
Abstract
Background:
Short-term dual antiplatelet treatment (DAPT) is superior to single antiplatelet treatment (SAPT) for secondary prevention in non-cardioembolic minor ischemic stroke and high-risk transient ischemic attack (TIA). As the real-world use of DAPT is broader than in trials, it is important to clarify its benefit/risk profile in a diverse population.
Methods:
Post hoc analysis of prospectively collected data from the READAPT cohort and three prospective stroke registries including patients with mild-to-moderate (National Institute of Health Stroke Scale (NIHSS) score 0–10) ischemic stroke receiving early DAPT or SAPT. The primary effectiveness outcome was 90-day return to pre-stroke neurological functioning using modified Rankin Scale (mRS) score. Secondary effectiveness outcomes were 90-day mRS shift, new ischemic stroke/TIA, vascular and all-cause death, 24 h early neurological improvement or deterioration. The safety outcome was 90-day intracranial hemorrhage.
Results:
We matched 1008 patients treated with DAPT and 1008 treated with SAPT. Compared to SAPT, patients treated with DAPT showed higher likelihood of 90-day primary effectiveness outcome (87.5% vs. 84.4%, risk difference 3.1% (95% confidence interval (CI): 0.1%–6.1%); p = 0.047, risk ratio 1.03 (95% CI: 1.01–1.07); p = 0.043) and higher rate of 24-h early neurological improvement (25.3% vs. 15.4%, risk difference 9.9% (95% CI: 6.4%–13.4%); p < 0.001, risk ratio 1.65 (95% CI: 1.37–1.97); p < 0.001). No differences were observed for other study outcomes. Subgroup analysis confirmed benefit of DAPT over SAPT for primary effectiveness outcome in patients with moderate stroke, those treated with intravenous thrombolysis, and those who received antiplatelet loading dose.
Conclusion:
Our findings suggest that DAPT use might be safe and more effective than SAPT even in the real world and in patients who do not strictly fulfill the criteria of landmark large clinical trials.
Introduction
Short-term dual antiplatelet treatment (DAPT) is the cornerstone of secondary prevention for non-cardioembolic minor ischemic stroke or high-risk transient ischemic attack (TIA).1 –4 However, the use of DAPT often extends beyond the indications established by the landmark trials, encompassing patients with moderate stroke severity, higher pre-stroke disability, or those who have undergone acute reperfusion therapies.5,6 Recently, the Antiplatelet Therapy in Acute Mild to Moderate Ischemic Stroke (ATAMIS) randomized trial suggested that DAPT with aspirin plus clopidogrel might be superior to aspirin alone in reducing the rate of early neurological deterioration (END) in patients with a baseline National Institute of Health Stroke Scale (NIHSS) score ranging from 4 to 10. 7 However, there was no significant difference between the two treatment options in terms of 90-day functional recovery and in the other efficacy outcomes (i.e. new stroke or other vascular events, vascular and all-cause mortality). 7 Furthermore, the ATAMIS trial enrolled mostly patients with baseline NIHSS 4–7 (82.8%, median NIHSS 5 (interquartile range (IQR) 4–6)). 7 On another hand, DAPT randomized controlled trials included patients with lower baseline NIHSS (ranging from 0 to 3 for the Platelet-Oriented Inhibition in New TIA and minor ischemic stroke (POINT) 2 and Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events (CHANCE) 1 trials, and from 0 to 5 for The Acute Stroke or Transient Ischemic Attack Treated with Ticagrelor and aspirin for Prevention of Stroke and Death (THALES) 3 trial). Overall, there is a paucity of real-world data on DAPT versus SAPT outcomes in patients with mild-to-moderate stroke, which are crucial for understanding how treatment performs outside the randomized controlled settings. In our study we aimed to compare outcomes of non-cardioembolic mild-to-moderate ischemic stroke patients treated with early short-term DAPT versus SAPT in a real-world setting.
Methods
Study design
This is a post hoc analysis of prospectively collected data. This study combined data from acute ischemic stroke patients enrolled in the prospective, observational, multicentric “Real-Life Study on Short-Term Dual Antiplatelet Treatment in Patients With Ischemic Stroke or Transient Ischemic Attack” (READAPT, NCT05476081) cohort with data from three single-center prospective stroke registries. The READAPT study prospectively recruited patients with acute non-cardioembolic stroke or TIA aged ⩾18 years and treated with DAPT across 64 Italian stroke centers from 1 February 2021 to 28 February 2023. Study procedures have been detailed in prior publications.5,6 Local stroke registries included ischemic stroke patients aged ⩾18 years admitted to three Italian stroke centers (S.Orsola-Malpighi Hospital of Bologna (BO), S. Maria della Misericordia Hospital of Perugia (PG), and Udine University Hospital (UD)) from the date of the registry inception (BO 2010, PG 2003, UD 2018).8 –10 Demographics (age and sex), medical history (cardiovascular risk factors), clinical information (pre-stroke modified Rankin Scale score (mRS), stroke severity and presumed cause, concomitant medications), and occurrence of 90-day outcomes were prospectively collected.
