical characteristics were compared between Y-ESUS with CIL and without CIL, between patients with cortical CIL and non-cortical CIL and between Y-ESUS with PFO and without PFO using a t-test for normally distributed continuous variables, Wilcoxon rank sum test for continuous variables with skewed distribution, and a chi-square test or Fishers’ exact test for categorical variables. The same statistical method for categorical variables was used to compare the occurrence of CIL and cortical CIL between Y-ESUS who had PFO and those who did not have PFO and between patients with unlikely, possible and probable PFO-related stroke. To examine the association of recurrence of ischemic stroke and the presence of CIL, an unadjusted and adjusted Poisson regression models with robust error variance were used, 3 and relative risk (RR) and 95% confidence intervals and p-values were reported. For the multivariable model, covariates were history of stroke or transient ischemic attack, diabetes, and cardiac arrest, which were the predictors that were significantly associated with recurrent stroke in the previous Y-ESUS publication. 3 To examine the association of presence of PFO with the presence of CIL, an unadjusted and adjusted logistic regression models were used and odds ratio (OR) and associated 95% confidence intervals and p-values were reported. The adjusted model included body mass index (BMI), sex, history of hypertension, history of diabetes and whether the patient was current smoker as covariates reflecting the factors of the RoPE Score. All analyses were conducted in SAS, version 9.4
Ethics
