
Abstract
Background:
Real-world data on the long-term trends in risk factors, acute antithrombotic strategies, medication adherence, and their impact on the prognosis of minor ischemic stroke (MIS) or transient ischemic attack (TIA) are limited.
Methods:
We analyzed cases of acute MIS (National Institutes of Health Stroke Scale score ⩽ 3) and TIA from the China National Stroke Registries (CNSRs), a series of multicenter, nationwide hospital-based registries in China. Stroke risk factors, acute antithrombotic strategies, and adherence to secondary prevention were compared between CNSR I (2007–2008) and CNSR III (2015–2018). The main outcomes were stroke recurrence, disability (modified Rankin Scale 3–5), and all-cause mortality at 3, 6, and 12 months of follow-up.
Results:
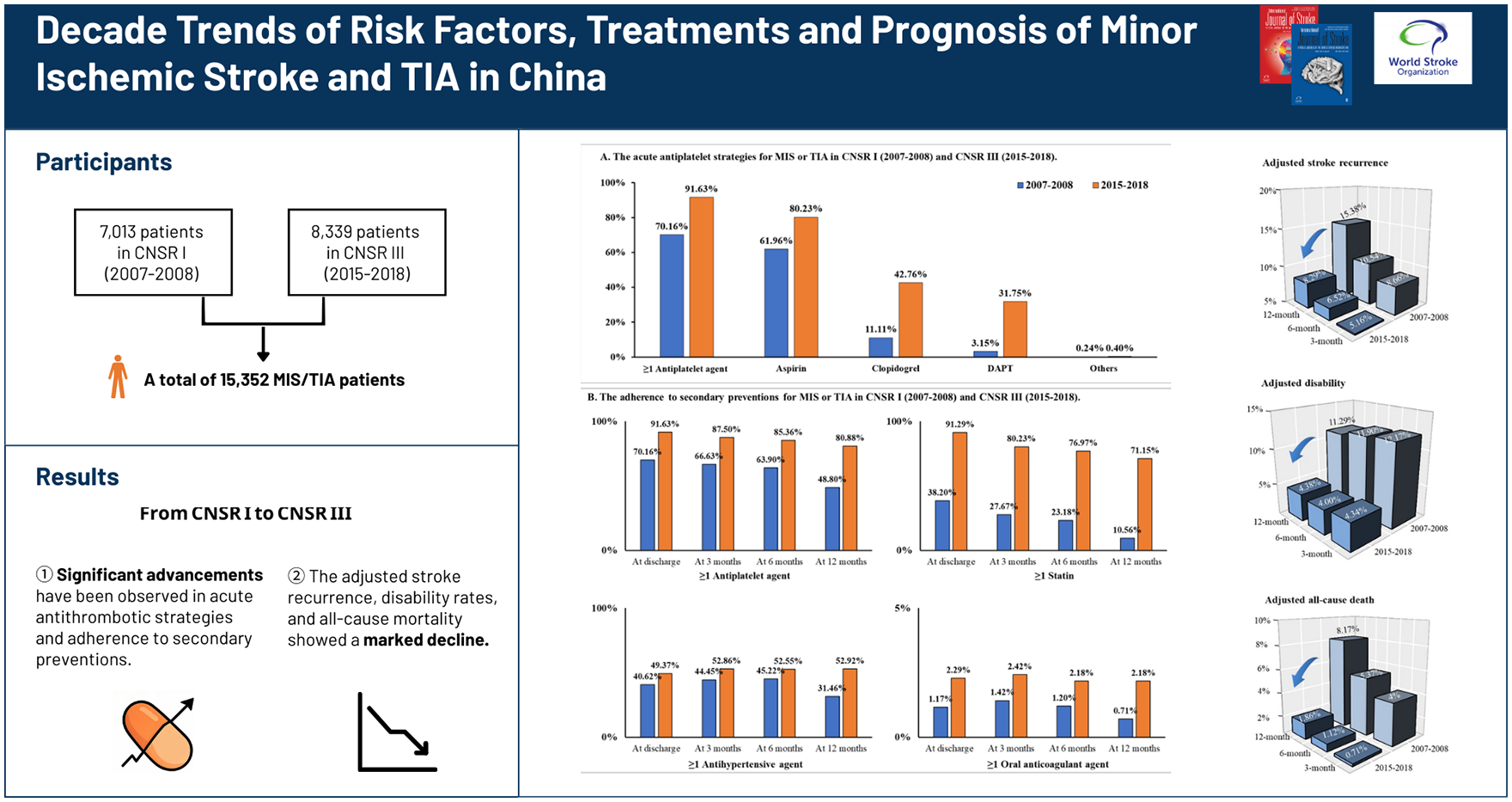
In total, 15,352 patients with acute MIS or TIA were included, including 7,013 patients from CNSR I and 8,339 patients from CNSR III. Over the past decade, there has been a 10-fold increase in the acute use of dual antiplatelet therapy (3.15% in CNSR I vs 31.75% in CNSR III) and a seven-fold increase in statin adherence at the 12 month follow-up (10.56% in CNSR I vs 71.15% in CNSR III). It was also observed that the adjusted cumulative incidence of stroke recurrence (15.38% [15.29%–15.47%] vs 8.29% [8.27%–8.32%]), disability rates (11.29% [11.12%–11.46%] vs 4.38% [4.32%–4.44%]), and all-cause mortality (8.17% [8.04%–8.30%] vs 1.86% [1.83%–1.89%]) at the 12-month follow-up showed a marked decline over the decade. Risk factors such as age (per 10 years), diabetes, and prior stroke were linked to a higher risk of 12-month stroke recurrence in CNSR I (CNSR I: odds ratio (OR) and 95% confidence interval (CI), 1.25 [1.17–1.33] for age per 10 years; 1.40 [1.18–1.66] for diabetes; and 1.96 [1.68–2.27] for prior stroke), and these associations remained significant after 10 years (CNSR III: OR and 95% CI, 1.15 [1.08–1.24] for age per 10 years; 1.35 [1.13–1.61] for diabetes; and 1.54 [1.29–1.84] for prior stroke).
Conclusion:
The past decade has witnessed significant advancements in both acute antithrombotic strategies and medication adherence, accompanied by marked reductions in stroke recurrence, disability, and mortality. These improvements highlight a positive shift toward more effective evidence-based care for patients with MIS or TIA.
Keywords
Introduction
Acute minor ischemic stroke (MIS) and transient ischemic attack (TIA) account for approximately 65.2% of all ischemic stroke events and pose a significant public health challenge globally. 1 According to TIAregistry.org, patients with MIS/TIA had a 12.9% risk of composite cardiovascular events and a 9.5% risk of stroke at 5 years, approximately twice the rates of 6.2% and 5.1%, respectively, reported at 1 year.2,3 Among recurrent ischemic stroke events, 40.9% were either disabling or fatal. 4 Given these serious consequences, it is crucial to review the trends in risk factors, management strategies, and both short- and long-term prognoses at the regional and national levels.