Data extraction and study population
We extracted from the READAPT cohort and local registries patients with mild-to-moderate (NIHSS 0–10) non-cardioembolic ischemic stroke in June 2024. We selected patients with a baseline NIHSS score of up to 10 to evaluate the real-world benefit-risk profile of DAPT across the full spectrum of stroke severity, where previous trials1 –4,7 demonstrated its superiority over SAPT. To minimize selection bias in the prescription of DAPT/SAPT, we extracted from local stroke registries only data from patients treated with SAPT who were enrolled from 1 January 2018, and up to the implementation of international guidelines11,12 recommending DAPT for all minor strokes and high-risk TIA (31 December 2020). Patients were eligible for the study analysis if they (1) had stroke symptom duration ⩾24 h or <24 h with evidence of recent ischemic lesion(s) on neuroimaging (brain non-contrast computed tomography (NCCT) or magnetic resonance imaging (MRI)), (2) initiated DAPT or SAPT within 24 h of symptoms onset (or 48 h if underwent hyperacute treatment), and (3) had follow-up visit within 80 ± 10 days of the index event. Conversely, exclusion criteria included urgent carotid endarterectomy or stenting during the follow-up period, incomplete follow-up information (⩾1 outcome not recorded), early discontinuation of DAPT (<21 days) or SAPT (before the date of follow-up visit) due to a condition requiring anticoagulation. This latter exclusion was based on concerns about the potential confounding effect of anticoagulation-related bleeding risks on the safety assessment of DAPT and SAPT.
Propensity score matching
Propensity scores were calculated based on a multivariable logistic regression model, which included demographics (age and sex), risk factors (arterial hypertension, diabetes, dyslipidemia, current smoking), pre-stroke mRS, stroke severity (NIHSS) and presumed cause, symptoms duration, hyperacute treatment, DAPT/SAPT loading dose. Patients treated with DAPT were matched with those treated with SAPT in a 1:1 ratio and within 0.2 × standard deviation (SD) of the logit of the propensity score by using a greedy nearest neighbor matching without replacement. The overall quality of the matching was evaluated by comparing the standardized difference of means and the ratio of the variances between the propensity scores of treatment groups and by inspecting graphics of propensity scores, and covariates balance distributions between the matched samples.
Outcomes
The primary effectiveness outcome was the return to baseline neurological functioning at 90 days, as defined by a mRS score of 0–1 in patients with pre-stroke mRS < 2 or by the 90-day return to the pre-stroke mRS score in those with baseline mRS ⩾ 2. The secondary effectiveness outcomes included the 90-day ordinal shift of mRS, 24 h early neurological improvement (ENI, decrease of 2 or more points in the NIHSS score) or END (increase of 2 or more points in the NIHSS score not due to cerebral hemorrhage), 90-day new stroke/TIA, vascular (death due to stroke, systemic hemorrhage, myocardial infarction, congestive heart failure, pulmonary embolism, sudden death or arrhythmia) and all-cause mortality. The safety outcome was 90-day intracranial hemorrhage as defined by any category of the Heidelberg bleeding classification system. 13
Statistical analysis
Categorical variables were presented as number and percentage, continuous as mean and SD or median and IQR according to distribution. For the primary effectiveness outcome, we calculated the risk difference and ratio of 90-day return to pre-stroke neurological functioning between the DAPT and SAPT groups with the two-sided 95% confidence intervals (CIs). For the secondary effectiveness outcomes, the 90-day ordinal distribution of mRS scores was compared using an ordinal generalized linear model, and results were presented as odds ratio (OR) with 95% CIs. Risk differences and ratios (95% CIs) between groups were calculated for 24 h ENI or END. The time-to-event 90-day risk of new stroke/TIA, vascular and all-cause death was compared using Cox regression and the corresponding treatment effect was presented as hazard ratio (HR) and 95% CIs. For the safety outcome, we calculated risk difference and ratio with 95% CIs. All outcomes were analyzed separately also in the unmatched cohort. Subgroup analysis of the primary effectiveness outcome was performed calculating risk differences of DAPT versus SAPT in 11 prespecified subgroups (age (<65 or ⩾65 years), sex (females or males), NIHSS (0–5 or 6–10), presumed stroke cause, pre-stroke mRS (<2 or ⩾2), symptoms duration (⩾ 24 h or <24 h), intravenous thrombolysis (IVT), endovascular thrombectomy (EVT), history of diabetes, SAPT/DAPT loading dose (prescription of ⩾300 mg for aspirin/clopidogrel, ⩾180 mg for ticagrelor)). Finally, we conducted a sensitivity analysis within the overall cohort comparing the 90-day risk of new stroke or TIA and the 24 h incidence of END, between DAPT and SAPT in patients with baseline NIHSS scores 0–3 and 4–10, respectively, to align with the main outcomes and stroke severity of the populations in the POINT 3 and ATAMIS 7 trials. All statistical analyses were performed using R software, version 4.2.0. A two-sided p value less than 0.05 was considered statistically significant.
Results
A total of 2908 patients with mild-to-moderate non-cardioembolic stroke were included in the analysis, of whom 1836 (63.1%) were treated DAPT and 1072 (36.9%) with SAPT. The number of excluded patients with reasons is reported in the study flowchart (Figure 1). No missing data were recorded in the variables used to calculate the propensity scores. We paired 1008 DAPT and 1008 SAPT patients. Patients treated with DAPT mostly received aspirin plus clopidogrel (99.7%) for a median time of 21 days (IQR 21–30). Conversely, patients treated with SAPT were mostly treated with aspirin (71.9%) or clopidogrel (27.1%). Measures of balance diagnosis indicated that the samples were adequately matched, with a standardized difference of the propensity scores means between groups of 0.17 (good balance <0.25), ratio of variances of propensity scores 1.10 (good balance from 0.5 to 2). 14 Graphics of propensity scores and covariates balance distributions between the matched samples confirmed a good overall quality of the matching (Supplemental Figures 1 and 2). The comparison of baseline characteristics further supported the good balance of our matched samples with a standardized difference of the propensity scores <0.25 in all variables (Table 1).
