
Abstract
Background:
The effects of blood pressure (BP) lowering in patients treated with intravenous tissue plasminogen activator (IV tPA) before endovascular thrombectomy (EVT) are unclear.
Aims:
This study aims to investigate whether intensive and conventional BP management affects outcomes differently, depending on IV tPA administration before EVT.
Methods:
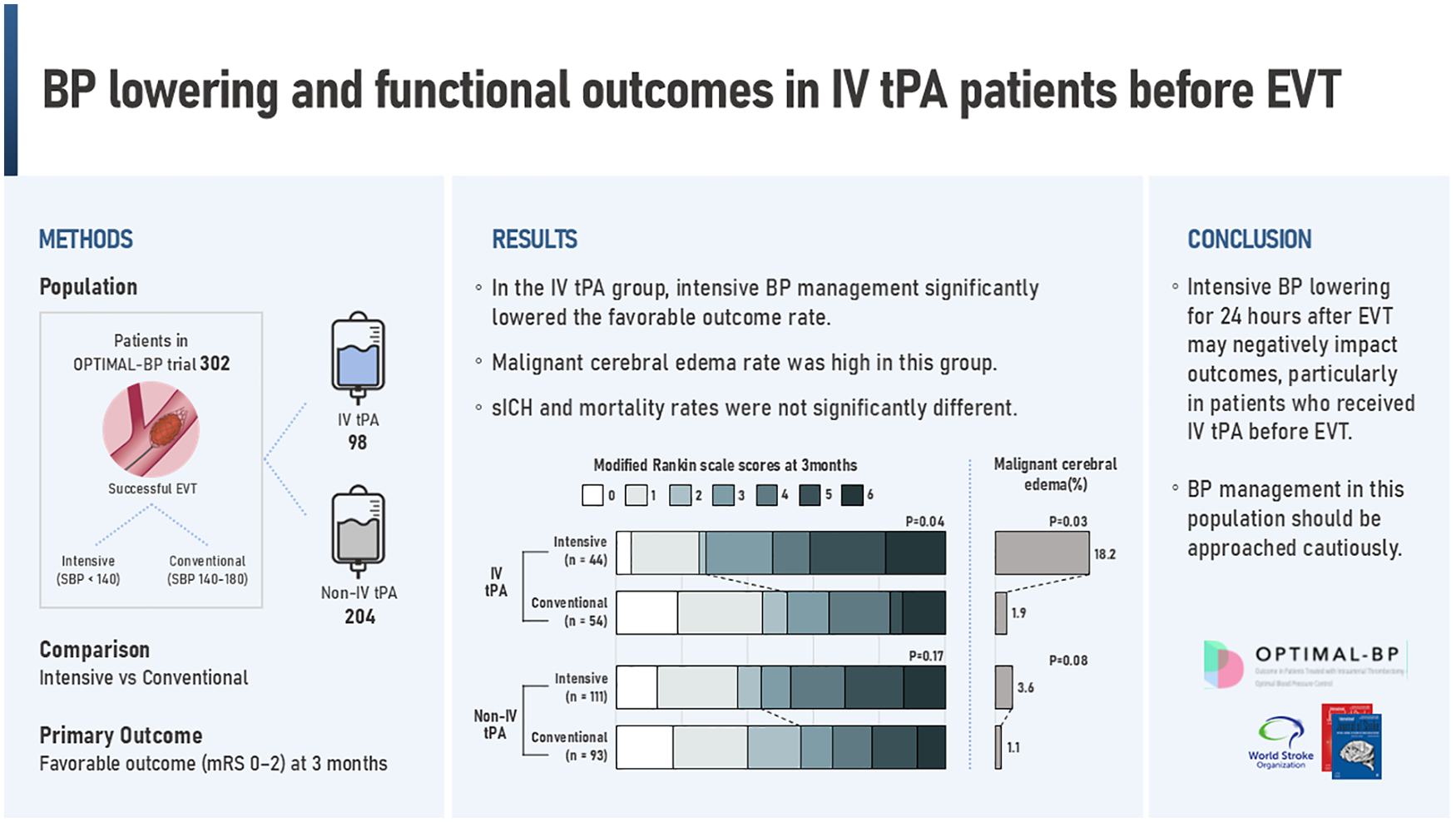
In this subgroup analysis of the Outcome in Patients Treated with Intra-Arterial Thrombectomy–Optimal Blood Pressure Control (OPTIMAL-BP; ClinicalTrials.gov Identifier: NCT04205305) trial, patients were divided into groups based on IV tPA use before EVT. Clinical outcomes of intensive (systolic BP target < 140 mm Hg) or conventional BP management (systolic BP target 140–180 mm Hg) were compared among groups. The primary efficacy outcome was a favorable outcome at 3 months (modified Rankin Scale score of 0–2). Primary safety outcomes included symptomatic intracerebral hemorrhage (sICH) within 36 h and stroke-related death within 3 months.
Results:
Among the 302 patients, the IV tPA group included 98 (32.5%) and the non-IV tPA group comprised 204 subjects (67.5%). In the IV tPA group, intensive BP management significantly lowered the favorable outcome rate (intensive, 27.3% vs. conventional, 51.9%; adjusted odds ratio [aOR], 0.36; 95% confidence interval [CI], 0.13–0.93; p = 0.04). In the non-IV tPA group, the risk difference rate of favorable outcome was not significantly different between intensive and conventional BP management (44.1% vs. 55.9%; aOR, 0.62; 95% CI, 0.31–1.22; p = 0.17). Notably, the proportion of malignant cerebral edema within 36 h in the IV tPA group was significantly higher in the intensive management group (18.2%) than in the conventional management group (1.9%; aOR, 10.72; 95% CI, 1.24–92.29; p = 0.03). sICH and mortality rates were not significantly different between intensive and conventional BP management in either study groups.
Conclusions:
Intensive BP management worsens 3-month functional outcomes after successful EVT without reducing sICH among patients who received IV tPA before EVT, indicating that BP lowering in this population should be cautious.
