
Abstract
Background:
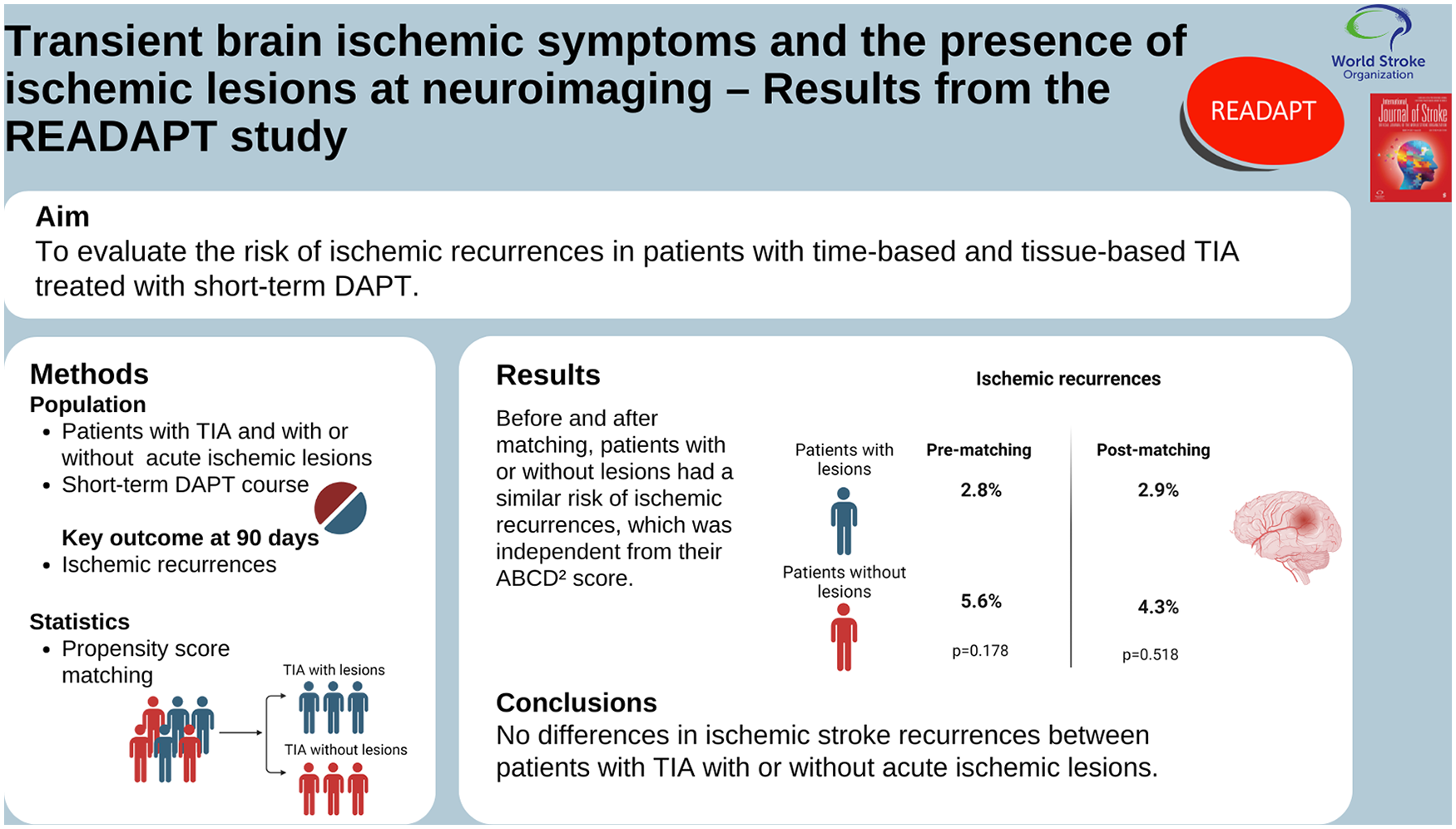
According to the literature, about one third of patients with brain ischemic symptoms lasting <24 h, which are classified as Transient ischemic attacks (TIAs) according to the traditional “time-based” definition, show the presence of acute ischemic lesions at neuroimaging. Recent evidence has shown that the presence of acute ischemic lesions at neuroimaging may impact on the outcome of patients with transient ischemic symptoms treated with dual antiplatelet treatment (DAPT). This uncertainty is even more compelling in recent years as short-term DAPT has become the standard treatment for any non-cardioembolic TIA or minor ischemic stroke.
Methods:
This is a pre-specified subgroup analysis from a prospective multicenter real-world study (READAPT). The analysis included patients with time-based TIA—that is, those with ischemic symptoms lasting <24 h—who started DAPT. In the whole population, we assessed the presence of acute brain ischemic lesions at neuroimaging and their association with the ABCD2 score. To assess the impact of acute brain ischemic lesions on 90-day prognosis, we performed a propensity score matching of patients with and without those lesions. We adopted a primary effectiveness outcome which was a composite of new stroke/TIA events and death due to vascular causes at 90 days.
Results:
We included 517 patients—324 (62.7%) male—with a median (interquartile range—IQR) age of 74 (IQR = 65–81) years; 144 patients (27.9%) had acute brain ischemic lesions at neuroimaging. The proportion of patients with brain ischemic lesions did not vary according to the ABCD2 score. At follow-up, 4 patients with brain ischemic lesions (2.8%) and 21 patients without lesions (5.6%) reported the primary effectiveness outcome, which was similar between the groups before (p = 0.178) and after matching (p = 0.518).
