
Abstract
Background:
While direct-acting oral anticoagulants (DOACs) have established efficacy in reducing the risk of ischemic stroke, they still leave a residual risk of stroke, which may be greater in practice (0.7–2.3%) than in controlled clinical trial settings. This meta-analysis examines four therapeutic approaches following a stroke in patients already on DOACs: continuing with the same DOAC, changing to a different DOAC, increasing the current DOAC dosage, or switching to a vitamin K antagonist (VKA), such as warfarin.
Methods:
Systematic review of literature from the MEDLINE, Embase, and Cochrane databases, was conducted in line with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The analysis focused on six studies with varied patient demographics, examining as outcomes as recurrent ischemic stroke, intracranial hemorrhage, other bleeding events, and mortality.
Results:
Six studies comprising 12,159 patients were included, all of them were observational. Patients who remained on their initial DOAC regimen had a lower risk of experiencing ischemic strokes (risk ratio (RR) 0.55; 95% confidence interval (CI) 0.43–0.70; p < 0.001; I2 = 0%), intracranial hemorrhage (RR 0.37; 95% CI 0.25–0.55; p < 0.001; I2 = 0%), and hemorrhagic events (RR 0.44; 95% CI 0.30–0.63; p < 0.001; I2 = 6%) compared to those who were switched to warfarin, with an increase in mortality rates (hazard ratio (HR) 1.85; 95% CI 1.06–3.24; p = 0.03; I2 = 84%). In contrast, neither changing to a different DOAC nor adjusting the dose proved to be more effective than the original regimen.
Conclusion:
Post-stroke adjustments to anticoagulation therapy—whether altering the drug or its dosage—do not yield additional benefits. In addition, the results suggest that warfarin may be less effective than DOACs for preventing stroke recurrence, bleeding complications, and death in this patient population.
Introduction
Anticoagulation is an important therapy for patients with non-valvular atrial fibrillation (NVAF), reducing the rates of ischemic stroke by 66%. 1 Traditional vitamin K antagonists (VKA), such as warfarin, have significant setbacks: the need for serum-level monitoring and interaction with food and other drugs. 2
Direct-acting oral anticoagulants (DOACs) have been developed as alternatives, with increasing adherence due to their easier management compared to VKA.3–5 Landmark studies have established their efficacy in reducing the risk of ischemic stroke in patients with NVAF.6–9 Even with the use of DOACs, patients still face a small but significant risk of stroke. Clinical trials have found this risk to range between 0.7% and 2.3%. However, the risk may be even higher in everyday practice outside clinical trials. 6
When a patient presents with an ischemic stroke while already using DOACs, four main strategies can be adopted: (1) maintaining the same drug and dose; (2) switching to another DOAC; (3) maintaining the drug but increasing the dose; and (4) switching to a VKA. This systematic review and meta-analysis aimed to compare these different strategies in terms of ischemic stroke recurrence and hemorrhagic events.
Methods
Following the Preferred Reporting Items for the Systematic Reviews and Meta-analysis (PRISMA) statement guidelines and Cochrane Collaboration Handbook of Systematic Review of Interventions, we performed this systematic review and meta-analysis.10,11 Ethical approval was not required as no new patient data were collected. This study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO: CRD42023470420).
Search strategy and data extraction
We systematically searched MEDLINE, Embase, and Cochrane Central Register databases from inception to October 2023. The search strategy included the terms “novel oral anticoagulant,” “direct oral anticoagulant,” “vitamin K antagonist,” “post-acute ischemic stroke,” and other similar terms in both “AND” and “OR” combinations to maximize the results obtained. The detailed search strategy can be found in the Supplementary Material. Previous systematic reviews, meta-analyses, and the references of the selected studies were also manually screened for any additional applicable studies. Two investigators (G.I.C. and R.B.R.) independently screened the results and performed data extraction using the Microsoft Excel (Microsoft Corp., Redmond, WA, United States) software. Discrepancies were solved by a third author (J.P.M.T.). Data were extracted from individual studies regarding study design, patient demographics (sex and age), treatment change plan strategies, and the outcomes of interest.
Eligibility criteria
Eligibility in this meta-analysis was restricted to studies that met all the following criteria: (1) randomized controlled trials (RCT), non-randomized trials, or observational studies; (2) including patients that suffered an ischemic stroke while using a DOAC; (3) analyzing strategies of modification of the previous treatment; and (4) reporting at least one outcome of interest.
We excluded studies that (1) were modeling studies; (2) included other types of strokes; (3) included patients with previous use of other anticoagulation medications, such as heparin; (4) did not present change in DOAC regimen; (5) presented overlapping patient populations.
Endpoints
Our outcomes of interest were ischemic stroke, intracranial hemorrhage, hemorrhagic events, and mortality. The event numbers of ischemic stroke, intracranial hemorrhage, and mortality were collected when mentioned directly by each study. Any intracranial or extracranial bleeding was considered a hemorrhagic event. Individual numbers of patients with and without events in each category were extracted to perform comparison among categories with different controls (maintaining DOAC regimen, switching to another DOAC, changing DOAC dose, and switching to warfarin).
Quality assessment
Risk of bias was assessed using the ROBINS-I tool (“Risk Of Bias In Non-randomized Studies—of Interventions”). 12 Two researchers evaluated the risk of bias independently, and disagreements were solved by a third author.
Statistical analysis
We used Review Manager 5.4.1 for all statistical analyses. The absolute numbers were collected for dichotomous outcomes to calculate risk ratios (RR) with a 95% confidence interval (CI). Hazard ratios (HRs) and corresponding 95% CIs from each trial were extracted for time-to-event clinical outcomes. These values underwent conversion to ln(HR) along with their respective standard errors, then combined using a random effects model. Heterogeneity was assessed with the Cochran’s Q test and I2 statistics. The p-values inferior to 0.10, and I2 ⩾ 25% were considered significant for heterogeneity. We used DerSimonian and Laird random-effects models.
Results
Our initial search yielded 1104 potential articles (Figure 1). After removing duplicates and initial title/abstract screening, 24 articles were retrieved and reviewed in full for possible inclusion. Of these, six studies were included in this systematic review.13–18 One study was not included in the pooled analysis, as compared to the maintenance of the previous oral anticoagulant (OAC) against the change of OAC after the stroke event without specifying outcomes by each agent change. 13 Among these studies, 4946 patients received the same regimen of DOAC after the stroke event, 2601 changed the type of DOAC, 1346 changed the dose of DOAC, and 465 changed DOAC to warfarin. One study reported data about adding antiplatelets in the treatment after the stroke event. 17 The follow-up ranged between 3 and 21.4 months. The baseline characteristics of the included studies are described in Table 1.
