
Abstract
Intracerebral hemorrhage (ICH) is a devastating disease, causing high rates of death, disability, and suffering across the world. For decades, its treatment has been shrouded by the lack of reliable evidence, and consequently, the presumption that an effective treatment is unlikely to be found. Neutral results arising from several major randomized controlled trials had established a negative spirit within and outside the stroke community. Frustration among researchers and a sense of nihilism in clinicians has created the general perception that patients presenting with ICH have a poor prognosis irrespective of them receiving any form of active management. All this changed in 2023 with the positive results on the primary outcome in randomized controlled trials showing treatment benefits for a hyperacute care bundle approach (INTERACT3), early minimal invasive hematoma evacuation (ENRICH), and use of factor Xa-inhibitor anticoagulation reversal with andexanet alfa (ANNEXa-I). These advances have now been extended in 2024 by confirmation that intensive blood pressure lowering initiated within the first few hours of the onset of symptoms can substantially improve outcome in ICH (INTERACT4) and that decompressive hemicraniectomy is a viable treatment strategy in patients with large deep ICH (SWITCH). This evidence will spearhead a change in the perception of ICH, to revolutionize the care of these patients to ultimately improve their outcomes. We review these and other recent developments in the hyperacute management of ICH. We summarize the results of randomized controlled trials and discuss related original research papers published in this issue of the International Journal of Stroke. These exciting advances demonstrate how we are now at the dawn of a new, exciting, and brighter era of ICH management.
Keywords
Intracerebral hemorrhage—the deadly sibling of ischemic stroke
Intracerebral hemorrhage (ICH) is caused by the rupture of cerebral vessels which results in bleeding within the brain parenchyma and/or ventricles. 1 Overall, ICH comprises approximately 10–15% of all strokes worldwide, but the rates are higher in low- and middle-income countries. 2 Compared to ischemic stroke, the incidence of ICH has increased in recent years and the prognosis remains poor.3,4 Current estimates predict a significant increase in the incidence of ICH in Europe related to aging and greater use of anticoagulants, with major implications for health care systems and societies. 5
Treatment of ICH before 2023—widespread frustration and nihilism
For decades, treatment of ICH has been overshadowed by limited evidence and a presumed lack of effective treatment options reflected by neutral and restrictive guideline recommendations.6,7 Several randomized controlled trials of surgical treatment (i.e. different approaches to evacuation of parenchymal or intraventricular hematoma),8–11 blood pressure (BP) control,12,13 and hemostatic therapies,14–16 resulted in either borderline significant or neutral results. The evidence was persuasive from INTERACT2, 12 and stronger when pooled with other trials as part of an individual patient data meta-analysis, 17 for a beneficial effect of early intensive BP lowering. Although a study-level meta-analysis of hematoma evacuation also found a potential benefit, 18 there is ongoing uncertainty over which patients have the most to gain from neurosurgery along with the optimal timing and technique of intervention. Collectively, these efforts have contributed to somewhat of a negative spirit within (and outside) the stroke community, and in turn degrees of frustration and nihilism regarding treatment approaches and the perception of a uniformly poor prognosis for patients with ICH. 19
Treatment targets in ICH
Several promising treatment targets exist for ICH (Figure 1). In the hyperacute phase, the primary aim is to stop the bleeding which grows from the original site in “domino” or “avalanche” fashion through the secondary shearing of neighboring vessels. 20 Restricting the ongoing bleeding cascade—usually depicted as hematoma expansion on follow-up imaging—is paramount as it is consistently identified as a major predictor of poor outcome from ICH.21–23 The other key predictors of outcome are an early time-window (i.e. <6 h of onset), high BP, baseline hematoma volume (medium to large), intraventricular extension, and prior use of oral anticoagulation therapy.24,25 Even a small initial hematoma may evolve into a devastating large lesion (Figure 2).