Conclusions:
In our population, patients with transient ischemic symptoms and acute ischemic lesions at brain magnetic resonance imaging (MRI) had a risk of recurrent ischemic events similar to those without lesions. The risk of recurrent ischemic events was low in both groups.
Keywords
Introduction
Transient ischemic attack (TIA) has traditionally been defined as a syndrome of focal neurological symptoms lasting <24 h that can be attributed to a vascular cause. 1 This “time-based” definition of TIA was issued at a time when neuroimaging was not available and has been challenged by the advent of advanced imaging like brain magnetic resonance imaging (MRI). The use of those diagnostic techniques showed that up to one third of patients with “time-based” TIA definition had acute brain ischemic lesions.2 –4 Those findings led to a revision of the definition of TIA as the presence of transient focal ischemic symptoms in the absence of lesions of the central nervous system that could be detected by neuroimaging. 5 This “tissue-based” definition has the advantage of clearly distinguishing patients with TIA from those with a minor ischemic stroke. However, the applicability of this definition depends on the availability of neuroimaging techniques such as brain MRI that more accurately detects ischemic lesions compared with brain computed tomography (CT).
It is unclear whether the presence of acute ischemic lesions on brain MRI can influence the prognosis of patients with transient ischemic symptoms. The short-term prognosis of patients with TIA is usually predicted via clinical scores, such as the ABCD 2 score, which considers patients’ age, blood pressure at onset, clinical symptoms and their duration, and the presence of diabetes mellitus. 6 The ABCD 2 showed a good ability to predict the prognosis of patients with TIA;7,8 however, it does not help in predicting the presence of acute ischemic lesions at neuroimaging. 9 Therefore, we speculate that the presence of acute ischemic lesions does not predict the short-term prognosis of patients with transient ischemic symptoms. This hypothesis is relevant to predict the prognosis of TIA given that some prognostic scores, such as the ABCD 2 -I, include the presence of an acute ischemic lesion at neuroimaging as a criterion for higher risk stratification of recurrent events.10,11
Short-term dual antiplatelet treatment (DAPT) is the treatment of choice for patients with minor ischemic stroke—defined as strokes with a National Institutes of Health Stroke Scale (NIHSS) score ⩽5—or high-risk TIA—defined as TIAs with an ABCD 2 score ⩾4.12 –14 The introduction of DAPT in clinical practice might have changed the short-term prognosis of patients with TIA or minor stroke. Therefore, it is clinically relevant to have real-world data on the outcomes of patients treated with DAPT. Recent evidence suggested that the efficacy of DAPT in preventing recurrent vascular events may be limited to patients with transient symptoms and neuroimaging evidence of acute ischemic lesions. 15 Hence, in the subgroup of patients with transient ischemic symptoms, robust real-world data might help to test the relevance of the “tissue-based” over the “time-based” definition of TIA by assessing the impact of the presence of acute brain ischemic lesions on the prognosis of those patients.
Aims
In this study, we aimed to assess the presence of acute brain ischemic lesions in patients with transient ischemic symptoms treated with DAPT and their impact on short-term prognosis.
Methods
READAPT study
The Real-Life Study on Short-Term Dual Antiplatelet Treatment in Patients With Ischemic Stroke or Transient Ischemic Attack (READAPT—NCT05476081) is an observational prospective multicenter real-world study coordinated by the University of L’Aquila and endorsed by the Italian Stroke Association—Associazione Italiana Ictus (ISA-AII; Supplemental Table 1). The study was carried out according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 16 (Supplemental Table 2) and was approved by the Internal Review Board of the University of L’Aquila in February 2021 with the code 03/2021. All included patients gave written informed consent to participate. Patients’ enrollment took place at 64 Italian Stroke centers spanning from 1 February 2021 to 28 February 2023. Patients aged ⩾18 years were included if they had an acute non-cardioembolic mild-to-moderate ischemic stroke or high-risk TIA and were treated with a short course of DAPT. Exclusion criteria were participation in any interventional randomized controlled trial (RCT) at the time of stroke presentation, ongoing DAPT for endovascular stenting procedures, and presence of conditions potentially affecting the compliance to study procedures. All patients were included as soon as possible after the index event—that is, baseline—and planned to be followed up for the subsequent 90 ± 10 days. A time cutoff from symptom onset to DAPT start was not predetermined; however, investigators were encouraged to start DAPT within 24 h from the index event whenever possible. At the end of the follow-up period, local investigators performed a face-to-face or remote visit. READAPT study procedures and methods of data collection are reported in detail elsewhere. 17
Subgroup analysis for this study
For this study, we selected patients with transient symptoms and defined as ischemic symptoms lasting <24 h with complete return to normal. This definition complies with the traditional “time-based” definition of TIA. 1 We excluded patients lost to follow-up and those who underwent revascularization procedures (intravenous thrombolysis, endovascular thrombectomy), as their inclusion could have influenced clinical outcomes and increased the risk of selection bias. Indeed, as these patients were also excluded from DAPT landmark controlled trials,12 –14 the decisions to prescribe DAPT in such cases were made off-label by local investigators on an individual basis.