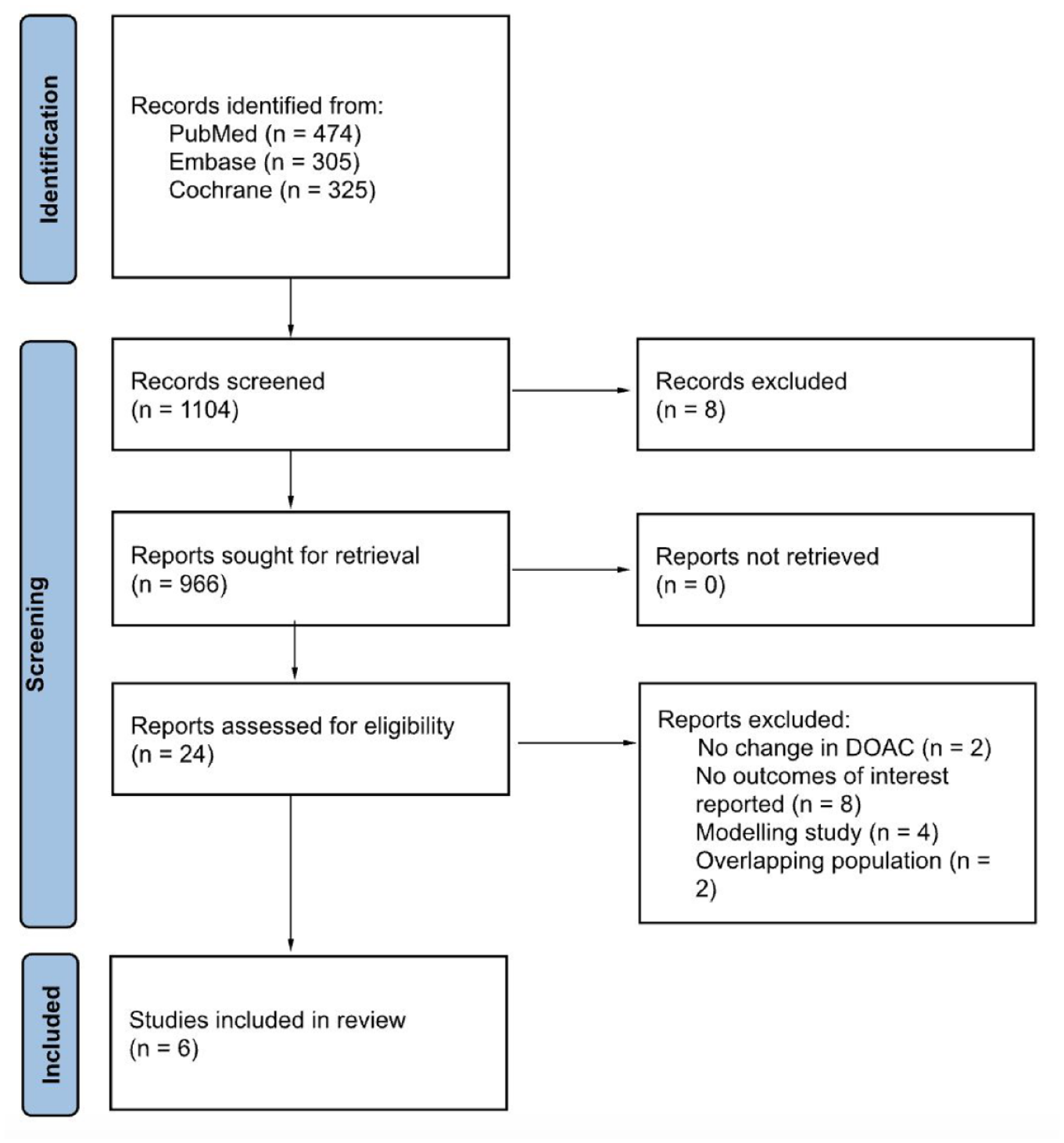
Flow diagram according to the PRISMA guidelines.
Characteristics of included studies.
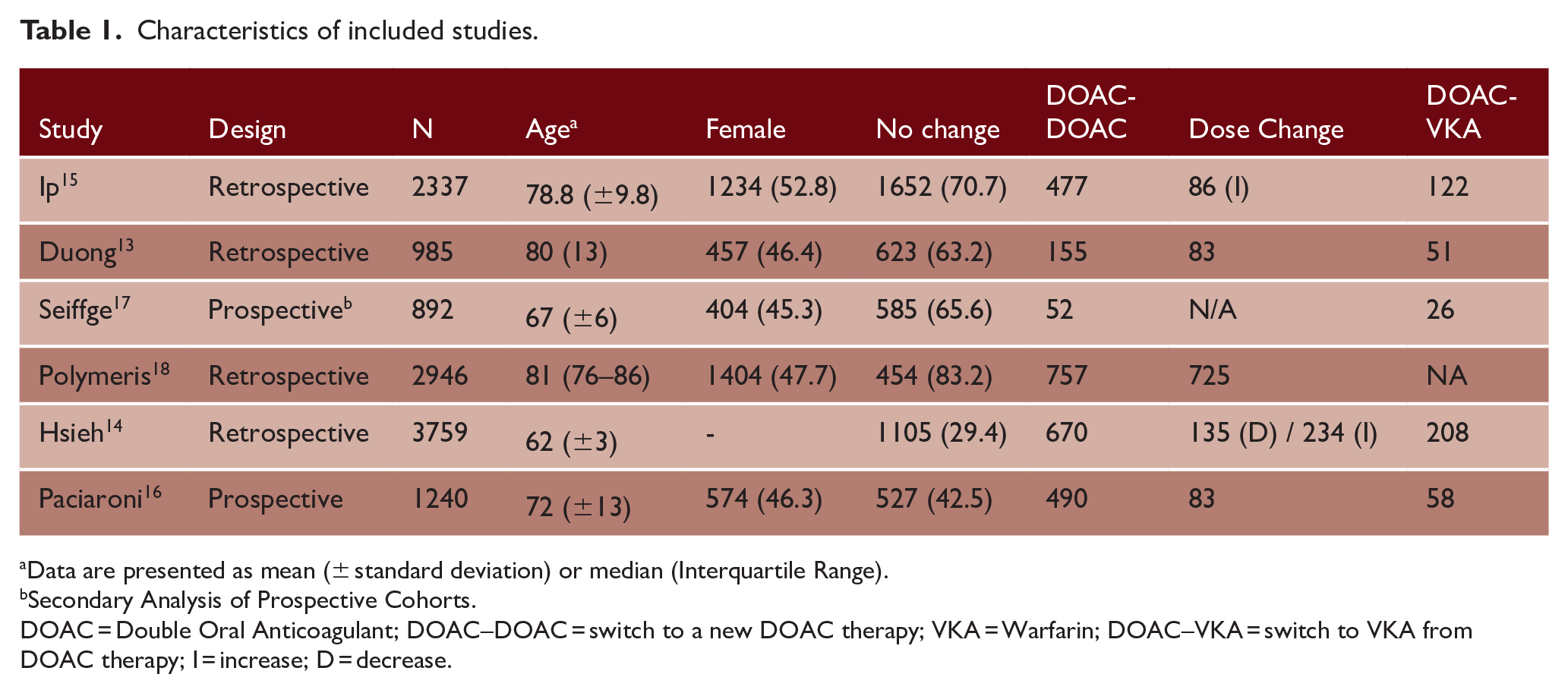
Data are presented as mean (± standard deviation) or median (Interquartile Range).
