
Abstract
Introduction:
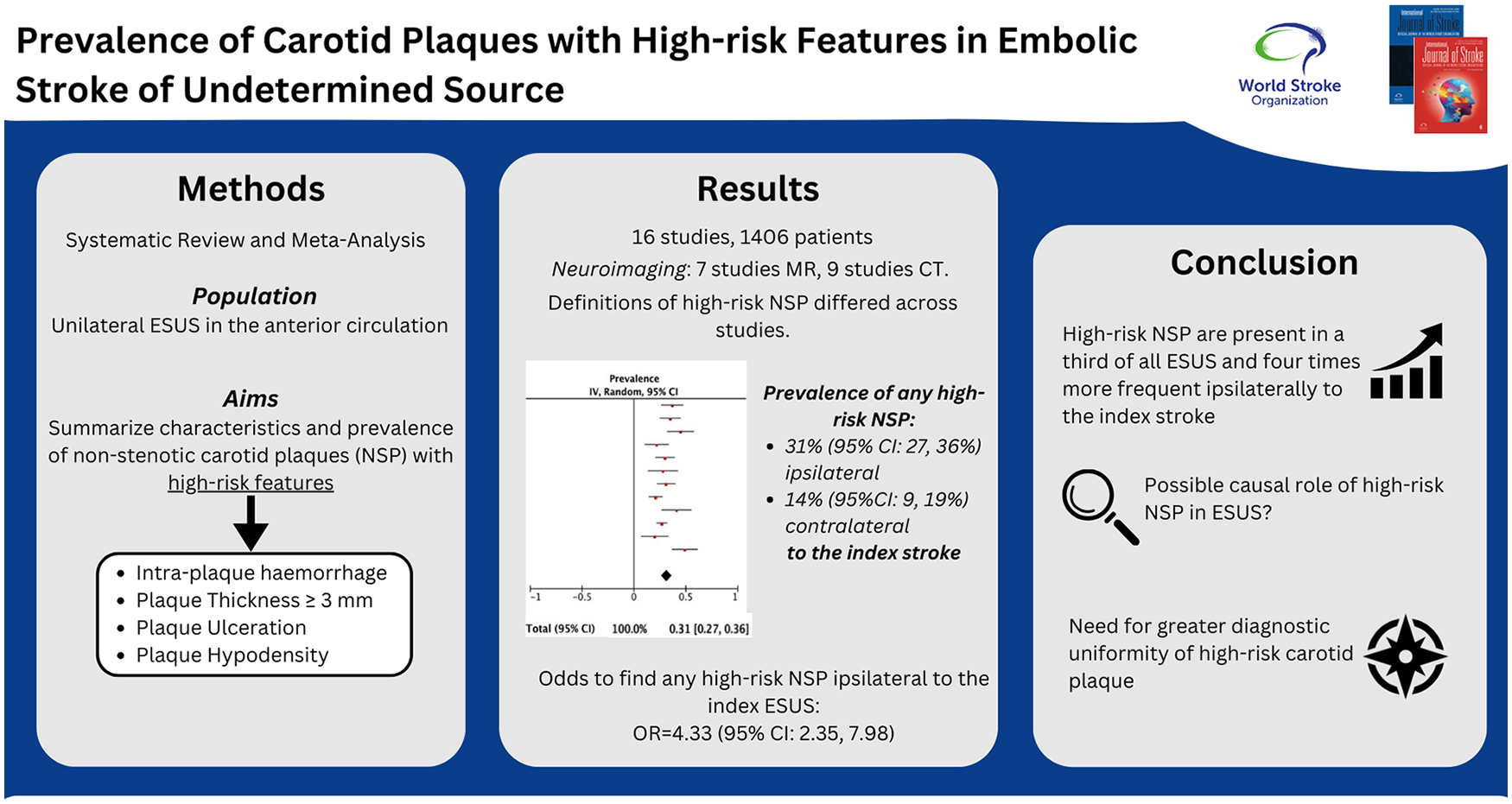
Recent evidence suggests a possible role of non-stenotic carotid atherosclerotic plaques in the etiology of embolic stroke of undetermined source (ESUS).
Methods:
We conducted a systematic review and meta-analysis of prevalence and characteristics of non-stenotic carotid plaques (NSPs) with high-risk features (complicated NSP) in internal carotid artery in unilateral ESUS in the anterior circulation. We searched MEDLINE and Ovid-Embase databases. High-risk features were intraplaque hemorrhage, thickness ⩾ 3 mm, ulceration, and hypodensity. We assessed the risk of bias (RoB), extracted the data, calculated the pooled prevalence and 95% confidence intervals (CI) using Inverse Variance Weighting method, and Random Effect models.
Results:
We included 16 studies and 1406 patients with different imaging for NSP assessment (1 ultrasound, 11 computed tomography (CT)-angiography, 4 magnetic resonance (MR) angiography). The RoB was moderate to low in most studies. Definition of complicated NSP differed across studies. The combined prevalence of any complicated NSP was 31% (95% CI = 27–36%) ipsilateral and 14% (95% CI = 9–19%) contralateral to the index stroke, the finding of any high-risk NSP was fourfold higher ipsilateral to the index stroke (OR = 3.63; 95% CI = 2.09–6.33). The prevalence of single high-risk features ipsilateral to ESUS was as follows: 35% (95% CI = 30–41%) for thickness ⩾ 3 mm; 24% (95% CI = 8–39%) for ulceration; 45% (95% CI = −2; 93%) for hypodensity, 16% (95% CI = 5–26%) for intraplaque hemorrhage.
Conclusion:
Complicated NSPs are present in around a third of all ESUS, and are four times more frequent ipsilaterally to the index stroke. Our results confirm the possible causal role in ESUS and highlight the need for greater diagnostic uniformity of plaque at risk.