Outcomes
The primary effectiveness outcome of the READAPT study was a composite of new stroke (ischemic or hemorrhagic), TIA events, or death due to vascular causes at 90 days. The primary safety outcome was moderate-to-severe bleeding at 90 days. Severity of bleeding events was rated according to The Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Artery (GUSTO) trial definitions. 18 Given the anticipated low risk of secondary effectiveness and safety outcomes of the READAPT study in patients with transient ischemic symptoms, we did not include them in the present subgroup analysis even if they were considered in the main analyses of READAPT. 17
Outcomes occurrence at 90 days was adjudicated by local investigators who completed specific electronic case-report forms. Outcomes were compared between patients with and without ischemic lesions at neuroimaging.
Statistical analysis
Baseline clinical, demographic, and neuroimaging characteristics were compared between patients with and without ischemic lesions. Descriptive statistics are reported as absolute numbers with percentages or medians with interquartile ranges (IQRs) as appropriate. Data were compared using the Wilcoxon test or the Pearson chi-square test, both used to test the significance of differences between two groups for continuous and categorical variables, respectively.
The prevalence of brain ischemic lesions was evaluated according to the ABCD 2 score, both for each score and as a dichotomous variable (ABCD 2 score ⩾4 vs. <4). Prevalence in each ABCD 2 score category was reported as numbers and percentages. Comparisons across each category were reported with chi-square test.
The occurrence of the outcomes at 90 days was reported as absolute number and percentage of patient experiencing at least an outcome event. The risk of outcomes was compared between patients with and without ischemic lesions and was reported using Kaplan–Meier curves. Differences between the two subgroups were tested using log-rank test.
Given the low expected number of short-term outcome events in our population of patients with TIA, we did not plan multivariable analyses or Cox regression to adjust comparisons. However, we performed a propensity score matching with a “nearest-neighbor” method, a 1:1 ratio, and a caliper width of 0.1 by using the following matching variables: age, sex, race, arterial hypertension, diabetes mellitus, modified Rankin Scale (mRS) score before symptom onset, time to DAPT initiation as a dichotomous variable (<24 h vs. ⩾24 h), DAPT loading dose, and brain MRI (performed vs. not performed). Propensity score matching was selected as the most suitable method for generating unbiased comparisons. Indeed, it facilitated direct subject-to-subject matching while simplifying the multidimensional covariate space into a single dimension. Variables used in the matching were pre-specified by the authors as they were anticipated to have an impact on patients’ outcomes. Radiological variables, including leukoaraiosis score and brain MRI findings, were not considered for matching as they were available only for a subset of patients.
All statistical analyses were performed with R software, version 4.2.
Results
Baseline characteristics
Out of the 2278 patients originally included in the READAPT cohort, we included 517 patients with transient symptoms meeting all the inclusion criteria for the present subgroup analysis (Figure 1). Among those patients, 324 (62.7%) were male. The median (IQR) age of the 517 patients was 74 (IQR = 65–81) years. The clinical characteristics of the whole cohort are reported in Table 1. All patients started DAPT within 48 h from symptom onset.
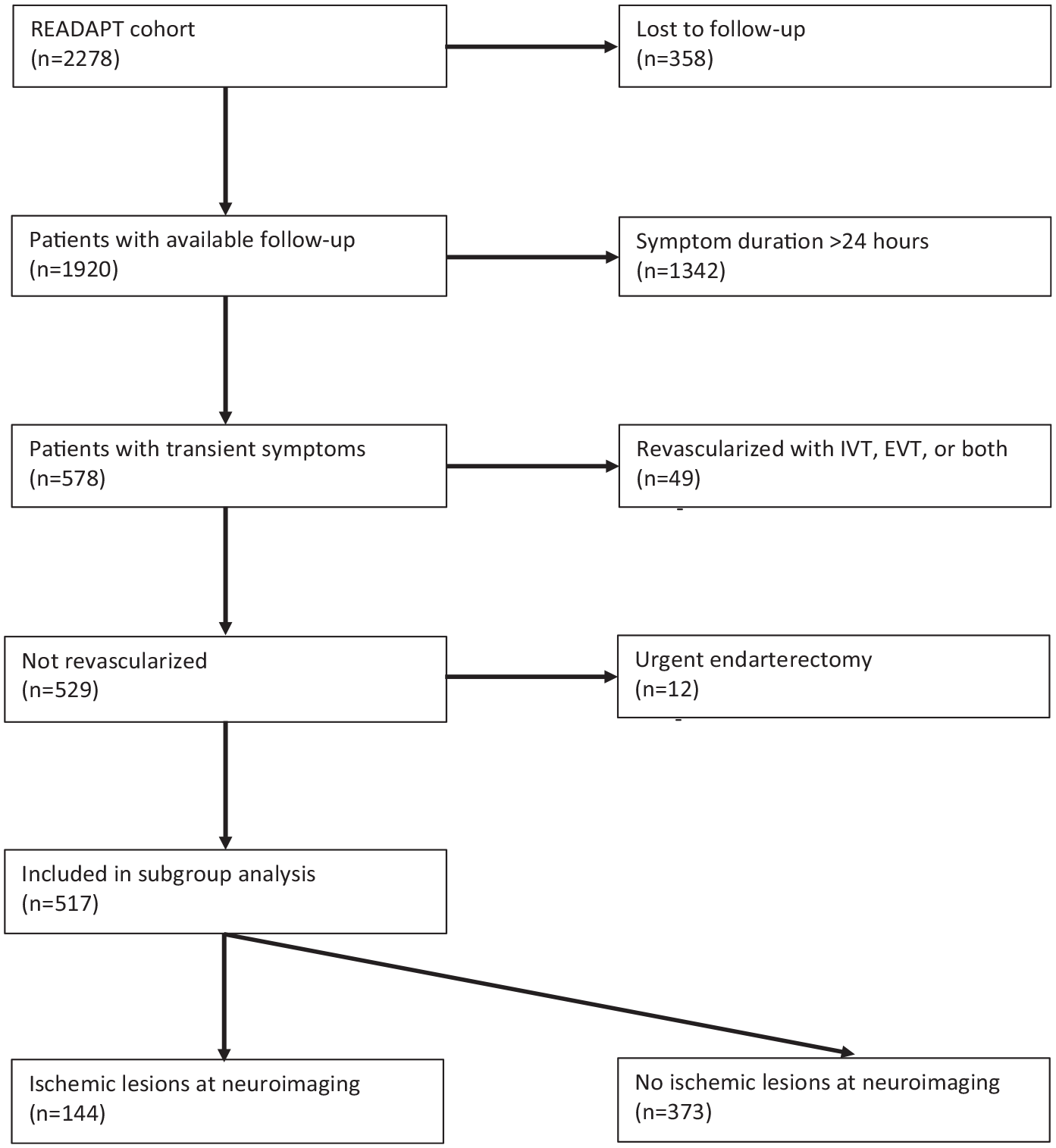
Flowchart of patients’ inclusion.