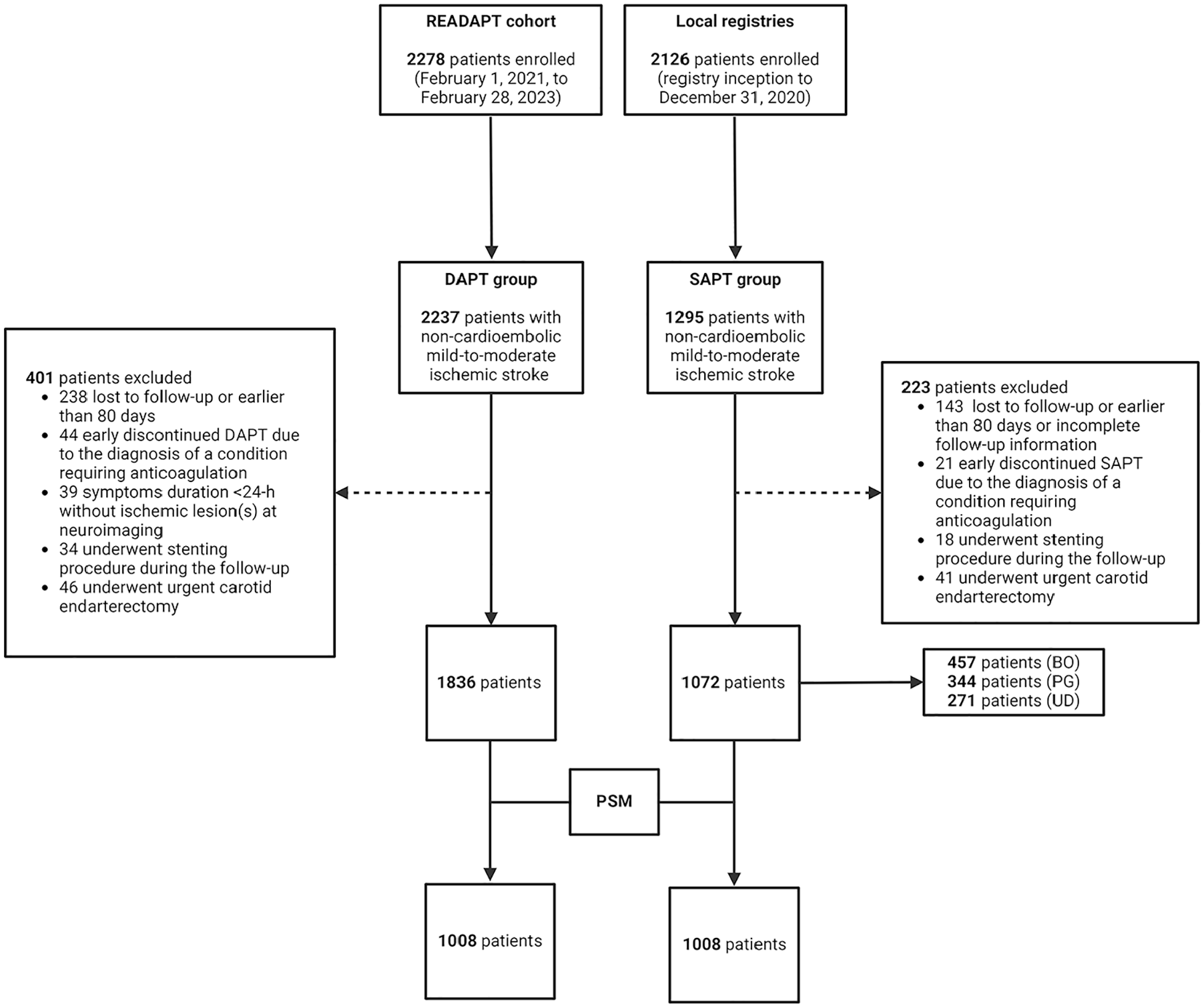
Study flowchart. BO: Bologna; DAPT: dual antiplatelet treatment; PG: Perugia; PSM: propensity score matching; SAPT: single antiplatelet treatment; UD: Udine.
Baseline characteristics.