Keywords
Introduction
Embolic stroke of undetermined source (ESUS) accounts up to a quarter of all ischemic strokes1,2 and represents a challenge for the management of secondary prevention. Atherosclerosis involving large vessels is responsible for ischemic stroke in around 10–15% of all strokes 3 with carotid and vertebral arteries being the most affected vessels.4,5 In the anterior circulation (i.e. carotid arteries), the causal role of the atherosclerotic plaque is confirmed when the plaque causes a narrowing of at least 50% in the vessel lumen. However, emerging evidence6–9 suggests that atherosclerotic plaques determining less than 50% luminal narrowing, namely non-stenotic plaque (NSP), are found in a relevant proportion of ESUS patients, particularly in the anterior circulation in the bulb of the internal carotid artery (ICA),10,11 leading to the hypothesis that in ESUS patients, NSP may be a cause of stroke. 2 The embolic potential NSPs are related to the so-called high-risk features of the plaque.12,13 High-risk feature is an umbrella term that encompasses plaque characteristics, such as hypodensity, plaque hemorrhage, ulceration, and other features, although there is no consensus regarding the pathogenetic role of each feature. Moreover, high-risk features have been investigated with various imaging techniques, such as magnetic resonance or computed tomography angiography (MR-based techniques or CTA, respectively), ultrasound (US), and fluorodeoxyglucose positron emission tomography (FDG-PET),13,14 but evidence regarding the optimal imaging technique is lacking.
Given the growing literature amount of this topic, we aim to summarize characteristics, definitions, and prevalence of high-risk features of NSP in patients with unilateral ESUS in the anterior circulation.
Methods
This study is compliant with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 15 Data search, extraction, analysis, and interpretation were performed following a prespecified study protocol developed by the investigators (not registered or published).
Search strategy, selection criteria, and data extraction
We searched PubMed and Ovid-Embase for the published studies reporting carotid plaque imaging characteristics in ESUS patients, from April 2012 to September 1, 2024 using the following search strategies, for PubMed: (Stroke OR transient ischemic attack OR cerebrovascular event) AND (plaque OR atherosclerosis OR atherosclerotic OR nonstenosing OR non-stenotic OR “non stenotic” OR “carotid artery disease*”) AND (cryptogenic OR “embolic stroke” OR “stroke of undetermined source*” OR ESUS OR “unknown cause*” OR “unknown etiology” OR “unknown origin*”) and the following for Ovid-Embase: (“cerebrovascular accident”/exp OR “cerebrovascular accident” OR “transient ischemic attack”/exp OR “transient ischemic attack”) AND (“atherosclerotic plaque”/exp OR “atherosclerotic plaque” OR “atherosclerosis”/exp OR “atherosclerosis” OR “carotid artery disease”/exp OR “carotid artery disease” OR atherosclerotic OR nonstenosing OR “non stenotic”) AND (“cardioembolic stroke”/exp OR “cardioembolic stroke” OR cryptogenic OR “stroke of undetermined source” OR esus OR “unknown cause” OR “unknown etiology” OR “unknown origin”) AND ([english]/lim OR (french) OR (italian) AND ((article) OR (article in press)/lim OR (conference paper)/lim OR (conference review)/lim OR (letter) OR (review)lim) NOT (“clinical trial” OR “randomized controlled trial”).
The systematic review was conducted and documented according to PRISMA 2020 statement. 16 We applied the following inclusion criteria: (1) English, French, and Italian written articles; (2) patients with ischemic stroke in the anterior circulation with unknown origin (ESUS) as defined in each index study according to Trial of Org 10172 in Acute Stroke Treatment (TOAST), ASCOD phenotyping (A: atherosclerosis; S: small-vessel disease; C: cardiac pathology; O: other causes; D: dissection) and Hart et al’s 17 definition from 2014; (3) defined and described characteristics of high-risk plaques in the carotid bulb. Case reports, conference abstracts, study protocols, and unpublished studies were not included. We excluded experimental or animal studies. RAYYAN Software® 18 was used to remove duplicates and screen titles and abstract by two independent authors (C.M.R. and A.G.). Disagreements about study inclusion were resolved through a third expert reviewer (F.A.). Full text of potentially eligible records was then independently evaluated by two independent authors. The reference list of eligible studies was screened to identify additional publications suitable for our purposes not included in the original list.
The following data were extracted from each full text: (1) year of publication; (2) study design; (3) number of patients; (4) demographic characteristics and risk factors of patients; (5) characteristics of NSP; (6) plaque imaging; (7) imaging delay from the index event (stroke); (8) high-risk features assessed; (9) frequency of any NSP with high-risk features and frequency of each feature when available.
To calculate the pooled prevalence of a complicated plaque ipsilateral to the ESUS, we included the following: (1) studies where the definition of complicated NSP was stated in the methods and (2) studies that focused on a single NSP high-risk features. We excluded from the pooled analysis: (1) studies that reported the frequency of single NSP high-risk features without reporting a definition of complicated plaque and (2) studies that analyzed putative features not present in any other study.
We included in the study the high-risk features with data regarding prevalence in at least two studies, thus we considered: (1) plaque thickness ⩾ 3 mm; (2) plaque ulceration; (3) hypodensity; and (4) intraplaque hemorrhage.
The risk of bias (RoB) of each included study was determined with the RoB tool for Prevalence Studies. 19
Outcomes
Our main outcome of interest was the pooled prevalence of complicated NSP (with at least one high-risk feature), as defined at the study level. When available, we calculated the pooled prevalence of each high-risk feature.
Statistics
Data were pooled in the meta-analysis when at least three studies had available data on the prevalence of complicated NSP. In all the analyses, we used a Generic Inverse Variance approach with random effects model with DerSimonian–Laird weights. The pooled prevalence and corresponding 95% confidence interval (CI) were provided. Statistical heterogeneity was assessed with I2 statistics and visual inspection of forest plots. Values of ⩽ 25%, 25–50%, and ⩾ 50% were defined as low, moderate, and high degrees of heterogeneity, respectively. The risk of having a complicated NSP in the carotid ipsilateral to the index stroke compared with the contralateral carotid was calculated and provided as odds ratio (OR) and corresponding 95% CIs. Publication bias was explored on funnel plots. All the analyses were performed in September 2024 using the meta-analysis software RevMan 5.3.