Over the past few decades, the management strategies for MIS and TIA have advanced rapidly. During the 2010s, several landmark randomized trials demonstrated the efficacy of various treatments such as dual antiplatelet therapy (DAPT) at the acute stage in patients with minor non-cardioembolic ischemic stroke,5 –8 anticoagulation in patients with atrial fibrillation, 9 and carotid endarterectomy or carotid artery stenting in patients with carotid artery stenosis. 10 Clinical guidelines have also evolved to offer evidence-based recommendations for reducing the MIS/TIA burden.10 –13 Consequently, the Florida Stroke Registry 14 reported a progressive increase in DAPT prescriptions since 2013. However, the real-world gaps still exist. 1 As reported by Lendaris et al, 15 nearly three-fourths of eligible high-risk TIA patients did not receive clopidogrel-aspirin, and TIAs were often underprescribed. Data from the Get with The Guidelines–Stroke program also revealed that approximately 53.0% of MIS patients did not receive DAPT, while 42.6% of non-MIS patients, who did not meet the CHANCE or POINT eligibility criteria, were inappropriately administered DAPT. 1 Similarly, the READAPT study 16 found that most patients receiving DAPT for the secondary prevention of minor stroke or high-risk TIA did not meet the strict criteria. Adherence to prescribed medications can significantly improve long-term survival rates in stroke patients. 17 However, an Australian Stroke Clinical Registry showed that approximately one-third of patients discontinued secondary prevention medications within 1 year of hospital discharge. 18
In real-world evidence studies, there is limited concurrent review of decade-long trends in baseline characteristics, risk factors, acute antithrombotic strategies, prescribing patterns, medication adherence, and their impact on MIS or TIA prognosis. Over the past decade, the China National Stroke Registries (CNSRs), covering 1% of the 13,372 general hospitals in China and spanning more than 10 years (2007–2018), have been launched to continuously provide evidence for clinical practice and enable a comparative analysis of trends in MIS and TIA.
This study utilized longitudinal data from CNSR I (2007–2008) and CNSR III (2015–2018) to examine decadal trends in risk factors, medical management, and prognosis of patients with MIS or TIA. Acute antithrombotic strategies and adherence to secondary prevention including antiplatelet therapy, anticoagulant agents, antihypertensive medications, and lipid-lowering agents were concurrently recorded. Stroke recurrence, disability, and mortality were monitored at 3, 6, and 12 months during each period.
Methods
CNSR program design and population
The CNSR is a nationwide, multicenter, consecutive hospital-based prospective registry sponsored by the Ministry of Health and Ministry of Science and Technology. CNSR-I enrolled 21,902 acute cerebrovascular stroke patients from 132 hospitals between September 2007 and August 2008. 19 CNSR-III enrolled 15,166 patients with acute ischemic stroke or TIA from 201 hospitals between August 2015 and March 2018. 20 The detailed protocol and baseline characteristics of CNSR-I 19 and CNSR-III 20 have been previously published.
Participants with acute MIS (National Institutes of Health Stroke Scale score ⩽ 3) and TIA from CNSR I and CNSR III were included in this study. TIA was defined as an episode of rapid-onset focal neurological dysfunction attributed to focal cerebral ischemia, with resolution within 24 h.21,22
The design and rationale of the CNSRs used in this study were approved by the Ethics Committee of Beijing Tiantan Hospital (approval number KY2015-001-01). Written informed consent was obtained from the participants or their legally authorized representatives. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. 23
Data acquisition
For each epoch, standardized data were collected by trained research coordinators and included demographic characteristics, physical examination, medical history, laboratory tests, in-hospital treatment, outcomes during hospitalization, and medications used at discharge. Medical history including hypertension, diabetes, dyslipidemia, stroke, TIA, coronary artery disease, heart failure, atrial fibrillation, and peripheral artery disease, was extracted from medical records. Medication use, including antiplatelet, anticoagulant, lipid-lowering, and antihypertensive strategies, was recorded by trained research personnel at 3, 6, and 12 months after stroke onset. Patients in CNSR-I were interviewed face-to-face at 3 months and contacted over the telephone at 6 and 12 months. All patients in CNSR-III were followed up at 3 months (face-to-face), 6 and 12 months (by telephone), and then annually for 4 more years (by telephone). Details of CNSR I 19 and CNSR III 20 data collection and variable definitions have been described previously.
Outcome assessment
The clinical outcomes evaluated at the 3-, 6-, and 12-month follow-up visits included stroke recurrence, disability, and all-cause death. Stroke recurrence included new ischemic stroke and recurrent hemorrhagic stroke (intracerebral hemorrhage and subarachnoid hemorrhage). Stroke recurrence was defined as a new symptomatic neurological deterioration that lasted for at least 24 h and was not attributable to a non-ischemic cause, or a new symptomatic neurological deterioration that was not attributable to a non-ischemic cause and was accompanied by neuroimaging evidence of a new brain infarction. 4 Poor functional outcome was defined as a modified Rankin Scale (mRS) score of 3–5, indicating a disability. All-cause death included mortality for any cause, including cardiovascular and nonvascular deaths.
Statistical analysis
Continuous variables were presented as mean (standard deviation) or median (interquartile range), and categorical variables were presented as numbers (percentages). Cumulative stroke recurrence, functional outcomes, and mortality were measured at 3, 6, and 12 months, with adjustments for age and sex to control for demographic differences. To track changes in risk factor patterns from CNSR I (2007–2008) to CNSR III (2015–2018), multivariable logistic regression models were used to examine the adjusted associations between stroke recurrence and disability at the 12-month follow-up, with interaction terms tested to explore the influence of the study period on these outcomes. We used a two-sided α level of .05 for all tests. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc).
Results
Baseline characteristics
In CNSR I, 21,902 patients with acute cerebrovascular events were initially recruited from 132 participating hospitals. Among them, 3906 patients with hemorrhagic stroke and 10,983 patients with major ischemic stroke were excluded. Finally, 7013 patients in CNSR I with acute MIS or TIA were included in this study. Among them, 3.7% (261/7013) were lost to follow-up at 3 months, 4.0% (272/6752) at 6 months, and 13.5% (873/6480) at 12 months (Figure 1(a)). In CNSR III, 15,166 patients with acute ischemic stroke were initially enrolled, and 8339 were diagnosed with acute MIS or TIA. Among them, 1.0% (84/8339) were lost to follow-up at 3 months, 0.1% (8/8255) at 6 months, and 1.0% (84/8247) at 12 months (Figure 1(b)). In summary, this study analyzed 15,352 patients with acute MIS or TIA, including 7013 patients from CNSR I (2007–2008) and 8339 patients from CNSR III (2015–2018).