Introduction
Blood pressure (BP) control following successful reperfusion therapy may influence outcomes for patients with acute ischemic stroke. The American Heart association (AHA) guideline recommends maintaining BP below 180/105 mmHg following intravenous tissue plasminogen activator (IV tPA) administration for 24 h. 1 However, specific recommendation for BP management after IV tPA does not exist in the European Stroke Organization (ESO) guideline. 2 After endovascular thrombectomy (EVT), both AHA and ESO guidelines recommend BP below 180/105 mmHg for 24 h.1,3
Recently, four randomized control trials (RCTs) have compared intensive BP management with guideline-based BP management among patients who underwent EVT with successful reperfusion.4–7 In recent meta-analyses, intensive BP lowering clearly resulted in worse functional outcomes without significant reduction of symptomatic intracerebral hemorrhage (sICH).8–10 The four RCTs included 30–59% of patients who received IV tPA before EVT. However, the effectiveness and safety of intensive BP lowering in patients with IV tPA before EVT was not reported.4–7
Although tPA effectively restores cerebral blood flow by resolving occluding thrombi, the risk of hemorrhagic transformation and reperfusion injury can be increased.11–13 Intensive BP control may help prevent hemorrhagic transformation after successful reperfusion with IV tPA and EVT. However, intensive BP lowering can also reduce cerebral perfusion pressure, potentially exacerbating ischemic injury in the early reperfusion phase and worsening outcomes associated with the adverse effects of IV tPA. In the present study, a subgroup analysis of the Outcome in Patients Treated with Intra-Arterial Thrombectomy–Optimal Blood Pressure Control (OPTIMAL-BP) trial was performed to investigate whether the effects of intensive BP lowering after successful EVT differ based on the IV tPA treatment before EVT.
Methods
Study design and population
The OPTIMAL-BP trial (NCT04205305) was a multicenter, randomized, open-label, blinded-endpoint trial conducted in 19 stroke centers across South Korea from June 2020 to November 2022. 6 The OPIMAL-BP trial assessed the effects of intensive BP management (systolic BP [SBP] target: <140 mm Hg) versus conventional BP management (SBP target: 140–180 mmHg) during the first 24 h after successful reperfusion in patients whose SBP exceeded 140 mmHg within 2 h after EVT. We analyzed all patients in the primary analysis of the OPTIMAL-BP trial.
Patients were stratified into two categories based on IV tPA administration before EVT: patients who received IV tPA (IV tPA group) before EVT and patients who did not receive IV tPA before EVT (non-IV tPA group). The institutional review boards of Severance hospital (Approval No.: 4-2019-1208) and participating hospital approved the OPTIMAL-BP trial study protocol, and written informed consent was obtained from all participants or their approved surrogate. The protocol is provided in Supplement 1, with the statistical analysis plan in Supplement 2. This study followed the Consolidated Standards of Reporting Trials (CONSORT) statement. 14 All participants were treated in facilities comparable to a stroke unit, with the capability for continuous BP monitoring and adherence to the best practice guidelines.1–3 Non-invasive methods were consistently utilized for BP measurement. IV BP medications were used to achieve and maintain the specific SBP target for each group.
Outcomes
The primary efficacy outcome was a favorable outcome at 3 months as measured using a modified Rankin Scale (mRS) score of 0–2. The primary safety outcomes were sICH within 36 h and mortality related to the index stroke within 3 months. The criteria for sICH were based on the European Cooperative Acute Stroke Study III. 15 Mortality related to the index stroke was defined as death occurring as a direct consequence of the brain lesion or to complications of immobility from the stroke within 3 months of onset.
There were nine secondary outcomes: (1) shift analysis of the distribution of mRS scores; (2) incidence of any type of ICH within 36 h; (3) National Institutes of Health Stroke Scale (NIHSS) score at 24 h; (4) proportion of patients with excellent recovery (a NIHSS score of 0–1 or an improvement of >8 points at 24 h); (5) successful reperfusion at 24 h, defined as modified Thrombolysis in Cerebral Infarction grade ⩾2b based on follow-up computed tomography angiography or magnetic resonance angiography at 24 (±12) h; (6) favorable outcome at 1 month; (7) 3-level EuroQoL 5-Dimension Self-Report Questionnaire (EQ-5D-3L) score at 3 months; (8) frequency of malignant cerebral edema within 36 h; and (9) infarction volume at 24 h after EVT. Malignant cerebral edema is a condition characterized by rapid neurological deterioration accompanied by substantial brain swelling on computed tomography or magnetic resonance imaging, and often leads to death or poor functional outcome.
Statistical analysis
Data are presented as mean with standard deviation (SD), median (interquartile range, IQR), or percentage (%), as appropriate. Baseline characteristics were compared between the intensive and conventional management groups in the IV tPA and non-IV tPA groups. Appropriate statistical methods including the t-test, Wilcoxon rank sum test, χ2 test, or Fisher exact test were utilized. For assessing the 24-h BP variation in the IV tPA and non-IV tPA groups, a linear mixed model was used.
Primary and secondary outcomes were analyzed using binomial logistic regression to calculate adjusted odds ratios (aORs) and 95% confidence intervals (CIs), as well as risk differences with 95% CIs. Among secondary outcomes, ordinal logistic regression was used for shift analysis of the mRS score. The NIHSS score at 24 h, the EQ-5D-3L score, and infarction volume were analyzed using quantile regression. Interaction analyses were conducted for all outcomes to investigate whether the effects of BP management differed between the IV tPA and non-IV tPA groups. Each analysis was adjusted age, sex, time from stroke onset to randomization, and the NIHSS score obtained immediately before EVT as covariates. Statistical significance was set at a two-sided p value < 0.05. All analyses were conducted using R software, version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Results
Study population and baseline characteristics
Among the 306 patients who were enrolled in the OPTIMAL-BP trial, 1 was excluded due to immediate withdrawal of consent after randomization and 3 were excluded due to follow-up loss. A total of 302 patients were included in this study (mean age, 73 years [SD, 11.5 years]; 180 [59.6%] men). A total of 98 patients (32.5%) received IV tPA before EVT and 204 patients (67.5%) did not receive IV tPA (Figure 1).