Baseline characteristics of patients with transient symptoms in the READAPT cohort (n = 517).
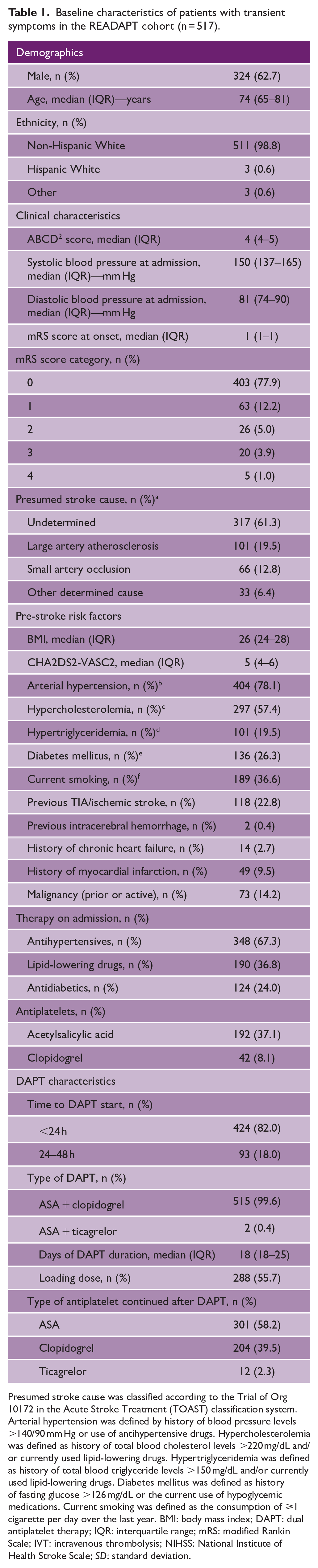
Presumed stroke cause was classified according to the Trial of Org 10172 in the Acute Stroke Treatment (TOAST) classification system. Arterial hypertension was defined by history of blood pressure levels >140/90 mm Hg or use of antihypertensive drugs. Hypercholesterolemia was defined as history of total blood cholesterol levels >220 mg/dL and/or currently used lipid-lowering drugs. Hypertriglyceridemia was defined as history of total blood triglyceride levels >150 mg/dL and/or currently used lipid-lowering drugs. Diabetes mellitus was defined as history of fasting glucose >126 mg/dL or the current use of hypoglycemic medications. Current smoking was defined as the consumption of ⩾1 cigarette per day over the last year. BMI: body mass index; DAPT: dual antiplatelet therapy; IQR: interquartile range; mRS: modified Rankin Scale; IVT: intravenous thrombolysis; NIHSS: National Institute of Health Stroke Scale; SD: standard deviation.
Relationship between ABCD 2 score and the presence of brain ischemic lesions
Overall, 144 patients (27.9%) had brain ischemic lesions at neuroimaging; those lesions were detected at brain MRI in 124 (86.1%) patients and at brain CT in 20 (13.9%) patients. The proportion of patients with brain ischemic lesions did not vary according to the ABCD 2 score, either considering each point of the score as a single category (p = 0.442, Figure 2) or dichotomizing the score in two categories (<4 or ⩾4; p = 0.305; Figure 2).