Participants provided written informed consent and the study was approved from institutional review boards at each participating site.
Data availability
Data of this study will be shared if a reasonable request and data analysis plan is sent to kanjana.perera@phri.ca and ethics approval has been obtained.
Results
Overall, 535 Y-ESUS were enrolled (Supplemental Figure S1). The mean age of registry participants was 40.4 (standard deviation (SD) = 7.3) years, 238 (44%) were female, and the median National Institutes of Health Stroke Scale (NIHSS) was 2 (interquartile range = 1–6). Of the 535 patients, 238 (45%) had MRI performed, whereas the rest had CIL assessed by CT imaging.
CIL presence
CILs were present in 76/534 (14.2%) patients. In one patient, information on CIL was missing. The median number of CILs was 1.0 (IQR = 1–2, see Table 1 for full details). In patients with CIL, 42/76 (55%) had at least one cortical CIL, 38/76 (50%) had at least one non-cortical CIL, and 3/76 (4%) had an uncertain phenotype.
Chronic ischemic lesions characteristics.
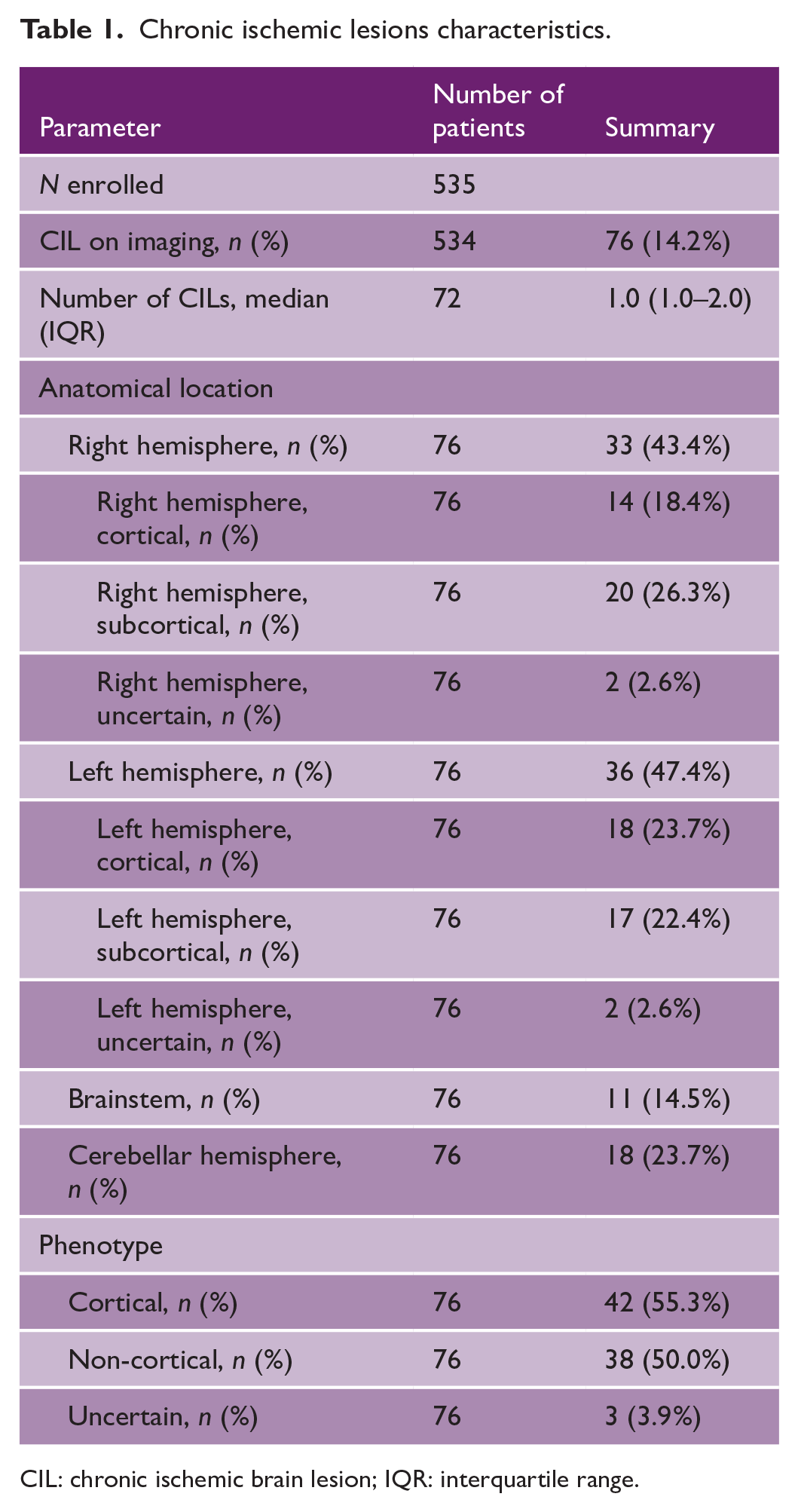
CIL: chronic ischemic brain lesion; IQR: interquartile range.
Among 37 patients with a medical history of prior stroke or transient ischemic attack, CIL was present in 25/37 (68%), whereas 51/76 (67%) Y-ESUS had CIL without a medical history of prior stroke or transient ischemic attack (TIA) (Table 2). There was no difference in the detection of CIL according to the imaging modality (MRI vs CT), that is, there was no difference in MRI obtained in those with CIL as compared to those without (50.0% vs 44.6%, p = 0.385).
Baseline characteristics by the presence of CIL.