Secondary Analysis of Prospective Cohorts.
DOAC = Double Oral Anticoagulant; DOAC–DOAC = switch to a new DOAC therapy; VKA = Warfarin; DOAC–VKA = switch to VKA from DOAC therapy; I = increase; D = decrease.
Pooled analysis of included studies
Same DOAC versus warfarin
Four studies compared the same regimen of DOAC and the change to warfarin.13–16 The group that maintained the same DOAC regimen had a significantly decreased risk of ischemic stroke (RR 0.55; 95% CI 0.43–0.70; p < 0.001; I2 = 0%; Figure 2(a)), intracranial hemorrhage (RR 0.37; 95% CI 0.25–0.55; p < 0.001; I2 = 0%; Figure 2(b)), and hemorrhagic events (RR 0.44; 95% CI 0.30–0.63; p < 0.001; I2 = 6%; Figure 2(c)) compared to the warfarin group. Despite the high heterogeneity, warfarin increased the risk of mortality (HR 1.85; 95% CI 1.06–3.24; p = 0.03; I2 = 84%; Figure 2(d)) compared to the same DOAC. Ip et al. 15 reported the mortality rates between the same DOAC and warfarin (30.9% versus 49.5%).
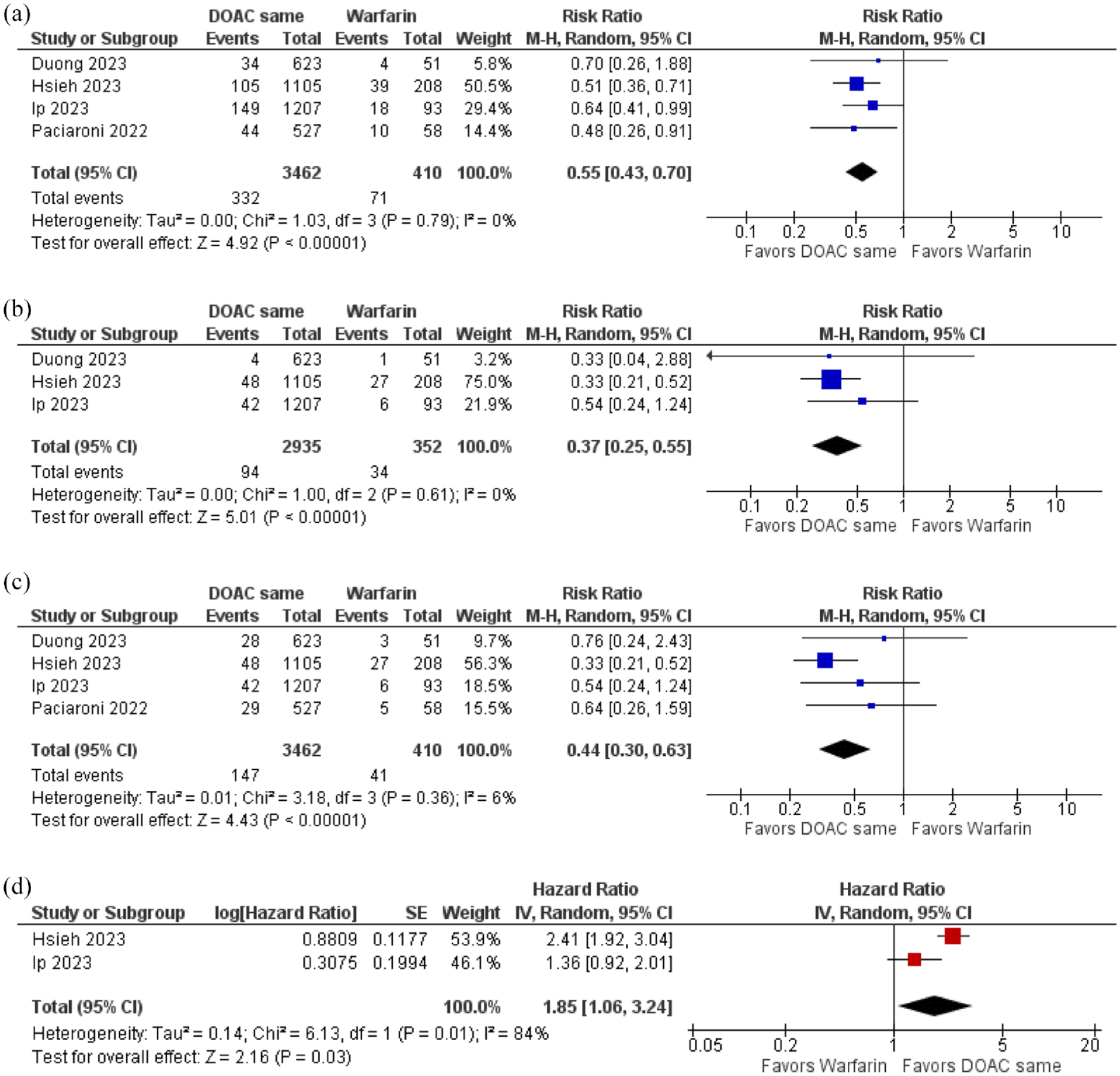
Maintaining the same regimen of DOAC compared to switching to warfarin was associated with a significant reduction of (a) ischemic stroke, (b) intracranial hemorrhage, and (c) hemorrhagic events. In (d), there was an increase in mortality after the stroke event when switching to warfarin compared to maintaining the same regimen of DOAC.