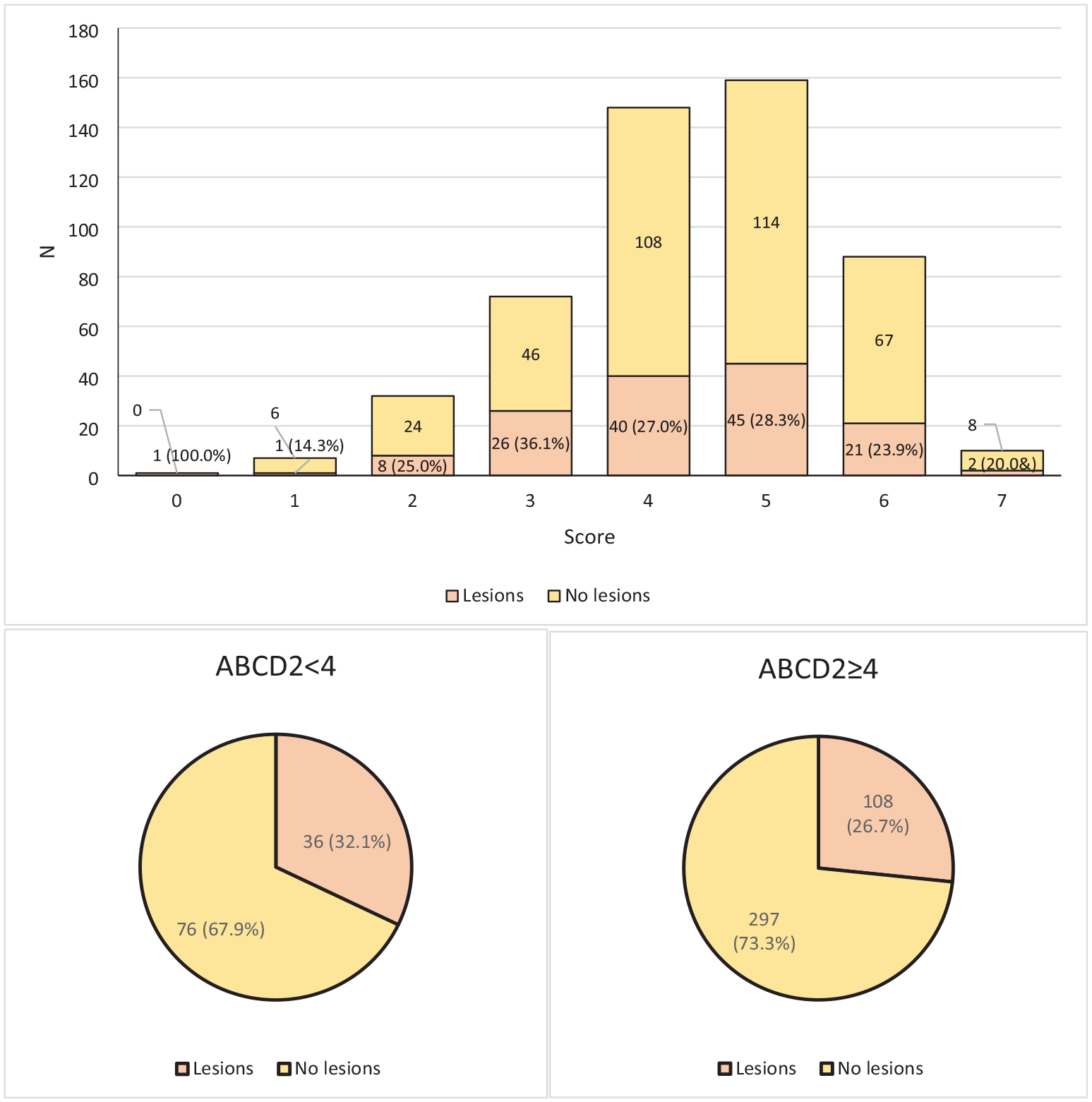
Prevalence of acute ischemic lesions at neuroimaging according to the ABCD 2 score.
Risk of primary outcomes according to the presence of brain ischemic lesions
Out of the 517 follow-up visits, 286 (55.3%) were remote and 231 (44.7%) face-to-face. At 90-day follow-up, 4 patients with brain ischemic lesions (2.8%) and 21 patients without lesions (5.6%) reported the primary effectiveness outcome; the corresponding numbers for the primary safety outcome were 0 and 4 (1.1%). After matching, which resulted in 139 patients for each group, four patients with lesions (2.9%) and six without lesions (4.3%) reported the primary effectiveness outcome, while no patient reported the primary safety outcome. The matched populations were well balanced (Table 2; Supplemental Figure 1), apart from the cause of the index event (Table 2). Nevertheless, standardized mean differences were overall low (Table 2). The cumulative incidence of the primary effectiveness outcome did not differ between patients with and without brain ischemic lesions, either before (p = 0.178) or after matching (p = 0.518; Figure 3). All primary outcome events were recurrent brain ischemic events in the absence of any vascular death.
Baseline characteristics according to the presence of ischemic lesions at neuroimaging, before and after propensity score matching.