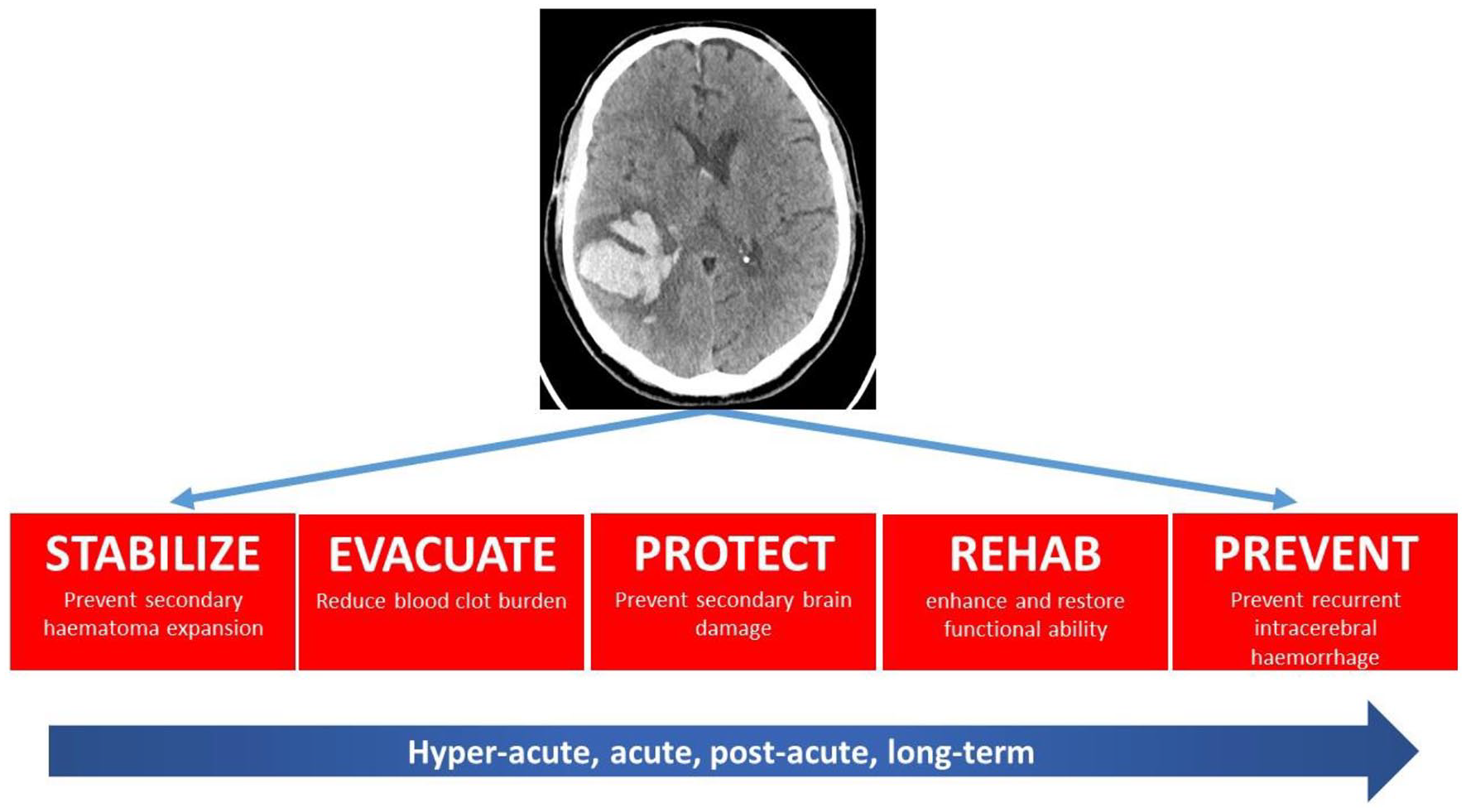
Treatment targets in intracerebral hemorrhage.