Results
The initial search retrieved 2157 articles. After removing duplicates (N = 379, 18%), we included 1763 studies. After screening for title and abstract, 42 studies were candidates for inclusion. We finally selected 16 studies for the systematic review, with a total of 1406 patients. Selection process is illustrated in Figure 1. Three studies were excluded because of overlapping population with other included studies.20–22 We included 7 retrospective and 9 prospective studies6,23–37 (Table 1), 10 were single-centered and 6 were multicentered studies, with a sample size ranging from a minimum of 35 and a maximum of 273 patients. Studies were performed between 2013 and 2024, eight were from America, one from Asia, five from Europe, and two were international. ESUS was defined in index studies as follows: in seven with TOAST, in one with ASCOD, in seven according to Hart et al’s definition from 2014, in one study, there was no clear reference to any classification.
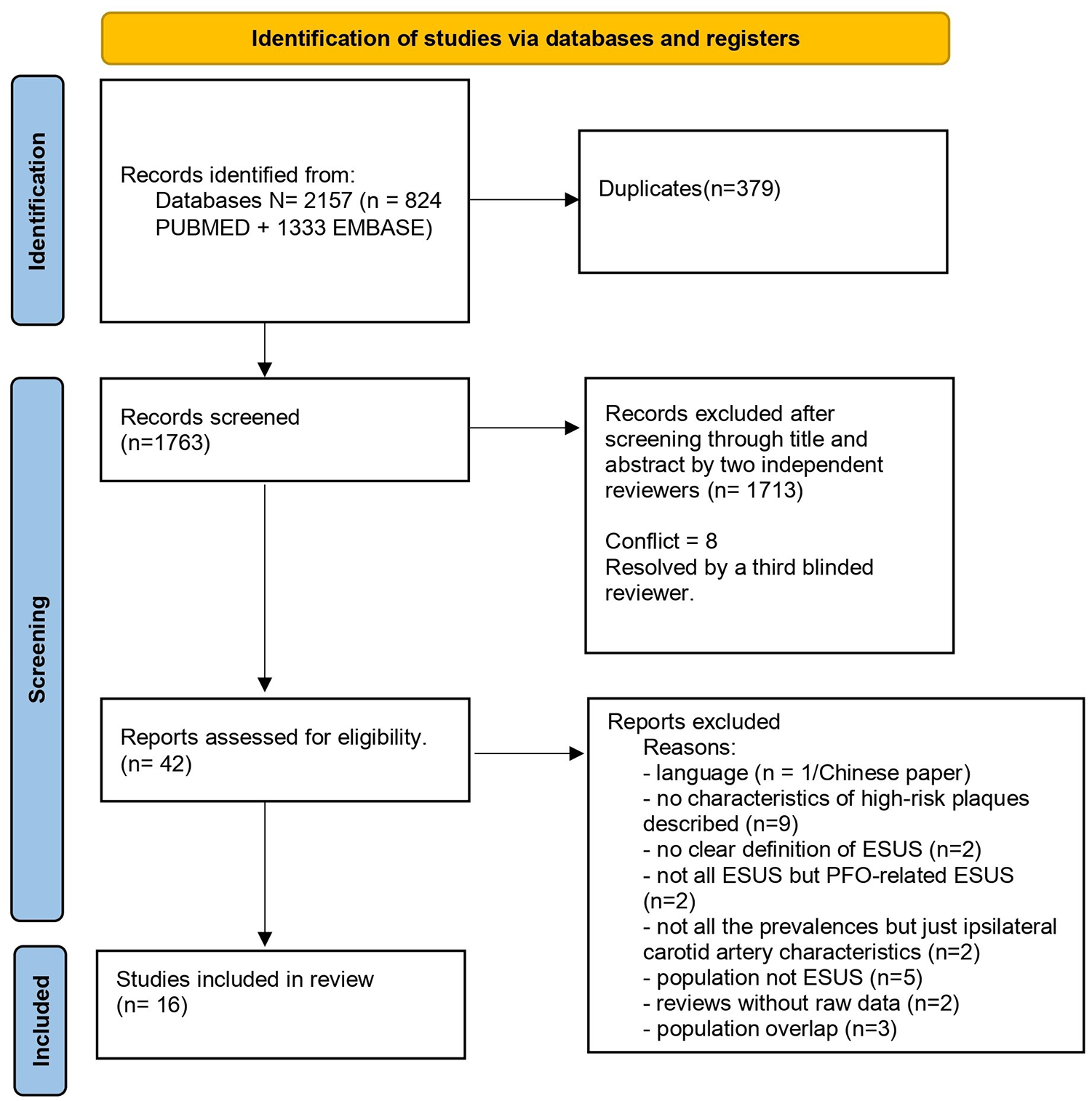
PRISMA flow diagram of included studies.
Characteristics of included studies in the qualitative synthesis.