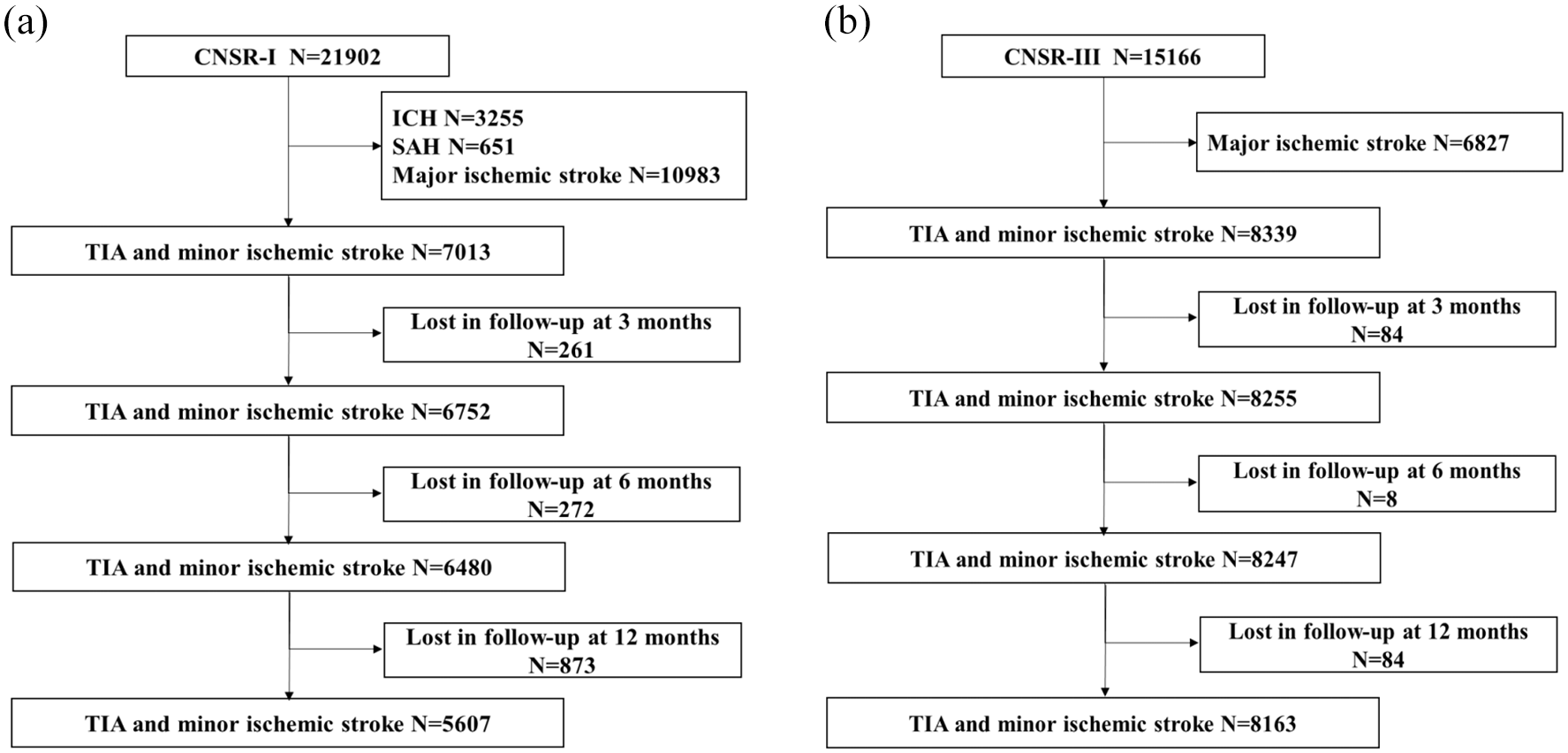
Flowchart of participants. Abbreviations: CNSR, China National Stroke Registries; TIA, transient ischemic attack; ICH, intracerebral hemorrhage; SAH, subarachnoid hemorrhage.
The baseline characteristics of the participants are presented in Table 1. In CNSR I (2007–2008), the median age of the patients was 65 years (interquartile range, 55–74 years), and 63.75% were men. Approximately 17% (1201/7013) had TIA and 83% (5812/7013) had MIS, and the median NIHSS score was 2 (1–3). In CNSR III (2015–2018), the median age of the patients was 62 years (interquartile range, 54–69 years), and 69.62% were men. Approximately 12% (1020/8339) had TIA and 88% (7319/8339) had MIS, and the median NIHSS score was 2 (1–2). As Table 1 shown, the proportions of traditional risk factors for acute MIS or TIA were similar over the program years (from CNSR I to CNSR III): hypertension (63.68% vs 62.50%), diabetes (20.39% vs 22.16%), and dyslipidemia (11.64% vs 8.53%).
Baseline characteristics of MIS/TIA patients by calendar year.