Same DOAC versus another DOAC
Regarding ischemic stroke, switching to another DOAC was not superior to maintaining the same DOAC (RR 0.97; 95% CI 0.66–1.42; p = 0.88; I2 = 74%; Figure 3(a)). There was no difference between the groups concerning intracranial hemorrhage (RR 1.10; 95% CI 0.76–1.60; p = 0.62; I2 = 0%; Figure 3(b)), hemorrhagic events (RR 1.03; 95% CI 0.78–1.37; p = 0.82; I2 = 0%; Figure 3(c)), and mortality (HR 0.98; 95% CI 0.85–1.13; p = 0.78; I2 = 0%; Figure 3(d)). Four studies contributed in these results.13–16 The mortality rate in DOAC same was very similar compared to another DOAC (30.9% versus 31%) in Ip (2023). 15
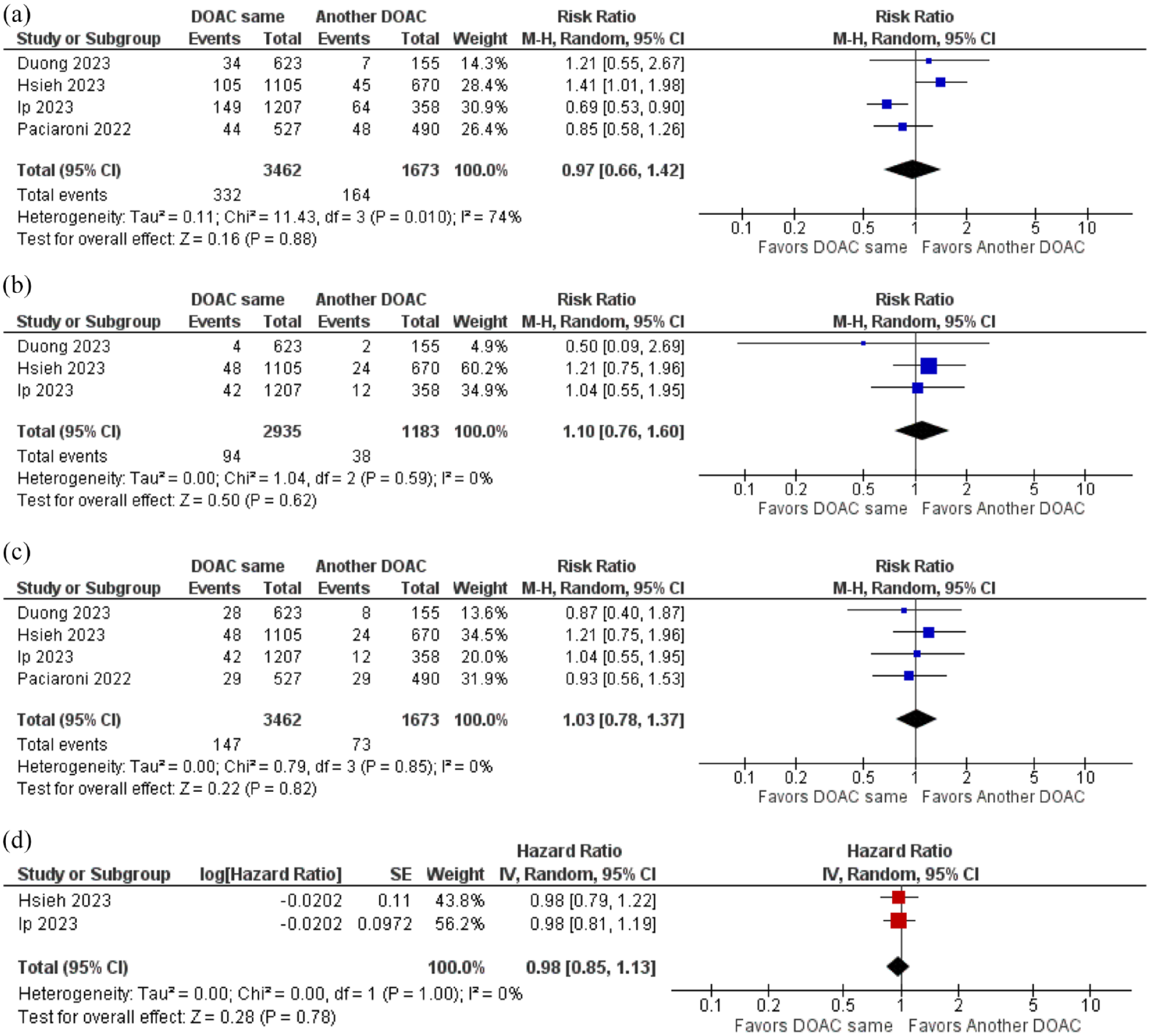
Maintaining the same regimen of DOAC compared to changing to another DOAC did not differ regarding (a) ischemic stroke, (b) intracranial hemorrhage, (c) hemorrhagic events, and (d) mortality after the stroke event.
Same DOAC versus switching DOAC dose
Switching DOAC dose was not superior compared to maintaining DOAC dose regarding ischemic stroke (RR 0.88; 95% CI 0.66–1.18; p = 0.39; I2 = 0%; Figure 4(a)), intracranial hemorrhage (RR 1.04; 95% CI 0.64–1.67; p = 0.88; I2 = 0%; Figure 4(b)), and hemorrhagic events (RR 1.10; 95% CI 0.69–1.74; p = 0.69; I2 = 0%; Figure 4(c)). Three studies reported outcomes in that comparison.13,14,16