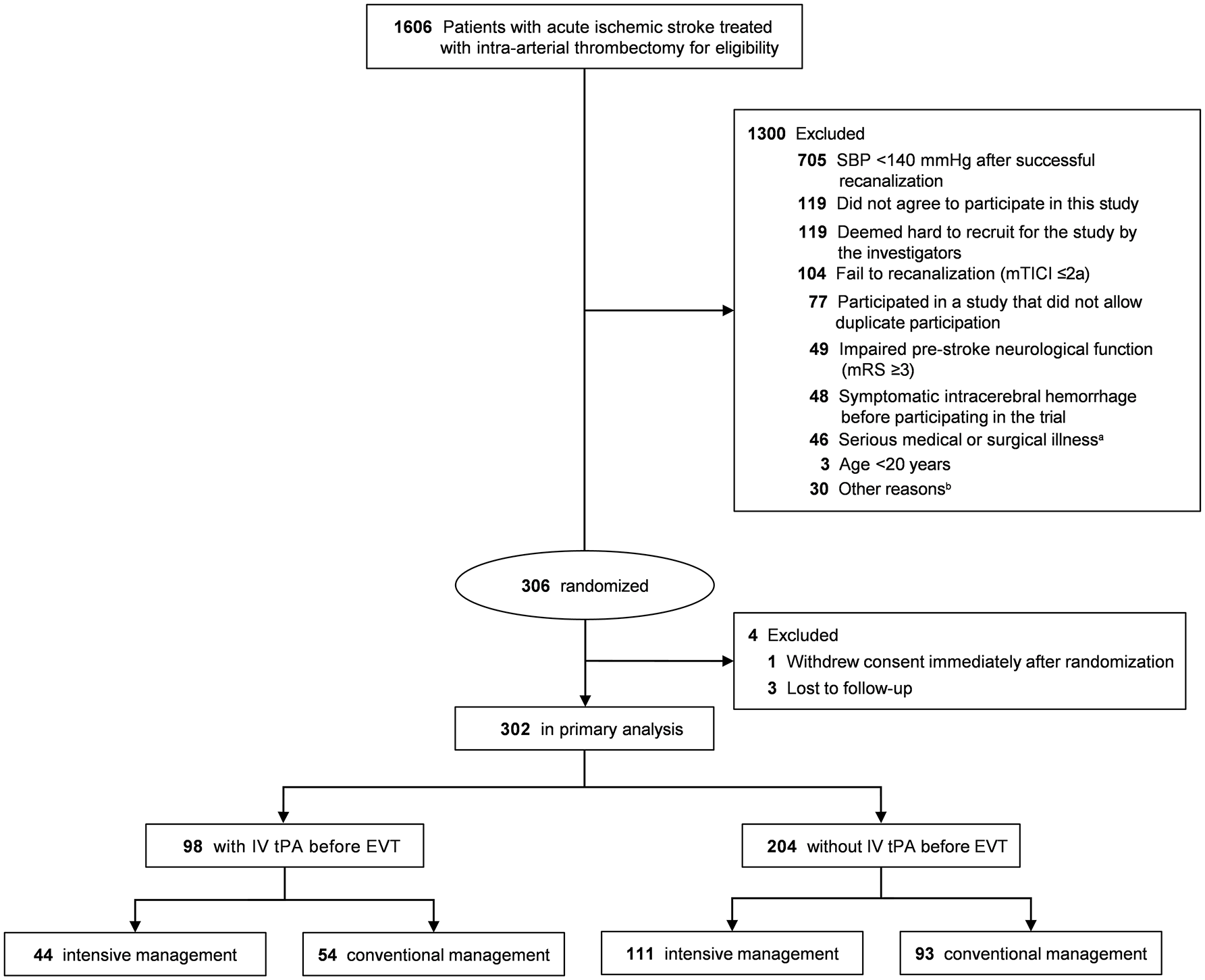
Flow chart of patient selection.
Baseline characteristics, including demographics, clinical characteristics, imaging, and procedural factors, showed no significant differences between IV tPA and non-IV tPA groups or between intensive and conventional BP management groups in either treatment groups. However, the IV tPA group had a shorter time interval from stroke onset to reperfusion than the non-IV tPA group (279 min [IQR, 218.8–346.5 min] vs. 577.5 min [IQR, 377.8–923.3 min]) and shorter time interval from stroke onset to randomization (330 min [IQR, 268.5–397.5 min] vs. 644 min [IQR, 417.5–960.0 min]) (Table 1 and Table S1).
Baseline characteristics of patients stratified by IV tPA use.