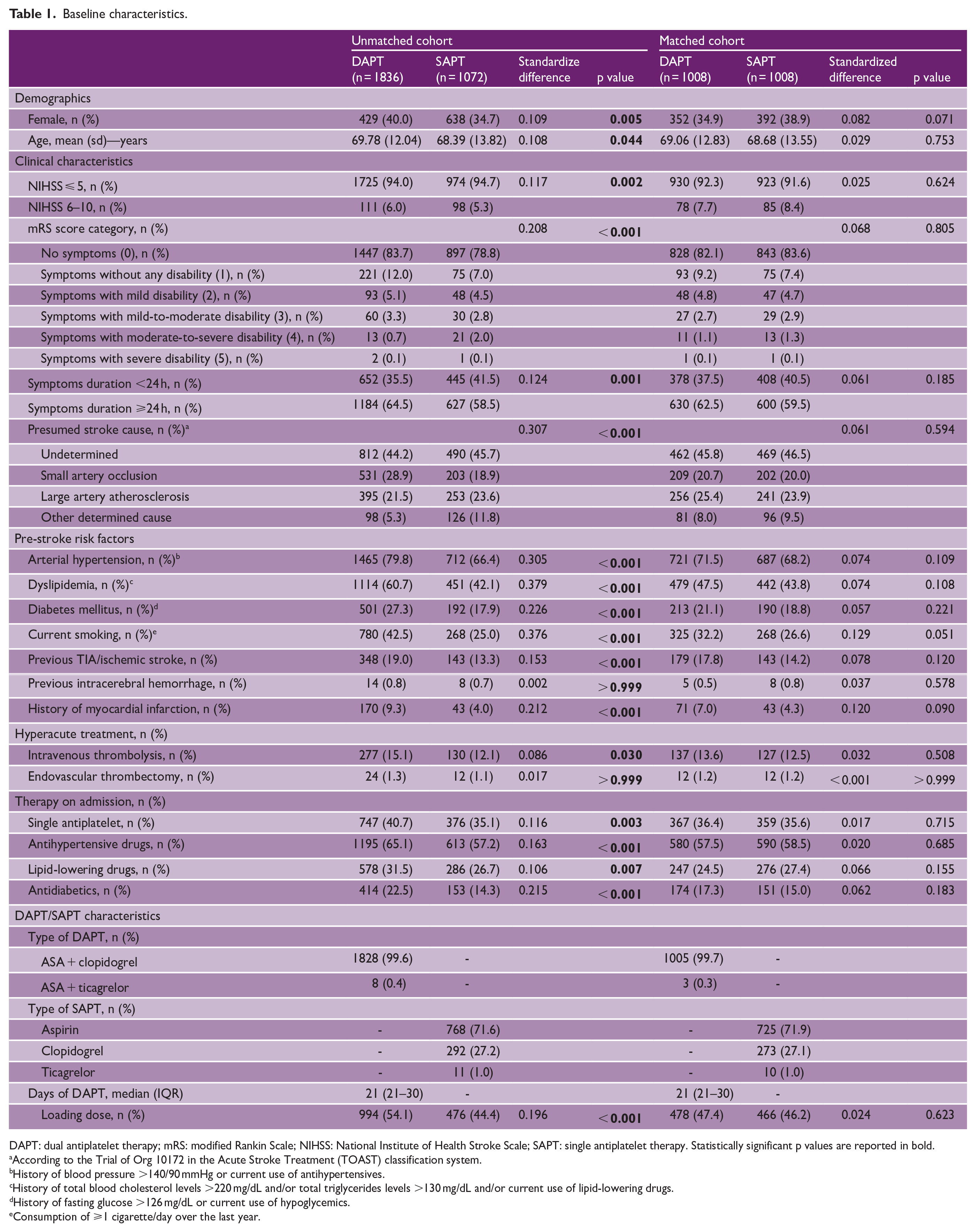
DAPT: dual antiplatelet therapy; mRS: modified Rankin Scale; NIHSS: National Institute of Health Stroke Scale; SAPT: single antiplatelet therapy. Statistically significant p values are reported in bold.
According to the Trial of Org 10172 in the Acute Stroke Treatment (TOAST) classification system.
History of blood pressure >140/90 mmHg or current use of antihypertensives.
History of total blood cholesterol levels >220 mg/dL and/or total triglycerides levels >130 mg/dL and/or current use of lipid-lowering drugs.
History of fasting glucose >126 mg/dL or current use of hypoglycemics.
Consumption of ⩾1 cigarette/day over the last year.
Primary effectiveness outcome
The percentage of patients returning to pre-stroke neurological functioning at 90 days was 87.5% in the DAPT group and 84.4% in the SAPT group. We found significant risk difference (3.1% (95% CI: 0.1%–6.1%); p = 0.047) and ratio (1.03 (95% CI: 1.01–1.07); p = 0.043) between the two groups in the rate of 90 day primary outcome (Table 2). Results of primary effectiveness outcome comparison in the unmatched cohort are displayed in Supplemental Table 1. Although the percentage of patients who returned to pre-stroke neurological functioning at 90 days was slightly higher in patients treated with DAPT (87.2%) versus SAPT (84.6%), statistical significance was not reached in the unmatched cohort (risk difference 2.6% (-0.1%–5.2%) risk ratio 1.03 (0.99–1.06) (Supplemental Table 1).
Study outcomes in the matched cohort.
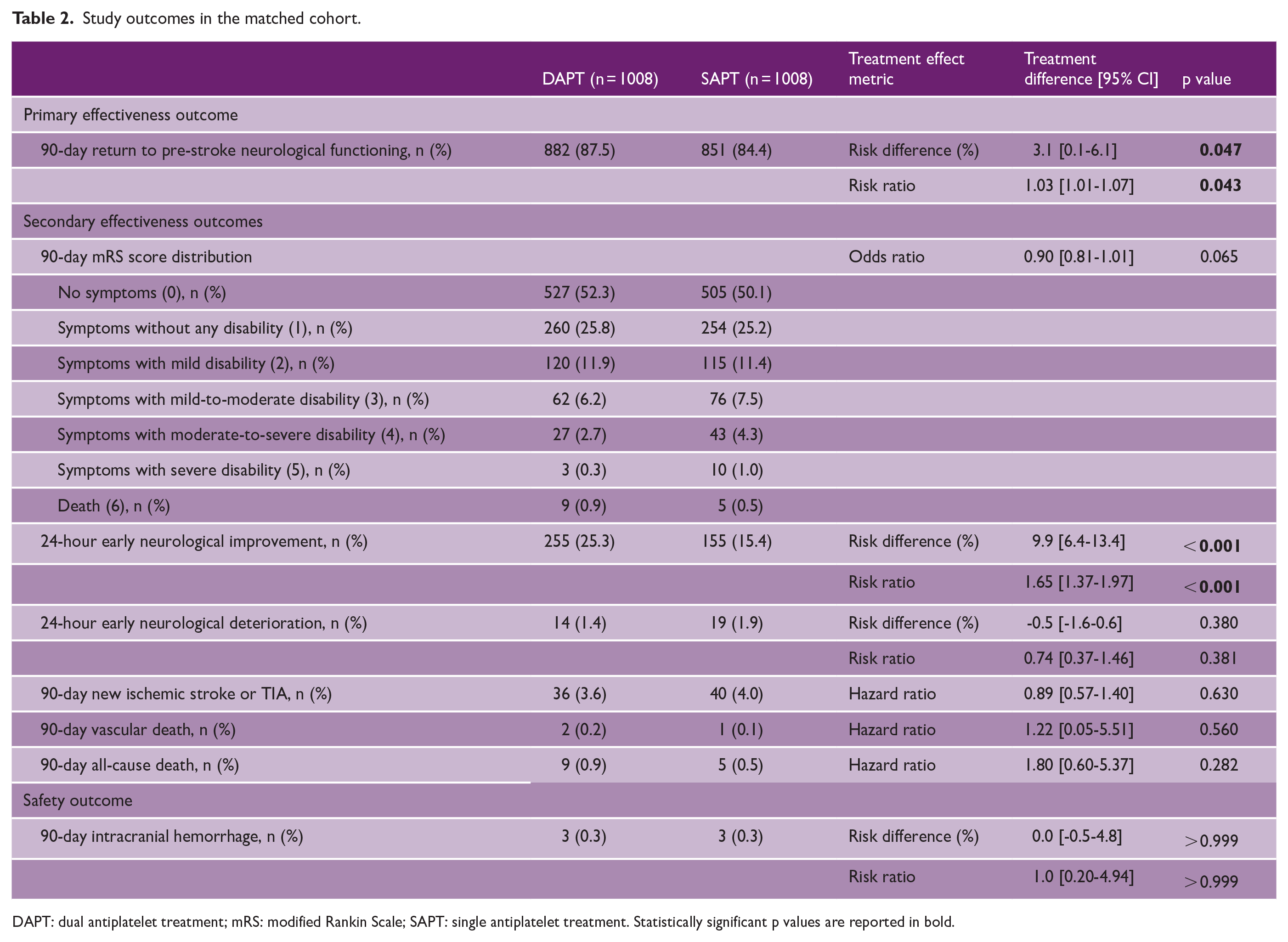
DAPT: dual antiplatelet treatment; mRS: modified Rankin Scale; SAPT: single antiplatelet treatment. Statistically significant p values are reported in bold.