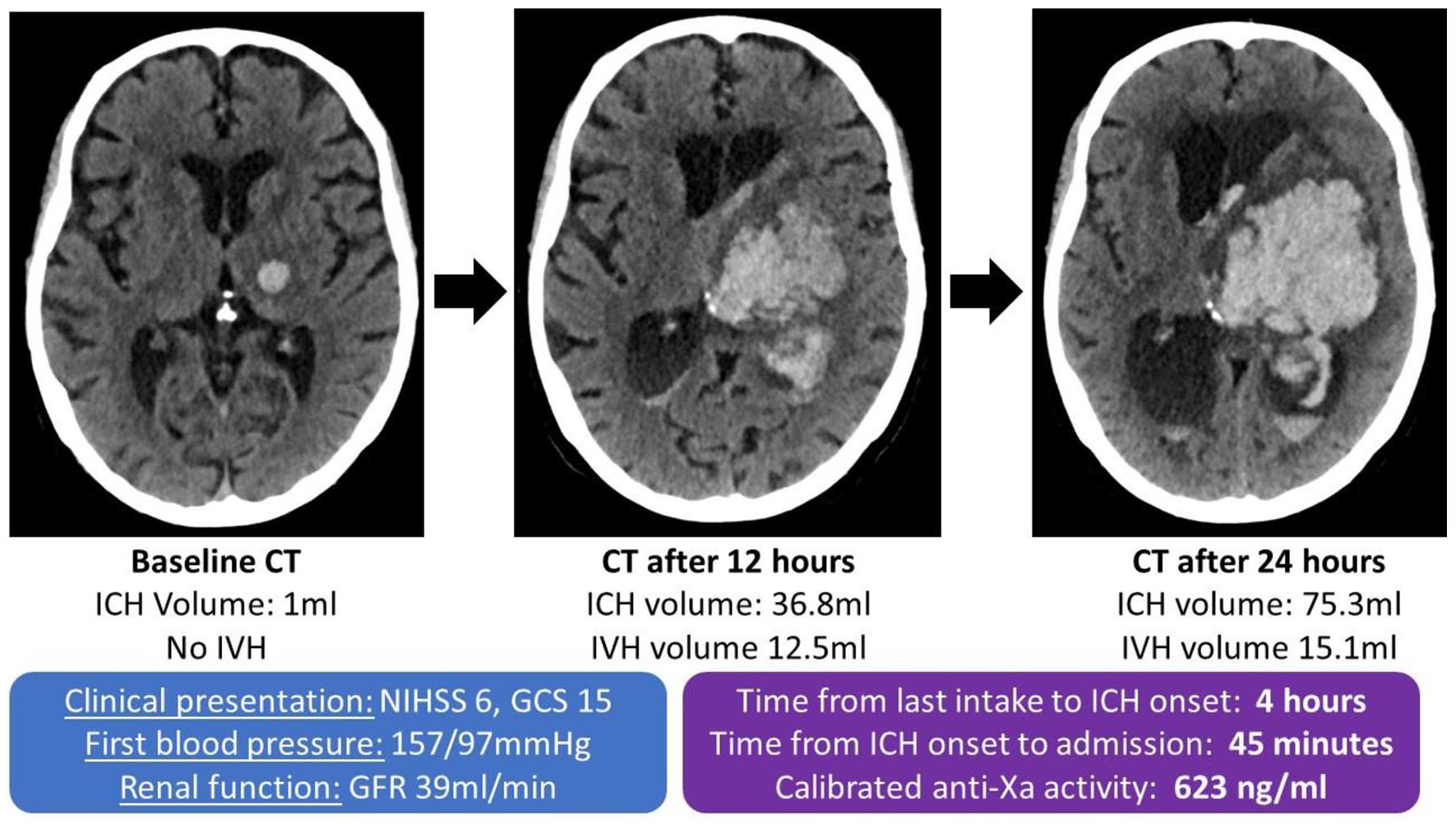
Case example of a patient with atrial fibrillation presenting with a small baseline hemorrhage early after onset with a recent intake of a factor Xa-inhibitor, high anti-Xa activity, and elevated blood pressure resulting in devastating hematoma expansion. ICH: denotes intracerebral hemorrhage, IVH: intraventricular hemorrhage, NIHSS: National Institute of Health stroke severity scale, GCS: Glasgow coma scale.
Hematoma evacuation to reduce the clot burden is conceptually simple as a pivotal treatment option to reduce direct and indirect/secondary brain damage after ICH. Yet, a series of randomized controlled trials conducted over 40 years have failed to clearly show a benefit from surgery on the pre-defined primary outcome. Pre-defined subgroup and secondary analysis have shown benefits of hematoma evacuation in patients with altered level of consciousness from a lobar ICH and from external ventricular drainage in those with occlusive hydrocephalus.6,26 Other treatment targets include the prevention of secondary brain damage (by mitigating the toxic effects of blood breakdown products), approaches to rehabilitation as the pattern of recovery is different in ICH to ischemic stroke, and in the secondary prevention of recurrent ICH as well as serious ischemic cardiovascular events.