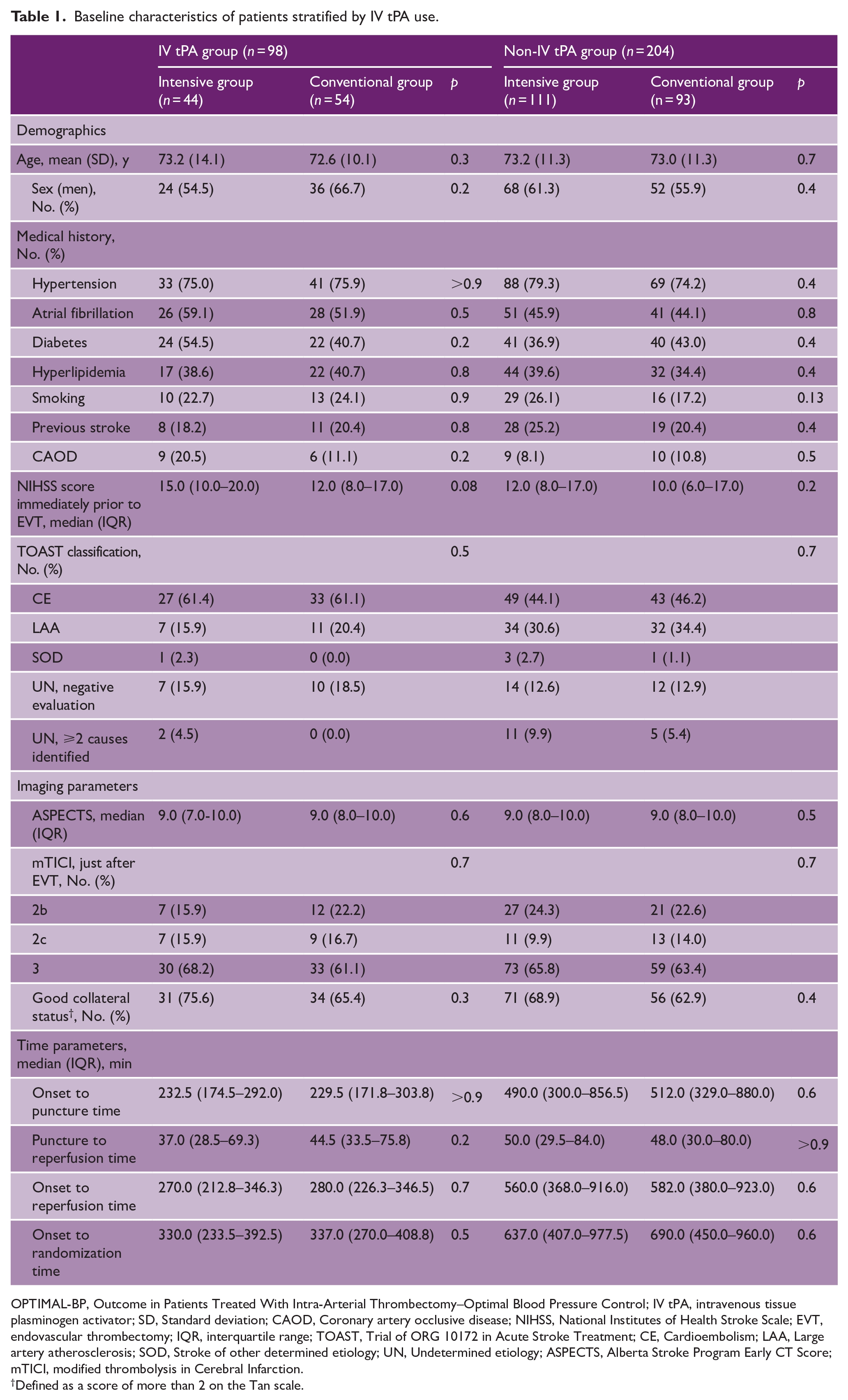
OPTIMAL-BP, Outcome in Patients Treated With Intra-Arterial Thrombectomy–Optimal Blood Pressure Control; IV tPA, intravenous tissue plasminogen activator; SD, Standard deviation; CAOD, Coronary artery occlusive disease; NIHSS, National Institutes of Health Stroke Scale; EVT, endovascular thrombectomy; IQR, interquartile range; TOAST, Trial of ORG 10172 in Acute Stroke Treatment; CE, Cardioembolism; LAA, Large artery atherosclerosis; SOD, Stroke of other determined etiology; UN, Undetermined etiology; ASPECTS, Alberta Stroke Program Early CT Score; mTICI, modified thrombolysis in Cerebral Infarction.
Defined as a score of more than 2 on the Tan scale.
BP measurements
In both the IV tPA and non-IV tPA groups, the intensive management group had significantly lower 24-h mean SBP compared with the conventional management group. In the IV tPA group, the mean SBP was 130.9 mmHg (SD 11.3 mmHg) in the intensive BP management group and 137.1 mm Hg (SD 17.5 mmHg) in the conventional BP management group (p < 0.01). In the non-IV tPA group, mean SBP was 129.9 mmHg (SD 9.9 mmHg) in the intensive BP management group and 137.5 mmHg (SD 20.7 mmHg) in the conventional BP management group (p < 0.01). The mean between-group difference in SBP over 24 h was −8.2 mm Hg (95% CI, −10.4 to −6.0 mmHg; p < 0.01) in the IV tPA group and −9.4 mm Hg (95% CI, −10.9 to −7.9 mmHg; p < 0.01) in the non-IV tPA group (Figure 2; Table S2).