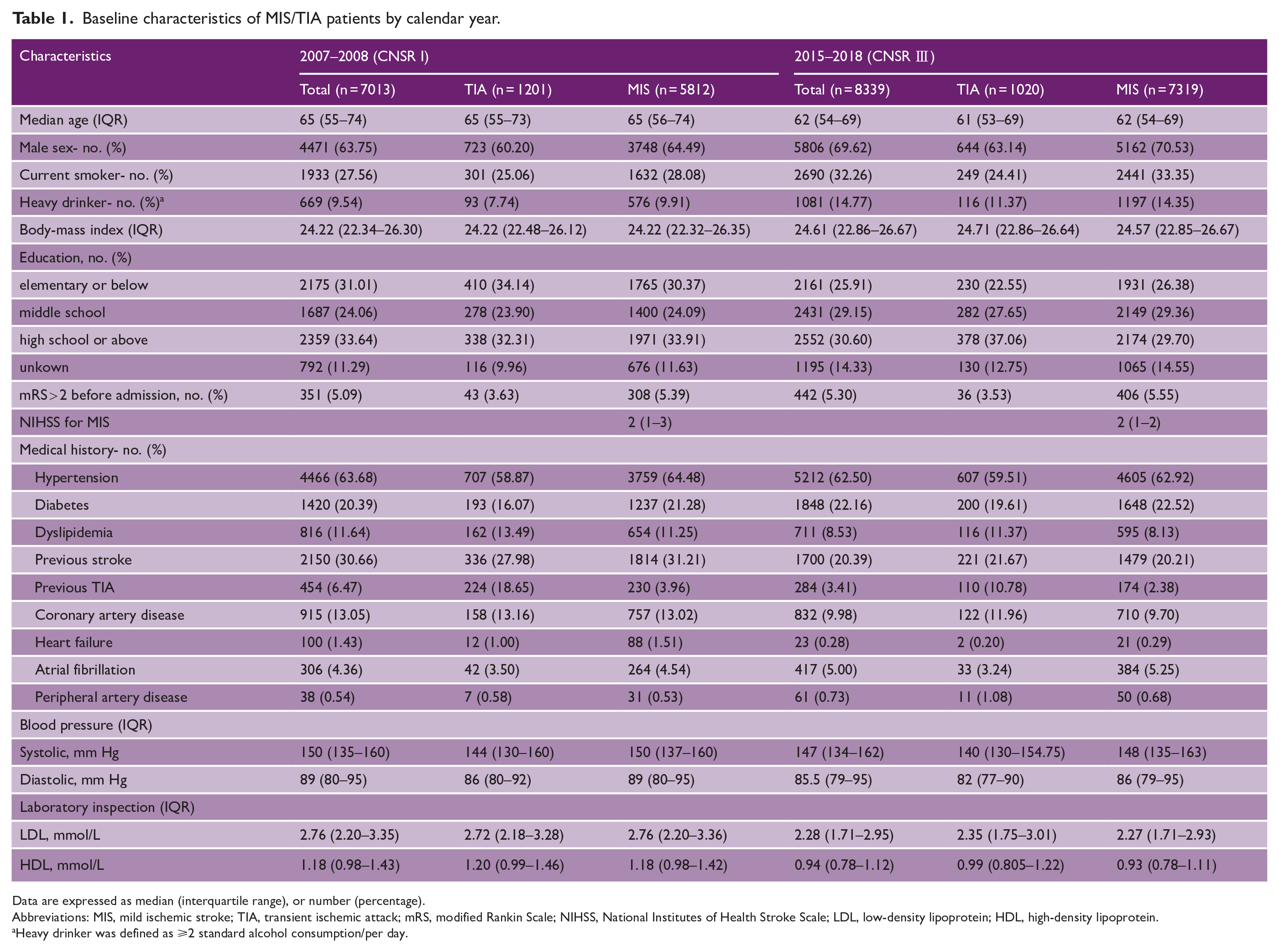
Data are expressed as median (interquartile range), or number (percentage).
Abbreviations: MIS, mild ischemic stroke; TIA, transient ischemic attack; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Heavy drinker was defined as ⩾2 standard alcohol consumption/per day.
Trends in management strategies
The overall data on the management strategy changes in patients with MIS/TIA are presented in Table 2. Figure 2 shows a clear visualization of the acute antithrombotic therapies and adherence to secondary prevention measures in CNSR I and CNSR III. Over the past decade, significant advancements have been made in acute antithrombotic therapies and adherence to secondary prevention.
Trend analysis of management strategies in patients with acute MIS or TIA.
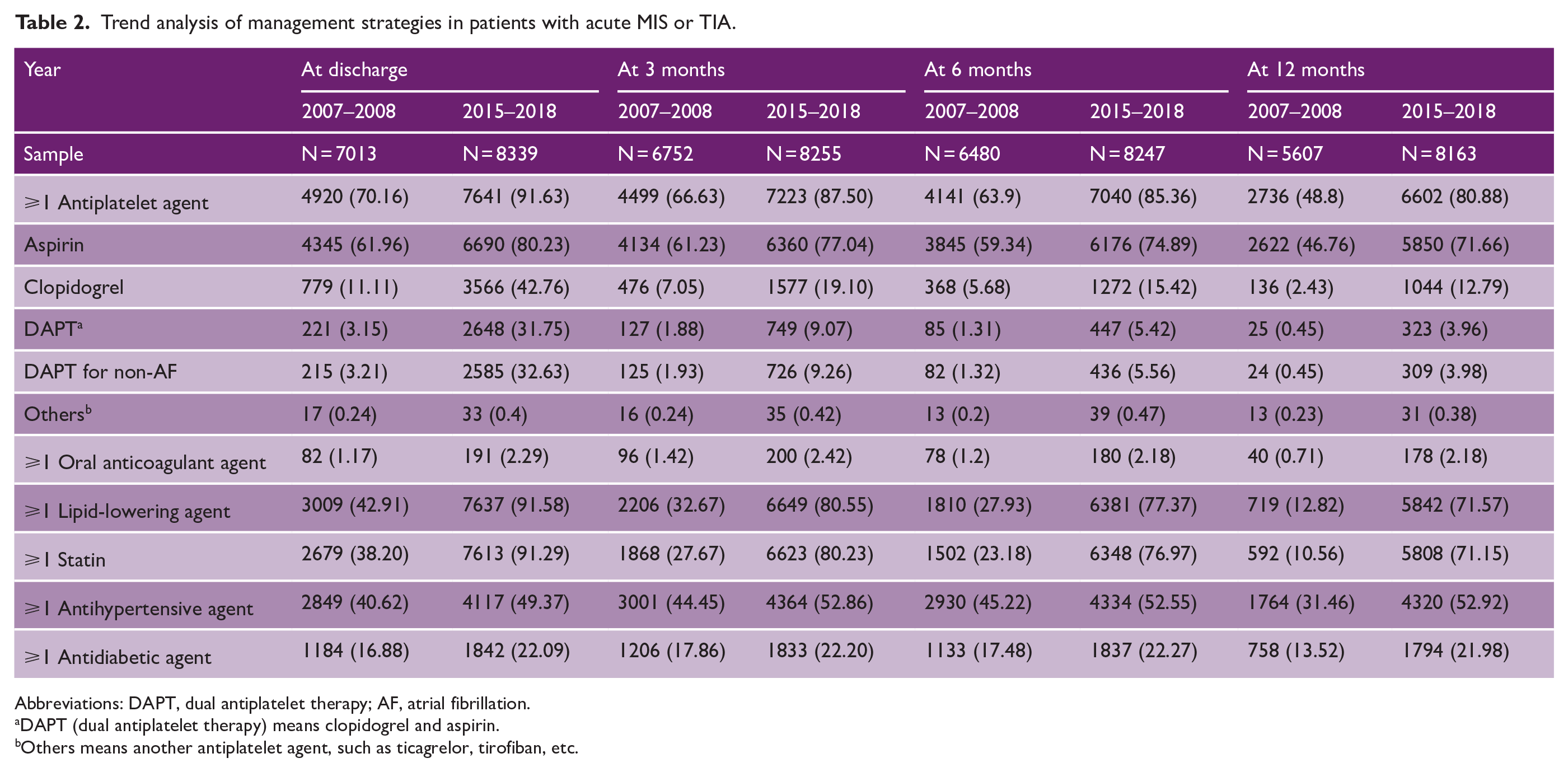
Abbreviations: DAPT, dual antiplatelet therapy; AF, atrial fibrillation.
DAPT (dual antiplatelet therapy) means clopidogrel and aspirin.