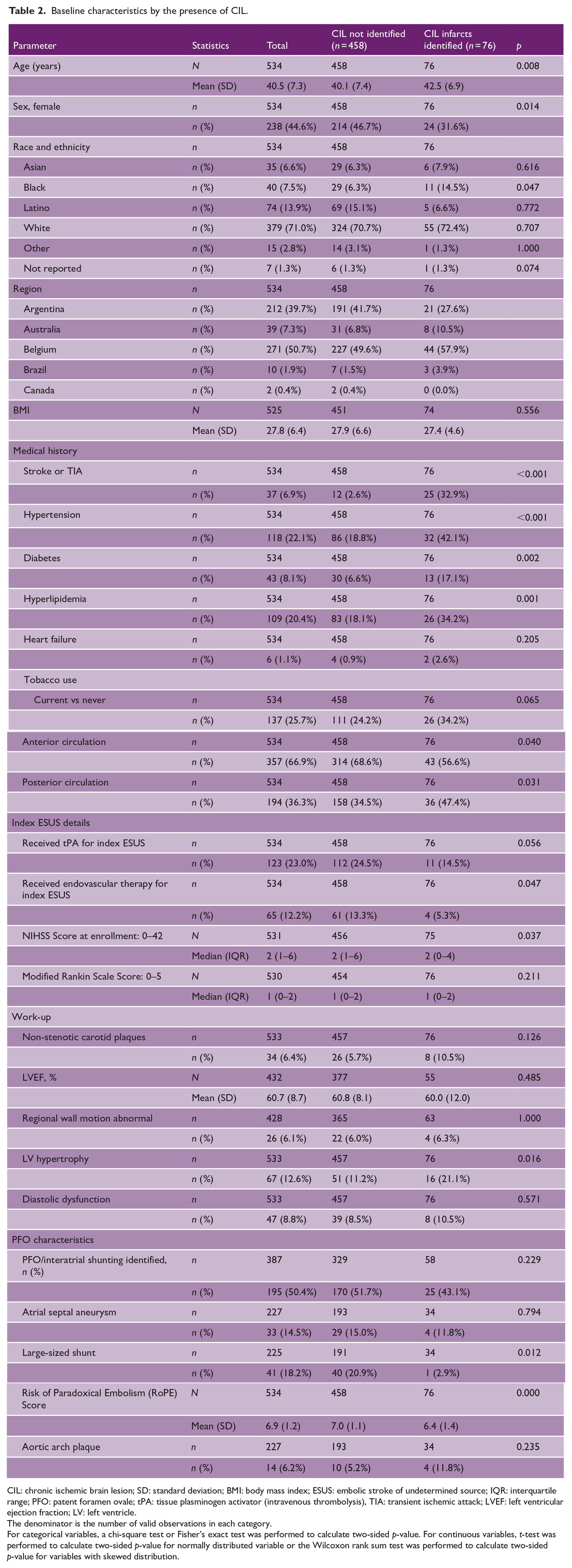
CIL: chronic ischemic brain lesion; SD: standard deviation; BMI: body mass index; ESUS: embolic stroke of undetermined source; IQR: interquartile range; PFO: patent foramen ovale; tPA: tissue plasminogen activator (intravenous thrombolysis), TIA: transient ischemic attack; LVEF: left ventricular ejection fraction; LV: left ventricle.
The denominator is the number of valid observations in each category.
For categorical variables, a chi-square test or Fisher’s exact test was performed to calculate two-sided p-value. For continuous variables, t-test was performed to calculate two-sided p-value for normally distributed variable or the Wilcoxon rank sum test was performed to calculate two-sided p-value for variables with skewed distribution.
Overall, Y-ESUS with CIL were more often male and had a higher cardiovascular risk profile: they were older, had more often hypertension, diabetes, and hyperlipidemia. In Y-ESUS with additional CIL, stroke was more frequent in the posterior circulation if compared to Y-ESUS without CIL (Table 2). There was a trend toward lower stroke severity on hospital admission and a lower usage of intravenous thrombolysis and mechanical thrombectomy in Y-ESUS with CIL (Table 2). There was no significant difference in baseline and clinical characteristics in Y-ESUS with a cortical CIL compared to patients without a cortical CIL (Supplemental Table S1). Atrial fibrillation (AF) was detected in one of 76 (1.3%) patients with CIL and 14/458 (3.1%) without CIL during 12-month follow-up (p = 0.41).
In unadjusted analysis, CIL patients had the same rate of recurrent ischemic stroke with an RR of 1.0 (95% CI = 0.23–4.4). After adjustment for the cardiovascular risk profile, CIL was associated with lower ischemic stroke recurrence rate with RR of 0.17 (95% CI = 0.05–0.61, Supplemental Table S2) setting non-CIL Y-ESUS as the reference. There was no difference in ipsilateral plaque/degree of stenosis between Y-ESUS with CIL and Y-ESUS without CIL (Table 2).