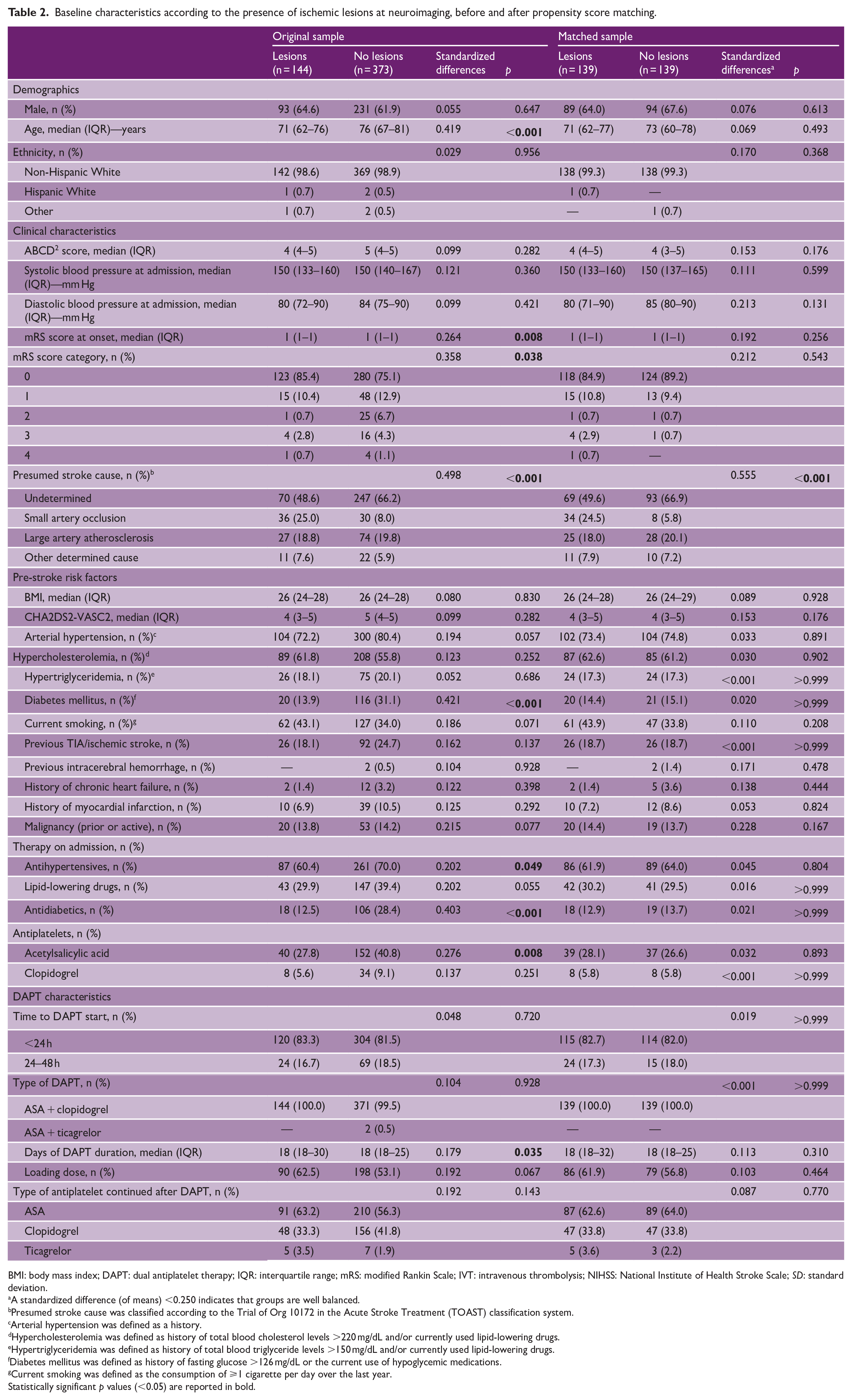
BMI: body mass index; DAPT: dual antiplatelet therapy; IQR: interquartile range; mRS: modified Rankin Scale; IVT: intravenous thrombolysis; NIHSS: National Institute of Health Stroke Scale; SD: standard deviation.
A standardized difference (of means) <0.250 indicates that groups are well balanced.
Presumed stroke cause was classified according to the Trial of Org 10172 in the Acute Stroke Treatment (TOAST) classification system.
Arterial hypertension was defined as a history.
Hypercholesterolemia was defined as history of total blood cholesterol levels >220 mg/dL and/or currently used lipid-lowering drugs.
Hypertriglyceridemia was defined as history of total blood triglyceride levels >150 mg/dL and/or currently used lipid-lowering drugs.
Diabetes mellitus was defined as history of fasting glucose >126 mg/dL or the current use of hypoglycemic medications.
Current smoking was defined as the consumption of ⩾1 cigarette per day over the last year.
Statistically significant p values (<0.05) are reported in bold.
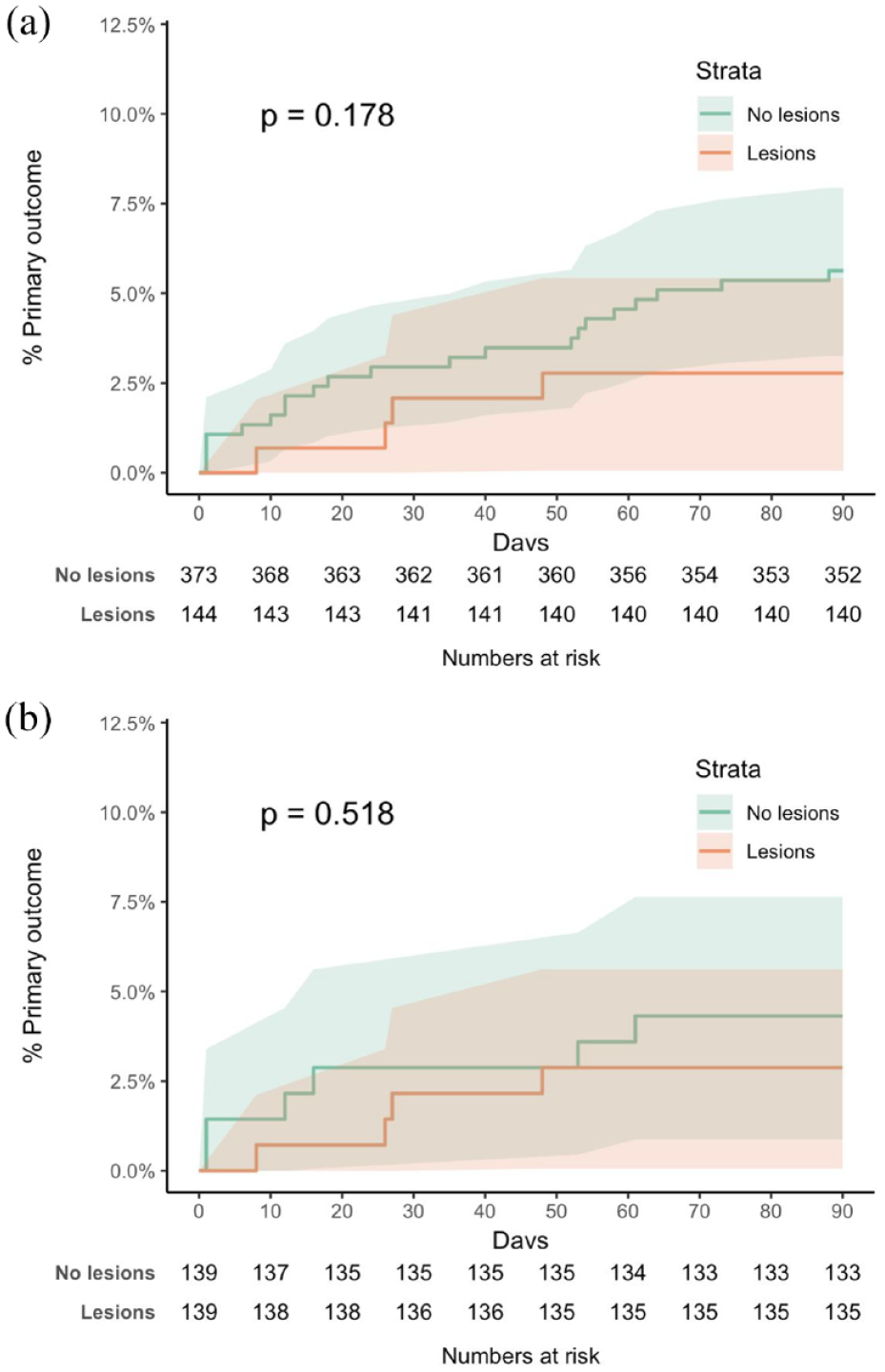
Cumulative incidence curves for the primary efficacy outcome in the two study subgroups before (a) and after (b) propensity score matching.
Discussion
Our main results in patients with transient ischemic symptoms treated with short-term DAPT were the following: (1) the prevalence of brain ischemic lesions at MRI was independent of the ABCD 2 score; (2) the short-term outcome of patients was independent of the presence of brain ischemic lesions.
Our findings are clinically relevant as they shed light on the value of the ABCD 2 score and of the presence of acute ischemic lesions on secondary prevention of brain ischemia. The ABCD 2 score was designed as a simple score to detect factors associated with short-term risk of ischemic stroke. 6 Although the validity of this score has not been solidly demonstrated,7,19 it is a simple tool to distinguish “high-risk” from “low-risk” TIA. Therefore, this score was used in RCTs of DAPT for short-term secondary prevention of ischemic stroke and TIA.12 –14 In clinical practice, where the therapeutic decisions of clinicians might not strictly follow the guidelines, it might happen that even patients with low ABCD 2 score, suggestive of low early risk of ischemic stroke, are treated with DAPT. 17 The discovery of acute ischemic lesions at brain MRI in patients with transient symptoms 3 has led to the incorporation of acute lesions into novel scores, such as the ABCD 2 -I 4 or ABCD 3 -I,10,11,20 with potentially superior ability in predicting early stroke risk compared with ABCD 2 . It has also led to a shift in the definition of ischemic stroke and TIA from “time-based” to “tissue-based” definitions. 