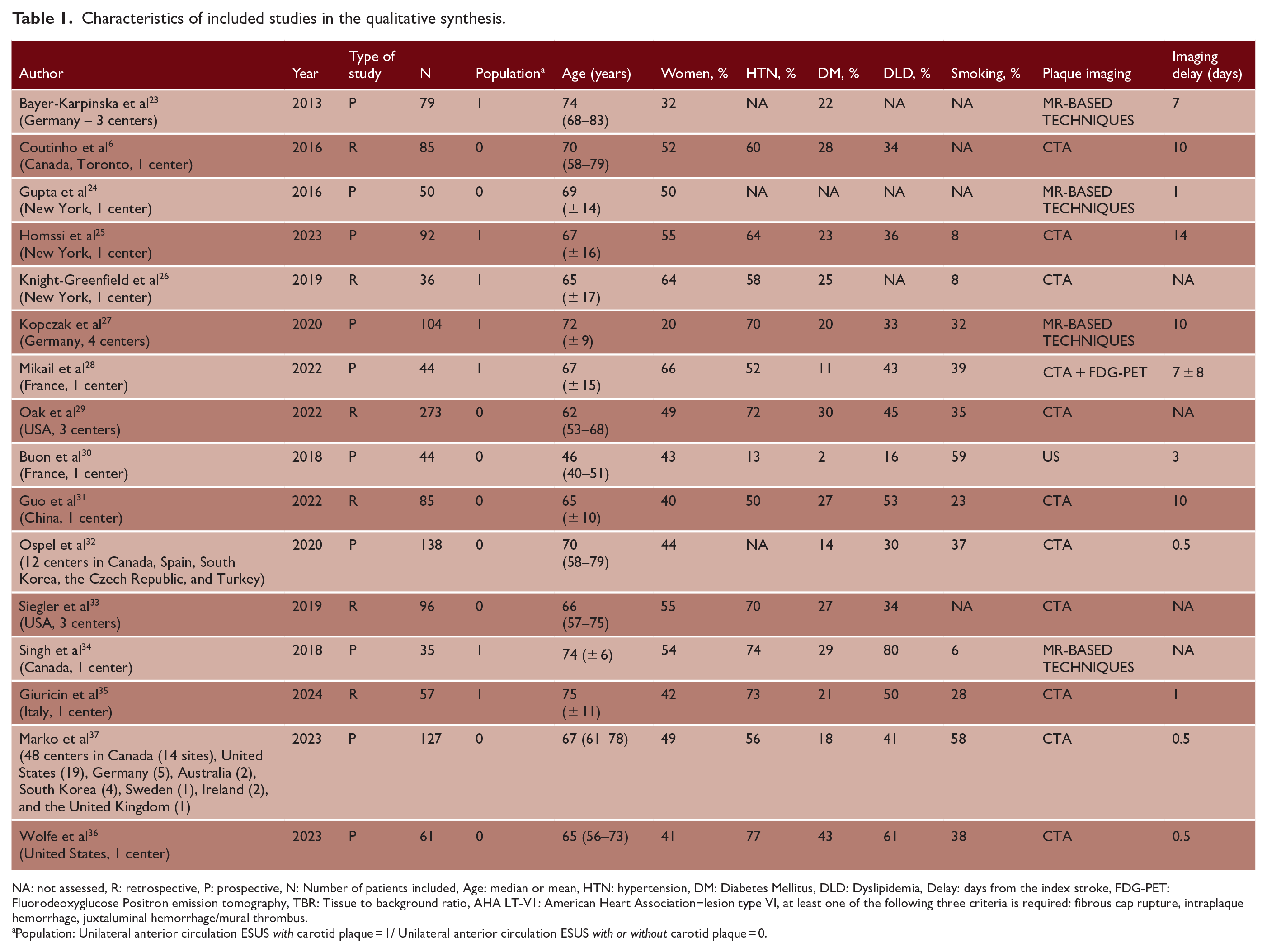
NA: not assessed, R: retrospective, P: prospective, N: Number of patients included, Age: median or mean, HTN: hypertension, DM: Diabetes Mellitus, DLD: Dyslipidemia, Delay: days from the index stroke, FDG-PET: Fluorodeoxyglucose Positron emission tomography, TBR: Tissue to background ratio, AHA LT-V1: American Heart Association−lesion type VI, at least one of the following three criteria is required: fibrous cap rupture, intraplaque hemorrhage, juxtaluminal hemorrhage/mural thrombus.
Population: Unilateral anterior circulation ESUS with carotid plaque = 1/ Unilateral anterior circulation ESUS with or without carotid plaque = 0.
In 1 study, high-risk features of NSP were assessed with doppler ultrasound, in 11 studies with CTA, and in 4 studies with MR-based techniques. In one study, a PET-FDG was added to CTA. All NSP assessments were performed between 0.5 and 14 days from the index stroke. The definition of high-risk plaque differed across studies: thickness ⩾ 3 mm was used in 9 studies, ulceration in 8 studies, hypodensity in 3, intraplaque hemorrhage in 3, and other definitions were also used (Figure 2 and Supplemental Table 1). Overall, RoB was generally low (Supplemental Table 2).
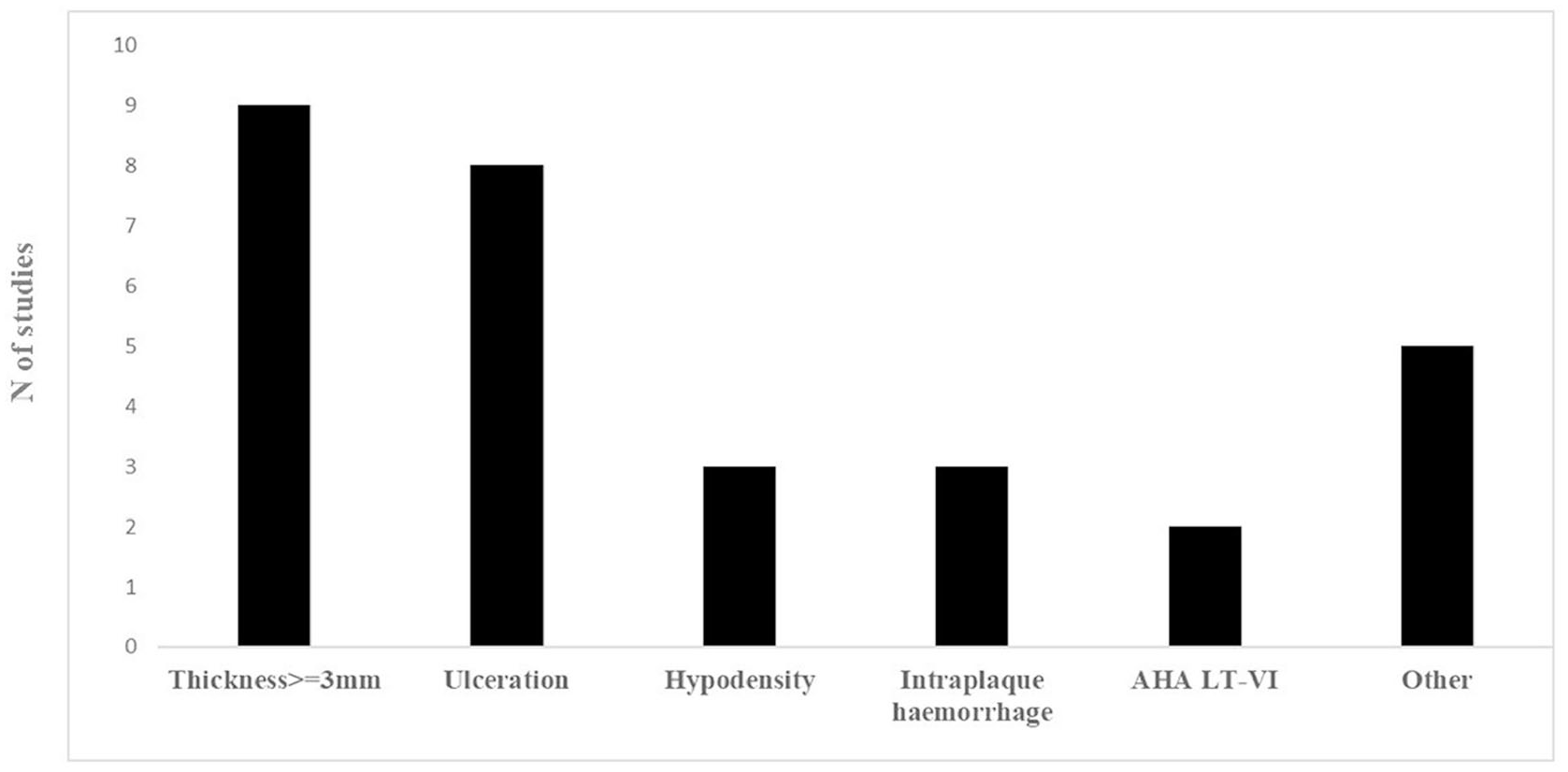
Definition of complicated NSP across different studies. AHA LT-V1: American Heart Association−lesion type VI. At least one of the following three criteria is required: fibrous cap rupture, intraplaque hemorrhage, juxtaluminal hemorrhage/mural thrombus.