Secondary effectiveness outcomes
Compared to SAPT patients, those treated with DAPT showed a higher frequency of 24 h ENI (risk difference: 9.9% (95% CI: 6.4%–13.4%); p < 0.001; risk ratio: 1.65 (95% CI: 1.37–1.97); p < 0.001). We found a similar risk of 90-day new stroke/TIA between groups, as well as of 90-day vascular and all-cause mortality. There were no significant differences in the 24 h risk of END. Although a slightly higher proportion of patients treated with DAPT (78.1%) showed 90-day excellent functional outcome (mRS 0–1) compared to SAPT (75.3%), we found no significant differences in the 90-day mRS shift (OR 0.90 (95% CI: 0.81–1.01); p = 0.065) (Table 2, Supplemental Figure 3). Comparison of secondary outcomes in the unmatched cohort showed no significant results, Supplemental Table 1.
Safety outcome
The 90-day risk of intracranial hemorrhage was very low and did not differ between DAPT and SAPT (both 0.3%; risk difference 0% (95% CI: −0.5% to 4.8%), risk ratio 1.0 (0.20–4.94) > 0.999) (Table 2). We found no significant differences also in the unmatched cohort (Supplemental Table 1).
Subgroup analysis
Results of subgroup analysis are presented in Figure 2 and Supplemental Table 2. We found a higher frequency of 90-day primary effectiveness outcome in patients with NIHSS 6–10 treated with DAPT versus SAPT (risk difference 19.9% (95% CI: 6.1%–33.7%); p = 0.004), as well as in those who received IVT (risk difference 17.4% (95% CI: 8.5%–26.2%); p < 0.001) or antiplatelet loading dose (risk difference 6.8% (95% CI: 2.2%–11.1%); p = 0.005). There was no significant risk difference in the 90-day rate of primary effectiveness outcome across other prespecified subgroups.