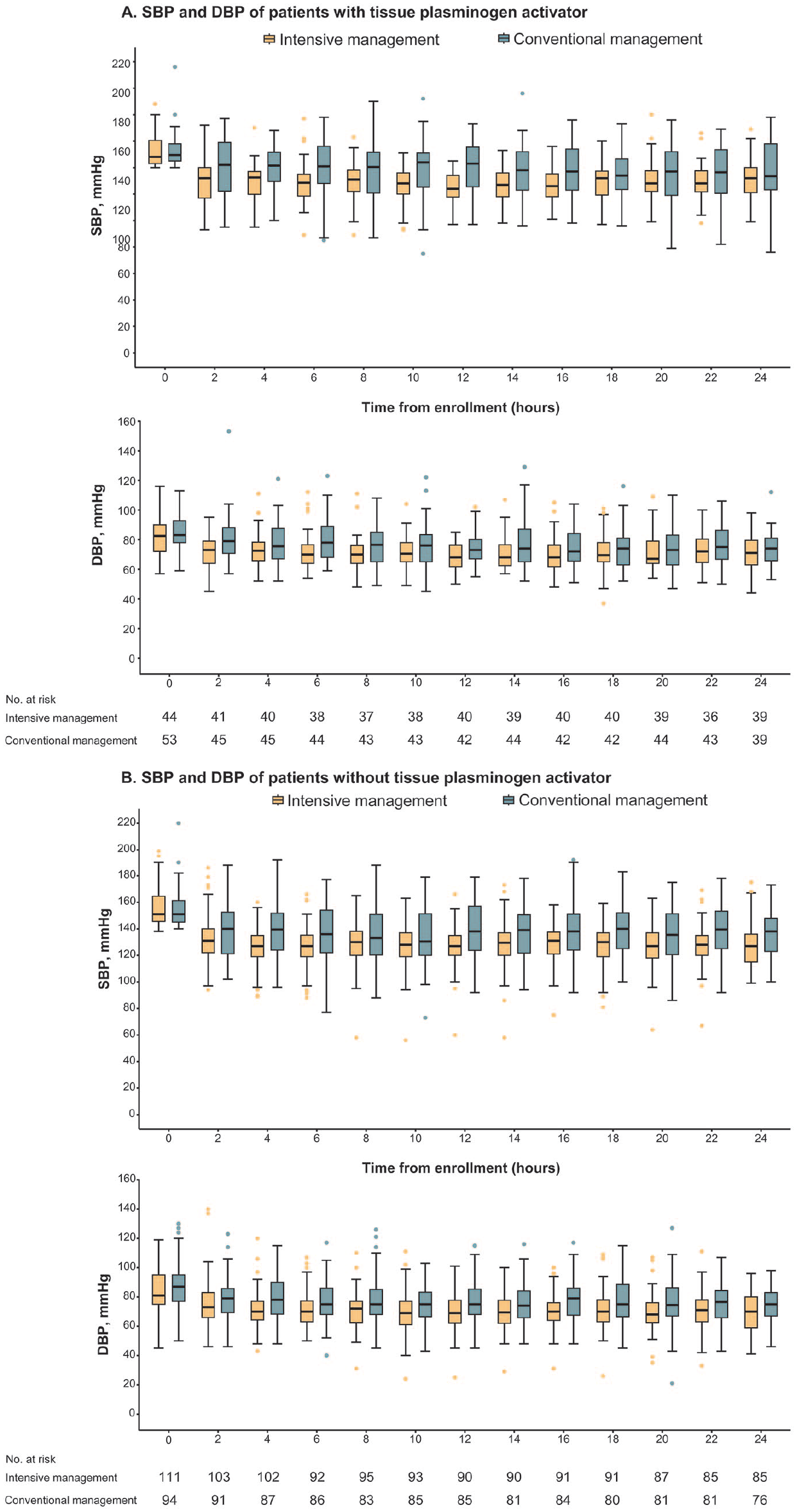
Changes in mean systolic and diastolic blood pressure from randomization to 24 h post-randomization by intravenous tissue plasminogen activator (IV tPA) use before endovascular thrombectomy.
Primary efficacy outcome
In the IV tPA group, the proportion of favorable outcome at 3 months was significantly lower in the intensive management group (12/44, 27.3%) than in the conventional management group (28/54, 51.9%). This resulted in a significant risk difference of −24.6% (95% CI, −43.3% to −5.8%) and an aOR of 0.36 (95% CI, 0.13−0.93; p = 0.04). In the non-IV tPA group, the intensive management group (49/111, 44.1%) achieved a lower rate of favorable outcome at 3 months than the conventional management group (52/93, 55.9%), the risk difference of −11.8% (95% CI, −25.5% to −2.1%) and aOR of 0.62 (95% CI, 0.31−1.22; p = 0.17), although there was no statistical significance (Table 2 and Figure 3).
Primary and secondary outcomes.
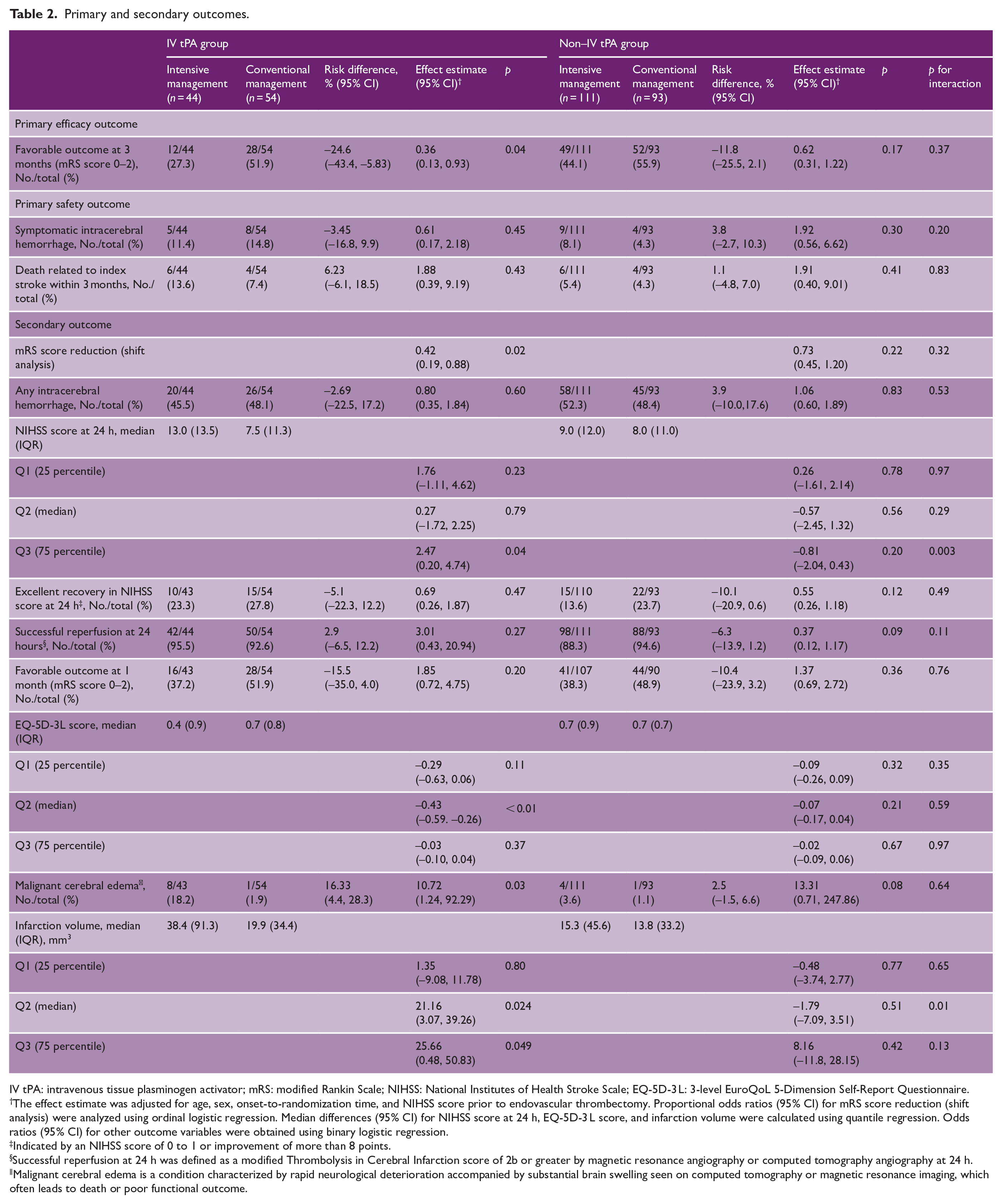
IV tPA: intravenous tissue plasminogen activator; mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; EQ-5D-3 L: 3-level EuroQoL 5-Dimension Self-Report Questionnaire.