Quantitative synthesis
Of the 16 studies included for the qualitative synthesis, in 4 studies (363 patients, 26%), the extraction of the prevalence of at least one high-risk feature was not possible and therefore excluded from the quantitative synthesis.30–33 This left 12 studies and 1043 (74%) patients with ESUS in the anterior circulation and available prevalence of complicated NSP and high-risk features for the quantitative analysis.
Considering all the imaging techniques, the pooled prevalence of any complicated NSP was 31% (95% CI = 27–36%) ipsilateral and 14% (95% CI = 9–19%) contralateral (Figure 3 and supplemental Figure 1). Statistical heterogeneity was high for both ipsilateral (I2 = 65%) and contralateral (I2 = 82%). We found no evidence of publication bias (Supplemental Figure 2).
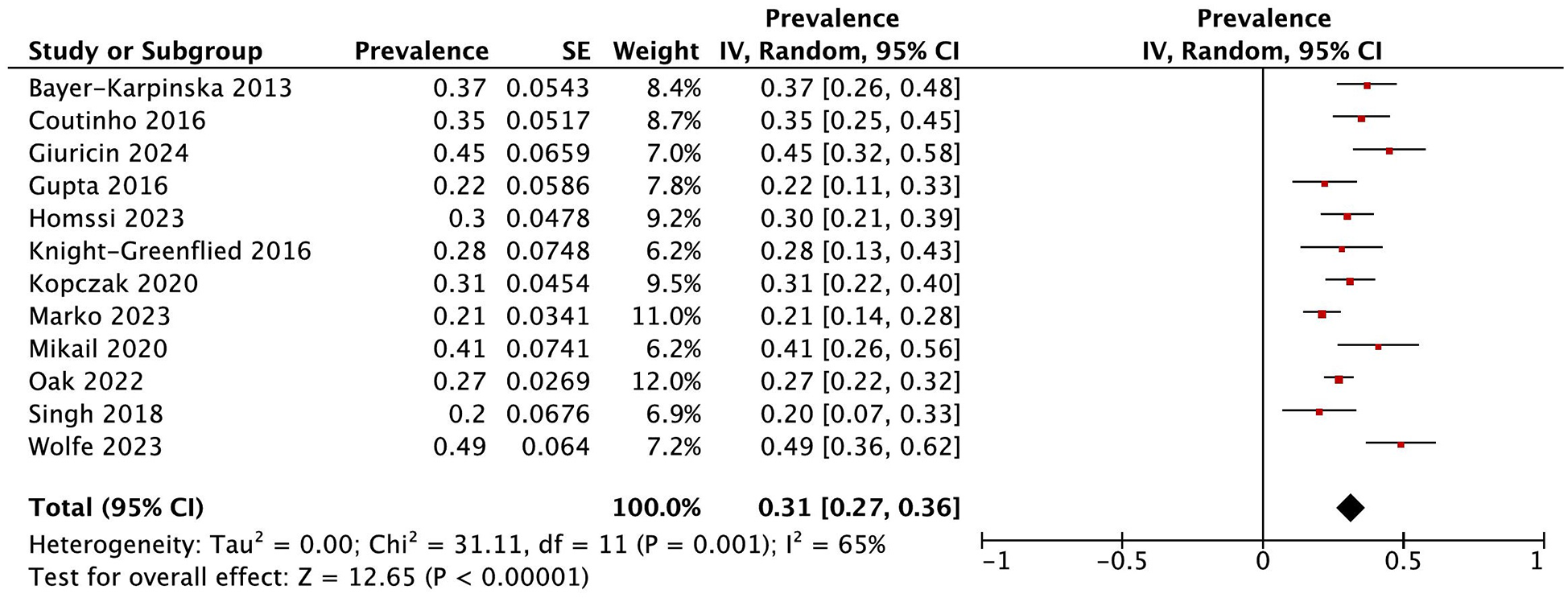
Pooled prevalence of any complicated NSP ipsilateral to the index stroke.
For studies performed with CTA as diagnostic method (N = 11), the pooled prevalence of any complicated plaque was available in 7 studies and was 33% (95% CI = 26–39%) ipsilateral, with high statistical heterogeneity (I2 = 73%) and 18% (95% CI = 11–24%) contralateral to the ESUS (Figure 4(a) and supplemental Figure 3(a)). For MR-based techniques studies (N = 4), the pooled prevalence of any complicated plaque was 28% (95% CI = 21–36%) ipsilateral, with moderate statistical heterogeneity (I2 = 46%) and 7% (95% CI = 1–13%) contralateral to the ESUS (Figure 4(b) and supplemental Figure 3(b)). For studies with ESUS patients with and without NSP (N = 5), the prevalence of any complicated plaque was 30% (95% CI = 22–38%, I2 = 77%), and for studies with ESUS with NSP, the prevalence was 34% (95% CI = 0.34–0.39%, I2 = 13%) (Supplemental Figure 4). The overall risk to find a complicated NSP in the carotid ipsilateral to the index stroke was more than threefold higher (OR = 3.63; 95% CI = 2.09–6.33) compared to the contralateral side.