Others means another antiplatelet agent, such as ticagrelor, tirofiban, etc.
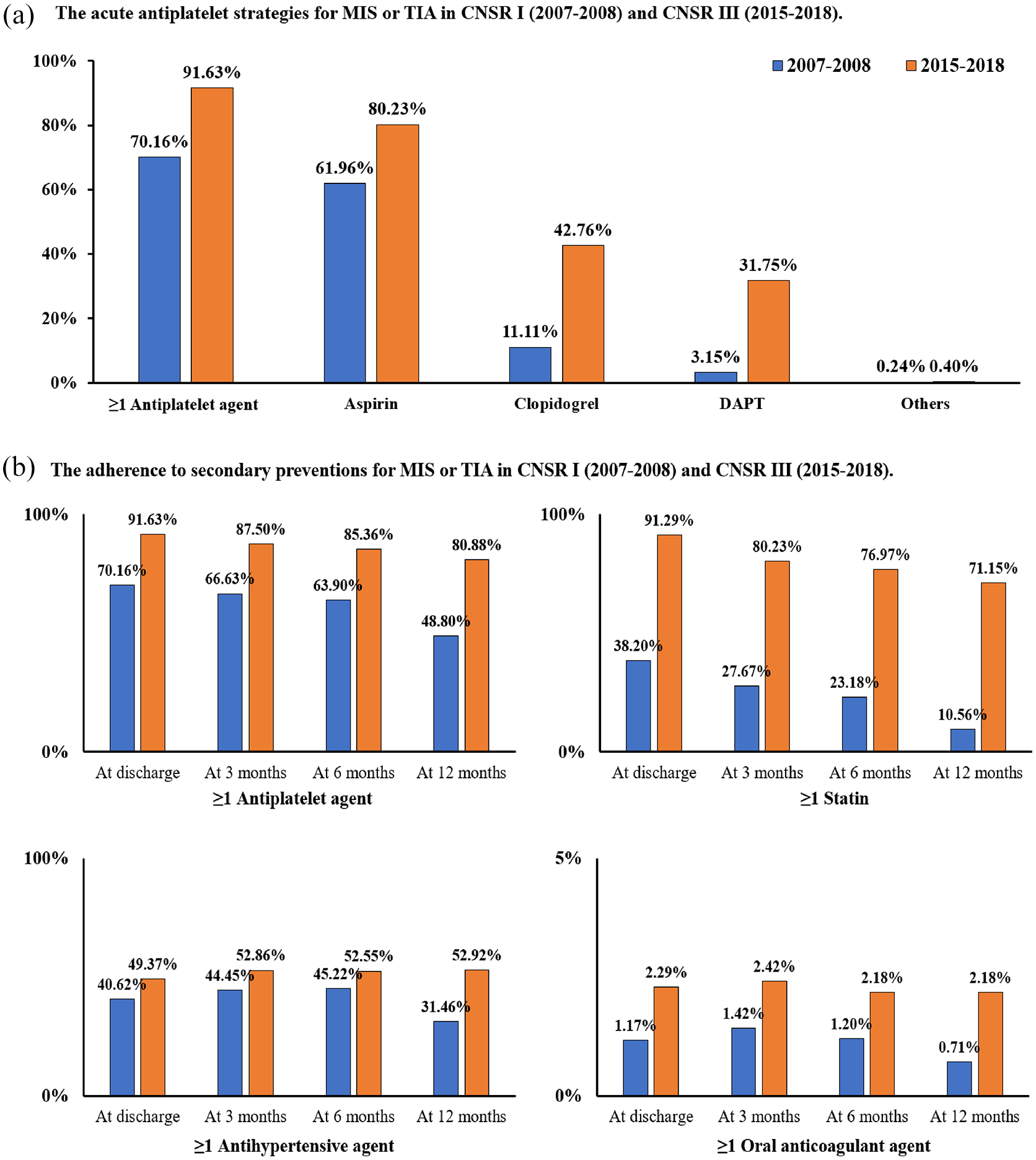
Trend analysis of acute therapies and adherence in MIS or TIA. Abbreviations: MIS, mild ischemic stroke; TIA, transient ischemic attack; DAPT, dual antiplatelet; CNSR, China National Stroke registries.
With respect to acute antithrombotic strategies (Figure 2(a)), participants from CNSR III were more likely to receive at least one antiplatelet agent at discharge (70.16% in CNSR I vs 91.63% in CNSR III, p for trend < 0.001). The proportion of aspirin use showed an upward trend (61.96% in CNSR I vs 80.23% in CNSR III, p for trend < 0.001), with an even more evident increase in clopidogrel use (11.11% in CNSR I vs 42.76% in CNSR III, p for trend < 0.001). Notably, an obvious shift was also observed in the use of DAPT at discharge, with a nearly 10-fold increase (3.15% in CNSR I vs 31.75% in CNSR III, p for trend < 0.001).
Regarding compliance with secondary preventive strategies (Figure 2(b)), antiplatelet use showed a significant increase, nearly doubling at 3 months (66.63% in CNSR I vs 87.50% in CNSR III, p for trend < 0.001), 6 months (63.90% in CNSR I vs 85.36% in CNSR III, p for trend < 0.001), and 12 months (48.80% in CNSR I vs 80.88% in CNSR III, p for trend < 0.001). Similarly, the proportion of statin use increased by nearly threefold at the 3-month follow-up (27.67% in CNSR I vs 80.23% in CNSR III, p for trend < 0.001), fourfold at the 6-month follow-up (23.18% in CNSR I vs 76.97% in CNSR III, p for trend < 0.001), and nearly sevenfold at the 12-month follow-up (10.56% in CNSR I vs 71.15% in CNSR III, p for trend < 0.001). A similar trend in medication adherence was observed for antihypertensive and antidiabetic agents.
Trends in stroke recurrence, disability, and mortality
Compared with the adjusted stroke recurrence at 3 months in CNSR I, that in CNSR III showed a notable downward trend (8.66% vs 5.16%), with similar trends observed at the 6 month (10.54% vs 6.52%) and 12 month (15.38% vs 8.29%) follow-ups (Figure 3). The rate of adjusted poor functional outcomes also decreased from CNSR I to CNSR III (12.17% vs 4.34% at 3-month follow-up; 11.90% vs 4.00% at 6-month follow-up; and 11.29% vs 4.38% at 12-month follow-up). Furthermore, there was a decremental trend in the adjusted all-cause mortality across all follow-up intervals from CNSR I to CNSR III (4.00% vs 0.71% at 3-month follow-up; 5.37% vs 1.12% at 6-month follow-up; and 8.17% vs 1.86% at 12-month follow-up). Similar trends were observed when patients were stratified by sex (Table 3).