PFO
In total, 387/535 (72%) patients had adequate work-up to reliably assess PFO status, namely, either transesophageal echocardiography or transthoracic echocardiography with bubble test and Valsalva maneuver. Among them, PFO was identified in 195/387 (50%), whereas PFO was not detected in 192/387 (50%). There was no difference in the number or phenotypes of CIL in Y-ESUS with and without PFO (Table 3). PFO patients had fewer vascular risk factors (hypertension, diabetes, hyperlipidemia) except smoking compared to Y-ESUS without PFO (Supplemental Table S3). Stroke severity on admission and functional impairment was lower in PFO patients (Supplemental Table S3). Also, after adjustment for baseline factors (including BMI, sex, hypertension, diabetes, and current smoking), CIL presence or phenotypes were not significantly associated with the presence of PFO (OR = 0.9; 95% CI = 0.48–1.72).
Chronic ischemic lesions characteristics by presence or absence of overall patent foramen ovale (PFO) and by the PFO-related stroke categories.
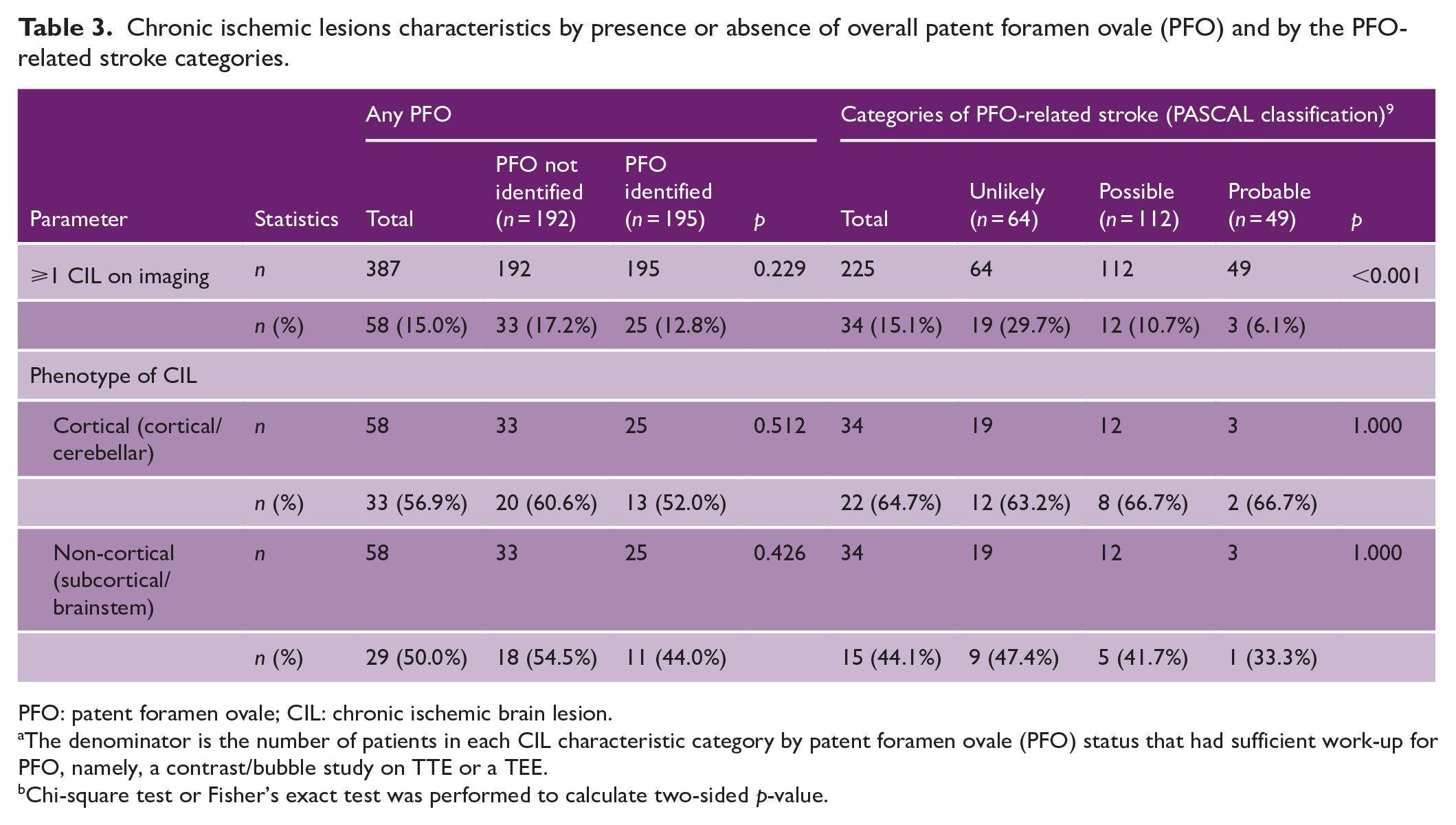
PFO: patent foramen ovale; CIL: chronic ischemic brain lesion.