The effect estimate was adjusted for age, sex, onset-to-randomization time, and NIHSS score prior to endovascular thrombectomy. Proportional odds ratios (95% CI) for mRS score reduction (shift analysis) were analyzed using ordinal logistic regression. Median differences (95% CI) for NIHSS score at 24 h, EQ-5D-3 L score, and infarction volume were calculated using quantile regression. Odds ratios (95% CI) for other outcome variables were obtained using binary logistic regression.
Indicated by an NIHSS score of 0 to 1 or improvement of more than 8 points.
Successful reperfusion at 24 h was defined as a modified Thrombolysis in Cerebral Infarction score of 2b or greater by magnetic resonance angiography or computed tomography angiography at 24 h.
Malignant cerebral edema is a condition characterized by rapid neurological deterioration accompanied by substantial brain swelling seen on computed tomography or magnetic resonance imaging, which often leads to death or poor functional outcome.
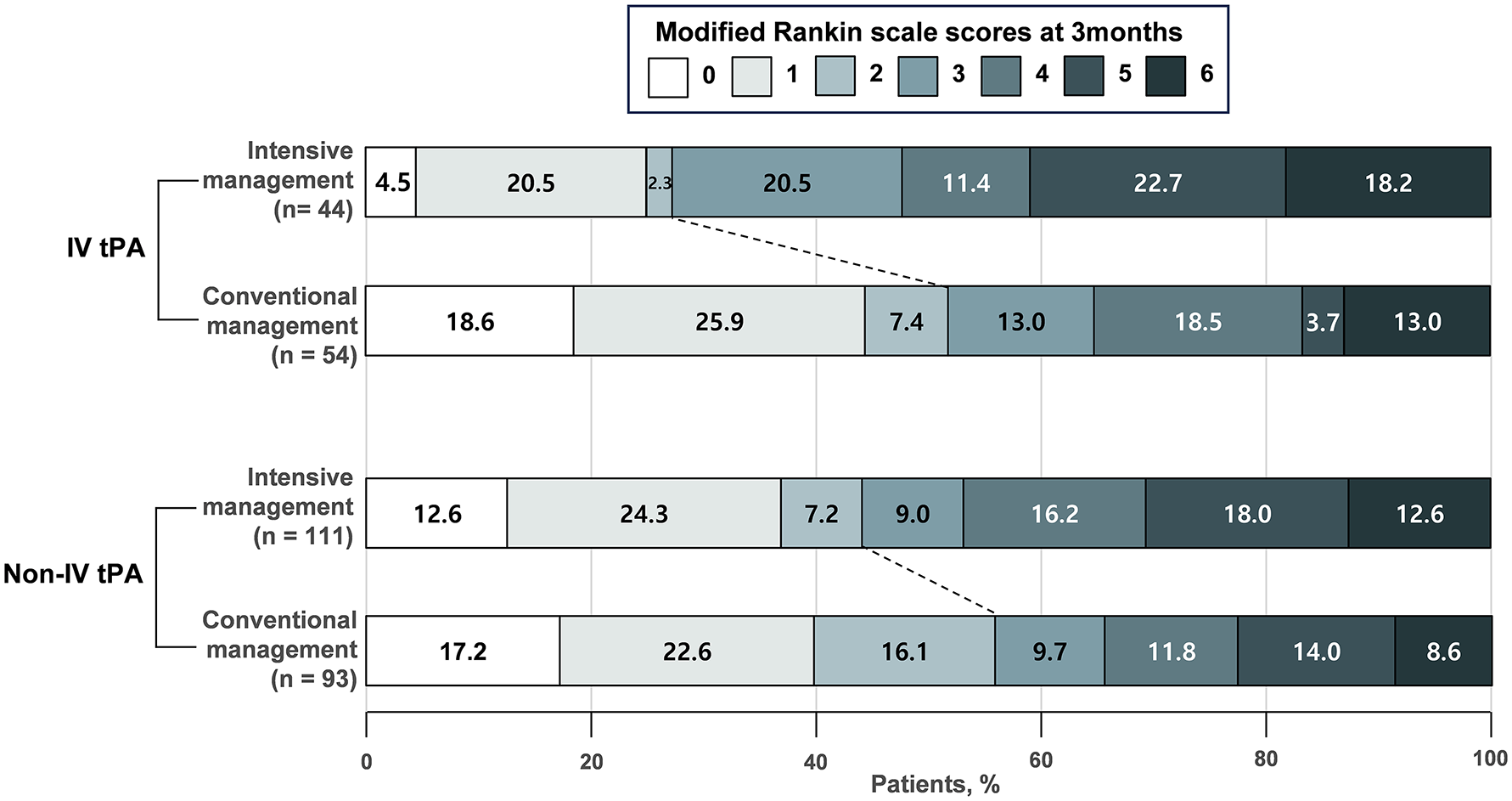
Distribution of mRS score at 3 months according to the study groups.