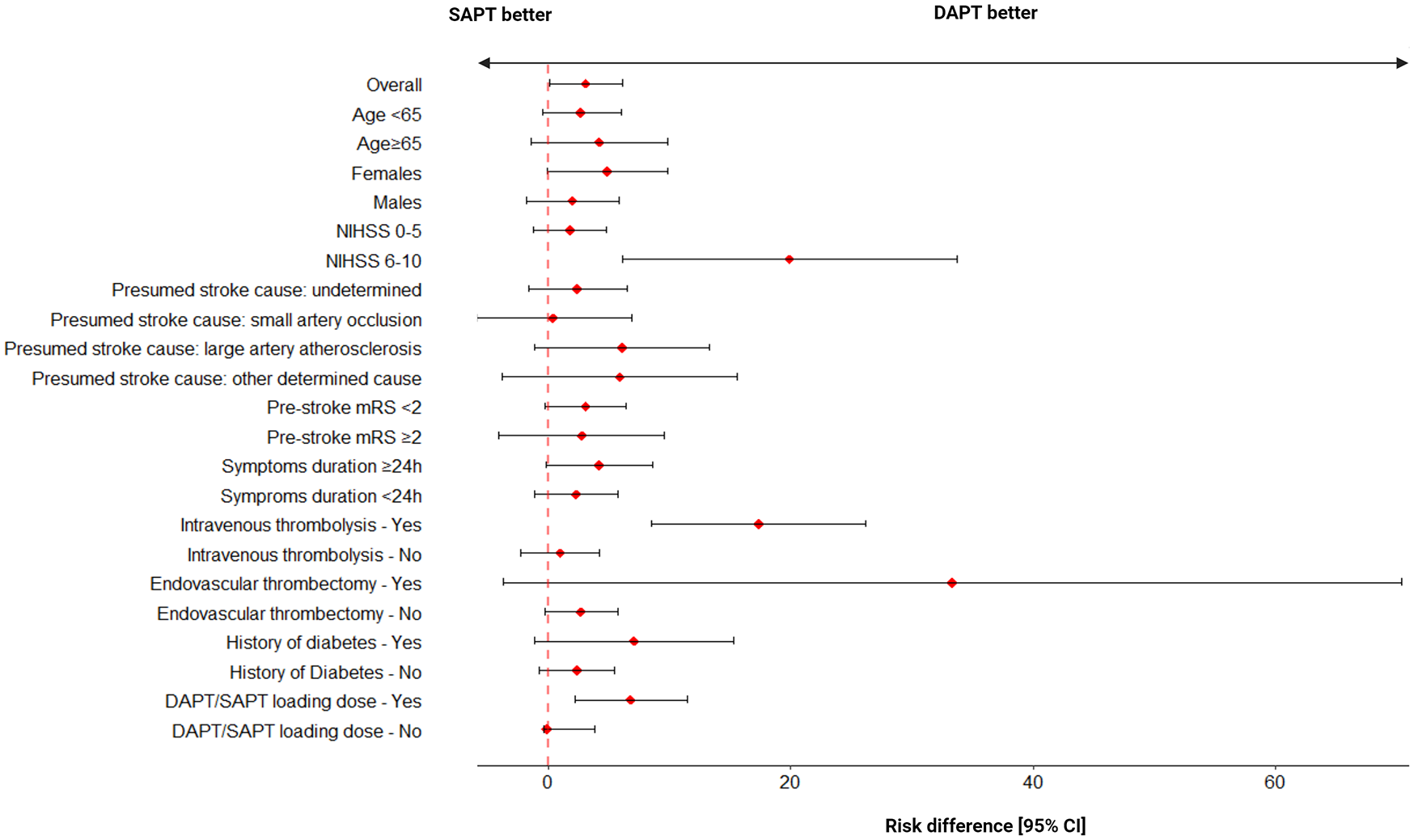
Risk differences in primary effectiveness outcome by prespecified subgroups. DAPT: dual antiplatelet treatment; mRS: modified Rankin Scale; NIHSS: National Institute of Health Stroke Scale; SAPT: single antiplatelet treatment. Red dots indicate risk difference, and black bars indicate a 95% confidence interval (CI).
Sensitivity analysis
Sensitivity analysis within the overall cohort showed that the 90-day risk of new stroke and TIA was significantly lower in patients with baseline NIHSS 0–3 treated with DAPT versus SAPT (2.7% vs. 5.8%, HR 0.46 (95% CI: 0.30–0.71); p < 0.001). We found a lower rate of 24 h END in patients with baseline NIHSS 4–10 treated with DAPT than SAPT (3.3% vs. 5.5%, risk difference −2.1 (−5.4% to 1.3%) risk ratio 0.62 (0.30–1.30) although the statistical significance was not reached (p = 0.201), Supplemental Table 3.
Discussion
In a real-world population of patients with non-cardioembolic mild-to-moderate stroke, we found that early short-term DAPT was associated with higher likelihood of returning to pre-stroke mRS at 90 days than SAPT. This extends evidence from landmark clinical trials that showed superiority of DAPT versus aspirin alone in preventing 90 day stroke recurrence among patients with minor stroke (NIHSS upper limit 3–5) or high-risk TIA on a diverse outcome and on a more unselected population.1 –4 The ATAMIS study demonstrated that DAPT outperformed SAPT in reducing the incidence of END at 7 days among patients with mild-to-moderate (NIHSS 4–10) strokes. 7 However, there was no significant risk difference in the rate of excellent functional outcome (mRS 0–1) nor in the ordinal mRS shift at 90 days between patients treated with DAPT or SAPT. 7 Within our population, the rates of 24 h END were similarly low in both patients who received DAPT and SAPT (1.4% vs. 1.9%), while DAPT outperformed SAPT in increasing the rate of 24 h ENI (25.3% vs. 15.4%). Benefits of DAPT on functional improvement and ENI may be attributed to the more potent and faster inhibition of platelet activation pathways provided by the early initiation of combined versus single antiplatelet treatment, which is likely more effective in halting blood clot growth and propagation during the acute ischemic stroke process. 15 Given the observational nature of our study, it is important to note that our primary effectiveness outcome may have been affected by a number of unmeasured confounders (i.e. type of stroke-related deficit, management of concomitant morbidities, patient compliance to prescribed therapies, efficacy of early post-stroke rehabilitation). Therefore, our findings need cautious interpretation, as we cannot draw any definitive conclusion on the potential direct role of DAPT in ameliorating the 90-day functional outcome.