The year 2023—dawn of a new era
The year 2023 will be remembered as the dawn of a new era in the treatment of ICH, with three pivotal randomized controlled trials showing clear benefits of different treatment approaches. First, the Early Minimally Invasive Removal of Intracerebral Hemorrhage (ENRICH) trial showed that a minimally invasive trans-sulcal parafascicular craniotomy with endovascular clearage to remove the hematoma was superior to usual standard of care for functional outcome. 1 First presented at the annual conference of the American Association of Neurological Surgeons in Los Angeles in April 2023, the results have only recently been published. 27 Second, the third Intensive Care Bundle with Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial (INTERACT3) found that the implementation of a care bundle protocol incorporating intensive BP lowering with other management algorithms for physiological control commenced within several hours of the onset of symptoms resulted in improved functional outcome for a broad range of patients with acute ICH. 28 Finally, the Randomised Trial of Andexanet alfa Versus Usual Care in Patients With Acute Intracranial Haemorrhage While on an Oral Factor Xa-Inhibitor (ANNEXa-I) found that use of intravenous andexanet alfa, a recombinant modified Factor Xa molecule, was superior to usual care (i.e. with 86% use of prothrombin complex concentrate) in terms of hemostatic efficacy for patients with ICH related to factor Xa-inhibitor anticoagulation therapy. 29 These three positive trials pave the way for an entirely new, more optimistic era, of hyperacute treatment of ICH. We discuss these papers along with several manuscripts reporting novel data on ICH in this issue of the International Journal of Stroke (IJS).
First: care bundle approaches for hyperacute treatment
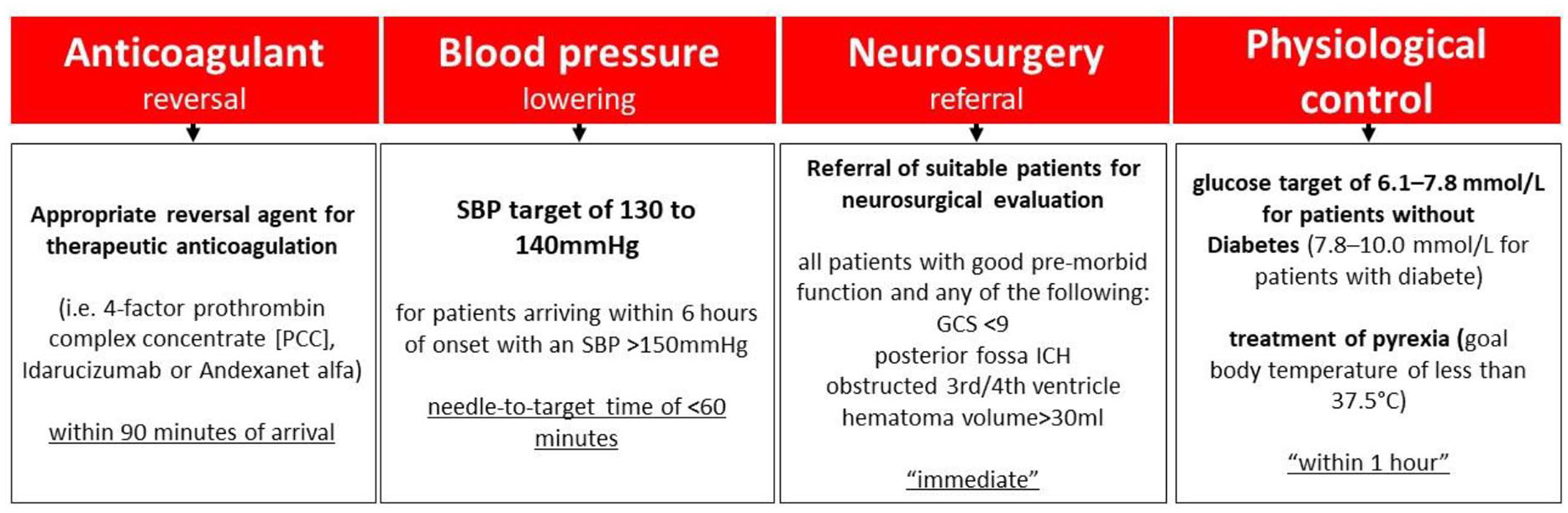
Although primary randomized controlled trials testing single interventions (i.e. BP control, hematoma evacuation) were neutral, these measures were implemented to different degrees in hyperacute treatment pathways due to positive signals from secondary analysis or non-randomized studies. Combining different measures in a care bundle—anticoagulation reversal, BP control and a care pathway for neurosurgery referral (Figure 3)—was first shown to reduce 30-day case fatality in a “before-and-after” quality improvement project in Manchester, UK. 30 The approach was subsequently rigorously evaluated with control of glucose and body temperature being included in protocols without neurosurgery referral using an international stepped wedge cluster randomized controlled design (INTERACT3) 28 where hospitals were centrally randomly allocated into three sequences of implementation of the care bundle across nine low- and middle-income and one high-income countries. Overall, for the 7036 patients with ICH at 121 hospitals with available outcome data, the likelihood of a poor functional outcome was significantly lower in the care bundle group (common odds ratio = 0.86, 