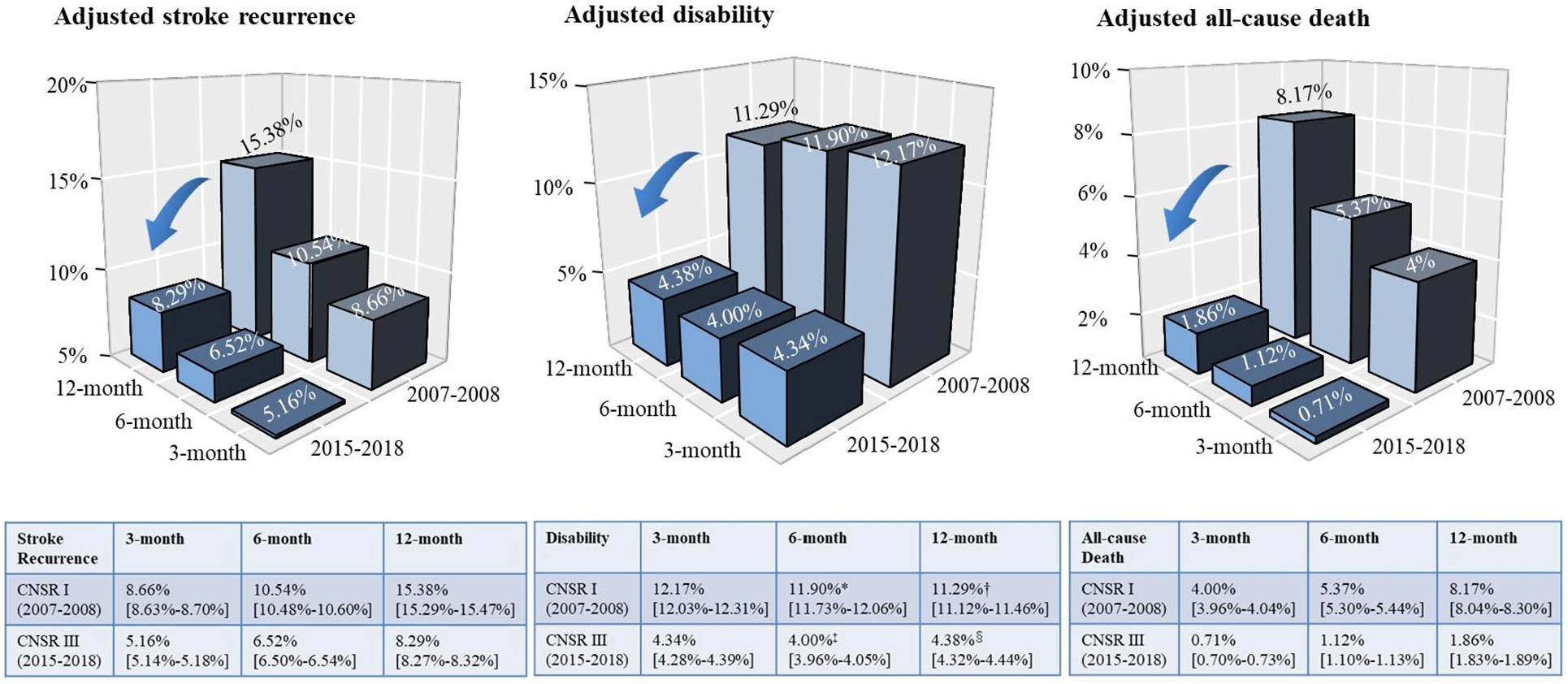
Trend analysis of prognosis in acute MIS or TIA. Abbreviations: MIS, mild ischemic stroke; TIA, transient ischemic attack; CNSR, China National Stroke registries.
Trend analysis of prognosis in MIS/TIA patients stratified by sex.
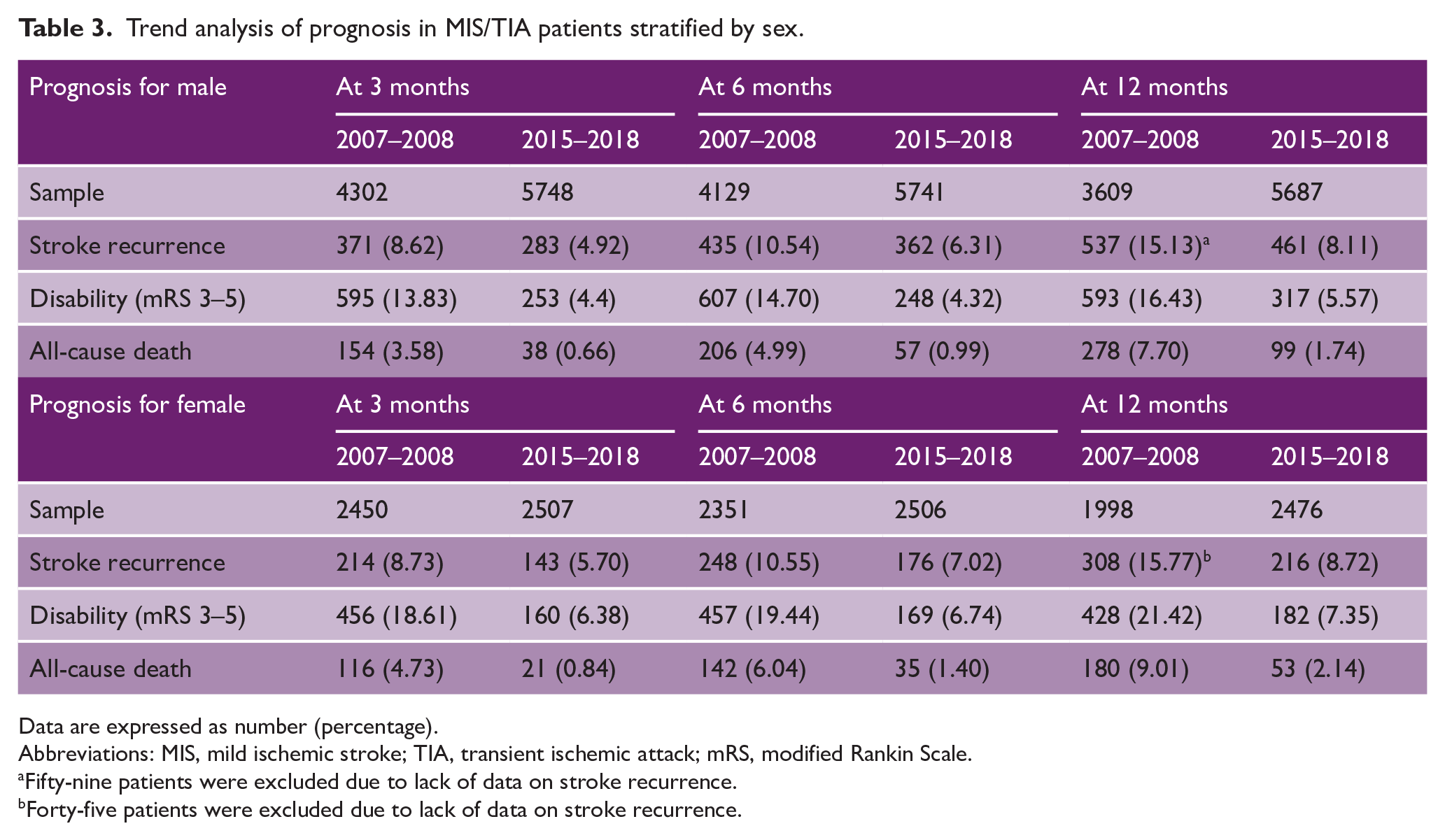
Data are expressed as number (percentage).