5 However, in most clinical practice settings, it is impractical to perform urgent brain MRI in all patients with transient ischemic symptoms to detect brain lesions, so that “time-based” are more frequent than the “tissue-based” diagnoses. 21 In recent years, the impact of DAPT on short-term prevention might have changed the short-term risk of ischemic stroke in patients with TIA and minor ischemic stroke. For all those reasons, it is clinically useful to understand whether the presence of acute brain ischemic lesions has an impact on the prognosis of patients with optimized secondary preventive treatment.
In our real-world population of patients with transient ischemic symptoms, acute ischemic lesions were detected in about one third of patients, in line with previous case series,2,3,22 even if brain MRI was used only in 338/582 (58.1%) patients. Notably, the rate of detection of acute ischemic lesions was independent from the ABCD 2 score (Figure 1), and the presence of acute lesions had no impact on short-term outcomes (Figure 2). Our findings contrast with those of a previous large series of 4574 patients with TIA in which the 7-day risk of ischemic stroke was 7.1% in patients with acute ischemic lesions and 0.4% in those without. 9 Our 90-day risk of recurrent ischemic events was lower than the 7-day risks found in patients with acute ischemic lesions in that previous study, which was performed before the widespread use of DAPT for secondary prevention. Therefore, we speculate that the short-term use of DAPT conferred a benefit in our patients and especially in those with acute lesions, so that the presence of those lesions was not a negative prognostic factor. This hypothesis is corroborated by the overall low rate of recurrent ischemic events in the READAPT population 23 and by the effectiveness of DAPT over single antiplatelet therapy in patients with TIA and positive neuroimaging found in a previous prospective cohort study. 15 Nevertheless, other arguments can explain our findings. First, in our observational study, we cannot exclude that some index events might have been recurrences of previous events, which might have led to an underestimation of recurrences. Besides, we cannot exclude that our population carried an intrinsically low risk of recurrent ischemic events. As we included all patients treated with DAPT in a real-world setting, we included a large proportion of patients with low ABCD 2 score. 17 A subgroup analysis on patients with high ABCD 2 score was prevented by the low number of patients and by the even lower number of patients with recurrent events. Underreporting of recurrent events and underpowering of analyses—as this was an exploratory subgroup analysis without a specific sample size calculation—are further possible explanations for our non-significant findings.