95% confidence interval = 0.76–0.97; p = 0.015). INTERACT3 therefore extends knowledge of the benefits of well-organized stroke care in showing that the implementation of a relatively simple, time- and target-based protocol of intensive BP lowering and other management algorithms for physiological control, initiated within several hours of the onset of symptoms, improves outcome from ICH. There is increasing agreement over the benefits of a care bundle approach and that it should be implemented in all hospitals that care for patients with ICH. 31 However, there are recognized implementation challenges according to the availability of resources and skill mix, 32 and concerns may arise over the relative effectiveness of various components of a care bundle. The most recent findings of the fourth INTEnsive ambulance-delivered BP Reduction in hyper-ACute stroke Trial (INTERACT4) are therefore very timely in showing clear benefits of rapid BP control within just a few hours of the onset of ICH. 33 Furthermore, these results provide evidence and underlying mechanistic support to reconfigure systems of care for time-intensive urgency toward the management of ICH as in ischemic stroke. 34
Second: direct oral anticoagulants—new challenges for ICH treatment
New challenges have arisen from the increased use of direct oral anticoagulants, 35 which have largely replaced vitamin K antagonists, for the treatment of atrial fibrillation, pulmonary embolism, and other thromboembolic conditions. Recent data from a study that combined two national stroke registries found a dramatic change in the spectrum of ICH with a shift from vitamin K antagonists to direct oral anticoagulants without a change in the profile of patients in the last decade. 36 The changing epidemiology of ICH in high income countries is further refined by a study of Gabriele et al. 37 published in this issue of the IJS. In a population-based study undertaken in the region of l’Aquila in Italy, the incidence of anticoagulation-associated ICH related to direct oral anticoagulants overtook that related to vitamin K antagonists (incidence rate ratio = 4.71) from 2020 after being stable over the period 2011 to 2020 (Figure 4). 37 Moreover, 30-day case fatality was extremely high at 48% in patients with anticoagulation-associated ICH. As well as highlighting the importance of direct oral anticoagulant-related ICH, it draws attention to the need of services to better manage the condition, further emphasized in a study that combined national stroke datasets in Norway and Switzerland where at 3 months, overall mortality was 43% and only 25% of patients who survived a direct oral anticoagulant-related ICH were functionally independent (defined by a modified Rankin scale score of 0–2). 36
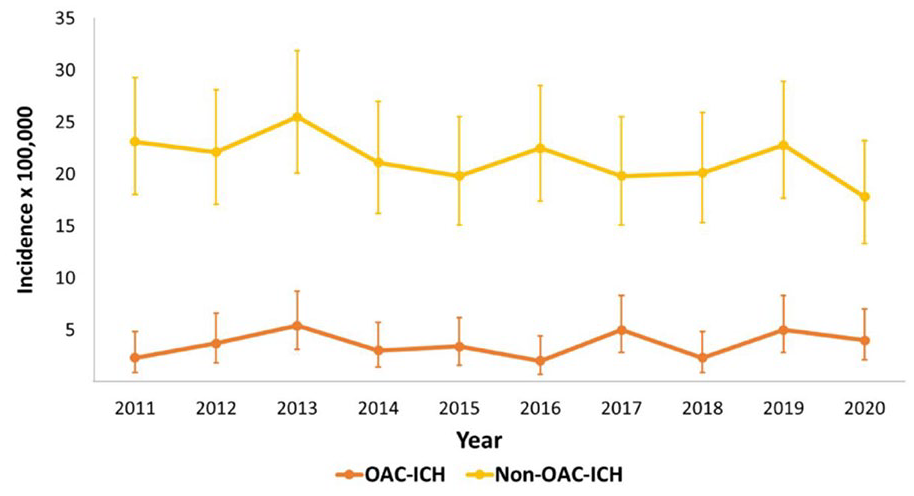
Gabriele et al. 37 report the incidence of anticoagulation-associated intracerebral hemorrhage (OAC-ICH) and non-anticoagulation-associated intracerebral hemorrhage (non-OAC-ICH) from a population-based study over a period of 10 years.