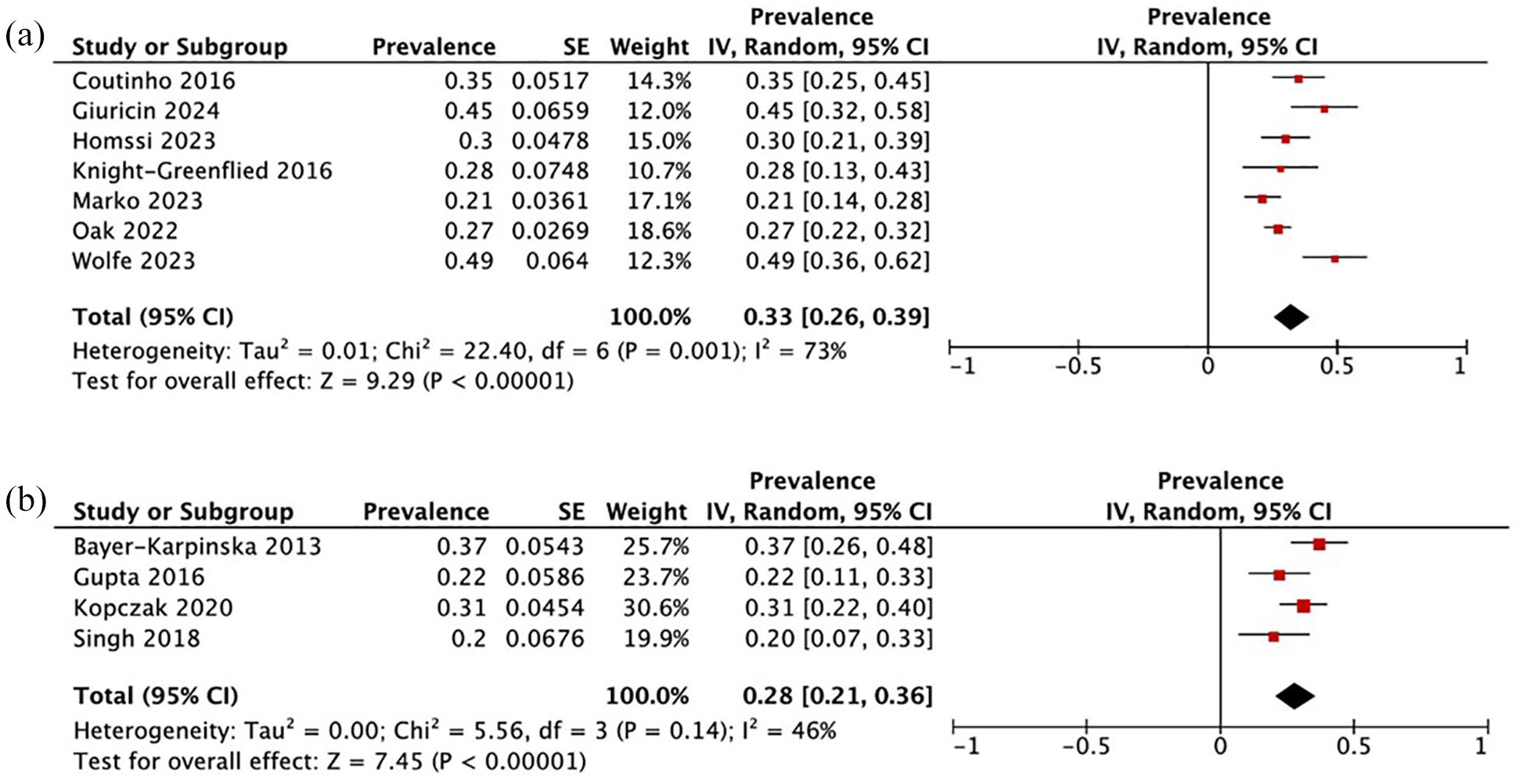
Pooled prevalence of any high-risk feature in NSP ipsilateral to the index stroke according to diagnostic technique: (a) CTA; (b) MR-based techniques.
Prevalence of single high-risk features
We obtained data about the prevalence of the single high-risk features in 10 of the included studies. The prevalence of plaque thickness ⩾ 3 mm in ipsilateral and contralateral carotid artery was 35% (95% CI = 30–41%) and 20% (95% CI = 8–33%), respectively, with heterogeneity ranging from moderate (ipsilateral I2 = 54%) to high (contralateral I2 = 88%) (Figure 5(a) and supplemental Figure 5(a)); for ulceration, 24% (95% CI = 8–39%) ipsilateral and 9% (95% CI = 2–15%) contralateral, respectively, with high heterogeneity (ipsilateral I2 = 98%; contralateral I2 = 80%) (Figure 5(b) and supplemental Figure 5(b)); for hypodensity 45% (95% CI = −2; 93%) ipsilateral and 10% (95% CI = 5–14%) contralateral with high heterogeneity (ipsilateral I2 = 99%; contralateral I2 = 80%) (Figure 5(c) and supplemental Figure 5(c)); for intraplaque hemorrhage in the carotid artery ipsilateral to the stroke (Figure 5(d)), it was 16% (95% CI = 5–26%) with low heterogeneity (I2 = 19%).