Abbreviations: MIS, mild ischemic stroke; TIA, transient ischemic attack; mRS, modified Rankin Scale.
Fifty-nine patients were excluded due to lack of data on stroke recurrence.
Forty-five patients were excluded due to lack of data on stroke recurrence.
Trends in risk factors patterns
As shown in Figure 4(a), factors such as age per 10 years, diabetes, and prior stroke were linked to a higher risk of 12-month stroke recurrence in CNSR I (CNSR I: odds ratio [OR] and 95% confidence interval [CI], 1.25 [1.17–1.33] for age per 10 years; 1.40 [1.18–1.66] for diabetes; and 1.96 [1.68–2.27] for prior stroke), and these associations persisted after 10 years (CNSR III: OR and 95% CI, 1.15 [1.08–1.24] for age per 10 years; 1.35 [1.13–1.61] for diabetes; and 1.54 [1.29–1.84] for prior stroke).
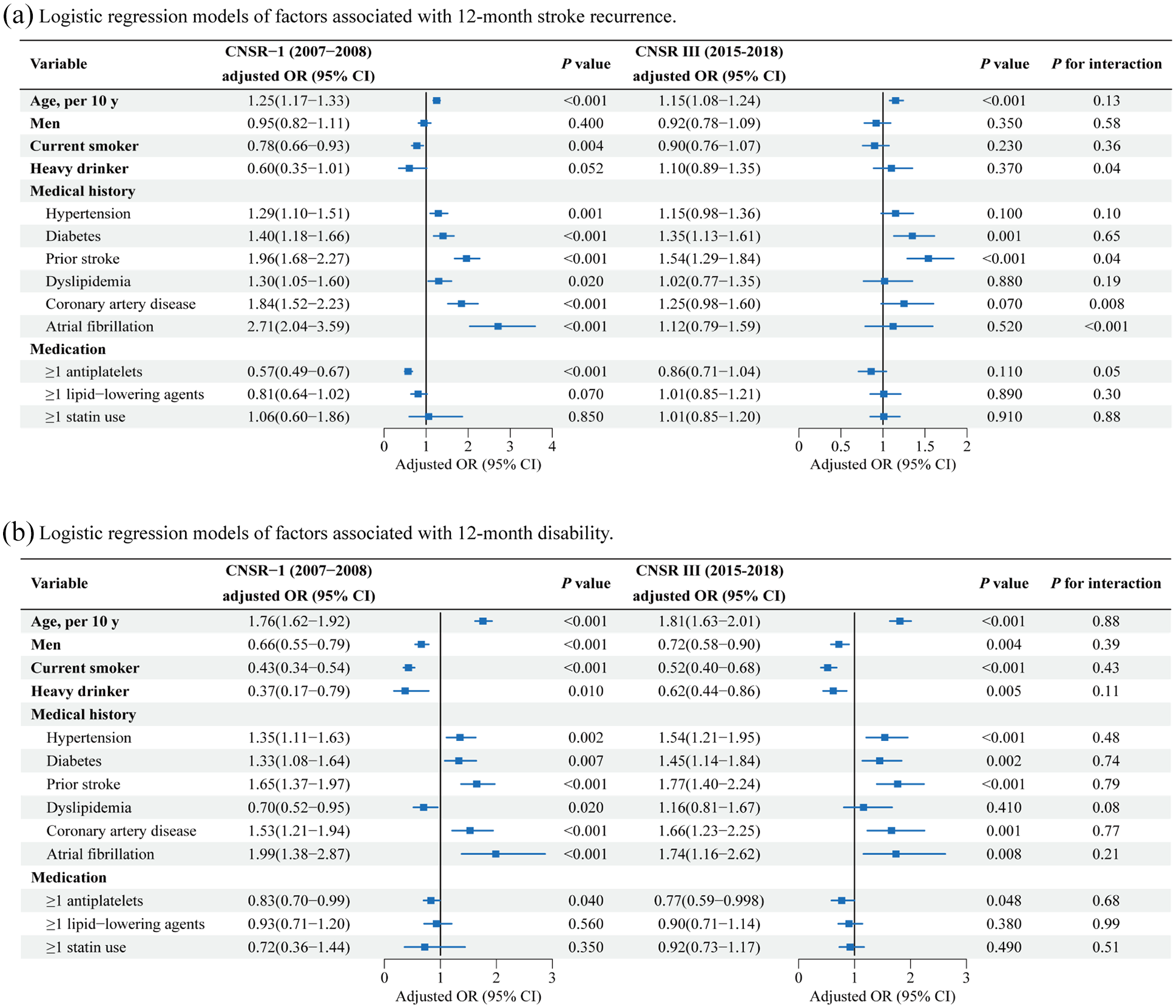
Logistic regression models of factors associated with 12-month stroke recurrence and disability.
As shown in Figure 4(b), factors associated with an increased risk of 12-month disability in CNSR I that remained significant after 10 years included age (per 10 years) (CNSR I: OR, 1.76; 95% CI, 1.62–1.92; CNSR III: OR, 1.81; 95% CI, 1.63–2.01), hypertension (CNSR I: OR, 1.35; 95% CI, 1.11–1.63; CNSR III: OR, 1.54; 95% CI, 1.21–1.95), diabetes (CNSR I: OR, 1.33; 95% CI, 1.08–1.64; CNSR III: OR, 1.45; 95% CI, 1.14–1.84), and prior stroke (CNSR I: OR, 1.65; 95% CI, 1.37–1.97; CNSR III: OR, 1.77; 95% CI, 1.40–2.24), among others.
Discussion
This study presents a decade-long analysis (2007–2018) of risk factors, medical management, and short- and long-term outcomes in patients with MIS or TIA in China. Our findings can be summarized as follows. First, the baseline characteristics and risk factors of MIS/TIA remained relatively consistent throughout the study period. Second, with a nearly 10-fold increase in the acute use of DAPT and nearly seven-fold increase in statin adherence, there was a significant reduction in stroke recurrence, morbidity, and mortality rates. These findings suggest that improving adherence to evidence-based acute therapies and medication compliance could be key focuses for quality improvement in the treatment of MIS or TIA patients.