The denominator is the number of patients in each CIL characteristic category by patent foramen ovale (PFO) status that had sufficient work-up for PFO, namely, a contrast/bubble study on TTE or a TEE.
Chi-square test or Fisher’s exact test was performed to calculate two-sided p-value.
The RoPE Score was lower in patients with CIL as compared to patients without CIL (6.4 vs 7.0, p < 0.001, Table 2). A large-size shunt was less frequently identified in CIL patients, which also less often had an atrial septal aneurysm (Table 2). When only considering pathogenic PFO according to the PASCAL classification, CILs were less frequent in probable pathogenic PFO (than with probable non-pathogenic PFO (29.7% vs 6.1%, p < 0.001)). The frequency of cortical phenotype was not found to be dependent on PFO-related stroke according to the PASCAL classification (Table 3).
Discussion
In this prospective cohort study including Y-ESUS, we provide a characterization of patients according to CIL presence and phenotypes and assessed the association with presence of PFO. The main findings of this study are: (1) one in seven Y-ESUS patients has additional CIL; (2) several vascular risk factors were associated with presence of CIL; and (3) neither any CIL nor cortical CILs were associated with presence of PFO on cardiac work-up. However, CILs were associated with a lower probability of a pathogenic PFO and lower stroke recurrence but not associated with a first episode of AF during follow-up.
The overall CIL rate of 14% found in our study is similar to other studies including stroke patients of less than 50 years of age.1,11–13 There was a nearly even split between cortical and non-cortical phenotypes; however, no relevant differences in age or vascular risk factor profile according to this imaging appearance could be identified. 67% of those with CIL had no medical history of prior stroke or TIA.
Several vascular risk factors were associated with the presence of CIL: Y-ESUS patients with additional CIL had roughly twice as often hypertension, diabetes, and hyperlipidemia. Hence, it could be reasonable to screen those with additional CIL more thoroughly, for example, using 24-h blood pressure monitoring or to use more sensitive screening tools (e.g. oral glucose tolerance test). It might also impact future trials on therapeutic strategies investigating the best secondary prevention strategies, stratifying patients accordingly (e.g. more aggressive lipid reduction, prolonged electrocardiogram (ECG) monitoring, tumor screening, 14 and antiphospholipid antibody testing in Y-ESUS patients with additional CILs). Although not reaching significance, Y-ESUS with CIL numerically more often had atherosclerosis (carotid and aortic plaques) indicating that atherosclerotic mechanisms might be more important among those patients.