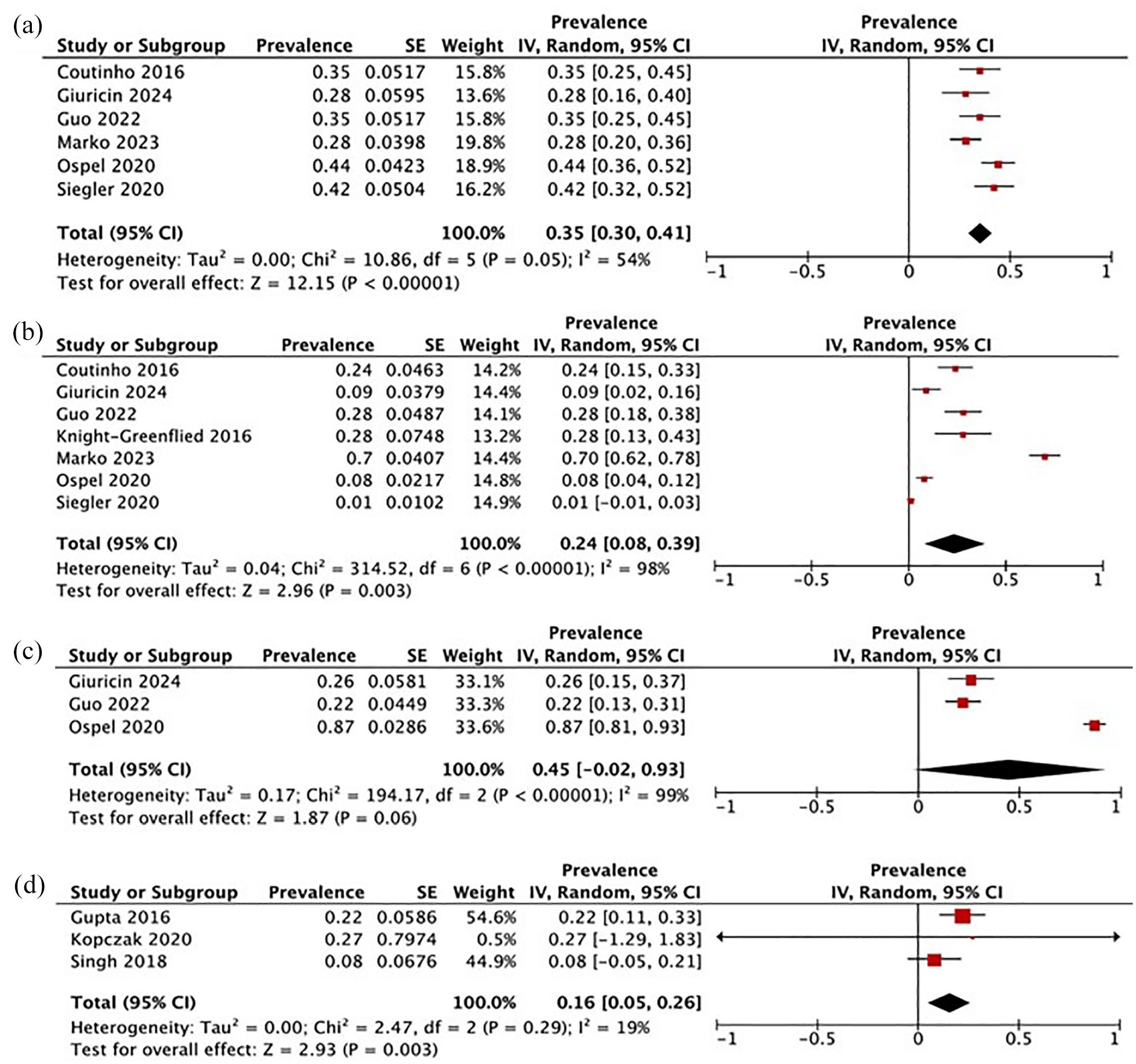
Prevalence of single high-risk features in NSP ipsilateral to the index stroke: (a) plaque thickness ⩾ 3 mm; (b) ulcerated plaque; (c) plaque hypodensity; (d) intraplaque hemorrhage.
Discussion
In this systematic review and meta-analysis of patients with unilateral ESUS in the anterior circulation, we found that the prevalence of complicated NSP (with at least one high-risk feature) was twice as high in the carotid artery ipsilateral to the ESUS compared to the contralateral. Accordingly, the odds of any high-risk feature were more than three times higher in the carotid ipsilateral to the index stroke compared to the contralateral one. The most frequent feature was intraplaque hypodensity and the less frequent was intraplaque hemorrhage. We found different definitions of complicated NSP across studies, possibly explaining the high statistical heterogeneity that we observed in the analysis.
Although NSP may potentially have an important role also in other stroke etiologies, we focused on patients with ESUS. In fact, around 20% of patients, the cause of the ischemic stroke remains unknown and poses a relevant challenge for the clinician targeting the secondary prevention. 2 The role of undetected atrial fibrillation in the ESUS population has been questioned, 2 and the neutral results of clinical trials comparing oral anticoagulants with antiplatelets in patients with ESUS38,39 suggested that the cardioembolic etiology is only partly responsible of ESUS, underscoring the need for further efforts in finding other causes of the stroke. An increasing amount of evidence suggested that certain atherosclerotic plaque characteristics, even with stenosis < 50% of the vessel lumen, may have a causal role in the cerebral ischemia6,7,11 and a study suggested that around 15% of ESUS might be reclassified into large vessel atherosclerosis in the presence of complicated NSP. 40 According to our results, the assumption of the hypothesized pathogenetic role of any complicated NSP would lead to around a third of ESUS patients reclassified into stroke from large vessel atherosclerosis. However, we observed inconsistencies in definition and identification of high-risk features of NSP.
Features of high-risk atherosclerotic plaques have been previously identified 13 outlining preferred imaging modalities to investigate plaques at risk, which were reported in around 40% of NSP.10,11 We observed a less prevalence of this figure and found a relevant heterogeneity in defining a complicated plaque across studies and therefore in prevalence of complicated NSP. MR-based techniques and CTA were the most frequent imaging modalities used to investigate complicated NSP, whereas ultrasound alone and FDG-PET combined to MR-based techniques or CTA were used in fewer studies, reflecting the complexity of the imaging technique itself and the limited diagnostic accuracy for some plaque characteristics, such as intraplaque hemorrhage. Interestingly, our subgroup analysis showed that the prevalence of any high-risk NSP was similar between CTA and MR-based techniques, reinforcing the main finding in around a third of ESUS. Furthermore, when considering only patients with ESUS with and without NSP (i.e. the whole ESUS population in clinical practice), the prevalence of NSP with high-risk features was only slightly lower than considering patients with ESUS only with NSP, reinforcing our main result about prevalence of any complicated NSP.