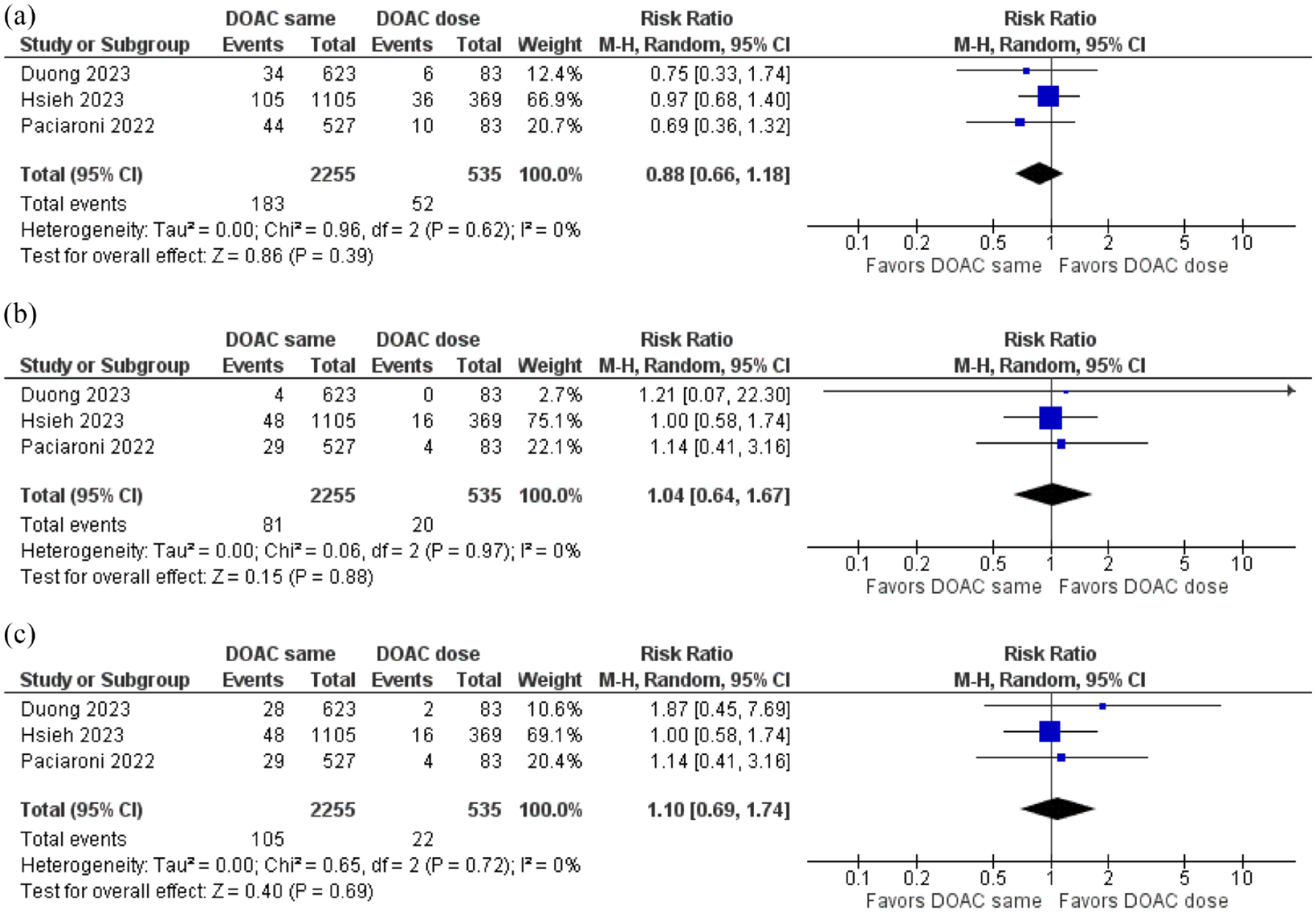
In patients using DOAC, maintaining the same regimen compared to changing DOAC dose did not differ regarding (a) ischemic stroke, (b) intracranial hemorrhage, and (c) hemorrhagic events after the stroke event.
Another DOAC versus warfarin
Four studies reported data comparing switching to another DOAC and switching to warfarin.13–16 Changing to another DOAC was superior to warfarin concerning ischemic stroke (RR 0.57; 95% CI 0.34–0.95; p = 0.03; I2 = 67%; Figure 5(a)). Regarding intracranial hemorrhage (RR 0.33; 95% CI 0.21–0.52; p < 0.001; I2 = 0; Figure 5(b)) and hemorrhagic events (RR 0.46; 95% CI 0.27–0.81; p = 0.007; I2 = 40%; Figure 5(c)), changing the DOAC agent was also better compared switching to warfarin. Ip et al. reported that the mortality rate in another DOAC was lower than warfarin (31% versus 49.5%).
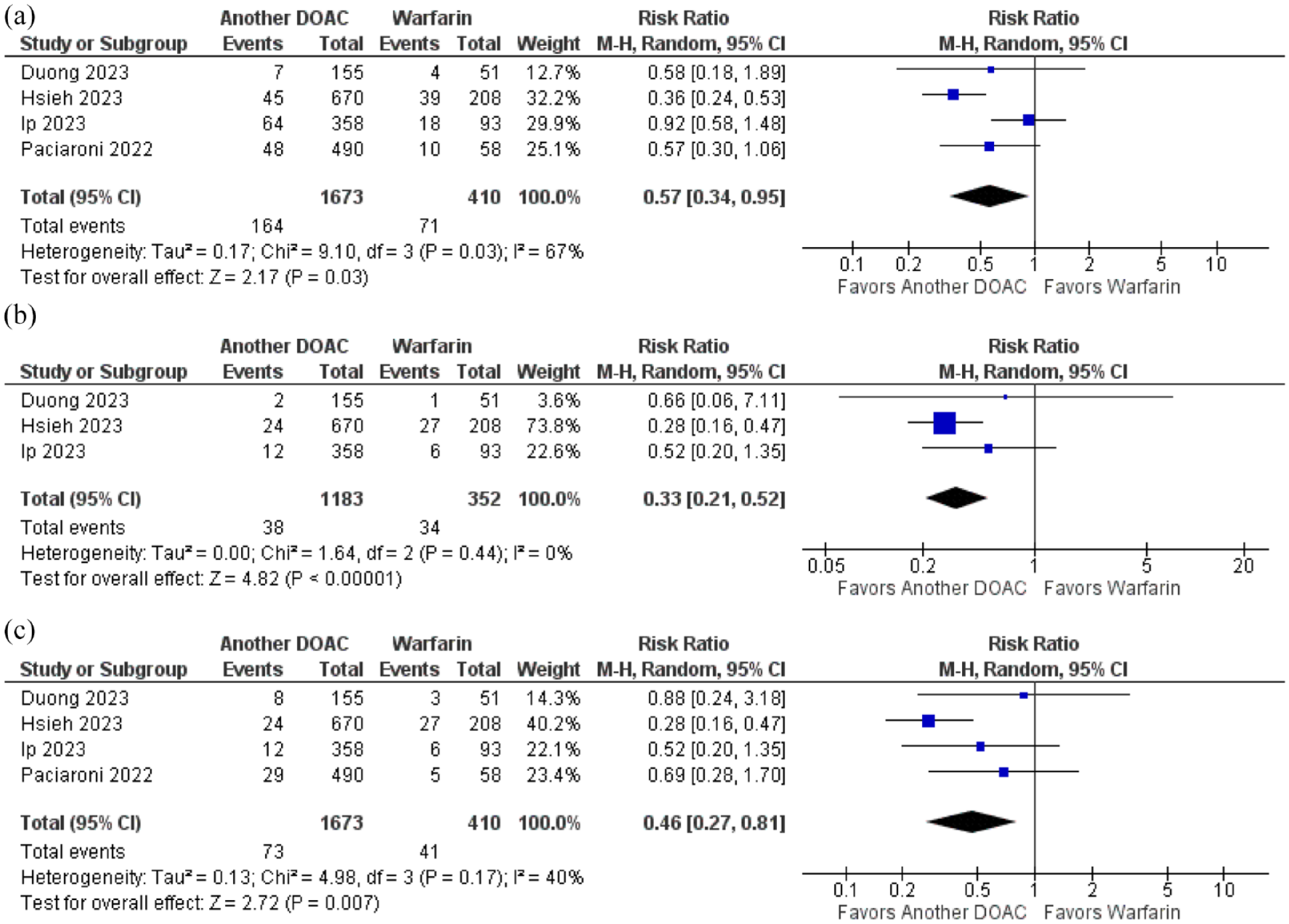
Switching to another DOAC compared to switching to warfarin was associated with a significant reduction of (a) ischemic stroke, (b) intracranial hemorrhage, and (c) hemorrhagic events after the stroke event.