At variance with landmark randomized trials,1 –4 we found no significant differences in the 90-day risk of new stroke/TIA, vascular and all-cause mortality, likely due to the relatively low number of these secondary outcome events. In addition, the inclusion of patients with varying pre-stroke disability, those who underwent hyperacute treatments, and differences in DAPT characteristics (different proportions of patients who received antiplatelet loading dose, shorter DAPT duration) could also have contributed to this inconsistency. Of note, our sensitivity analysis in the overall cohort showed that the 90-day risk of new stroke/TIA was significantly lower in patients treated with DAPT versus SAPT when aligning with the baseline NIHSS range (0–3) of the POINT 3 trial. Similar to the ATAMIS 7 and recent observational studies,16,17 we registered low rates of intracranial hemorrhage at 90 days in both treatment groups (0.3%), proving safety and feasibility of short-duration DAPT also in moderate strokes.
We also found that DAPT benefit in terms of primary effectiveness outcomes was greater in the subgroups of patients with moderate (NIHSS 6–10) stroke, those treated with IVT, and who received antiplatelet loading dose. The ATAMIS trial showed that patients with baseline NIHSS 4–10 had a positive trend in terms of END at 7 days when treated with DAPT versus SAPT. 7 Similarly, our sensitivity analysis in patients with baseline NIHSS 4–10 suggested superiority of DAPT over SAPT in reducing the rate of END within the overall cohort, although statistical significance was not reached, and our definition of END was based on a shorter timeframe (24 h) compared to ATAIMS 7 (7 days). Remarkably, the majority of patients enrolled in our study had mild neurological deficits (91.1%), which may have weakened the statistical power of subgroup analyses concerning moderate strokes. Therefore, our findings require cautious interpretation and confirmation in larger samples. Regarding IVT, the increased probability of return to baseline mRS observed among patients treated with alteplase plus DAPT might suggest a synergistic effect in promoting neurological recovery. Indeed, alteplase, as a short-lived agent, might counter the progression of acute thrombosis while early DAPT start might reduce the risk of early worsening. This result aligns with a recent subgroup analysis of the READAPT study, which showed better 90-day mRS score distribution in patients treated with IVT plus DAPT versus DAPT alone, without increased risk of major bleedings. 18 Finally, the higher frequency of primary outcome in those treated with DAPT versus SAPT loading dose highlights the importance of combined platelet inhibition for a more favorable functional prognosis 15 and encourages to treat all patients with an antiplatelet loading dose (a practice often overlooked in real-world scenarios 5 ).
The main study strength is the adoption of rigorous propensity score matching to reduce the effect of potential confounders when testing outcome differences between groups. However, we cannot exclude residual confounding due to the observational design of the READAPT and local stroke registries. Notably, the latter did not systematically collect data on patient ethnicity, and we could not account for this demographic characteristic in the matching. The follow-up period of this study was also limited to 90 days, as DAPT is a short-term treatment. Anyway, the two treatment options might lead to different outcomes in the long term. Furthermore, while we limited data extraction to a specific timeframe predating the implementation of DAPT guidelines11,12 (1 January 2018–31 December 2020), there remains the possibility that some patients were deemed eligible for DAPT rather than SAPT by local physicians based on their stroke risk profile. Another relevant limitation is the lack of imaging data. Although all patients underwent at least a brain NCCT/MRI on admission, we did not collect detailed neuroimaging findings or results of brain vessel exams. Therefore, the appropriateness of stroke diagnosis and presumed stroke causes were determined by local investigators. In addition, although all patients from the READAPT study and local stroke registries were followed up either on-site or via phone interview, ensuring that clinically relevant intercurrent events were recorded even if the patient was not admitted to one of the participating centers, we cannot exclude the possibility that some recurrences with mild or transient symptoms went unreported. This may have resulted in an underestimation of the primary effectiveness outcome in both cohorts. Furthermore, patients who early discontinued DAPT (n = 44) or SAPT (n = 21) due to the need for anticoagulation were excluded, and their outcomes were not recorded. Although this subset accounted for only 1.9% and 1.0% of the initial DAPT and SAPT samples (Figure 1), we were unable to assess the impact of transitioning from DAPT to anticoagulation on effectiveness and safety outcomes. Finally, as the local stroke registries were established prior to the COVID-19 pandemic, we cannot rule out a potential negative impact on 90-day outcomes due to factors such as prolonged door-to-needle or door-to-groin times for patients undergoing IVT or EVT, reduced access to early rehabilitation, and suboptimal management of cardiovascular comorbidities. However, mild-to-moderate stroke patients enrolled in 2020 comprised only 4.4% of the original SAPT cohort.
In conclusion, our results support DAPT use as safe and more effective than SAPT in patients with non-cardioembolic mild-to-moderate stroke. Treatment with DAPT may not only better prevent recurrences1 –4 but also favor neurological improvement and functional recovery. The benefits of DAPT are confirmed in patients with stroke of moderate severity and those treated with IVT, therefore suggesting that DAPT benefits could extend to patients who are beyond the selection criteria of landmark large clinical trials.