Primary safety outcomes
In the IV tPA group, the incidence of sICH was not significantly different between the intensive management group (5/44, 11.4%) and the conventional management group (8/54, 14.8%; aOR, 0.61; p = 0.45). Similarly, in the non-IV tPA group, sICH rate was not significantly different between the intensive and conventional management groups (9/111 [8.1%] and 4/93 [4.3%], respectively; aOR, 1.92; p = 0.30). Death rates related to the index stroke within 3 months were not significantly different between the intensive and conventional management groups in either the IV tPA (6/44, 13.6% vs. 4/54, 7.4%, aOR 1.88; p = 0.43) or non-IV tPA group (6/111, 5.4% vs. 4/93, 4.3%, aOR 1.91; p = 0.41) (Table 2).
Secondary outcomes
In the IV tPA group, a shift toward worse mRS outcomes at 3 months was observed in the intensive management group (aOR, 0.42; p = 0.02); however, no significant shift was found in the non-IV tPA group (aOR, 0.73; p = 0.22). In the IV tPA group, the intensive management group had significantly higher NIHSS scores at 24 h at the 75th percentile (Q3, effect estimate, 2.47; p = 0.04) than the conventional management group. The intensive management group had significantly lower median EQ-5D-3L scores than the conventional management group at 3 months (effect estimate, −0.43; p < 0.01). Notably, the proportion of malignant cerebral edema within 36 h in the IV tPA group was significantly higher in the intensive management group (8/43, 18.2%) than in the conventional management group (1/54, 1.9%; aOR, 10.72; p = 0.03). The median (IQR) infarction volume was 38.4 (91.3) in the intensive management group versus 19.9 (34.4) in the conventional management group. Quartile regression analysis showed a significantly larger median (Q2, effect estimate 21.16, p = 0.024) and 75th percentile (Q3, effect estimate 25.66, p = 0.049) infarction volume in the intensive management group than in the conventional management group. In contrast, in the non-IV tPA group, the NIHSS score at 24 h, the EQ-5D-3L score at 3 months, the proportion of malignant cerebral edema, and mean infarction volume were not significantly different between the intensive and conventional management groups (Table 2).
Discussion
In this subgroup analysis of the OPTIMAL-BP trial, intensive BP lowering was associated with a lower rate of favorable outcome at 3 months in the IV tPA group. The intensive BP lowering in the IV tPA group was also associated with a shift toward worse mRS outcomes at 3 months, lower NIHSS score at 24 h, and lower EQ-5D-3L score at 3 months. Notably, in the IV tPA group, the intensive management group had a higher incidence of malignant cerebral edema. In both the IV tPA or the non-IV tPA groups, sICH and death related to index stroke did not significantly differ based on the BP management strategy.
The intensive management group had a lower rate of favorable outcomes at 3 months in the IV tPA group but not in the non-IV tPA group. In addition, malignant cerebral edema was 10-fold more frequent in the intensive management group compared with the conventional management group in the IV tPA group. Although the beneficial activity of tPA is due to its thrombolytic effect that restores blood flow, potential adverse effects including reperfusion injury, blood brain barrier (BBB) breakdown, and increased risk of cerebral edema have been reported in several preclinical studies.12,16–18 Results of studies on traumatic brain injury suggested that IV tPA disrupts autoregulation during hypotension, impairing cerebral hemodynamics and causing cell damage.13,19–22 Similarly, we hypothesized that BP lowering may further exacerbate the injury in patients treated with IV tPA and EVT. In addition, the beneficial thrombolytic effects of tPA may be reduced when EVT is performed in non-recanalized patients after IV tPA. 23 However, most of these earlier findings were from preclinical studies. In acute ischemic stroke patients, the net benefit of IV tPA treatment is well established.
The discrepancy between the results of the present study and the Intensive Blood Pressure Control After Endovascular Thrombectomy for Acute Ischemic stroke (ENCHANTED2/MT) should be acknowledged. In the ENCHANTED2/MT, patients not administered IV tPA showed a significant benefit from less intensive treatment. 5 However, subjects in the present study who did not receive IV tPA showed a nonsignificant trend favoring less intensive treatment (conventional BP management). 5 We hypothesized that the discrepancy in outcomes observed in patients treated with IV tPA was due to differences in risk factors between studies. For example, atrial fibrillation was twice as common in the OPTIMA-BP trial (48.3%) compared with the ENCHANTED2/MT (22.3%). Furthermore, the OPTIMAL-BP trial included a higher proportion of embolic large-vessel occlusion cases (228/302, 75.5%) compared with the ENCHANTED2/MT (282/816, 34.6%). Embolic strokes are more susceptible to reperfusion injury and malignant cerebral edema.24,25 Finally, the imbalance in patient distribution between the IV tPA and non-IV tPA groups increased the possibility of random findings. Further studies or individual patient data meta-analyses are needed to clarify these findings.
In the present study, IV tPA use did not affect the occurrence of sICH or any ICH. The findings indicate that, despite hemorrhage concerns of IV tPA use, current guideline-recommended BP management (<180/105 mmHg), does not lead to an increase incidence of sICH in patients who received bridging therapy.
In the non-IV tPA group, the intensive BP lowering resulted in a worse outcome at 3 months compared with conventional BP management, but the difference was not statistically significant. However, the notable 11.8% risk difference raises concerns regarding potential negative effects of intensive BP lowering in patients undergoing EVT alone.