Third: andexanet alfa—a specific reversal agent for factor Xa-inhibitor–associated ICH
The results from Gabriele et al. 37 and the Swiss-Norwegian study 36 clearly identify the unmet medical need to improve the management of patients with factor Xa-inhibitor–associated ICH. A study from Hong Kong found that the use of prothrombin complex concentrate, frequently recommended in guidelines, 38 was not associated with any benefit in patients with direct oral anticoagulant-associated ICH, 39 further amplifying the need for better treatment options. Andexanet alfa, a recombinant modified factor Xa molecule that acts as a decoy and sequesters factor Xa-inhibitors, was first tested in a single arm unblinded study (ANNEXa-4) without any control group. 40 To overcome these limitations, Siepen et al. 41 performed an individual patient data analysis of ANNEXa-4 and TICH-NOAC (NCT02866838) published in this issue of the IJS. 41 Outcomes for patients who received andexanet alfa (from ANNEXa-4) were compared with patients who received usual care (i.e. no treatment or prothrombin complex concentrate) in a small randomized controlled trial conducted in Switzerland, where patients received add-on therapy with tranexamic acid or placebo on top of usual care. 41 Both trials were ideally suited to be combined as the baseline characteristics (i.e. age, time since last intake, etc) of participants were comparable, important confounders (i.e. anti-Xa activity, treatment metrics) were prospectively collected, and all the outcomes (i.e. hematoma expansion, functional outcome, and thromboembolic events) were systematically captured and adjudicated by central blinded reviewers. Siepen et al. found that andexanet alfa was independently associated with lower odds of hematoma expansion compared to usual care without any association with thromboembolic complications or differences in functional outcome or mortality. The results provide support for andexanet alfa being superior to usual care through the provision of hemostatic efficacy in patients with factor Xa-inhibitor–associated ICH, a finding which requires confirmation in randomized controlled trials.
After conditional approval by the US Food and Drug Administration (FDA), ANNEXa-I was initiated to compare andexanet alfa with usual care in patients with intracranial hemorrhage. 29 The study enrolled patients with factor Xa-inhibitor associated ICH within 15 h of last intake and 6 h of the onset of symptoms. A total of 900 patients were planned to be enrolled, but the trial was stopped after the first prespecified interim analysis for efficacy was undertaken in 450 patients in May 2023, and the results in a final sample of 530 participants were presented at the World Stroke Congress in October. In both data sets (450 and 530 patients, respectively), andexanet alfa was superior for hemostatic efficacy compared to usual care, with absolute differences of 13% and 11%, respectively. However, andexanet alfa increased the incidence of serious thromboembolic complications, with an absolute between-group difference of 4.6%. However, the trial was not powered to show a difference in mortality or functional outcome, and only assessed at 30 days.
These data indicate that andexanet alfa is superior for hemostatic efficacy in patients with factor Xa-inhibitor–associated ICH, with findings of the individual patient data analysis of Siepen et al. 42 confirm the results of ANNEXa-I. However, given the current cost of andexanet alfa and its associated potential complications further data are required to guide its application in routine practice.