Supplemental Material
sj-docx-1-wso-10.1177_17474930241302991 – Supplemental material for Real-world comparison of dual versus single antiplatelet treatment in patients with non-cardioembolic mild-to-moderate ischemic stroke: A propensity matched analysis
Supplemental material, sj-docx-1-wso-10.1177_17474930241302991 for Real-world comparison of dual versus single antiplatelet treatment in patients with non-cardioembolic mild-to-moderate ischemic stroke: A propensity matched analysis by Matteo Foschi, Raffaele Ornello, Lucio D’Anna, Eleonora De Matteis, Federico De Santis, Valentina Barone, Marilina Viola, Maria Giulia Mosconi, Diletta Rosin, Michele Romoli, Tiziana Tassinari, Silvia Cenciarelli, Bruno Censori, Marialuisa Zedde, Marina Diomedi, Marco Petruzzellis, Vincenzo Inchingolo, Manuel Cappellari, Paolo Candelaresi, Alessandra Bavaro, Anna Cavallini, Maria Grazia Piscaglia, Valeria Terruso, Alessandro Pezzini, Giovanni Frisullo, Francesco Muscia, Andrea Zini, Ruggiero Leone, Carmela Palmieri, Letizia Maria Cupini, Michela Marcon, Rossana Tassi, Enzo Sanzaro, Giulio Papiri, Giovanna Viticchi, Daniele Orsucci, Anne Falcou, Susanna Diamanti, Roberto Tarletti, Patrizia Nencini, Eugenia Rota, Federica Nicoletta Sepe, Luigi Caputi, Gino Volpi, Salvatore La Spada, Mario Beccia, Vincenzo Mastrangelo, Paolo Invernizzi, Giuseppe Pelliccioni, Maria Vittoria De Angelis, Laura Bonanni, Giampietro Ruzza, Emanuele Alessandro Caggia, Monia Russo, Agnese Tonon, Maria Cristina Acciarri, Sabrina Anticoli, Cinzia Roberti, Gaspare Scaglione, Francesca Pistoia, Chiara Alessi, Antonella De Boni, Alessandra Sanna, Alberto Chiti, Leonardo Barbarini, Maela Masato, Massimo Del Sette, Francesco Passarelli, Maria Roberta Bongioanni, Manuela De Michele, Stefano Ricci, Mariarosaria Valente, Gian Luigi Gigli, Giovanni Merlino, Maurizio Paciaroni, Maria Guarino and Simona Sacco in International Journal of Stroke
Supplemental Material
sj-docx-2-wso-10.1177_17474930241302991 – Supplemental material for Real-world comparison of dual versus single antiplatelet treatment in patients with non-cardioembolic mild-to-moderate ischemic stroke: A propensity matched analysis
Supplemental material, sj-docx-2-wso-10.1177_17474930241302991 for Real-world comparison of dual versus single antiplatelet treatment in patients with non-cardioembolic mild-to-moderate ischemic stroke: A propensity matched analysis by Matteo Foschi, Raffaele Ornello, Lucio D’Anna, Eleonora De Matteis, Federico De Santis, Valentina Barone, Marilina Viola, Maria Giulia Mosconi, Diletta Rosin, Michele Romoli, Tiziana Tassinari, Silvia Cenciarelli, Bruno Censori, Marialuisa Zedde, Marina Diomedi, Marco Petruzzellis, Vincenzo Inchingolo, Manuel Cappellari, Paolo Candelaresi, Alessandra Bavaro, Anna Cavallini, Maria Grazia Piscaglia, Valeria Terruso, Alessandro Pezzini, Giovanni Frisullo, Francesco Muscia, Andrea Zini, Ruggiero Leone, Carmela Palmieri, Letizia Maria Cupini, Michela Marcon, Rossana Tassi, Enzo Sanzaro, Giulio Papiri, Giovanna Viticchi, Daniele Orsucci, Anne Falcou, Susanna Diamanti, Roberto Tarletti, Patrizia Nencini, Eugenia Rota, Federica Nicoletta Sepe, Luigi Caputi, Gino Volpi, Salvatore La Spada, Mario Beccia, Vincenzo Mastrangelo, Paolo Invernizzi, Giuseppe Pelliccioni, Maria Vittoria De Angelis, Laura Bonanni, Giampietro Ruzza, Emanuele Alessandro Caggia, Monia Russo, Agnese Tonon, Maria Cristina Acciarri, Sabrina Anticoli, Cinzia Roberti, Gaspare Scaglione, Francesca Pistoia, Chiara Alessi, Antonella De Boni, Alessandra Sanna, Alberto Chiti, Leonardo Barbarini, Maela Masato, Massimo Del Sette, Francesco Passarelli, Maria Roberta Bongioanni, Manuela De Michele, Stefano Ricci, Mariarosaria Valente, Gian Luigi Gigli, Giovanni Merlino, Maurizio Paciaroni, Maria Guarino and Simona Sacco in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AZ reports compensation from Angels Initiative, Boehringer-Ingelheim, Daiichi Sankyo for consultant services; from Angels Initiative, Boehringer-Ingelheim, CSL Behring for speaking honoraria or other education services; from Daiichi Sankyo for meeting; from Bayer, and Astra Zeneca for participation on a Data Safety, Monitoring or Advisory Board; he is member of ESO guidelines, ISA-AII guidelines, and IRETAS steering committee. RO reports grants from Novartis and Allergan; compensation from Teva Pharmaceutical Industries, Eli Lilly and Company, and Novartis for other services; and travel support from Teva Pharmaceutical Industries. SS reports compensation from Novartis, NovoNordisk, Allergan, AstraZeneca, Pfizer Canada, Inc, Eli Lilly and Company, Teva Pharmaceutical Industries, H. Lundbeck A/S, and Abbott Canada for consultant services; compensation from Novartis for other services. MP reports compensation from Daiichi Sankyo Company, Bristol Myers Squibb, Bayer, and Pfizer Canada, Inc., for consultant services. The other authors report no conflicts.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The READAPT study was approved by the University of L’Aquila Internal Review Board (03/2021). Local stroke registries were approved by the respective ethics committee at each site (S.Orsola-Malpighi University Hospital—398/2018, Udine University Hospital—CEUR-2020-Os-173), or conducted in accordance with the national and local regulations (Perugia Stroke Registry—DL 1995/2003).
Informed consent
All patients gave written informed consent for being included in this study.
Data availability
The complete dataset used for this study will be shared upon request from any qualified researcher to the corresponding author.
ORCID iD
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.