Switching DOAC dose versus switching to warfarin
Three studies compared the switch of DOAC dose and the switch to warfarin.13,14,16 Ischemic stroke (RR 0.58; 95% CI 0.41–0.83; p = 0.003; I2 = 0%; Figure 6(a)) and intracranial hemorrhage (RR 0.36; 95% CI 0.21–0.61; p < 0.001; I2 = 0%; Figure 6(b)) were significantly decreased in DOAC dose change group compared to the warfarin group. Regarding hemorrhagic events, DOAC dose change was also superior (RR 0.37; 95% CI 0.22–0.62; p < 0.001; I2 = 0%; Figure 6(c)) between these treatment groups.
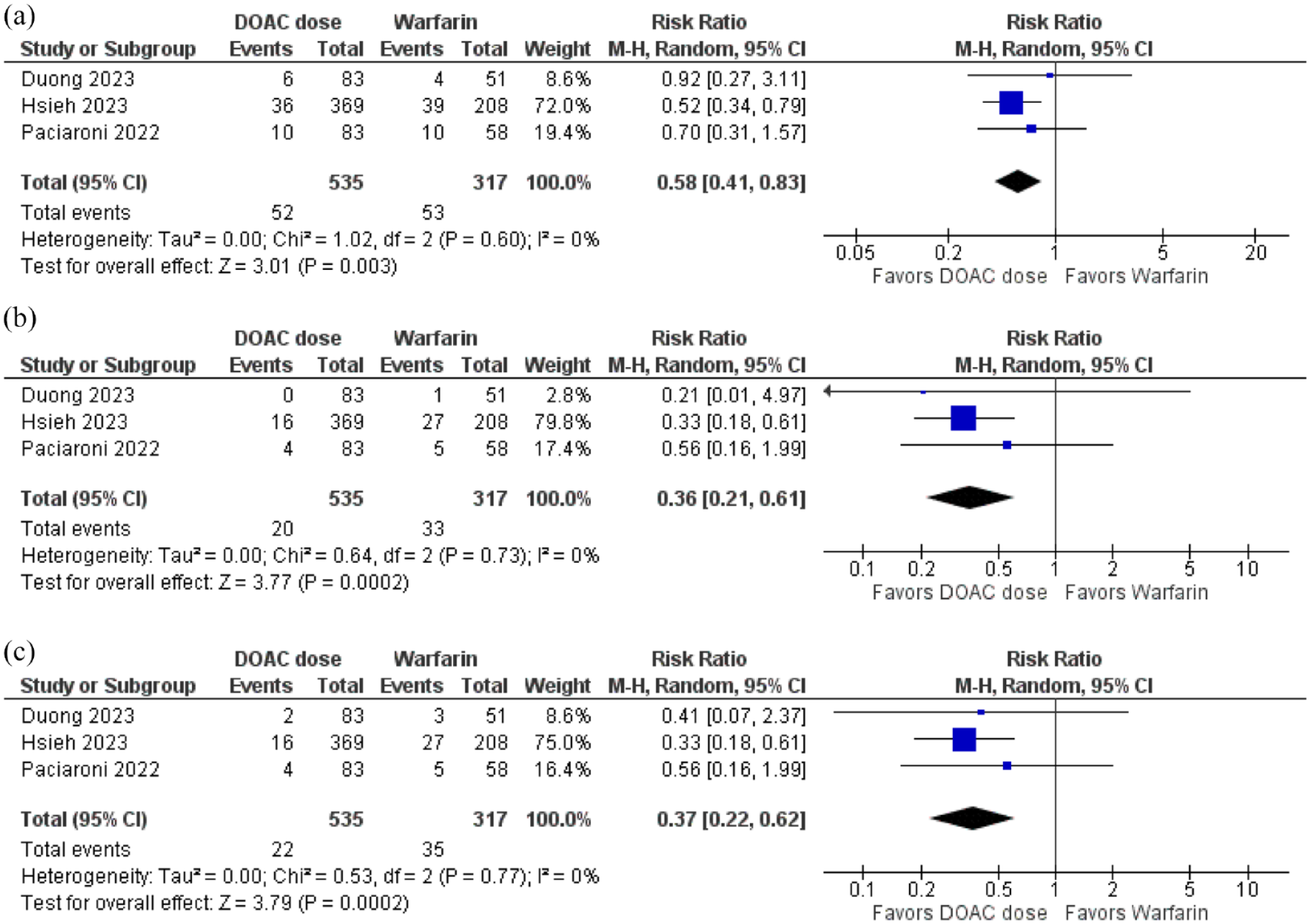
Switching DOAC dose was superior to warfarin concerning decreasing the risk of (a) ischemic stroke, (b) intracranial hemorrhage, and (c) hemorrhagic events after the stroke event.