Fourth: future challenges—factor XI inhibitors
Novel factor XI inhibitors are promising treatment options for stroke prevention in patients with arteriosclerosis-related ischemic stroke or atrial fibrillation as they inhibit thrombosis without compromising hemostasis. 43 Cerebral microbleeds are hemorrhagic imaging markers of bleeding-prone cerebral small vessel disease, a major cause underlying ICH in elderly adults. 44 It is hypothesized that cerebral microbleeds may either directly convert into symptomatic macrohemorrhage and/or predict ICH through the overall small vessel disease burden in patients on anticoagulants. 45 In this issue of the journal, Balali et al. 46 report reassuring data from secondary analysis of PACIFIC-STROKE (NCT04304508), 47 a randomized controlled phase-II trial assessing the factor XI inhibitor asundexian. They found that patients receiving asundexian were not at increased risk of developing new cerebral microbleeds on follow-up magnetic resonance imaging (MRI), hemorrhagic transformation of baseline ischemic stroke, or intracranial bleeding compared to patients receiving placebo. Taken together, asundexian appears safe in patients with non-cardioembolic ischemic stroke and hemorrhage-prone cerebral small vessel disease marked by cerebral microbleeds on MRI.
Fifth: hematoma evacuation: one positive trial and unanswered questions
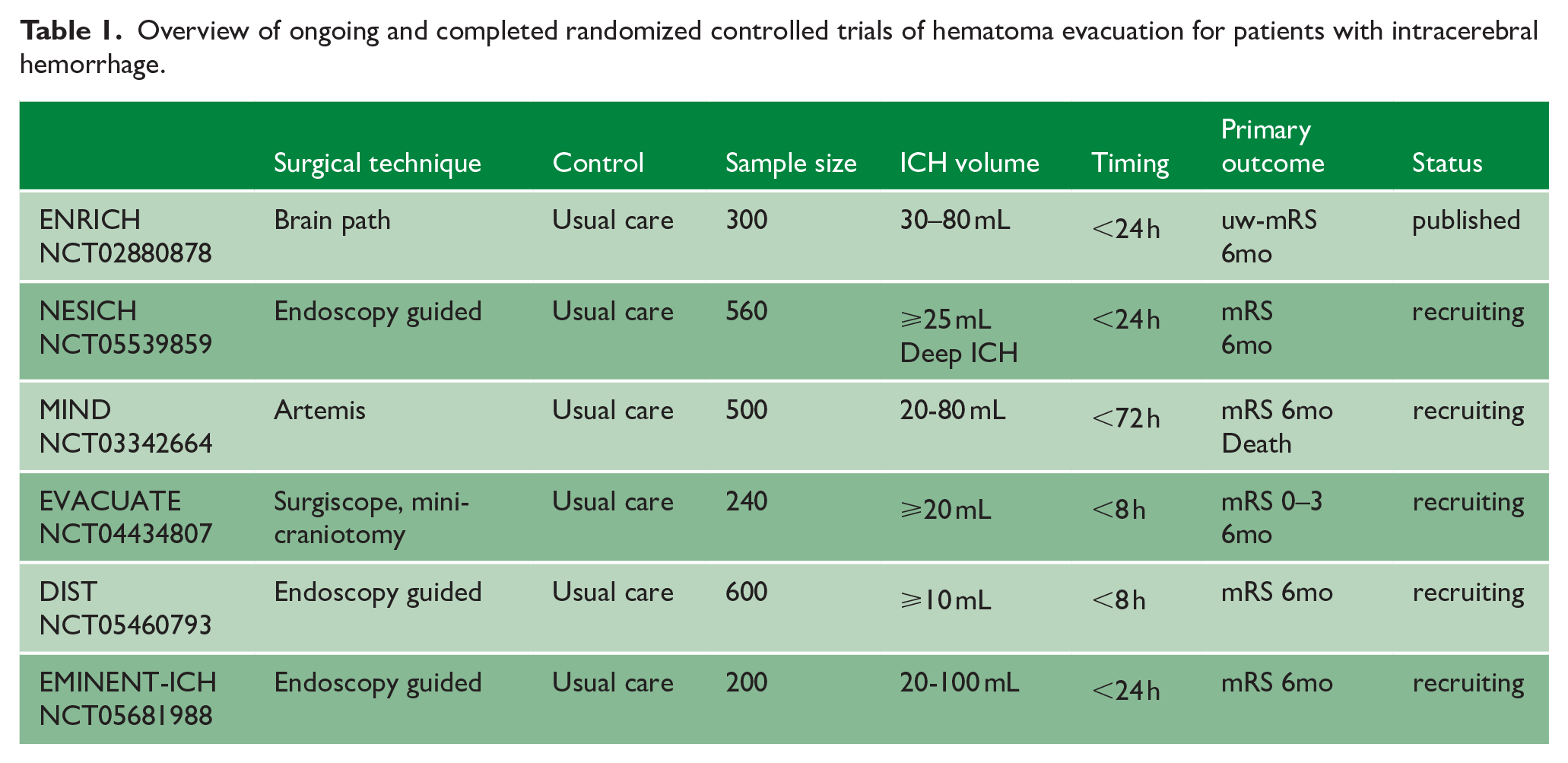
In theory, early evacuation of the blood clot from the brain should translate into significant benefits for patients with ICH, likely comparable to the benefits seen with mechanical thrombectomy for large vessel occlusion ischemic stroke. 48 Unfortunately, several pivotal trials of different interventional approaches9–11 have been neutral, although a systematic review and meta-analysis identified a treatment benefit. 18 ENRICH included 300 patients to show a benefit of early minimal invasive surgery compared to usual care in ICH. 27 After a preplanned interim efficacy analysis, enrollment of patients with deep anterior hematomas was stopped so that the final study population comprised approximately 70% of patients with lobar ICH. Overall, minimal invasive hematoma evacuation was shown superior to usual care on the utility weighted modified Rankin scale score approach assessing functional outcome. This is a major step forward to support surgery for ICH, but several questions remain over the optimal timing, technique, patient selection, and use of ancillary treatments. A number of ongoing trials will assess different approaches for haematoma evacation (Table 1). In this issue of