Strengths of our study included its prospective design and the adoption of rigorous procedures to improve the accuracy and quality of collected data, as guaranteed by regular quality check of the READAPT electronic database. Conversely, the study suffered from some relevant limitations. The low number of outcome events probably led us to underpowered analyses. Since this was a multicenter observational study without formal monitoring activities, and most follow-up visits were conducted remotely, some outcomes might have been unreported. In addition, we cannot exclude that some patients with very early (<48 h) recurrent events were included at the time of their first recurrence, which may have reduced the probability of subsequent vascular events. The propensity score matching was not exact and might have hindered residual differences between the two groups. We chose not to perform multidimensional testing or apply inverse probability weighting to avoid the risk of an overfitted model, increased variance, and diminished covariate balance due to the disproportion between patients with and without transient symptoms and the small number of outcome events.
In conclusion, our exploratory subgroup analysis performed in the real-world setting showed that patients with transient ischemic symptoms and acute ischemic lesions at brain MRI had a similar risk of recurrent ischemic events compared with those without lesions. The risk of recurrent ischemic events was low in both groups. The use of DAPT and possibly of other effective secondary preventive measures might have had a positive role in the short-term prognosis of those patients.
Supplemental Material
sj-docx-1-wso-10.1177_17474930241302691 – Supplemental material for Transient brain ischemic symptoms and the presence of ischemic lesions at neuroimaging: Results from the READAPT study
Supplemental material, sj-docx-1-wso-10.1177_17474930241302691 for Transient brain ischemic symptoms and the presence of ischemic lesions at neuroimaging: Results from the READAPT study by Raffaele Ornello, Matteo Foschi, Federico De Santis, Michele Romoli, Tiziana Tassinari, Valentina Saia, Silvia Cenciarelli, Chiara Bedetti, Chiara Padiglioni, Bruno Censori, Valentina Puglisi, Luisa Vinciguerra, Maria Guarino, Valentina Barone, Maria Luisa Zedde, Ilaria Grisendi, Marina Diomedi, Maria Rosaria Bagnato, Marco Petruzzellis, Domenico Maria Mezzapesa, Pietro Di Viesti, Vincenzo Inchingolo, Manuel Cappellari, Mara Zenorini, Paolo Candelaresi, Vincenzo Andreone, Giuseppe Rinaldi, Alessandra Bavaro, Anna Cavallini, Stefan Moraru, Pietro Querzani, Valeria Terruso, Marina Mannino, Umberto Scoditti, Alessandro Pezzini, Giovanni Frisullo, Francesco Muscia, Maurizio Paciaroni, Maria Giulia Mosconi, Andrea Zini, Ruggiero Leone, Carmela Palmieri, Letizia Maria Cupini, Michela Marcon, Rossana Tassi, Enzo Sanzaro, Cristina Paci, Giovanna Viticchi, Daniele Orsucci, Anne Falcou, Susanna Diamanti, Roberto Tarletti, Patrizia Nencini, Eugenia Rota, Federica Nicoletta Sepe, Delfina Ferrandi, Luigi Caputi, Gino Volpi, Salvatore La Spada, Mario Beccia, Claudia Rinaldi, Vincenzo Mastrangelo, Francesco Di Blasio, Paolo Invernizzi, Giuseppe Pelliccioni, Maria Vittoria De Angelis, Laura Bonanni, Giampietro Ruzza, Emanuele Alessandro Caggia, Monia Russo, Agnese Tonon, Maria Cristina Acciarri, Sabrina Anticoli, Cinzia Roberti, Giovanni Manobianca, Gaspare Scaglione, Francesca Pistoia, Alberto Fortini, Antonella De Boni, Alessandra Sanna, Alberto Chiti, Leonardo Barbarini, Maela Masato, Massimo Del Sette, Francesco Passarelli, Maria Roberta Bongioanni, Danilo Toni, Stefano Ricci, Simona Sacco and Eleonora De Matteis in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.Z. reports compensation from Angels Initiative, Boehringer-Ingelheim, and Daiichi Sankyo for consultant services; from Angels Initiative, Boehringer-Ingelheim, and CSL Behring for speaking honoraria or other education services; from Daiichi Sankyo for meeting; from Bayer and Astra Zeneca for participation on a Data Safety, Monitoring Board or Advisory Board; and he is member of ESO guidelines, ISA-AII guidelines, and IRETAS steering committee. R.O. reports grants from Novartis and Allergan; compensation from Teva Pharmaceutical Industries, Eli Lilly and Company, and Novartis for other services; and travel support from Teva Pharmaceutical Industries. S.S. reports compensation from Novartis, NovoNordisk, Allergan, AstraZeneca, Pfizer Canada, Inc., Eli Lilly and Company, Teva Pharmaceutical Industries, H. Lundbeck A/S, and Abbott Canada for consultant services; employment by Università degli Studi dell’Aquila; and compensation from Novartis for other services. MP reports compensation from Daiichi Sankyo Company, Bristol Myers Squibb, Bayer, and Pfizer Canada, Inc., for consultant services. DT reports compensation from Alexion, Astra Zeneca, Medtronic, and Pfizer for consultant services and participation on a Data Safety, Monitoring Board or Advisory Board. The other authors report no conflicts.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
Data from this study are available from the corresponding author upon reasonable request.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.