Switching DOAC dose versus another DOAC
There was no difference between switching DOAC dose and switching DOAC agent regarding ischemic stroke (RR 1.14; 95% CI 0.90–1.45; p = 0.27; I2 = 0%; Figure 7(a)). Intracranial hemorrhage (RR 1.05; 95% CI 0.63–1.77; p = 0.84; I2 = 0%; Figure 7(b)) and hemorrhagic events (RR 0.99; 95% CI 0.60–1.64; p = 0.98; I2 = 0%; Figure 7(c)) also did not differ between these treatment groups. Five studies reported data on these outcomes.13–16,18
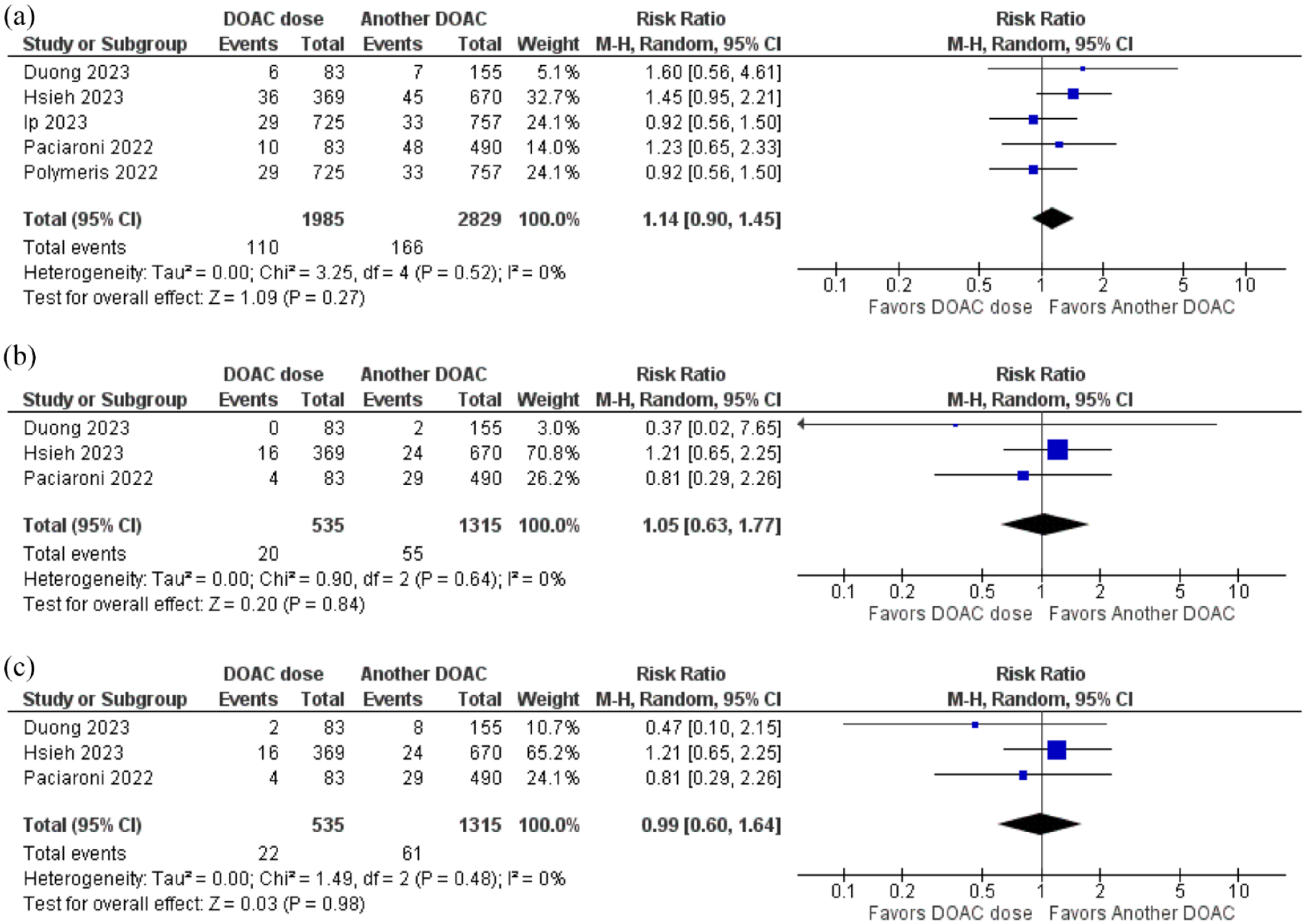
Concerning switching DOAC dose and changing the type of DOAC, there are no differences related to the risk of (a) ischemic stroke, (b) intracranial hemorrhage, and (c) hemorrhagic events after the stroke event.
Risk of bias
Most studies (four out of six) were classified as having a serious overall risk of bias, while one was classified as critical and one as moderate risk. The most significant factors considered in this analysis were indication bias, which notably affected the confounding domain in most studies, and bias in the selection of participants, attributable to the observational design of these studies. Bias in the measurement of outcomes was classified as moderate in all studies due to the potential influence of knowledge of the intervention received on the outcome measure.
Hsieh et al. (2023) presented multiple weaknesses, including an unclear definition of interventions, resulting in ambiguity and a critical bias in the classification of interventions domain. Table 2 presents the risk of bias results for each study along with a summary of each item.
Risk of bias analysis of included studies by The Risk Of Bias In Non-randomized Studies of Intervention (ROBINS-I).
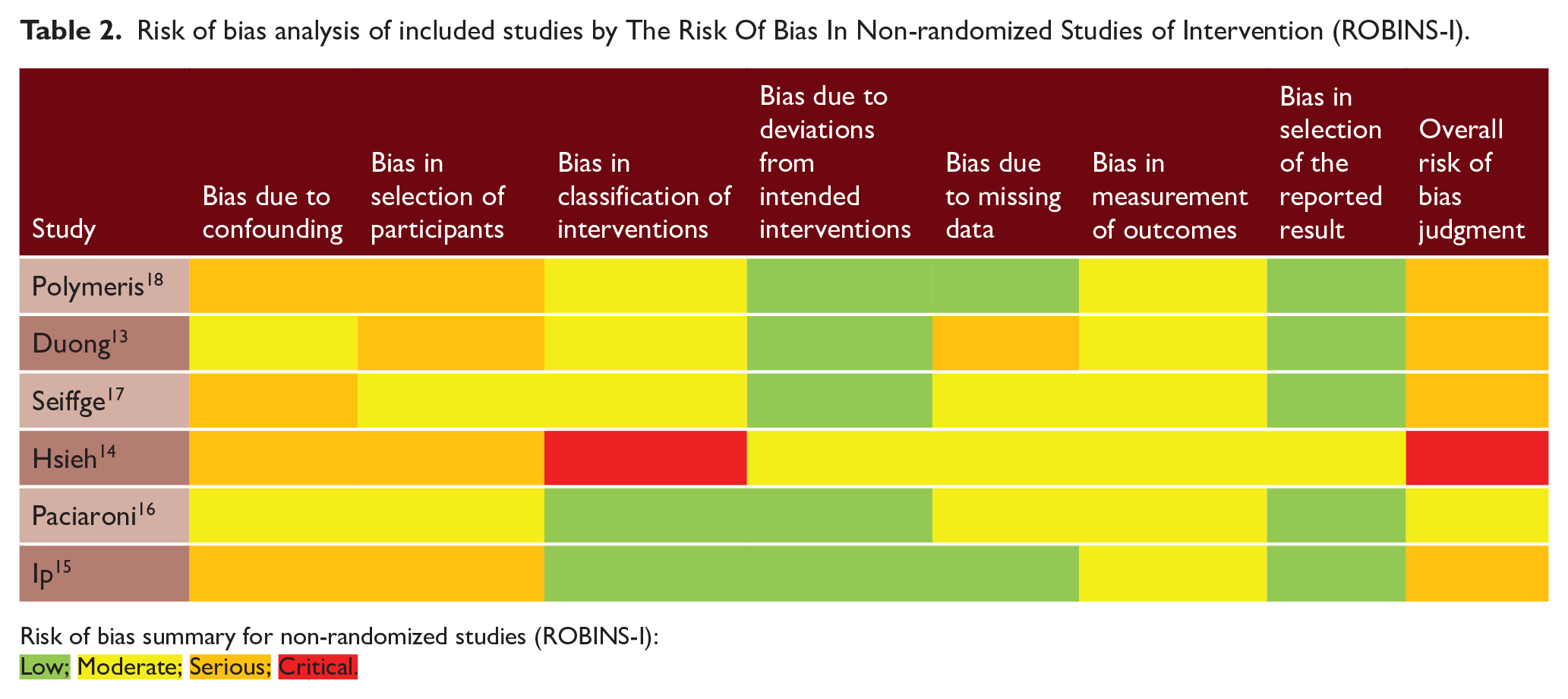
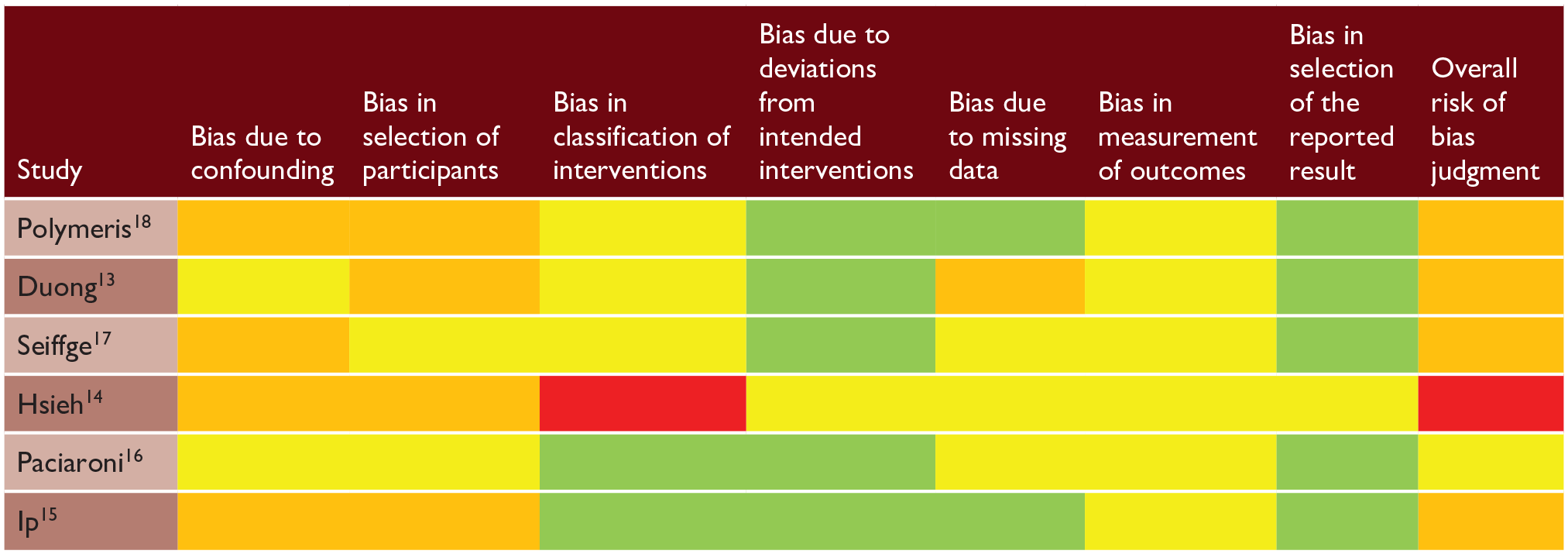
Risk of bias summary for non-randomized studies (ROBINS-I):

Discussion
In this article, we analyzed different anticoagulation strategies for patients presenting with an ischemic stroke while already on DOACs. Overall, switching to warfarin is inferior to most strategies in terms of stroke recurrence, hemorrhagic events, and mortality. Changing the DOAC agent or dose was not superior to maintaining the same drug in any outcome.
Patients who present with an ischemic stroke despite anticoagulation are a frequent challenge. 19 Current guidelines on atrial fibrillation indicate DOACs as the preferred option for anticoagulation in this population. 20 However, even though a specific failure rate is expected, as demonstrated by clinical trials, the clinician often interprets a new stroke as a drug-related treatment failure.