An operative definition of complicated NSP should be employed for large multicenter studies with standardized imaging modalities and protocols to better define the causal role of NSP and for inclusion of patients in clinical trials of secondary prevention. We observed different prevalence values across high-risk features, reflecting different biological mechanisms underlying their development during the atherosclerotic process and possibly the relative pathogenic role, but also different techniques for plaque assessment. We found hypodensity as the most frequent, although the pooled prevalence was calculated from only three studies and data extracted only from CTA studies, followed by plaque thickness and ulceration, and intraplaque hemorrhage as the least frequent. Such results may inform clinicians and researchers about expected findings when approaching NSP in ESUS. However, they may also reflect the different diagnostic accuracy of different imaging techniques requested for the assessment of each feature: for example, the prevalence of plaque thickness and intraplaque hemorrhage was investigated respectively with CTA and MR-based techniques. Further cross-validation studies and comparisons across imaging techniques (e.g. CTA, MR-based techniques, US) are requested to establish the standards for diagnostic accuracy for relevant high-risk features. Implementation of Artificial Intelligence software may potentially enhance the diagnostic accuracy in detecting some plaque characteristics. 13 Although the prevalence differed with the type of high-risk NSP feature, we found that the cumulative odds to find at least one complicated NSP were more than three times more likely in the carotid ipsilateral to the ischemic stroke compared with the contralateral, thus supporting the causal role of complicated NSP in ESUS. The therapeutic implications of this finding should be evaluated in future studies. Besides strict management of risk factors, lipid lowering drugs may help plaque stabilization, 41 and dual antiplatelet therapy may reduce the risk of stroke recurrence; however, net benefits, timing and the length of treatment need to be balanced toward the risk of bleeding. Although observational data may provide data regarding the risk of stroke recurrence, randomized controlled trials in this important subgroup of patients (i.e. ESUS with NSP) are warranted.
Our study has limits. Although we summarized characteristics of complicated NSP, we found relevant differences in definitions of high-risk plaque and imaging acquisition protocols across studies, and this may lend imprecision to our estimates of prevalence. For some high-risk features, such as intraplaque hemorrhage and hypodensity, we found high statistical heterogeneity, suggesting that the summarized prevalence data should be taken with caution, highlighting the need for further data to provide more precise prevalence estimates. Again, we did not have enough data to provide estimates regarding the prevalence of more than one feature, which could occur in clinical practice and potentially increase the odds of the causal role of the NSP. Finally, MR-based techniques and CTA have been used to assess different plaque characteristics: the use of a single imaging modality may underestimate the prevalence of certain plaque characteristics, although the prevalence of any high-risk NSP feature was similar in the subgroup analysis. In this regard, it should be noted that other plaque characteristics, such as necrotic core, fibrous cap, atherosclerotic burden, are emerging as high-risk features of NSP, but we were not able to find enough data to summarize the prevalence. We underscore that in selected cases, both imaging techniques (MR-based techniques and CTA) could be adopted since each imaging can add some information to the whole picture, as previously suggested. 7
The strengths of our study include a low RoB for most of the included studies, and the generalizability of results given that studies were from different countries and mainly with good sample size.
Conclusion
Complicated NSPs are present in around a third of all ESUS and around three times more frequent in the carotid ipsilateral to the index stroke. The prevalence of each high-risk feature is variable, with the most frequent being plaque hypodensity and the least frequent being intraplaque hemorrhage. Although more effort is needed to clarify the causal role of NSP in ESUS and to define high-risk features, assessment of NSP may guide clinicians when no clear cause of stroke is found and researchers to design clinical trials for secondary prevention in ESUS.
Supplemental Material
sj-docx-1-wso-10.1177_17474930251317321 – Supplemental material for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis
Supplemental material, sj-docx-1-wso-10.1177_17474930251317321 for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis by Costanza Maria Rapillo, Alessandro Giuricin, Cristina Sarti, Mascia Nesi, Simona Marcheselli, Ivano Lombardo, Rosario Pascarella, Marialuisa Zedde and Francesco Arba in International Journal of Stroke
Supplemental Material
sj-jpg-2-wso-10.1177_17474930251317321 – Supplemental material for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis
Supplemental material, sj-jpg-2-wso-10.1177_17474930251317321 for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis by Costanza Maria Rapillo, Alessandro Giuricin, Cristina Sarti, Mascia Nesi, Simona Marcheselli, Ivano Lombardo, Rosario Pascarella, Marialuisa Zedde and Francesco Arba in International Journal of Stroke
Supplemental Material
sj-jpg-3-wso-10.1177_17474930251317321 – Supplemental material for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis
Supplemental material, sj-jpg-3-wso-10.1177_17474930251317321 for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis by Costanza Maria Rapillo, Alessandro Giuricin, Cristina Sarti, Mascia Nesi, Simona Marcheselli, Ivano Lombardo, Rosario Pascarella, Marialuisa Zedde and Francesco Arba in International Journal of Stroke
Supplemental Material
sj-jpg-4-wso-10.1177_17474930251317321 – Supplemental material for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis
Supplemental material, sj-jpg-4-wso-10.1177_17474930251317321 for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis by Costanza Maria Rapillo, Alessandro Giuricin, Cristina Sarti, Mascia Nesi, Simona Marcheselli, Ivano Lombardo, Rosario Pascarella, Marialuisa Zedde and Francesco Arba in International Journal of Stroke
Supplemental Material
sj-jpg-5-wso-10.1177_17474930251317321 – Supplemental material for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis
Supplemental material, sj-jpg-5-wso-10.1177_17474930251317321 for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis by Costanza Maria Rapillo, Alessandro Giuricin, Cristina Sarti, Mascia Nesi, Simona Marcheselli, Ivano Lombardo, Rosario Pascarella, Marialuisa Zedde and Francesco Arba in International Journal of Stroke
Supplemental Material
sj-jpg-6-wso-10.1177_17474930251317321 – Supplemental material for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis
Supplemental material, sj-jpg-6-wso-10.1177_17474930251317321 for Prevalence of carotid plaques with high-risk features in embolic stroke of undetermined source: Systematic review and meta-analysis by Costanza Maria Rapillo, Alessandro Giuricin, Cristina Sarti, Mascia Nesi, Simona Marcheselli, Ivano Lombardo, Rosario Pascarella, Marialuisa Zedde and Francesco Arba in International Journal of Stroke
Footnotes
Acknowledgements
The authors thank Dr Tessa Piazzini for her help in research strategy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.