Since CIL was not independently associated with PFO detection on work-up, the presence or absence of CIL should not influence which Y-ESUS should undergo PFO work-up. Although overall there was no difference in PFO detection between Y-ESUS with and without CIL, the association of CIL with lower likelihood of PFO-related stroke according to the PASCAL classification fits to the higher cardiovascular risk factor profile of CIL patients. Of note, a large-size shunt (high-risk feature) was less frequently identified in CIL patients. It should be noted that at the timepoint of the trial, those patients with PFO and high-risk features were still considered ESUS patients, whereas today they would be categorized as PFO-related stroke patients. 15 Finally, there was no difference in cortical CILs according to presence of any or pathogenic PFO, suggesting that most PFO-associated strokes are manifest on the first embolic event and do not frequently embolize prior causing covert cortical CILs.
Overall, stroke recurrence risk was the same in Y-ESUS with and without CIL. However, after adjustment, Y-ESUS patients with additional CIL had a lower recurrence risk. This might represent a chance finding since on crude analysis, there was no such signal and the lower recurrence found after adjustment. It might also be due to the fact that those without additional chronic CIL might have a higher recurrence rate due to other underlying causes not necessarily linked to vascular risk factors (e.g. occult cancer, thrombophilia, or other). Finally, it could be explained by more aggressive work-up, risk factor control, and secondary prevention in those with additional CIL. This is backed-up by the fact that patients with CILs more often received antihypertensive medication and insulin treatment (Supplemental Table S4).
Strengths and limitations
Strengths include a large, prospectively collected high-quality database from various global regions with a very low percentage of missing data in a well-defined cohort of patients. There are several limitations already mentioned in the publication of the main study results3: those include mainly inclusions at specific high-volume stroke centers, which may not accurately represent the full spectrum of stroke cases; furthermore, the informed consent process may have introduced selection bias toward less severe stroke and exclusion of patients with aphasia, although next-of-kin inclusion was possible; and finally, strategies for AF screening beyond 24 h of monitoring were site-specific. 3 More importantly for this analysis, acquisition of brain imaging was heterogeneous (CT and MRI), reading of brain imaging was done locally and without blinding or analysis of agreement. However, the sensitivity analysis restricting the findings to patients who underwent MRI showed consistent results (Supplemental Table S5). The classification of cortical involvement was based on the assumption that cerebellar hemisphere involvement corresponded to a cortical phenotype, and the details about the size or fulfillment of criteria of lacunar type were not available. Very small CILs might have been missed, as they were not specifically core-lab adjudicated. In addition, not all patients had sufficient echocardiographic work-up to rule-in or rule-out PFO.
Summary and conclusions
One in seven Y-ESUS had an additional CIL and most of the CILs were not related to previous history of stroke or TIA. CILs were associated with several vascular risk factors, markers of atheromatosis, and lower probability of a pathogenic PFO. Surprisingly, Y-ESUS with CIL presented a lower stroke recurrence rate compared to Y-ESUS without CIL.
Supplemental Material
sj-docx-1-wso-10.1177_17474930231217917 – Supplemental material for Chronic ischemic lesions and presence of patent foramen ovale in young adults with embolic stroke of undetermined source: Results of the young ESUS patient registry
Supplemental material, sj-docx-1-wso-10.1177_17474930231217917 for Chronic ischemic lesions and presence of patent foramen ovale in young adults with embolic stroke of undetermined source: Results of the young ESUS patient registry by Thomas Raphael Meinel, Kate Tsiplova, Amanda Taylor, Elena Meseguer, Karl Georg Haeusler, Robert G Hart, Marcel Arnold and Kanjana S Perera in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.G.H. reports speaker’s honoraria, consulting fees, lecture honoraria, and/or study grants from Abbott, Amarin, AstraZeneca, Bayer Healthcare, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol-Myers Squibb, Daiichi Sankyo, Edwards Lifesciences, Medronic, Novartis, Pfizer, Portola, Premier Research, Sanofi, SUN Pharma, and W.L. Gore and Associates outside the submitted work. R.G.H. reports research support and stipends from Bayer AG for serving as the co-principal investigator of the NAVIGATE ESUS trial. The other authors declare no potential conflicts of interest for the content of this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Population Health Research Institute and in part by Bayer in the first 2 years of the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.