This study had several limitations. First, the OPTIMAL-BP trial was not intended to evaluate the effects of BP lowering in patients receiving IV tPA. The analyses were post hoc, involving small patient groups and multiple comparisons, which increased the risk of type 1 errors. Meta-analyses of multiple randomized controlled trials, especially with individual patient-level data, may provide a more comprehensive understanding of this subgroup. These analyses could lead to more robust conclusions about their associated outcomes. Second, because the participants in the OPTIMAL-BP trial were all Koreans, the results should be interpreted with consideration of potential ethnic differences. Finally, the potential for interobserver variability exists in the determination of malignant cerebral edema. We allowed local investigators to determine the presence of malignant cerebral edema as rapid neurological deterioration with substantial brain swelling within 36 h. They made a diagnosis based on clinical correlation, with supporting imaging studies. We believe this approach is more practical than relying solely on imaging.
Conclusion
In this subgroup analysis of the OPTIMAL-BP trial, patients receiving intensive BP management for 24 h after receiving IV tPA before EVT were less likely to achieve favorable outcome at 3 months compared with those with conventional BP management. These results suggested that intensive BP lowering for 24 h after EVT may negatively impact outcomes, particularly in patients who received IV tPA before EVT. Further studies, including individual patient data meta-analyses, are required to draw more robust conclusions.
Supplemental Material
sj-docx-1-wso-10.1177_17474930251315630 – Supplemental material for Effects of blood pressure lowering in patients treated with intravenous thrombolysis before endovascular thrombectomy
Supplemental material, sj-docx-1-wso-10.1177_17474930251315630 for Effects of blood pressure lowering in patients treated with intravenous thrombolysis before endovascular thrombectomy by Jaeseob Yun, Kwang Hyun Kim, Jae Wook Jung, Young Dae Kim, JoonNyung Heo, Hyungwoo Lee, Jin Kyo Choi, In Hwan Lim, Soon-Ho Hong, Byung Moon Kim, Dong Joon Kim, Na Young Shin, Bang-Hoon Cho, Seong Hwan Ahn, Hyungjong Park, Sung-Il Sohn, Jeong-Ho Hong, Tae-Jin Song, Yoonkyung Chang, Gyu Sik Kim, Kwon-Duk Seo, Kijeong Lee, Jun Young Chang, Jung Hwa Seo, Sukyoon Lee, Jang-Hyun Baek, Han-Jin Cho, Dong Hoon Shin, Jinkwon Kim, Joonsang Yoo, Minyoul Baik, Kyung-Yul Lee, Yo Han Jung, Yang-Ha Hwang, Chi Kyung Kim, Jae Guk Kim, Chan Joo Lee, Sungha Park, Soyoung Jeon, Hye Sun Lee, Sun U Kwon, Il Hyung Lee, Oh Young Bang, Ji Hoe Heo and Hyo Suk Nam in International Journal of Stroke
Supplemental Material
sj-docx-2-wso-10.1177_17474930251315630 – Supplemental material for Effects of blood pressure lowering in patients treated with intravenous thrombolysis before endovascular thrombectomy
Supplemental material, sj-docx-2-wso-10.1177_17474930251315630 for Effects of blood pressure lowering in patients treated with intravenous thrombolysis before endovascular thrombectomy by Jaeseob Yun, Kwang Hyun Kim, Jae Wook Jung, Young Dae Kim, JoonNyung Heo, Hyungwoo Lee, Jin Kyo Choi, In Hwan Lim, Soon-Ho Hong, Byung Moon Kim, Dong Joon Kim, Na Young Shin, Bang-Hoon Cho, Seong Hwan Ahn, Hyungjong Park, Sung-Il Sohn, Jeong-Ho Hong, Tae-Jin Song, Yoonkyung Chang, Gyu Sik Kim, Kwon-Duk Seo, Kijeong Lee, Jun Young Chang, Jung Hwa Seo, Sukyoon Lee, Jang-Hyun Baek, Han-Jin Cho, Dong Hoon Shin, Jinkwon Kim, Joonsang Yoo, Minyoul Baik, Kyung-Yul Lee, Yo Han Jung, Yang-Ha Hwang, Chi Kyung Kim, Jae Guk Kim, Chan Joo Lee, Sungha Park, Soyoung Jeon, Hye Sun Lee, Sun U Kwon, Il Hyung Lee, Oh Young Bang, Ji Hoe Heo and Hyo Suk Nam in International Journal of Stroke
Supplemental Material
sj-docx-3-wso-10.1177_17474930251315630 – Supplemental material for Effects of blood pressure lowering in patients treated with intravenous thrombolysis before endovascular thrombectomy
Supplemental material, sj-docx-3-wso-10.1177_17474930251315630 for Effects of blood pressure lowering in patients treated with intravenous thrombolysis before endovascular thrombectomy by Jaeseob Yun, Kwang Hyun Kim, Jae Wook Jung, Young Dae Kim, JoonNyung Heo, Hyungwoo Lee, Jin Kyo Choi, In Hwan Lim, Soon-Ho Hong, Byung Moon Kim, Dong Joon Kim, Na Young Shin, Bang-Hoon Cho, Seong Hwan Ahn, Hyungjong Park, Sung-Il Sohn, Jeong-Ho Hong, Tae-Jin Song, Yoonkyung Chang, Gyu Sik Kim, Kwon-Duk Seo, Kijeong Lee, Jun Young Chang, Jung Hwa Seo, Sukyoon Lee, Jang-Hyun Baek, Han-Jin Cho, Dong Hoon Shin, Jinkwon Kim, Joonsang Yoo, Minyoul Baik, Kyung-Yul Lee, Yo Han Jung, Yang-Ha Hwang, Chi Kyung Kim, Jae Guk Kim, Chan Joo Lee, Sungha Park, Soyoung Jeon, Hye Sun Lee, Sun U Kwon, Il Hyung Lee, Oh Young Bang, Ji Hoe Heo and Hyo Suk Nam in International Journal of Stroke
Footnotes
Author contributions
J.Y. and H.S.N. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have no financial conflicts of interest except for J.K. and J.Y., who report research grants from Chong Kun Dang Pharm.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of Patient-Centered Clinical Research Coordinating Center (PACEN) funded by the Ministry of Health & Welfare, Republic of Korea (Grant No.: RS-2024-00398053) and a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (Grant No.: RS-2023-00265165).
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.