IJS, Wang et al. 49 report their protocol for a new trial, NEuroendoscopic Surgery for Intracerebral Hemorrhage (NESICH) (NCT05539859), which aims to recruit up to 560 patients with ICH to compare neuroendoscopic surgery with usual care according to the primary endpoint of good functional outcome (modified Rankin scale score 0–3) at 180 days. This trial will be conducted in China, a country with a significant burden of ICH and established approaches to neurosurgical hematoma evacuation for ICH. A different approach was the use of decompressive hemicraniectomy to release pressure in large deep ICH without evacuating the blood clot, in the Swiss trial of decompressive craniectomy versus best medical treatment of spontaneous supratentorial intracerebral hemorrhage (SWITCH) (NCT02258919) trial. 50 The results were presented at the European Stroke Organisation Conference in Basel, Switzerland in 15–17 May 2024. Decompressive surgery is now a possible option in patients with space-occupying large deep ICH (Beck et al 2024). 51
Overview of ongoing and completed randomized controlled trials of hematoma evacuation for patients with intracerebral hemorrhage.
Summary and outlook
There is now renewed vigor in the management of patients with ICH in the community, driven by several abovementioned positive trials of hyperacute treatment: benefits of a care bundle approach driving by early intensive BP lowering, and the use of early endoscopic surgical hematoma evacuation and reversal of factor Xa-inhibitor activity using andexanet alfa in appropriately selected patients. For the first time in history, there is now convincing evidence that ICH is a treatable disease. We therefore need to abandon nihilism and inertia. While ongoing trials will add further evidence to this landscape, the time has come to shift in systems of care toward urgent, active management of patients with ICH. The year 2023 was the starting point; responsibility for the new era of ICH management is now upon us all.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.J.S. received funding from the Swiss National Science Foundation, the Swiss Heart Foundation, the Bangerter-Rhyner foundation, and AstraZeneca. D.J.S. received fees (paid to his institution) for speaker bureau and consultancy from AstraZeneca, VamX, Bioxodes, Javelin, and Pfizer. C.S.A. reports receiving research grants from the National Health and Medical Research Council of Australia, the Medical Research Council and Medical Research Foundation of the UK, and Penumbra and Takeda, paid to his institution.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.