Before considering a new stroke treatment failure, one must carefully assess patient adherence and possible drug interactions.3,21 Rivaroxaban, for instance, must be taken with a meal to achieve optimal bioavailability. 22 All DOACs interact with p-glycoprotein/CYP3A4 inducers, such as phenytoin, carbamazepine, St. John’s wort, or rifampin. Our study shows that changing the DOAC dose or drug usually does not add significant benefit in terms of recurrent stroke reduction. Therefore, enhancing adherence and observing pharmacological interactions might be the most appropriate approach.
Another important aspect before considering treatment failure is to evaluate whether the new stroke could be attributed to a non-atrial fibrillation-related stroke etiology. 19 A large-vessel stenosis or small-vessel-related stroke might require a different secondary prevention strategy.
Provided inadequate adherence, unfavorable drug interactions, and other stroke mechanism have been carefully excluded, and the management of these patients is still uncertain. Although major guidelines hardly mention the subject, previous literature shows very divergent strategies: for example, many German neurologists favored changing between DOACs, while Irish neurologists usually switch to warfarin.23,24
DOACs have been consistently associated with better outcomes and safety profiles than warfarin in multiple randomized trials and meta-analyses.25,26 The results of this meta-analysis further demonstrate that switching to warfarin when a patient presents with an ischemic stroke while on a DOAC is not advisable, as it leads to a higher risk of recurrent stroke, hemorrhagic events, and death.
Two ongoing studies will add relevant information to guide the management of these patients: the INTERCEPT (NCT05723926) and the ELAPSE (NCT05976685). The INTERCEPT is evaluating whether the addition of bilateral carotid filters in addition to oral anticoagulation could reduce recurrent stroke compared to oral anticoagulation only. The ELAPSE is evaluating whether left atrial appendage closure in addition to oral anticoagulation is superior to oral anticoagulation only.
Strengths and limitations
This study has some limitations. There are no head-to-head randomized trials on the topic, which would be the highest standard of evidence. Mortality was evaluated mostly within narrow time windows of 3 months and is likely influenced by the index stroke severity, regardless of the secondary prevention strategy. Furthermore, interventions were not standardized, and DOAC dose changes were not performed uniformly. However, the article presents numerous strengths. It encompasses a large, real-life population, reflecting the actual management of these patients. The results show very small heterogeneity overall. To our knowledge, this is the first meta-analysis on the topic.
Conclusion
For patients with NVAF who present with an ischemic stroke while on DOAC, changing the drug or increasing the dose does not seem to reduce the risk of recurrent stroke. Switching to warfarin was associated with a higher risk of stroke, hemorrhagic events, and mortality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.