Previous large cohort studies have reported trends in stroke recurrence after the onset of TIA/MIS. A recent meta-analysis of 206,455 unique TIA patients over five decades revealed a decreasing trend in post-TIA stroke risk before 1990 that continued through 2007, but this decline was not observed after 2007. 24 Moreover, the Framingham Heart Study, 22 which spanned from 1948 to 2017, found that compared with those during the earlier period of 1948–1985, the short- and long-term stroke risks after TIA significantly decreased during 2000–2017. A study in Australia reported a comparable trend in the first decade of the 2000s, showing that the age- and sex-adjusted risk of stroke within 90 days of TIA decreased by 3% per year. 25 However, these studies22,25 followed longitudinal cohorts and tracked the same group of individuals over time, without simultaneously recording risk factors and treatment strategies.
Consistent with previous studies,25,26 our study also observed a decline in stroke recurrence across two distinct cross-sectional populations, both of which were examined and followed up consistently. Although antiplatelet drugs, statins, and lipid-lowering agents are theoretically effective in reducing stroke recurrence, our analysis did not reveal a similar trend. In addition, the proportion of patients with smoking, alcohol use, and possibly diabetes increased over the past decade, yet disability at discharge decreased. This highlights the complexity of real-world situations in which factors such as patient adherence, treatment timing, and comorbidities influence outcomes. Although DAPT is widely recommended for secondary prevention, its effectiveness may vary based on individual characteristics and factors not captured in our analysis.
Breakthroughs in stroke prevention strategies have marked a period of profound change with the potential to significantly reduce stroke recurrence on a broad scale. Pivotal clinical trials, including the CHANCE 5 and POINT 6 trials, have provided robust evidence supporting the use of DAPT, especially in the acute phase following MIS or high-risk TIA. Following these findings, the American Heart Association/American Stroke Association (ASA/AHA) guidelines first listed DAPT as a Class IIb (Level of Evidence B) recommendation for acute use in TIA/MIS in 2014 and later upgraded it to a Class IIa (Level B-R) recommendation in 2018.11,12,27 Moreover, European guidelines 28 have also been revised to incorporate DAPT recommendations. Post-2015, there has been an increasing interest in exploring personalized therapies, such as ticagrelor for CYP2C19 loss-of-function carriers, as potential options for secondary prevention. 8 In this study, the nearly 10-fold increase in DAPT and 8-fold increase in statin adherence at the 12 month follow-up underscored the success of both acute and long-term therapeutic strategies. This reflects improvements in clinical guidelines, healthcare systems, and patient education, suggesting that more patients will benefit from evidence-based treatments.
In the coming decade, clinical trials for MIS and TIA are increasingly focusing on intensive antiplatelet therapy and thrombolysis. The TARDIS (Triple Antiplatelets for Reducing Dependency after Ischaemic Stroke) trial 29 enrolled 3,096 participants with TIA, evaluating the safety and efficacy of intensive triple antiplatelet therapy (a combination of aspirin, clopidogrel, and dipyridamole) against guideline-based antiplatelet treatment. However, the results indicated that triple antiplatelet therapy did not reduce the incidence of recurrent stroke or TIA but increased the risk of major bleeding. This suggests that future antiplatelet trials should focus on individuals with atherosclerotic disease. The upcoming CHANCE-4 trial (NCT06319846) aims to compare the efficacy and safety of the short-term use of tirofiban in addition to DAPT in preventing stroke recurrence in patients with intracranial artery stenosis and high-risk acute non-disabling cerebrovascular events, potentially providing further insights into triple antiplatelet therapy. Moreover, ongoing phase 3 trials are evaluating the efficacy and safety of novel factor XIa inhibitors for stroke prevention in patients with non-cardioembolic stroke or high-risk TIA, including the OCEANIC-STROKE study (NCT05686070) for asundexian and the LIBREXIA STROKE study (NCT05702034) for milvexian.
Regarding intravenous thrombolysis, the consensus continues to recommend against its use in non-disabling minor stroke or TIA because of an unfavorable risk-benefit profile. 30 The potential use of the new thrombolytic drug tenecteplase (TNK) in MIS/TIA patients remains uncertain. The TEMPO-2 trial, 31 which included 886 patients with MIS and intracranial occlusion or focal perfusion abnormalities, found no benefit, and possible harm, from treatment with intravenous TNK. Moreover, ongoing trials such as TRACE-4 (NCT06414499) will compare the efficacy and safety of TNK versus standard medical care in preventing stroke recurrence in patients with MIS. These ongoing trials for MIS/TIA have marked a significant step forward, but much work remains to be done. The continued focus is on developing safer, more effective, evidence-based antithrombotic strategies and comprehensive risk management approaches.
A remarkable finding of this study is that the development of antithrombotic strategies in the acute phase and the adherence to secondary prevention have significantly improved the prognosis of MIS and TIA in the real world over the past decade. The strengths of this study include its large sample size (15,352 participants) and extended follow-up period (at 3-, 6-, and 12-month follow-ups). Moreover, it recorded a decade of changes in adherence to secondary prevention. Nevertheless, this study has several limitations. First, this study did not account for factors influencing the prognosis that are difficult to quantify, such as rural-urban disparities, variations in healthcare coverage, and public awareness of stroke. 32 Second, insufficient data on ABCD2 scores, separate ischemic or hemorrhagic stroke recurrence, and loss to follow-up in the CNSR I phase may have affected the accuracy of the analysis. Finally, we did not record newly diagnosed atrial fibrillation during follow-up.
Conclusion
A comparison of CNSR I and CNSR III data shows that the past decade has witnessed significant advancements in both acute antithrombotic strategies and medication adherence, accompanied by marked reductions in stroke recurrence, disability, and mortality. These improvements highlight a positive shift toward more effective evidence-based care for patients with MIS or TIA.
Footnotes
Contributors
Y.J.W., J.J., and X.W.X. designed the study and supervised the project. T.L., C.H., Y.S., X.M.Y., X.M., Z.X.L, X.Q.Z., H.L., and Y.L.W. provided clinical samples for the study. Y.J. and M.X.W. performed statistical analyses. Q. M.J. and X.W.X wrote the manuscript.
J. J. is the guarantor of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China (grant nos. U20A20358; 82271329; 82471356), Beijing Hospitals Authority Youth Program (code: QML20230503), and AstraZeneca Investment (China) Co., Ltd.
Ethics approval
This study involved human participants and was approved by the IRB of Beijing Tiantan Hospital, Capital Medical University.
Patient consent for publication
Participants provided informed consent to participate in the study before taking part.
Provenance and peer review
Not commissioned; externally peer reviewed.
Data availability statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.